
Abstract
Objectives
Subclinical bacteriuria (SB) is bacterial colonization of the urinary tract in the absence of clinical signs. The purposes of this study were to determine the prevalence of SB in cats and to describe results of the contemporaneous urinalysis. Secondarily, patient characteristics associated with SB were compared with those for cats without SB.
Methods
An electronic search identified all urine cultures performed on cats at a teaching hospital between 2009 and 2015. Results were subcategorized based on the presence or absence of lower urinary tract disease (LUTD) and SB-positive cases identified. The first control population was from samples without LUTD. The second control population was from all samples not identified as a SB-positive sample, including subclinical negative samples and those with LUTD. Five controls for each SB-positive sample were selected for both control groups. Medical records for all groups were reviewed.
Results
In all, 31/500 (6.2%) subclinical samples were positive. Most infections were a single organism (n = 27); four contained multiple organisms. Escherichia coli was the most common species (58%) followed by Enterococcus species (25%). Positive specimens were more likely to be from female cats (n = 24) vs male (n = 7; P = 0.0054). SB was strongly associated with bacteriuria (60% vs 6%; P <0.0001) and pyuria (67% vs 19%; P <0.0001). Positive specimens were significantly more likely to have an abnormal sediment examination (odds ratio 13.5, P <0.0001). When compared with all specimens including those with LUTD, SB was significantly associated with a lower urine specific gravity (1.022 vs 1.030; P = 0.0256) and presence of chronic kidney disease (68% vs 46%; P = 0.0168).
Conclusions and relevance
In this study, SB appears to be uncommon in cats and, in most cases, is associated with an abnormal urine sediment examination. Based on this study, there is little indication to perform a culture in a cat with no clinical signs of LUTD and an unremarkable sediment examination.
Introduction
Bacterial colonization of the urinary tract in the absence of clinical signs of urinary tract infection (UTI) is termed subclinical bacteriuria (SB). 1 There is currently limited and contradictory information regarding this finding in cats, with two recent studies reporting prevalence rates of 0.9% and 28.8%, respectively.2,3 In human medicine, SB is thought to be relatively common and is not routinely treated in non-pregnant and otherwise healthy individuals.4–9
Bacterial cystitis is thought to be relatively uncommon in cats compared with dogs and humans.10–13 This likely reflects more effective innate defenses, such as highly concentrated urine. 13 In studies of cats with clinical signs of lower urinary tract disease (LUTD) such as gross hematuria, stranguria, pollakiuria and periuria, bacterial infection rates range from 2–45%,10,12,14,15 with lower rates generally reported in younger, otherwise healthy cat populations. Various comorbid conditions such as increasing age, a previous perineal urethrostomy, 13 chronic kidney disease (CKD), 16 hyperthyroidism (HT) and diabetes mellitus (DM)14,17 have been associated with an increased risk of UTI, although the majority of these studies did not distinguish between symptomatic and asymptomatic cases.
A quantified urine culture (QUC) is routinely recommended for cats with recognized risk factors for UTI, such as CKD, DM and HT.14,17 There is currently little consensus regarding the prevalence of SB and appropriate treatment if SB is identified. The primary objectives of this study were to determine the prevalence of SB in cats evaluated at a veterinary teaching hospital, to report the associated bacterial isolates and to describe the findings on contemporaneous urinalysis. Secondarily, patient characteristics associated with SB were compared with those for cats without SB. We hypothesized that there would be a low prevalence of SB, that bacterial species would be similar to those identified in cats with LUTD and a positive QUC could be predicted by findings on urine microscopic sediment examination (MSE). It was also hypothesized that female sex, increasing age, CKD, HT and DM would increase the likelihood of SB in cats.
Materials and methods
An electronic medical record database was searched to identify QUCs performed on urine samples from cats admitted to the Veterinary Medical Teaching Hospital at Texas A&M University between 2009 and 2015. If multiple QUCs were performed on samples from the same patient during this time period, each result was considered separately. The associated visit summary was reviewed. Results of the QUC were excluded from further analysis if the culture was performed to assess the response to treatment for a previous UTI or if the QUC result was suggestive of contamination (ie, <1000 colony-forming units [CFU]/ml).1,13 Results were also excluded if a contemporaneous urinalysis was not available or if the medical record lacked sufficient information to determine the presence or absence of overt LUTD. LUTD was defined as the presence of dysuria, stranguria, pollakiuria or gross hematuria regardless of etiology (eg, infection, idiopathic, urolithiasis, neoplasia, etc). Identification of LUTD was primarily dependent on owner observations but was also influenced by abnormalities noted on physical examination such as overt discomfort associated with bladder palpation.
