
Abstract
Objectives
The objective was to evaluate a nadir-led protocol for transitioning porcine lente insulin suspension (PLIS)-treated diabetic cats onto human recombinant protamine zinc insulin (PZIR).
Methods
Recently diagnosed (<5 months) diabetic cats, treated with PLIS q12h for ⩾6 weeks, were recruited. Fructosamine, 24 h blood glucose curve (BGC), quality of life assessment (DIAQoL-pet score) and Diabetic Clinical Score (DCS) were assessed at enrolment (PLIS-treated) and 2, 4 and 12 weeks after transitioning to PZIR (starting dose 0.2–0.7 U/kg q12h). Short duration of insulin action was defined as <9 h. Linear mixed effects modelling assessed for change in fructosamine, mean blood glucose (MBG) during BGCs, DIAQoL-pet score, DCS and q12h insulin dose. McNemar’s tests compared the proportion of cats with hypoglycaemia at week 0 (PLIS-treated) and week 4 (PZIR-treated).
Results
Twenty-two cats were recruited. Median PLIS dose at enrolment was 0.5 U/kg (interquartile range 0.3–0.7 U/kg) q12h, equalling median PZIR starting dose (0.5 U/kg; interquartile range 0.3–0.7 U/kg q12h). Transitioning was followed by significant decreases in fructosamine (P = 0.00007), insulin dose (P = 0.02), DCS (P = 8.1 × 10−8) and DIAQoL-pet score (P = 0.003), indicating improved quality of life. MBG did not alter significantly (P = 0.1). Five cats (22.7%) achieved remission. Hypoglycaemia was recorded in 30/190 12 h BGCs (15.8%) and five cats experienced clinical hypoglycaemia. The proportion of cats with hypoglycaemia did not differ between PLIS (week 0) and PZIR (week 4) (P = 1.0). Duration of action was analysed in 19 cats. Six cats (31.6%) showed short duration of action on PLIS, compared with two cats (10.5%) after 4 weeks on PZIR. All six cats with short PLIS duration showed duration of ⩾9 h on PZIR.
Conclusions and relevance
Used alongside a low-carbohydrate diet, transitioning to PZIR was associated with significantly improved clinical signs and quality of life, with some cats achieving remission. Transition to PZIR should be considered for cats with short duration of action on PLIS.
Introduction
The major goals in managing feline diabetes mellitus (DM) are to reduce or eliminate diabetic clinical signs while avoiding hypoglycaemia and other complications. 1 Treatment can also result in diabetic remission, which can substantially improve the quality of life of both cats and their owners. 2 Subcutaneous insulin q12h and a low-carbohydrate, high-protein diet are the mainstays of treatment.3,4 Although several different insulin types have been used for feline DM, a number of recent guidelines and a systematic review on diabetic remission recommend the use of long-acting insulin preparations when treating diabetic cats.3–5 Long-acting insulins include protamine zinc insulin (PZI) and the recombinant human insulin analogues glargine and detemir, and have been associated with a longer duration of action than porcine lente insulin suspension (PLIS), 6 which has an intermediate duration of action. This longer duration of action could help eliminate diabetic clinical signs, and could also increase a cat’s chance of diabetic remission because early, effective glycaemic control might reduce the deleterious effects of glucotoxicity on pancreatic beta-cells.5,7,8 However, until recently, PLIS (Caninsulin; MSD Animal Health) had been the only veterinary-licensed insulin in the UK and Europe.
The licensing of a human recombinant protamine zinc insulin solution (PZIR) (ProZinc; Boehringer Ingelheim) has recently changed the above situation, and information on transitioning cats from PLIS onto PZIR is therefore necessary. A previous study examining the efficacy of PZIR in diabetic cats included a small proportion of cats (n = 13) that were previously treated with other insulin types (mainly ultralente and neutral protamine Hagedorn). 9 However, no previous studies have specifically assessed the progress of PLIS-treated cats following transition to PZIR, or evaluated how best to conduct the transition. The aim of this study was therefore to evaluate prospectively the efficacy of a standardised nadir-based protocol to transition PLIS-treated cats onto PZIR using the manufacturer-recommended PZIR starting dose, and to document the effects in individual cats following this transition.
