
Abstract
Objectives
Bronchial lumen to pulmonary artery diameter (BA) ratio has been utilized to investigate pulmonary pathology on high-resolution CT images. Diseases affecting both the bronchi and pulmonary arteries render the BA ratio less useful. The purpose of the study was to establish bronchial lumen diameter to vertebral body diameter (BV) and pulmonary artery diameter to vertebral body diameter (AV) ratios in normal cats.
Methods
Using high-resolution CT images, 16 sets of measurements (sixth thoracic vertebral body [mid-body], each lobar bronchi and companion pulmonary artery diameter) were acquired from young adult female cats and 41 sets from pubertal female cats.
Results
Young adult and pubertal cat BV ratios were not statistically different from each other in any lung lobe. Significant differences between individual lung lobe BV ratios were noted on combined age group analysis. Caudal lung lobe AV ratios were significantly different between young adult and pubertal cats. All other lung lobe AV ratios were not significantly different. Caudal lung lobe AV ratios were significantly different from all other lung lobes but not from each other in both the young adult and pubertal cats.
Conclusions and relevance
BV ratio reference intervals determined for individual lung lobes could be applied to both young adult and pubertal cats. Separate AV ratios for individual lung lobes would be required for young adult and pubertal cats. These ratios should allow more accurate evaluation of cats with concurrent bronchial and pulmonary arterial disease.
Introduction
The evaluation of bronchial lumen to pulmonary artery diameter (BA) ratio from high-resolution CT images has been utilized successfully in human and veterinary medicine for detection of bronchiectasis.1,2 Conditions associated with an increase in BA ratio include bronchiectasis, aging and altitude.1–5 Increases in the pulmonary artery to bronchus ratio (ABR), a similar yet inverted ratio, have been reported with pulmonary hypertension. 6 Asthma has been reported as a cause of both increased and decreased BA ratio depending on chronicity.1,7 The BA ratio would be potentially unsuitable to evaluate bronchial lumen size in conditions that result in changes to both the bronchus and pulmonary artery (eg, feline heartworm-associated respiratory disease and parasitic lung disease) or when concurrent conditions affecting these structures exist (eg, bronchiectasis and pulmonary hypertension). Therefore, we propose that comparison of bronchial and pulmonary artery diameter with a fixed structure within the thoracic cavity, such as a vertebral body, might provide more reliable assessment of bronchial lumen and pulmonary artery diameter in complex cases. The purpose of the study was to establish the bronchial lumen to vertebral body diameter (BV) ratio and pulmonary artery to vertebral body diameter (AV) ratio in normal cats.
Materials and methods
Previously acquired CT images from 41 specific pathogen-free cats were included in the study. Cats were normal as evaluated by physical examination, thoracic radiographs and complete blood count. Eleven cats had serial CT images available, resulting in these cats having multiple studies over time available for interpretation; five of these cats had images that spanned both the pubertal and young adult age groups. In total, 41 sets of measurements were studied from pubertal cats (6–10 months), and 16 sets of measurements were studied from young adult cats (>12 months). 8 Cats were 7-month-old to 2-year-old female intact domestic shorthairs. Body weight ranged from 1.5–4.8 kg. The studies had the approval of the Auburn University Institutional Animal Care and Use Committee, and cats were housed in an Association of Assessment and Accreditation of Laboratory Animal Care (AAALAC)-approved facility.
Thoracic CT images were acquired with a helical single detector row CT unit (CT/i scanner, General Electric Co, Milwaukee, WI) with cats positioned in sternal recumbency. The entire lung field was imaged with 5 mm collimated transverse images and 1 mm transverse images acquired with a detail algorithm. All CT exams were performed with 120 kV peak tube voltage and 80–120 mAs tube current. The 5 mm collimated study used a pitch of 1.3 with a 512 × 512 matrix and a 1 s tube rotation time for a total scan time of 28.7 s. The 1 mm transverse study was obtained with a pitch of 1.5, 512 × 512 matrix and a 1 s tube rotation time with an averagescan time of 64.7 s. Non-ionic intravenous contrast (Isovue-370; Bracco Diagnostics) was administered (92 mgI/kg) and the study was repeated after a 25 s delay for post-contrast image acquisition. All contrast was given via hand injection. A previously published standardized anesthetic protocol was utilized. 9 Cats were premedicated with intramuscular injection of ketamine hydrochloride (Fort Dodge Animal Health), butorphanol tartrate (Fort Dodge Animal Health), and dexmedetomidine hydrochloride (Pfizer Animal Health). After endotracheal intubation, general anesthesia was maintained with isoflurane administered through a Bainnon-rebreathing system. A single-breath hold technique (airway pressure maintained at 14–15 cm of water) was utilized during thoracic CT image acquisition.
