
Abstract
Practical relevance:
Auditory function is a sense that is central to life for cats - being important in situational awareness of potential predators, pursuit of prey, and for communication with conspecifics, humans and other species. Deafness in cats is most frequently the result of a genetic disorder, strongly associated with white fur and blue eyes, but may also result from acquired causes such as advancing age, ototoxic drugs, infection, environmental noise and physical trauma. Deafness can be sensorineural, where there is loss of cochlear hair cells, or conductive, where sound is muffled on its way to the inner ear.
Clinical challenges:
Establishing whether a cat is deaf can be difficult as behavioral testing of hearing is subjective and does not reliably detect unilateral deafness. Brainstem auditory evoked response testing is an objective measure but is limited in its availability. Currently, sensorineural deafness is irreversible because no treatments are available to restore lost hair cells. Conductive hearing loss can usually be treated, although full hearing recovery following otitis media may take weeks as the body clears the middle ear of debris.
Evidence base:
The author draws on the published literature and his extensive research on clinical aspects and molecular genetics of deafness, principally in companion animals, to review types and forms of deafness in cats. He also discusses current diagnostic approaches and provides brief advice for managing cats with hearing loss.
Auditory function, along with vision, is a sense that is central and critical to life for cats. It is important in situational awareness of potential predators, for pursuit of prey, and in communication with conspecifics, humans, and other species, among numerous other activities. Impairment or loss of auditory function is at best an inconvenience, but it can be life-threatening due to undetected dangers such as motor vehicles and predators.
Anatomy and physiology of hearing
In the normal ear, vibrations of sound in the ear canal - alternating compressions and rarefactions - produce vibrations of the tympanic membrane. These vibrations are transmitted by the three ossicles of the middle ear (malleus, incus and stapes) to the oval window of the inner ear (Figure 1), becoming amplified in the process. The vibrations are in turn transmitted into the inner ear as a standing wave going up the fluid-filled scala tympani to the apex and back down the scala vestibuli (which is continuous with the scala tympani) to the round window, which deflects 180° out of phase with the oval window. The pressures in the scala tympani and scala vestibuli cause deflections of the basilar membrane in the scala media (cochlear duct), upon which sits the organ of Corti that contains the sensory hair cells that ultimately transmit information about the sound into the brain via cranial nerve VIII (Figure 3).


Structures of the feline ear. 1 = pinna; 2 = external ear canal, consisting of a vertical canal and a horizontal canal; 3 = tympanic membrane; 4 = bulla/middle ear space; 5 = auditory tube; 6 = middle ear ossicles (malleus, incus and stapes); 7 = cochlea; 8 = vestibular structures; 9 = cranial nerve VIII. Reproduced from Ryugo and Menotti-Raymond, 1 with permission


Structures of the cochlea in cross-section. Inner hair cells in the organ of Corti are the primary sensory transduction cells, while the outer hair cells utilize active processes to increase or decrease sensitivity. Pigment cells in the stria vascularis play a major role in maintaining high potassium levels in the cochlear duct to support hair cell viability. Hair cells synapse on neurons of the spiral ganglion, which in turn become components of cranial nerve VIII. Reproduced from Bloom and Fawcett,8 with permission
The organ of Corti consists of one row of inner hair cells and three rows of outer hair cells that map out along the basilar membrane as it coils around in the snail-shell shaped cochlea. The inner hair cells are primarily sensory in function, while the outer hair cells primarily serve as an active system that can increase or decrease sensitivity. In addition to the outer hair cells providing a means to decrease hearing sensitivity, the brain also has a mechanism to protect the cochlea against loud sounds through the actions of two muscles in the middle ear: the tensor tympani and stapedius muscles. These muscles contract as a reflex response to loud sounds (and prior to vocalizations or in response to touch) and, in so doing, dampen the transmission of sound through the ossicles. This protective reflex is not fast enough, however, to guard against percussive sounds like gunfire.