Materials and methods
This was a prospective, uncontrolled cohort study conducted at the Royal Veterinary College (RVC) Diabetic Remission Clinic between December 2013 and December 2015. Ethical approval was granted by the RVC Ethics and Welfare Board, and the Veterinary Medicines Directorate (Animal Test Certificate Number ATC-S-036). To be eligible, cats must have been diagnosed with DM in the last 5 months. This reasonably short duration of DM was chosen to increase the likelihood that some cats might achieve diabetic remission following transitioning because remission is reported to be more likely early in the course of a cat’s DM. 8 Diagnosis of DM was based on a history of compatible clinical signs (polyuria, polydipsia, polyphagia) and persistent hyperglycaemia (>15 mmol/l) at the time of their first trial appointment. These criteria were similar to those used in a previous study examining the effect of PZIR therapy in diabetic cats. 9 Recruited cats must have been receiving PLIS (Caninsulin; MSD Animal Health) q12h for a minimum of 6 weeks prior to their initial trial visit. This minimum duration of PLIS treatment aimed to allow cats to achieve stable glycaemic control using PLIS by the time of their trial recruitment visit. This initial treatment period also allowed cats with concurrent disease or suspected insulin resistance to be identified prior to their first trial visit. All cats were transitioned onto a high-protein, low-carbohydrate diet (<15% carbohydrate as metabolisable energy) a minimum of 10 days before their first trial appointment.
Final eligibility was based on the results of underlying disease screening at the initial visit. This involved clinical history and physical examination by residency-trained or board-certified internal medicine specialists (RG, CS, KH and SJMN). Cats then underwent complete blood cell count, serum biochemistry, serum total thyroxine, serum fructosamine, insulin-like growth factor-1 (IGF-1) and feline pancreatic lipase immunoreactivity (fPLI) measurement using assays previously validated for cats. Cystocentesis samples were submitted for urinalysis and bacterial culture, and cats also received abdominal ultrasonography and echocardiography by a residency-trained specialist.
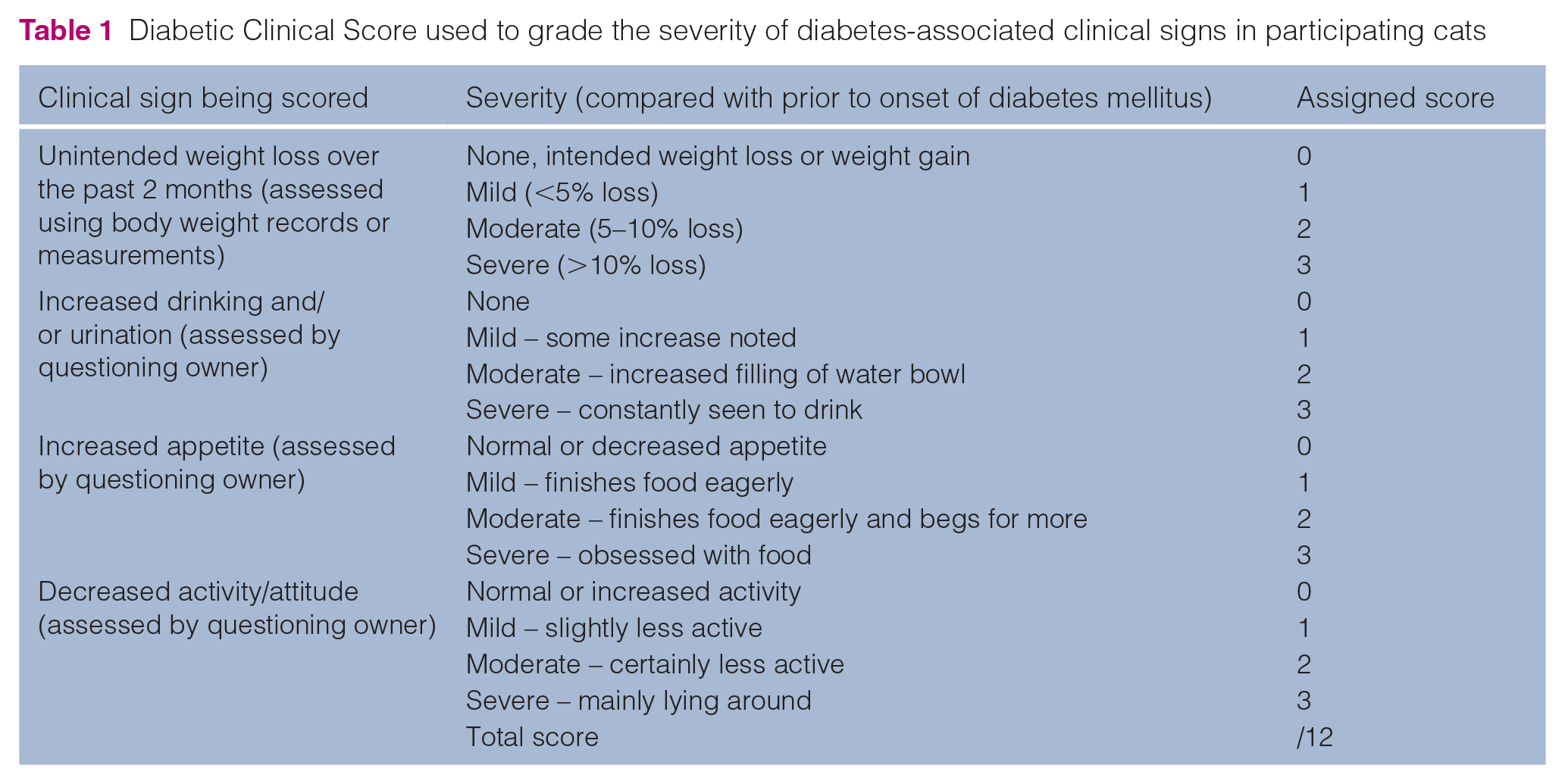
Each cat also underwent a 24 h blood glucose curve (BGC) to assess glycaemic control on their current PLIS regime. Curves were conducted using the Guardian REAL-Time Continuous Glucose Monitoring System (CGMS; Medtronic), starting at least 12 h after all laboratory tests and diagnostic imaging were complete. Curves were completed using 2-hourly readings with a veterinary handheld glucometer (AlphaTRAK 2; Zoetis) if the CGMS failed during the 24 h monitoring period. Each cat’s clinical signs at recruitment were graded using a validated clinical scoring system (Diabetic Clinical Score; Table 1). 