Figure 1 outlines the following groups. Results of QUCs meeting these initial inclusion criteria were then subcategorized based on the presence (LUTD+) or absence (LUTD–) of dysuria, stranguria, pollakiuria or gross hematuria at the time of sample collection. The LUTD– samples comprised the SB study group; those with a positive QUC were defined as SB+ and those with a negative QUC were defined as SB–. Patient age, sex, breed, contemporaneous urinalysis findings, serum creatinine concentration, recent glucocorticoid administration (ie, given within 2 weeks of urine sample collection) and specific concurrent diseases (ie, HT, DM and CKD) were recorded for each SB+ sample.

Case flow diagram indicating how the sample populations were identified for the groups. QUC = quantified urine culture; UTI = urinary tract infection; cfu = colony-forming units; LUTD = lower urinary tract disease; SB = subclinical bacteriuria
In order to identify risk factors and clinical pathological data associated with SB, two control populations were created by random selection, and the case information described above was extracted from the associated visit summary. The first control population (subclinical controls) was derived from the SB study group, with five SB– samples for each SB+ sample. The second control population was derived from all samples not in the SB+ group; that is, SB– and all LUTD+ samples. Again, five controls were randomly selected for each SB+ sample. This second control group was created to minimize potential bias associated with the SB study group and was defined as the combined controls.
Urine was routinely collected by cystocentesis and submitted in a plastic syringe or plain glass tube to the institution’s clinical pathology laboratory within the hour for analysis. Other methods of collection included spontaneously voiding or catheterization, at the discretion of the attending clinician. Urine specific gravity (USG) was measured via refractometry (ATAGO automatic and water-resistant refractometer), dipstick analysis was performed with Multistix 10SG (Multistix 10SG; Siemens Healthcare Diagnostics) and MSE was performed by trained laboratory technicians. Pyuria was defined as more than three leukocytes per high power field (HPF), and microscopic hematuria was defined as >10 erythrocytes/HPF. The presence of bacteria was confirmed using a modified Wright–Giemsa stain (Siemens) on an air-dried smear. 18 An abnormal MSE was defined as the presence of one or more of the following: pyuria, hematuria, bacteriuria.
Samples for culture were either submitted in a sterile syringe or plain-glass tube if plating was performed promptly, or placed in a boric acid tube (BD Vacutainer Plus C&S preservation tube; Becton Dickinson) if plating was delayed. A 10 μl aliquot of urine was plated on trypticase soy agar supplemented with 5% sheep’s blood (BAP) and MacConkey agar. The inoculated plates were incubated at 35ºC in atmospheric air (MacConkey) or air supplemented with 5% CO2 (BAP) for up to 5 days and inspected daily for growth. If there was growth, two BAP plates were inoculated at different concentrations (1:100 and 1:1000 dilutions) and bacterial concentrations recorded as CFU/ml were calculated.
All statistical analyses were undertaken using commercially available software (GraphPad Prism). The prevalence of UTI in each group was expressed as a percentage. Nominal data were evaluated with Fisher’s exact test. Normality of numerical data was determined with the D’Agostino and Pearson test. A t-test or Mann–Whitney test was used for parametric or non-parametric numerical data, respectively. In all circumstances, differences were considered significant if P values were ⩽0.05.
Results
In total, 940 urine specimens from 649 cats were cultured over the 6 year period (2009–2015). Of these, 184 were excluded for various reasons (122 specimens were collected to follow-up from a previous UTI, 35 had incomplete medical records and 27 had <1000 CFU/ml), resulting in a total of 756 samples in the initial study group. Of these, 256 were categorized as LUTD+ (Figure 1).
A total of 500 specimens from 368 cats met the inclusion criteria for the SB study group (ie, LUTD–). Of these, 31 (6.2%) specimens from 29 cats were positive on QUC; 469 were negative for bacterial growth. Of the 31 culture-positive samples, 19 were collected by cystocentesis, and three were voided samples; the method of collection was not reported for the remainder. A total of 36 bacterial isolates were reported, with a single organism infection in 27 specimens (87%) and multiple organisms identified in four. Twenty-three samples with 25 isolates had >100,000 CFU/ml. Table 1 shows the culture results. The most common isolate was Escherichia coli (n = 21) followed by Enterococcus species (n = 9) and Staphylococcus species (n = 2). The samples with polymicrobial infections all included E coli plus an Enterococcus species (n = 3) or Citrobacter species (n = 1). There were two cats that had positive cultures on separate occasions and both cultured the same isolate each time (E coli and Enterococcus species, respectively).