The organ of Corti sensory cells - the hair cells - have stereocilia on their top surface that project upward into a gelatinous structure in the cochlear duct known as the tectorial membrane, and are surrounded by a potassium-rich fluid called endolymph (Figure 3). The stereocilia on each hair cell are arranged in a chevron pattern, pointing from the shortest on one edge of the top surface to the tallest at the opposite edge (Figure 4). Each stereocilium is attached to adjacent stereocilia by fine microfilaments that are in turn attached to potassium ion channels. When the basilar membrane is deflected upward by a sound wave, the hair cell stereocilia are pressed against the tectorial membrane, bending them and putting tension on the microfilaments. The tension opens mechanically gated potassium channels, allowing a large influx of potassium ions from the endolymph; this influx depolarizes the inside of the hair cell. The potassium-mediated depolarization in turn opens voltage-gated calcium ion channels, and the resultant calcium influx further depolarizes the hair cell and triggers the release of the excitatory neurotransmitter glutamate onto afferent spiral ganglion neurons that ultimately join to become cranial nerve VIII.

Scanning electron micrographs of cochlear hair cells. (a) Hair cells and their stereocilia. (b) Higher magnification view of the stereocilia on an outer hair cell. The stereocilia are approximately 5 μm in length. Reproduced from Bear et al, 9 with permission
The high potassium levels in the endolymph fluid surrounding the hair cells are maintained by a modified vascular structure called the stria vascularis, located on the lateral wall of the cochlear duct. Important cellular components of the stria vascularis are melanocytes that migrated embryologically from the neural crest, and which play a vital role in maintaining the elevated potassium levels in the endolymph. Damage to hair cells can produce deafness as a primary event, but damage to the stria vascularis can also produce deafness, with hair cell death occurring secondarily to the strial degeneration and loss of potassium in the endolymph.
Forms of deafness
Numerous authors have discussed or examined the condition of deafness in white cats, dating back to as early as 1829 10 and including Darwin in ‘The origin of species’.1,10-33 However, many forms of deafness are possible, which creates the need for a classification system using a variety of criteria.
Hearing loss can be variously classified as: 34
Peripheral deafness can in turn be classified based on three pairs of criteria:
These last three criteria combine into eight possible combinations including: hereditary congenital sensorineural deafness (the most common type in cats); acquired late-onset conductive deafness (probably the second-most common type); acquired late-onset sensorineural deafness; and others (Table 1).
Types of peripheral hearing loss
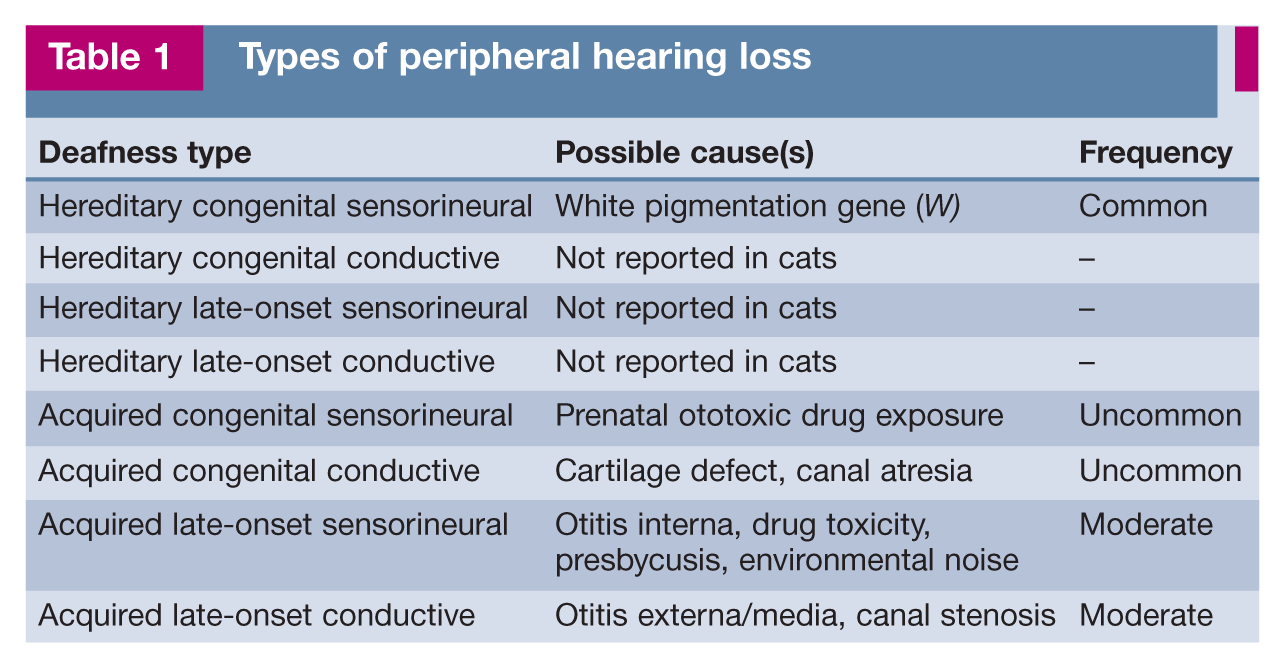
Not all of these types of peripheral deafness have been reported in cats. Hereditary congenital sensorineural deafness - the only type of hereditary deafness reported in cats to date - is most commonly associated with white fur, especially in cats with blue eyes. Acquired late-onset conductive deafness is most commonly associated with otitis media and/or externa. Acquired late-onset sensorineural deafness is most commonly associated with drug ototoxicity (eg, gentamicin) or age-related hearing loss (presbycusis).


Deafness in blue-eyed white cats is perhaps the most recognized form of deafness in animals. ©iStock.com/Pley