10 The Diabetic Clinical Score (DCS) scores major clinical signs of poor diabetic control from 0 (absent) to 3 (severe) to generate a final score out of 12. Finally, cat and owner quality of life was estimated through owners completing the validated DIAQoL-pet quality-of-life questionnaire for diabetic cats. 11 The DIAQoL-pet generates an average-weighted impact score (AWIS) to reflect pet and owner quality of life, with more negative values reflecting a more negative impact of DM. Cats were excluded following the initial visit if they met one or more of the following exclusion criteria: long-acting glucocorticoid administration within the previous 60 days, or other systemic/inhaled glucocorticoids within the previous 30 days; administration of megesterol acetate or progestogens within the previous 6 months; an IGF-1 concentration of >1000 ng/ml, indicating likely hypersomatotropism; 12 concurrent hyperthyroidism – cats that had undergone successful radioactive iodine therapy or thyroidectomy remained eligible; clinical signs of pancreatitis accompanied by consistent pancreatic changes on abdominal ultrasonography and/or an fPLI concentration of >5.4 µg/l; concurrent disease of which management would have affected ability to comply with trial commitments, including IRIS stage 3 and 4 chronic kidney disease; patient aggression or fearfulness.
Diabetic Clinical Score used to grade the severity of diabetes-associated clinical signs in participating cats
Re-examination protocol
Enrolled cats had their insulin therapy changed to PZIR at the manufacturer’s recommended starting dose of 0.2–0.7 U/kg q12h at the time of discharge from their first appointment. Doses were chosen based on cats’ previous sensitivity to PLIS. All doses used throughout the study, including starting doses, were multiples of 0.5 U. Cats were re-examined at the Diabetic Remission Clinic 2, 4 and 12 weeks after starting PZIR therapy. At each visit, cats underwent assessment of serum fructosamine, DCS, 24 h water intake and a 24 h BGC. Results of 24 h BGCs at the 0, 2, 4 and 12 week re-examinations were used to calculate a mean blood glucose (MBG) concentration for each cat at these time points. Owners completed a repeated DIAQoL-pet questionnaire at 4 and 12 weeks. Cats also received a 12 h BGC at the 1 and 8 week time points, which could be performed at their primary care clinic, or at home using a handheld glucometer (AlphaTRAK 2; Zoetis), and could receive additional BGCs at home, or in primary practices, if clinically indicated.