Quantified urine culture results and amount of growth (colony-forming units [CFU]/ml) from 31 samples from 29 cats with subclinical bacteriuria
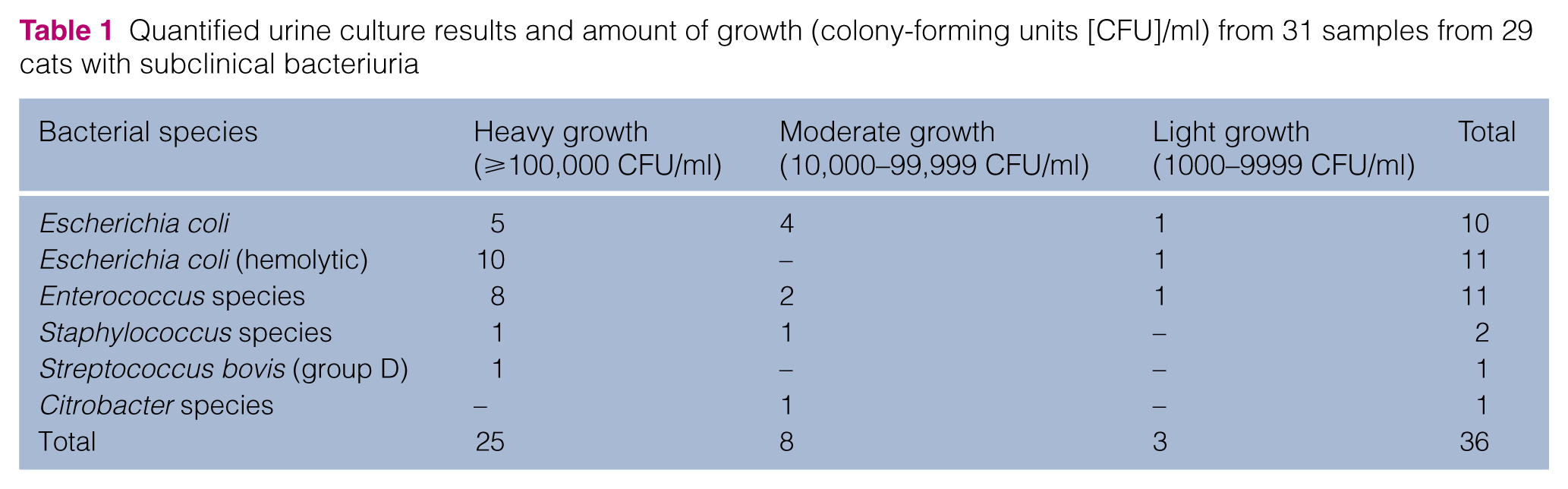
Table 2 shows the results of the contemporaneous urinalyses for the SB study group. Median USG was similar for SB+ specimens (1.022; range 1.008–1.060) and subclinical controls (1.024; range 1.008–1.068). The prevalence of proteinuria as determined by dipstick testing was also similar (84% vs 80%). Results of a MSE were available for 30/31 samples with a positive culture. Both pyuria (67% vs 19%; odds ratio [OR] 8.7, 95% confidence interval [CI] 3.7–20.5; P <0.0001) and bacteriuria (60% vs 6%; OR 24.3, 95% CI 9.0–65.7; P <0.0001) were strongly associated with a positive QUC; however, the likelihood of microscopic hematuria was similar for the SB+ samples and subclinical controls (33% vs 30%). Specimens with a positive QUC were substantially more likely to have an abnormal MSE (OR 13.5, 95% CI 3.9–45.5; P <0.0001). Only three samples with a positive QUC had an unremarkable MSE, giving this screening test a 97% negative predictive value for SB. These three samples all came from spayed female cats with various ages and clinical presentations, including a 16-year-old with acute progression of CKD, a 7-year-old with megacolon and a 5-year-old with acute vomiting and pyrexia.
Urinalysis results for specimens from cats with subclinical bacteriuria (SB+) and subclinical controls. Quantitative data are expressed as the median and range; qualitative information is expressed as a number and percentage

Data are n (%) unless otherwise stated
Microscopic sediment examination results were not available for one SB+ case, n = 30
The median age of cats in the SB study group was 13 years (range 1–23 years); median age for SB+ cases was similar to the subclinical control group (14 vs 13 years). Cats in the SB+ group were more likely to be female (77% vs 50%; P = 0.0054). A smaller body weight was also associated with a positive QUC (median 3.8 kg vs 4.44 kg; P = 0.0031). Serum creatinine concentrations, the presence or absence of HT, DM and CKD, and a history of recent glucocorticoid administration were not significantly different between the SB+ and subclinical control groups. Table 3 shows the demographic and clinical data of the SB+ cases and subclinical controls.