Hereditary deafness
Pathology of hereditary deafness
The forms of hereditary deafness can be separated based on the type of pathology present. Steel35-37 developed a classification system with three types of pathology that cover observed forms of deafness. These include a morphogenetic pathology and two types of degenerative pathology, as described below.
Morphogenetic
This category includes all structural abnormalities of the membranous and bony labyrinths, which at its extreme includes a complete absence of auditory and / or vestibular components. The effects of this pathology on hearing can vary from profound deafness to no hearing loss that nevertheless is accompanied by effects on vestibular structures. This rare condition is essentially a major birth defect.
Neuroepithelial
This pathology presents with a loss of cochlear hair cells as the primary event, beginning when normal histological development of the organ of Corti is finishing following birth. outer hair cells degenerate before inner hair cells, beginning in the upper part of the basal turn and progressing to both the apex and the base. 35 Supporting cells of the organ of Corti collapse, leaving the basilar membrane and dedif -ferentiated cells (ie, those that have reverted back to their undifferentiated state). The stria vascularis and Reissner’s membrane are initially unaffected and any or all vestibular structures can be affected. The expression of this pathology is typically bilateral. An endocochlear potential (voltage measured between the cochlear duct and the exterior of the cochlea, and produced by potassium secretion by the stria) may still be present in the endolymph of the cochlear duct because of continued potassium secretion by the stria vascularis. 38
This pathology has been reported in mice, 39 guinea pigs,40,41 dogs42-44 and humans. 45 It may also occur in cats based on reports of the presence of deafness with coexisting vestibular pathology,46,47 but this has not been documented histologically.
Cochleosaccular
This condition, also known as Scheibe type pathology, results from an initial degeneration of the stria vascularis on the outer wall of the cochlear duct, proceeding to degeneration of hair cells, and collapse of Reissner’s membrane. It may occasionally also include collapse of the saccule, with collapse of the saccule wall and macular damage but without any effect on the remainder of the vestibular structures. The expression of this pathology is more often unilateral, but both ears can be affected. No endocochlear potential remains due to the strial degeneration. The initial strial degeneration is usually linked to the absence of functioning melanocytes, and as a result may be described as pigment-associated, often also linked to lack of pigmentation in the skin, iris and tapetum lucidum.
Cochleosaccular pathology has been reported in the white cat,21,22,48 the Dalmatian49-51 and other dog breeds,52,53 Hedlund white mink,54,55 several mouse mutants,56,57 and as Waardenburg syndrome in humans. 58 As background reference, the normal postnatal maturation of the stria vascularis has been described for the dog 59 and the functional morphology of melanocyte types has been described for the mouse. 60 Unilateral congenital deafness has been shown to produce minor alterations in the ventral cochlear nucleus in rats 61 and cerebral cortex in cats,62-64 but the changes are not sufficiently extensive to affect brain function except for localization of sound sources.