PZIR dose was altered following each BGC over the 12 week trial using a nadir-based protocol (Table 2). All hypoglycaemic events, and episodes of diabetic remission, following transition to PZIR were recorded. Diabetic remission was defined as maintenance of normoglycaemia without receiving antihyperglycaemic medication (with the exception of low-carbohydrate diet) for a minimum of 28 days. This definition was based on the findings of a recent systematic review examining feline diabetic remission. 5 Hypoglycaemia was defined as a blood glucose (BG) concentration of <3 mmol/l (<54 mg/dl), based on a definition used by recent guidelines on the treatment of feline DM. 4 Any clinical signs compatible with hypoglycaemia, and other potential adverse events, were also recorded.
Nadir-based protocol used to alter PZIR dose according to the results of blood glucose curves (BGCs) during the 12 week study period

BG = blood glucose; PZIR = human recombinant protamine zinc insulin
A basic comparison of duration of insulin action was carried out between week 0, when cats were treated with PLIS, and week 4, when treated with PZIR. The week 4 time point was chosen a priori for calculation of PZIR duration of action in order to provide sufficient time for cats to stabilise on PZIR, yet also being early enough in the trial’s follow-up to avoid substantial numbers of trial withdrawals or the development of other complicating factors, such as cats entering diabetic remission. Duration of insulin action was calculated as the time from insulin administration until the time at which BG returned to its pre-insulin value following the patient’s BG nadir. This duration of action was calculated for each 12 h period in a cat’s 24 h BGC, and a mean value was taken. When BG did not return to its pre-insulin value, the duration of action for that 12 h period was assigned a value of 12 h, which is referred to as ‘long duration of action’ in the remainder of this study. In contrast, duration of action of <9 h was defined as ‘short duration of action’ on the basis that clinical signs are often expected when insulin duration is below this cut-off. 1 Any BGCs in which insulin was withheld to check for diabetic remission were excluded from duration of action analysis.
Statistical analysis
Continuous and ordinal data were assessed for normality using Shapiro–Wilk normality tests, and examination of descriptive statistics and histogram plots. Average values are expressed as mean ± SD for normally distributed data, and as median (interquartile range [IQR]) for non-normally distributed data.
Linear mixed-effects modelling with compound symmetry covariance structure assessed for change in MBG, serum fructosamine, q12h insulin dose, DCS and DIAQoL-pet score over the 12 week study period. Twice-daily insulin dose and DCS were logarithmically transformed in order to meet the model’s assumptions. For parameters that showed significant change, Fisher’s least significant difference post-hoc comparison was used to assess pairwise differences between each time point and week 0.
The proportion of cats affected by short and long duration of insulin action at the week 0 and week 4 time points was compared using McNemar’s tests. Cats with a short duration of action with either insulin type were evaluated to assess whether short duration of action was also present using the alternative insulin. A McNemar’s test was also used to assess the proportion of cats that had at least one hypoglycaemic reading detected during week 0 and week 4 BGCs.
Results
Thirty-nine cats were examined for trial inclusion between October 2013 and September 2015. Seventeen cats were excluded, with the most common reasons being identification of neoplasia or mass lesions (n = 4), likely hypersomatotropism (n = 3), excessive fearfulness or aggression (n = 3) and cats being non-insulin-dependent, based on in-hospital blood glucose monitoring (n = 2). Other reasons for exclusion were hyperthyroidism, gastrointestinal disease, suspected forebrain disease, hypertrophic cardiomyopathy with congestive heart failure and owners’ deciding against study enrolment (all n = 1).