Demographic and clinical data for the subclinical bacteriuria cases, subclinical controls and combined controls

Quantitative data are expressed as the median and range; qualitative information is expressed as a number and percentage
Female sex compared with subclinical controls (P = 0.0054)
Weight compared with subclinical controls (P = 0.0031)
Reference interval 0.3–2 mg/dl
n = 154
n = 148
Presence of CKD compared with combined controls; P = 0.0168
n = 152
n = 147
CKD = chronic kidney disease; IRIS = International Renal Interest Society
The initial search identified 256 specimens from cats with LUTD. Of these, 46 (18.0%) were culture positive from 45 cats with a total of 54 isolates. There were 38 single organism infections and eight polymicrobial infections. The most common bacterial isolate was E coli (n = 23; 42.5%) followed by Enterococcus species (n = 11; 20.4%) and Staphylococcus species (n = 11; 20.4%). Table 4 shows QUC results for the specimens from cats with signs of LUTD.
Culture results and amount of growth (colony-forming units [CFU]/ml) from 46 urine samples from cats with lower urinary tract disease

Demographic and clinicopathological findings for the SB+ group were compared with the combined control group (Table 3). The median ages were similar (14 vs 11 years; P = 0.066). The SB+ specimens had a significantly lower median USG than the combined control group (1.022 vs 1.030; P = 0.0256). Although mean serum creatinine concentrations were similar for the SB+ and combined control group (1.79 vs 1.89 mg/dl [reference interval 0.3–2 mg/dl]; P = 0.7899), SB was significantly associated with CKD; of the 31 SB+ cases, 20 samples (64.5%) were from cats with CKD vs 70/153 (45.8%) of the combined control specimens (P = 0.0168). Similar numbers of cats in the SB+ and combined control groups had concurrent DM, HT or were receiving glucocorticoids.
Discussion
This study suggests that SB is relatively uncommon in cats, with a prevalence of 6.2% in feline patients evaluated at a veterinary teaching hospital. This result sits between the previous studies describing feline SB with prevalence rates of 0.9–28.8%. The stark contrast in these two rates likely reflects patient population differences, as one study evaluated healthy cats in Norway with a median age of 4 years (0.9% prevalence), 2 whereas the other study (28.8% prevalence) evaluated an older population of Australian cats with a median age of 14 years and various concurrent disorders. 3 The median age of the cats in our SB study group was 13 years, and 73% had recognized risk factors for UTI, namely CKD,19,20 HT 17 and DM. 14 It is therefore somewhat surprising that the prevalence of SB in our study was substantially lower than that reported in similarly aged Australian cats. This may reflect unrecognized differences in sample handling or in the selection of patients for QUC. Additionally, regional influences or variations in bacterial virulence could also play a role.
The bacterial isolates identified in this study are similar to those found in previous reports of feline UTIs.3,13,21,22 Gram-negative species, predominately E coli, were commonly identified, followed by Enterococcus and Staphylococcus species. The species identified in specimens from cats with SB were similar to those found in cats with LUTD. In humans with UTIs, strain differences and their associated virulence factors are thought to influence the likelihood of developing associated clinical signs. E coli is responsible for over 80% of both SB and symptomatic UTI in humans.5,23 However, type 1 and P fimbriae, found predominantly in uropathogenic E coli, lead to cytokine production and subsequent cystitis; these strains are more frequently identified in patients with overt clinical signs of lower urinary tract inflammation.6,8,24 It is possible that similar associations between strain, virulence factors and host response occur in feline patients. Litster et al explored this possibility by classifying the E coli strains isolated from cats with SB into phylogenetic groups, and found that 82.4% belonged to group B2, the most common for extra-intestinal pathogenic E coli. 3 This phylogenetic group shares virulence factors with strains associated with human UTI, but apparently colonizes the feline urinary tract without routinely causing signs of LUTD. It has been hypothesized that virulence factors found in uropathogenic E coli are required for survival within the harsh environment of the feline bladder but do not trigger the same inflammatory response in cats as they do in people. Further studies are needed to elucidate the interactions between bacterial species and host that determine clinical symptomology in this species.