Genes associated with hereditary deafness
Along with deafness in Dalmatians, deafness in blue-eyed white cats is perhaps the most recognized form of deafness in animals. Most hereditary deafness in cats involves cochleosaccular pathology, although some neuroepithelial pathology associated with vestibular signs may also exist. Whether two genes or a single gene is responsible for white pigmentation in the cat is unsettled, as discussed on page 280. 65

Neuroepithelial deafness
Cases of combined deafness and vestibular disease have been reported in Siamese and Burmese kittens,46,47 but little is known about neuroepithelial deafness in cats. Vestibular signs appear at or shortly after birth, are non-progressive, and may disappear with time. In some cases, deafness was determined based on behavioral tests; BAER testing was not routinely performed and histological studies were not reported.
Acquired deafness
Acquired hearing loss is much less common than hereditary deafness in cats. The most frequently encountered form is due to ototoxicity; other forms include presbycusis, and deafness due to infection, anesthesia, environmental noise or physical trauma. 77
Ototoxicity
A variety of drugs and other chemicals have been demonstrated to have toxic effects on the inner ear, affecting auditory and / or vestibular function.78-83 The most prominent of these are the aminoglycoside antibiotics,84-88 antineoplastic agents, 89 diuretics and antiseptics.
Aminoglycosides
Aminoglycosides are the most frequently used antibiotics worldwide for treating gramnegative infections in humans, and are likewise heavily used in veterinary medicine. This drug class includes gentamicin, tobramycin, neomycin, kanamycin, amikacin and streptomycin. Gentamicin is one of the most commonly used antibiotics for topical treatment of otitis externa.
The side effects of aminoglycosides are nephrotoxicity (often reversible) and ototoxicity (both cochlear and vestibular, usually irreversible), and can result from systemic or topical application. Toxicity usually develops after long-term, high-dose administration, but is unpredictable and may occur after a single high dose 90 or long after cessation of treatment. Three weeks of twice daily topical otic treatment in dogs produced no observable BAER changes with either intact or excised tympanic membranes. 91 Perinatal cats are less susceptible to aminoglycoside toxicity than older animals, but still may be affected. 92
Studies in recent years have revealed the sequential mechanisms of ototoxicity to be iron chelation, followed by free radical formation, and thereafter caspase-dependent apoptosis. 93 Co-administration of aspirin 94 or other antioxidants such as D-methionine or N-acetylcysteine with gentamicin has been shown to reduce or prevent gentamicin ototoxicity, but the clinical utility of such treatments in veterinary practice has not been demonstrated. Other possibly protective antioxidants include deferoxamine, dihydroxy -benzoic acid, glutathione and a-lipoic acid. 83
Different aminoglycoside antibiotics vary in their effects on the cochlea and vestibular structures; as a result, vestibular signs may be more prominent than auditory deficits. The auditory deficits, which are progressive, are frequently not noticed by owners or clinicians until significant damage has occurred. In addition to gentamicin, streptomycin, neo -mycin and others in this drug class may cause hearing loss.
Antineoplastic agents
Chemotherapeutic agents such as cisplatin and carboplatin produce irreversible hearing loss by their actions on hair cells and on the stria vascularis, but the vestibular system is not affected. The mechanism is thought to be through production of reactive oxygen species. Co-administration of antioxidants may provide some protective effect when drug use is deemed necessary.
Diuretics and other drugs
Loop diuretics, especially furosemide and etacrynic acid, can produce hearing loss, but the loss is usually temporary. However, diuretics can potentiate the ototoxicity of aminoglycosides and antineoplastics. 83 The mechanism is probably related to effects on ion transport by the stria vascularis. Salicylates and quinine can also produce hearing loss, which is often accompanied by tinnitus, but the effects are usually reversible with discontinuation of the drug.
Antiseptics
The antiseptic chlorhexidine has demonstrated permanent ototoxicity. This was especially prevalent when chlorhexidine was marketed in an otic preparation, but as with other ototoxic products the toxicity was not consistent. 95 Removal of the otic indication from the product has reduced the prevalence of this toxicity, but some practitioners still apply dilutions of other chlorhexidine formulations for otic use as a misguided economy measure.