All remaining 22 recruited cats completed the study. These consisted of 12 neutered males and 10 neutered females, and included 17 domestic shorthair cats, two domestic longhair cats and one cat of each of the following breeds: Abyssinian, Norwegian Forest and Singapura. Mean ± SD age was 10.6 ± 2.3 years and mean ± SD body weight was 4.9 ± 1.4 kg with a median body condition score of 6 (IQR 4–7/9). Cats had been diagnosed with DM a median of 71 days (IQR 49–93 days) prior to enrolment and had been receiving PLIS q12h for a median of 65 days (IQR 47–91 days) before enrolment. The exact date on which a low-carbohydrate, high-protein diet was started was known for 17 cats and was a median of 29 days (IQR 16–44 days) prior to their first trial appointment. The median PLIS dose received by cats at time of enrolment was 0.5 U/kg (IQR 0.3–0.7 U/kg) q12h and median starting dose of PZIR was 0.5 U/kg (0.3–0.7 U/kg) q12h. Seventeen owners (77%) used home blood glucose monitoring (HBGM) as part of their cat’s diabetic management.
Table 3 shows change in indicators of diabetic control over the 12 week study, and change in q12h insulin dose over the trial period is illustrated in Figure 1. A significant change was detected in serum fructosamine (P = 0.00007), q12h insulin dose (P = 0.02), DIAQol-pet AWIS (P = 0.003) and DCS (P = 8.1 × 10−8) over the study period. Post-hoc analysis revealed a significant decrease in both serum fructosamine concentration and DCS at every time point compared with week 0, whereas q12h insulin dose and DIAQoL-pet AWIS had both significantly decreased compared with baseline by week 12 (Table 3). MBG did not significantly change over the study period (P = 0.1). Over the trial period, 12 cats (55.4%) experienced an increase in body weight, nine cats (41%) experienced a decrease in body weight and body weight remained stable in one cat. Median water intake while hospitalised decreased from 28.6 ml/kg/day (IQR 19.6–39.0 ml/kg/day) at week 0 to 10.4 ml/kg/day (IQR 7.5–16.8 ml/kg/day) by week 12. Four cats (18.2%) entered diabetic remission during the study period, and one other cat had stopped PZIR by week 12 and went on to achieve successful remission.
Change in indicators of diabetic control among recruited cats over the 12 week study period. The table also indicates whether these changes reached statistical significance in linear mixed-effects modelling

All average values are reported as median (interquartile range)
P <0.5, **P <0.01 and ***P <0.001 compared with week 0 value in post-hoc analysis
BG = blood glucose; DCS = Diabetic Clinical Score; DIAQoL-pet = quality of life assessment; AWIS = average-weighted impact score
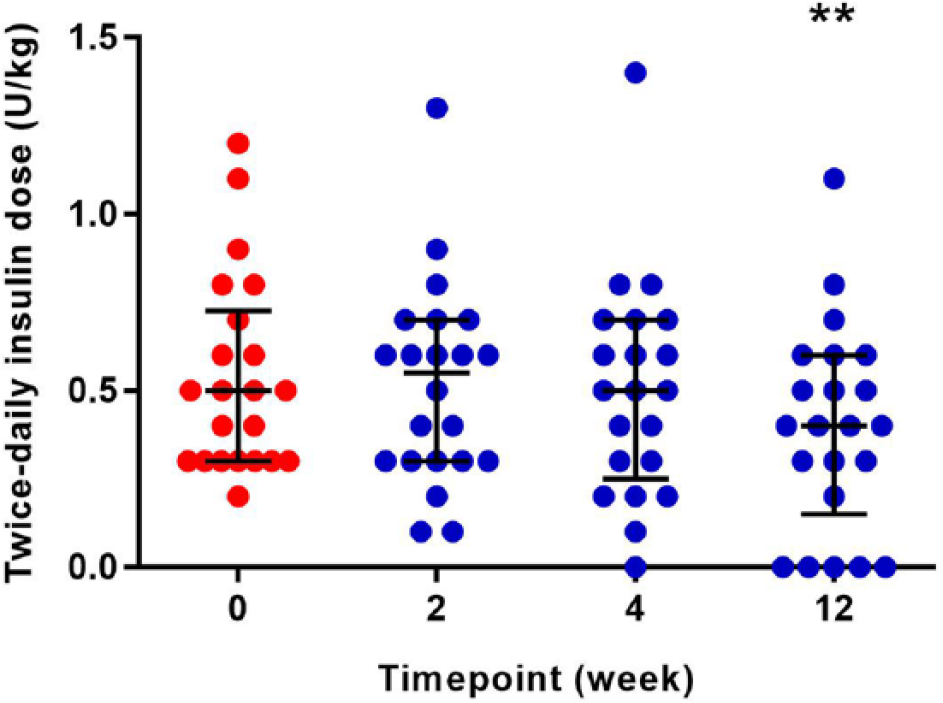
Scatterplot showing change in twice-daily insulin dose over study period. Red symbols indicate values when treated with porcine lente insulin suspension q12h, and blue symbols indicate values when treated with protamine zinc insulin solution q12h. **Significant difference compared with week 0 (P <0.01). Horizontal line and error bars indicate median and interquartile range
The study population underwent a total of 190 12 h periods of BG monitoring during the trial and hypoglycaemia was detected during 30 (15.8%) 12 h BGCs. Five cats experienced a hypoglycaemic episode associated with clinical signs. One clinical hypoglycaemic episode was detected during a BGC, whereas four were confirmed by owners performing a BG check on their cat at home. Clinical signs included subdued demeanour (n = 1), incoordination (n = 3), incoordination and blindness (n = 1) and collapse (n = 1). Three cases resolved with feeding and two cases recovered following intravenous glucose treatment. One of the five cats with symptomatic hypoglycaemia subsequently achieved remission. Seven of 22 cats (31.8%) became hypoglycaemic during their week 0 BGC using PLIS, whereas 4/19 cats (21.1%) that had a BGC at week 4 using PZIR experienced hypoglycaemia during their week 4 curve (P = 1.0). One cat developed a transient subcutaneous swelling at the site of PZIR administration. This swelling resolved without treatment.