As hypothesized, findings on the MSE were helpful in predicting the outcome of the QUC, with pyuria and bacteriuria strongly predictive of a positive result. This finding supports previous studies of feline SB that showed a significant association between urinary leukocyte counts and a positive QUC.13,19,20 However, pyuria alone has been shown in previous studies to be an inconsistent finding in infected urine; 22 this was confirmed in our study, as pyuria was not reported in 10/31 (33%) of the SB+ samples. The utility of the MSE as a diagnostic tool increased when pyuria, hematuria and bacteriuria were evaluated together as an active or inactive MSE. An inactive MSE (defined as the absence of pyuria, hematuria and bacteriuria) had a negative predictive value of 97%, suggesting that this is an excellent screening tool for SB in cats. Our findings suggest that QUC is of questionable value in a cat without signs of LUTD and an inactive MSE.
Females were over-represented in the SB+ group; this finding matches previous studies in both cats and humans.3,5,20,25 This is likely due to an increased risk of ascending infection related to differences in urethral anatomy and its closer proximity to the anus. The impact of sex likely explains the difference in median body weight for the SB+ and subclinical control cats. Further differences between these two groups, such as USG, patient age, concurrent diseases or steroid usage, were not identified. This could be a type II error due to inherent selection bias: the decision to perform a QUC was made by the attending clinician and was probably influenced by the presence of risk factors for UTI such as HT, CKD and DM.14,17,19,20 Consequently, most of the QUCs performed on asymptomatic cats came from patients with recognized risk factors; this may have confounded our ability to identify true predispositions for feline SB.
To minimize this selection bias, a combined control population was created, irrespective of the presence or absence of LUTD. Comparisons between the SB+ cases and this wider control group showed that SB+ samples were more likely to come from cats with a lower USG and concurrent CKD. These findings echo previous studies, where it has been postulated that cats with CKD have compromised lower urinary tract defense mechanisms.17,19,20 This study did not reveal differences between the SB+ group and the combined control population with regard to age, or concurrent HT, DM or steroid administration. It is possible that these are not risk factors for SB in cats, although it seems more likely that our efforts to mitigate selection bias had only limited effects. A prospective study in which a QUC is performed on every cat examined at the teaching hospital would be necessary to determine fully the risk factors for SB in this species.
The presence and management of subclinical bacteriuria have been extensively studied in people; however, there is limited research available in the veterinary field. Subclinical bacteriuria in cats appears to be associated with decreased host defenses or increased pathogen virulence factors.3,13 There is currently no consensus on the management of these patients or if treatment is necessary. In human medicine, treatment is not associated with a difference in outcome and not recommended in otherwise healthy individuals.4,5,9 A recent abstract followed 67 cats over 3 years and found no difference in survival between cats with untreated SB and cats that did not develop SB. 16 This supports the theory that SB may not require antimicrobial treatment; however, the current study did not evaluate this hypothesis. Additional, prospective, studies are indicated to determine the benefits (if any) of treatment for SB.
The major limitations of this study pertain to its retrospective nature. Information regarding methods of urine collection was inconsistently recorded, and sample storage and handling prior to plating was variable. Samples were often submitted to the clinical pathology and microbiology laboratories immediately after collection. However, there were occasional delays in submission and some urine was held overnight in urine transport tubes prior to submission for QUC. A recent study using canine urine showed that storage method, time and temperature could affect bacterial colony counts. 26 Any variation in handling of specimens may have resulted in either fewer positive or fewer negative cultures and affected the results. It is possible that a delay in plating for samples with low bacterial numbers could have resulted in a falsely negative QUC. Additionally, the authors had to rely on contemporaneous medical records to determine the presence or absence of LUTD. It seems unlikely that dysuria or pollakiuria would be overlooked or not recorded, but we were unable to verify specifically the clinical status of every cat. These signs were also primarily based on owner observations which may have led to some inaccuracies. There is also substantial selection bias in the cases included in the SB study group, as the decision to perform a QUC was probably driven by a perception of increased risk of UTI in that individual cat.
Conclusions
Subclinical bacteriuria appears to be relatively uncommon in cats evaluated at this veterinary teaching hospital and is extremely unlikely in the absence of bacteriuria, pyuria and/or hematuria on MSE. These results suggest that the decision to culture the urine of a cat without clinical signs of LUTD and an unremarkable MSE should be considered on a case-by-case basis and may not be routinely necessary. Further studies are needed to determine the clinical significance of SB in cats.
Footnotes
Acknowledgements
We thank Geoff Fosgate BSc, DVM, PhD, DipACVPM, Deparatment of Production Animal Studies, Faculty of Veterinary Science, Onderstepoort, South Africa for his assistance with in the statistical analysis.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.