Presbycusis
Presbycusis refers to reduced auditory perception with advancing age.96-98 The mechanisms are primarily sensorineural, although conductive middle ear effects may contribute, and are progressive. 96 The mechanisms are also primarily peripheral, although there may be central changes as a component.
Little research has been published on presbycusis in animals,99-103 and no feline clinical studies appear to have been reported. one long-term study of dogs using tone-evoked BAER demonstrated a progressive loss of hearing in aging dogs, with middle and high frequencies affected first. 100
It is highly likely that presbycusis develops in a similar pattern in geriatric cats, but more study is required. Cats are considered to be geriatric based on when they are most likely to start having diseases associated with aging: >11.88 + 1.94 years, according to one source. 104 Another source classifies ⩾15 years of age as being geriatric and 11-14 years as being senior. 105 Based on what is known in dogs, the onset of losses associated with presbycusis might be expected to occur before the cat reaches geriatric age. However, recent unpublished data from the author’s laboratory show that presbycusis is uncommon in cats in their teen years, and, if present after that age, is much less severe than in dogs.
The presence of presbycusis may contribute to problem behaviors in older animals.106,107
Other forms
A variety of other, less common forms of hearing loss exist, although the cause of acute-onset hearing loss is often never identified.
Diagnosis of hearing loss
A cat presented with suspected hearing loss should first have otitis externa and otitis media ruled out by otoscopic examination, and otitis interna ruled out to the extent possible by testing for sensitivity to palpation of the ear and the presence of vestibular signs. Factors that can suggest other etiologies are age (presbycusis), skin/hair/iris color (white/white/blue, hereditary), and a history of recent treatment with potentially ototoxic drugs (especially gentamicin), noise exposure or trauma.

BAER testing
Objective testing of hearing is performed using the BAER (brainstem auditory evoked response), also known as the auditory brainstem response and several other variants.115-118 This test can be performed both in awake and unconscious cats and is unaffected by drugs (except ototoxic drugs). An auditory stimulus is inserted into an ear and the response of the auditory pathway is detected by subdermal needle electrodes placed on the cranial vertex and outside the ear canal (Figure 6). The response is a series of peaks that occur within about 5 ms. The amplitude of the response is small enough (microvolts) that responses to multiple stimuli must be averaged to remove the confounding effects of physiologic (electromyogram and electroencephalogram) and other unrelated biologic and external signals that can mask the response. The stimulus typically used is a click sound, which contains all but the highest of the audible frequencies in the cat. Pure tone stimuli may also be used if attempting to obtain an audiogram of thresholds at different frequencies, but anesthesia is required and the process is time-consuming.

Cat gently restrained, with electrodes in place, and BAER testing of the right ear being performed
In the clinical setting, the BAER is used most commonly to screen for hearing or deaf ears, since pigment-associated hereditary congenital deafness nearly always presents as either total deafness in an ear or a normal response. The BAER recording of a deaf ear is essentially a flat line (Figure 7). The extent of partial hearing loss, when present, is very difficult to assess objectively with the BAER test. Response peak latencies increase and peak amplitudes decrease with increasingly softer stimuli or with progressively greater hearing loss, but due to test-retest variability and subject-to-subject variability it is unsafe to attempt to quantify partial hearing loss in the manner that is done in human subjects.

(top) BAER recording from a 2-year-old normal cat, with peaks I, II, III and V labeled on the tracing. Peak I is generated by cranial nerve VIII entering the brain, while the later peaks are generated in the brainstem. (bottom) By comparison, this essentially flat line is a recording from a bilaterally deaf cat. 0.5 μv/div and 1 ms/div
The availability of BAER testing is limited because of equipment costs. A partial listing of available test sites, both within and outside of North America, is available online. 119
Other tests of auditory function
other tests of auditory function are available, but are less commonly utilized. 120 One of these involves otoacoustic emissions (oAEs), where the ear generates sounds, either spontaneously or in response to introduced test stimuli. OAEs are thought to reflect the function of cochlear outer hair cells, which contain contractile proteins that allow the cells to shorten or lengthen at a rapid frequency. Spontaneous OAEs are present in most normal ears at very low levels, and can occasionally be loud enough to be detected without amplification by the listener. 121 Evoked OAEs provide a sensitive early indicator of loss of auditory function, but only of the outer hair cells by definition.