Three cats were excluded from the analysis of duration of insulin action due to cessation of insulin by the 4 week time point (n = 2) or missing the 4 week re-examination owing to owner illness (n = 1). Six cats showed a short duration of action on PLIS compared with two cats after 4 weeks on PZIR (P = 0.18) (Figure 2). Six cats had long duration of action when treated with PZIR vs three cats when treated with PLIS (P = 0.5). All six cats that had a short duration of insulin action on PLIS, had a duration of PZIR action of ⩾9 h 4 weeks after transitioning. Both cats with short duration of action on PZIR had a duration of action ⩾9 h on PLIS (Figure 2).

Paired scatterplot showing duration of action of porcine lente insulin suspension (PLIS) q12h and protamine zinc insulin solution (PZIR) q12h in individual cats. Dashed line indicates short duration of insulin action (<9 h). Red symbols indicate duration when treated with PLIS q12h, and blue symbols indicate duration when treated with PZIR q12h. Pairs of values from individual cats have joining lines. Two pairs of cats had the same duration of action before and after transitioning (two decreasing from 12 h to 10.9 h and two increasing from 7 h to 12 h), resulting in only 17 data pairs being visible on the graph
Discussion
This study examined the efficacy of transitioning PLIS-treated diabetic cats onto PZIR using a standardised, nadir-led dosing protocol in conjunction with feeding a low-carbohydrate, high-protein diet. Transitioning using this protocol and appropriate dietary management was associated with an improvement in both fructosamine concentration and DM-related clinical signs within 2 weeks of starting PZIR. Pet and owner quality of life had significantly improved within 12 weeks of starting PZIR treatment, and 22.7% of cats achieved diabetic remission after starting PZIR. Individual cats that experienced short duration of PLIS action showed a resolution of this problem 4 weeks following transition onto PZIR. Hypoglycaemia was the most common side effect, as expected, although was rarely symptomatic, and was treated successfully. Hypoglycaemia was not more common with either insulin type when two, a priori, set time points were compared (t = 0 and t = 4 weeks post-transition).
The findings of this study support that PZIR is an effective therapy for feline DM, and that PZIR treatment can be associated with a rapid improvement in fructosamine concentration and clinical signs of DM in cats previously treated with PLIS, when used in a nadir-based protocol alongside a low-carbohydrate, high-protein diet. These findings agree with two previous trials which examined the efficacy of PZIR, 9 or related bovine- and porcine-derived PZI, 13 in both insulin-naïve and previously-treated diabetic cats. These studies found that approximately 85% of the whole study population achieved good glycaemic control within 45 days of starting PZI therapy, and 65–70% of previously-treated feline diabetics showed good diabetic control after 45 days of PZI therapy. However, both of these studies contained only one cat treated with PLIS q12h, so were unable to assess specifically the outcome of transitioning PLIS-treated cats onto PZI. This new information will be of particular interest to veterinarians looking for alternative insulin types for feline diabetics in the UK and Europe where PLIS has, until recently, been the only licensed veterinary insulin.
The current study is the first to include quality-of-life measurement as a treatment outcome and found that cat and owner quality of life, measured using a validated quality-of-life tool, was unchanged from baseline after 1 month of PZIR treatment, and had significantly improved by the end of the 12 week study. This improvement could be owing to owners and cats becoming accustomed to the treatment of DM, and that some cats had achieved diabetic remission by this time point. Remission would be expected to substantially increase the wellbeing of cats and their owners. Change in patients’ clinical signs of DM has been assessed by previous studies on PZI treatment in diabetic cats.9,13 However, this is also the first study to use a validated clinical scoring system 10 as a treatment outcome. This aimed to more consistently assess changes in clinical signs in a standardised fashion, representing an improvement on the methodology of previous trials.
PZI is proposed to offer better glycaemic control than PLIS in diabetic cats.3,4 This recommendation is founded on previous studies, which have shown PZI to have a longer duration of action than lente insulin in healthy cats, 6 as well as compared with other intermediate-duration insulin types in diabetic cats. 14 To our knowledge, no previous study has compared the duration of action of PZIR and PLIS in diabetic cats. Assessing duration of insulin action can be particularly challenging in diabetic cats because duration of action cannot be reliably estimated when cats have poorly controlled DM. 1 Also, diabetic cats typically receive insulin therapy every 12 h so measuring insulin duration of >12 h would not be possible without disrupting their usual treatment regime. This limitation prevented a precise comparison of insulin duration in the current study, which instead assessed duration of action characteristics by focusing on those cats that had a short duration of action when treated with either insulin type. All cats with a short duration of insulin action on PLIS showed a resolution of this problem when treated with PZIR. However, two cats were found to have a short duration of action when transitioned to PZIR but did not experience this problem on PLIS. Furthermore, nine other cats showed a decreased duration of action with PZIR compared with PLIS, but remained above the limit for short duration of action (Figure 2). These findings support previous observations that individual diabetic cats can be unpredictable in their response to different insulin types, 1 or their response can be difficult to ascertain reliably owing to documented day-to-day variability of BGCs in feline diabetics. 15 The employed CGMS had a maximum measureable blood glucose limit of >22.2 mmol/l (400 mg/dl) and this could have artificially reduced the estimated duration of action in some cats.
The only adverse events recorded in this study were hypoglycaemia, as expected, and one episode of transient swelling at the site of PZIR administration. The latter has been previously reported in PZIR-treated cats. 9 Hypoglycaemia was detected in 15.8% of all 12 h BGCs in the current study. This is slightly greater than the proportion of 9.0% detected in a trial examining the use of bovine/porcine PZI, 13 but less than the proportion of 22.2% reported in a previous study examining PZIR. 9 A higher proportion of cats in the current study experienced confirmed clinical hypoglycaemia compared with these two previous trials. However, most cat owners in the current study used HBGM to monitor their cat’s DM, whereas neither previous trial utilised HBGM. Four out of five clinical hypoglycaemic episodes in the current study were diagnosed by owners performing a one-off BG measurement at home. This frequent use of HBGM likely increased the number of confirmed clinical hypoglycaemic episodes compared with previous trials because owners were likely to check their cat’s BG promptly if concerned about their pet’s demeanour. This is in contrast to a previous PZIR study where BG measurement could not be performed at several times of suspected hypoglycaemia. 9 Finally, the current study predominantly carried out BGCs using CGMSs, which have been shown to detect hypoglycaemic BGC nadirs that might be missed during curves using handheld glucometers. 16 This is likely to have ensured that most hypoglycaemic episodes in this trial were successfully documented, especially when combined with the frequent use of HBGM. The current study is therefore likely to provide an accurate estimate of the incidence of hypoglycaemia among diabetic cats transitioned to PZIR.