The evoked OAE that has proven most useful in humans is the distortion product OAE (DPOAE). Two pure tones (f1 and f2, f2 > f1) are introduced into the ear canal and the resulting pure tone - the distortion product - is recorded at a frequency of 2f1-f2. The frequency span of the cochlea is tested by varying f1 and constraining the frequency ratio to f2/f1 = 1.21, a ratio proven to produce the strongest response. 122 A response to a given test frequency pair that falls below the noise threshold may indicate loss of function. DPoAEs are increasingly being used in the veterinary setting, especially when it is desired to know what audible frequencies may be affected.103,123,124
An alternate test is the transient evoked oAE (TEoAE), where a transient evoked response to a series of wideband clicks or chirps is recorded. DPoAEs evaluate a wider frequency range (above 10 kHz) than do TEoAEs, and might be preferred in species like the cat (or dog) with a higher frequency hearing range, albeit offer less sensitivity to minor and subclinical conditions. A failed oAE test typically mandates referral for BAER testing, so a lower instrument cost and briefer testing time may be offset by the need for further tests.
Middle ear and auditory tube function can be assessed using tympanometry (or impedance audiometry), which is a widely accepted and used technique in human medicine. This non-invasive method of examining the function of the middle ear involves varying the atmospheric pressure in the external ear canal and inferring the amount of sound energy that is transmitted through the tympanum by measuring the reflected sound energy.120,125,126 Pressure is typically varied from -400 to +200 daPa (decaPascals or mmH2o) while a continuous 226 Hz tone is presented, and the intensity of reflected sound is measured and plotted as a function of ear canal pressure. The resulting graph displays the compliance (or static acoustic impedance or admittance) of the tympanum. Variations from the normal response graph can indicate ossicle disarticulation, tympanum scarring or otosclerosis, middle ear fluid, tympanum rupture or auditory tube dysfunction.
Treatment approaches and limitations
The treatment approach is dictated by the form of deafness or mechanism responsible for the hearing loss.
Conductive hearing loss can usually be treated by mechanical (ear canal cleaning), surgical or antibiotic approaches. Full hearing recovery following otitis media may take a few weeks as the body clears the middle ear of debris.
Sensorineural deafness, whether due to genetics, aging, ototoxicity or noise, cannot be treated because no treatment modalities are available at present to restore lost hair cells. Current research suggests that this may be possible in the future.
Management of cats with hearing loss
Cats with unilateral deafness or partial hearing loss require no specific management, except that those with suspected hereditary deafness should not be used for breeding and those with acquired hearing loss should have the causative source removed or eliminated where possible.
With bilaterally deaf cats, the primary concern is protection from undetected dangers such as motor vehicles or predators.127,128 Preferably these cats should be kept as indoor pets since it can be difficult (although not impossible) 129 to constrain cats with yard fencing and hence to protect them from threats. Some deaf cats with outdoor privileges have been trained to return in response to flashing porch lights, but behavioral training is notoriously challenging in cats. The danger to infants and toddlers from reflex bites or scratches inflicted when a deaf cat is startled should be kept in mind.
The use of gesture communication, including canine obedience training signals, American Sign Language signs, and others, has been found to be effective in deaf dogs. 127 Deaf animals are naturally more visually attentive to humans, making them amenable to training in this form of communication. owners of deaf cats may, with patience, be able to train their pets with this system.
Key Points
The most common form of deafness in cats is congenital and hereditary, and associated with white pigmentation, especially in white cats with blue eyes.
Ototoxicity, frequently from aminoglycoside antibiotics like gentamicin, can be unpredictable and often results in total and irreversible deafness before the owner or veterinarian is aware of hearing loss.
Behavioral testing of hearing is often unreliable. The brainstem auditory evoked response (BAER) test is the most reliable assessment tool, but access to testing facilities is limited.
Sensorineural deafness is not currently treatable. Conduction deafness from obstructions of the outer or middle ear may be reversed.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.