This study did not document an improvement in MBG concentration over the duration of the study, despite an improvement in serum fructosamine concentration, DCS and several cats entering diabetic remission. As mentioned, the CGMS used to perform BGCs in this study had a maximum measureable BG concentration of 22.2 mmol/l (400 mg/dl), and this might have lowered the MBG values in some cats. Also, the BGCs, from which MBG was calculated, were all performed in hospital and so stress-related hyperglycaemia from hospitalisation might have affected BG measurements. 17 The study did aim to minimise stress-related hyperglycaemia by using a CGMS to perform BGCs and ensuring that all BGCs were performed more than 12 h after hospital admission. Although no significant change was detected in MBG, the fact that serum fructosamine concentration improved over the study period suggests that these in-hospital curves might not reflect cat’s diabetic control between re-examination visits. The earlier mentioned day-to-day variability of BGCs is also likely associated with this apparent discrepancy. 16
This study has some limitations. Although several markers of glycaemic control improved in included cats following their transition from PLIS to PZIR, the current trial was not designed to demonstrate unequivocally that one insulin preparation is superior to the other. For instance, it is possible that included cats would also have experienced an improvement in their diabetic control had they remained on PLIS therapy for longer, or had received PLIS according to a nadir-based protocol used in this study. Despite this, cats in the current study showed a rapid, significant improvement in diabetic clinical signs after starting PZIR, whereas a previous trial found that 3 months of PLIS therapy was needed to produce a significant improvement in clinical signs when starting diabetic cats on PLIS. 18
Other factors might also have played a role in the documented improvement post-transition in the current trial. These factors include the use of a nadir-based protocol, support from a dedicated DM clinic during the trial, and the fact that cats were transitioned onto a low-carbohydrate diet as part of the study protocol. Dietary carbohydrate restriction is likely to promote good glycaemic control in diabetic cats. 19 In this study, cats’ transition to a low-carbohydrate, high-protein diet was carried out before trial recruitment to allow the benefits of feeding a low-carbohydrate, high-protein diet to take effect before their first study visit. Although the minimum time for this diet change was 10 days prior to enrolment, recruited cats were fed a low-carbohydrate high-protein diet for a median of 29 days before their first trial appointment. A previous study found that insulin-treated diabetic cats experienced a significant decrease in MBG within 4 weeks of transitioning to a low-carbohydrate diet. 19 It is therefore likely that the benefits of changing to a low-carbohydrate, high-protein diet in the current study were already apparent by many cats’ first trial appointment and that subsequent improvements in glycaemic control were more related to other factors, including the change from PLIS to PZIR. Overall, an unbiased direct comparison of PZIR and PLIS would ultimately require an adequately powered, well designed, randomised clinical trial, which is currently lacking in the veterinary literature, as discussed in a recent systematic review of feline diabetes treatment. 5 However, the transition process described in this study provides valuable information, which can now be used to inform effective and safe transition protocols for cats requiring transition from PLIS to PZIR, for one reason or another.
Conclusions
Diabetic cats treated with intermediate-acting PLIS can be transitioned successfully onto long-acting PZIR using a nadir-led protocol and the manufacturer-recommended starting dose, alongside appropriate dietary management. When carried out through a dedicated feline DM clinic, transitioning to PZIR was associated with an improvement in fructosamine, diabetic clinical signs, and pet and owner quality of life, and a proportion of cats entered diabetic remission after starting PZIR therapy. Incidence of hypoglycaemia was similar to that previously described with PZI use in cats. This documented incidence of hypoglycaemia, the potential for diabetic remission and the efficacy of PZIR at modest dosages could nevertheless mean that conservative PZIR dosing should be used in cats where close monitoring cannot be performed. In conclusion, this study provides a framework for transitioning diabetic cats from PLIS to PZIR, if needed. Additionally, veterinary-licensed human recombinant PZI proved to be an effective treatment for feline DM and was associated with increased duration of action in those PLIS-treated cats with short duration of action. Licensed long-acting PZIR therefore provides a viable alternative treatment option to licensed intermediate-acting PLIS in feline diabetics, especially as recent recommendations emphasise the preferential use of long-acting insulin types.
Footnotes
Acknowledgements
With thanks to the staff of the Royal Veterinary College Clinic Investigation Centre, Dr Yu-Mei Chang for statistical assistance, and to cats and owners who participated in this study.
Conflict of interest
This study was supported by Boehringer Ingelheim.
Funding
This research was supported by Boehringer Ingelheim. The Royal Veterinary College Diabetic Remission Clinic also receives support from Nestlé Purina PetCare and Zoetis. The primary author’s PhD was supported by the Beryl Evetts and Robert Luff Animal Welfare Trust.