Images were reviewed using a dedicated image viewing station and commercially available software (eFilm 3.3 Merge Healthcare). Measurements were recorded using the embedded caliper tool (measurement tool-line) by the same investigator (TLF). Repeat measurements were acquired to compare consistency by the same investigator (TLF) and inter-observer variation by another investigator (RC). Vertebral body height measurements were acquired mid-body at T6 using a bone window (WW 2500; WL 480; Figure 1). All measurements were obtained with the vertebral body in the center of the image field to reduce parallax error. All bronchial lumen and pulmonary artery diameter measurements were taken using a lung window (WW 1500; WL 600). Internal diameter of the bronchial lumen and pulmonary artery diameter were measured for each lung lobe using the 1 mm high-resolution scan whenever possible. The cranial subsegment of the left cranial lung lobe and right cranial lung lobe were measured at the T4–T5 intervertebral disc space. The caudal subsegment of the left cranial lung lobe and right middle lung lobe were measured at the level of the T6–T7 intervertebral disc space, and the left and right caudal lung lobes measurements were obtained at the T9–T10 intervertebral disc space (Figure 2). The exact location was chosen when the artery and bronchi could be clearly defined and may necessitate moving one slice cranial or caudal to the prescribed location. The accessory lung lobe was not evaluated due to inconsistency of clear identification of a measurable bronchus and pulmonary artery in all cats. BV ratios and AV ratios were calculated.

CT image of a normal young adult cat with measurement of the vertebral body
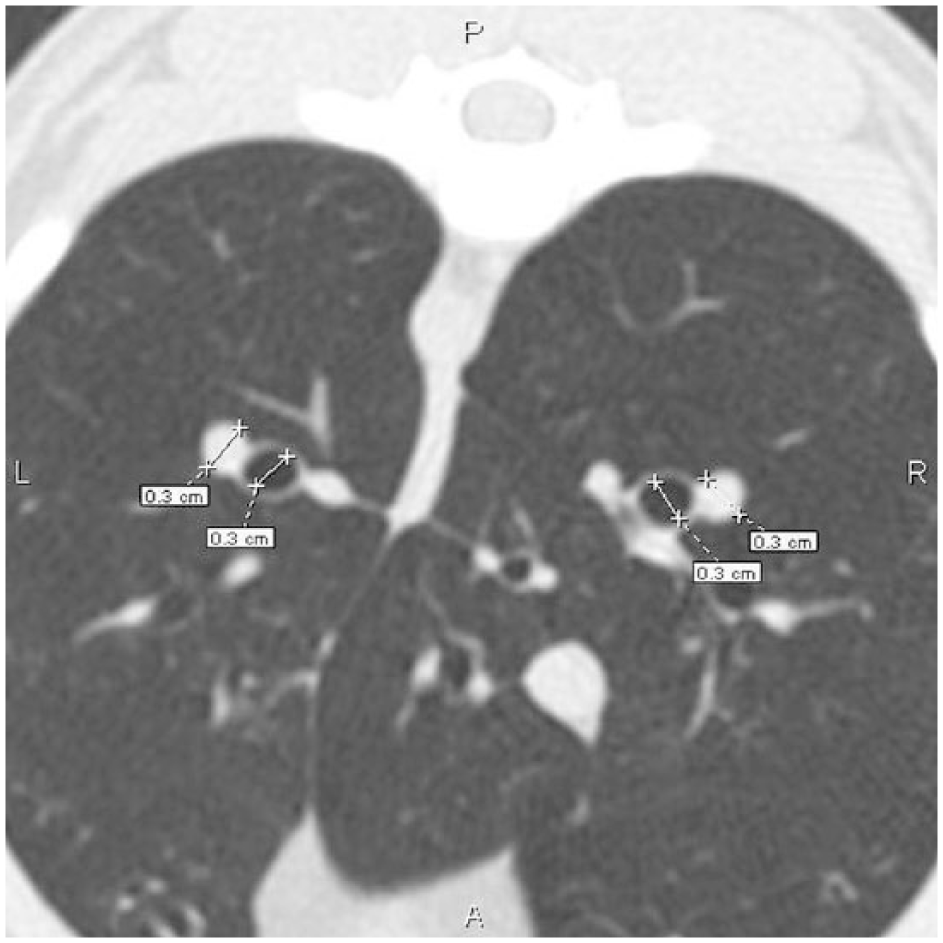
CT image of a normal young adult cat with measurement of right and left caudal lobe pulmonary arteries and bronchi
The mean and SD of the AV and BV ratios of young adult cats and pubertal cats were calculated. Mean BV and AV ratios with a range of 2 SDs would include 99% of all normal cats studied, and reference intervals were established in this manner. Comparisons between young adult and pubertal cat AV and BV ratios utilized a Mann–Whitney Rank Sum test. A Kruskal–Wallis One Way ANOVA on Ranks compared combined age group BV ratios between individual lung lobes, lung lobe AV ratios of young adult cats and lung lobe AV ratios of pubertal cats. A Mann–Whitney Rank Sum test was used to compare vertebral body diameter between young adult cats and pubertal cats, arterial diameter in the caudal lung lobes between young adult and pubertal cats, repeated measures with one observer and independent observer repeated measures with two observers. A statistical software package (Sigma Plot 12.0, Systat Software Inc, San Jose, CA) was utilized with statistical significance set at P <0.05.
Results
Repeated measures by a single observer (TLF) did not reveal a significant difference in any measurements or ratios. Independent observer repeated measures with two observers (TLF and RC) revealed a significant difference in the right cranial bronchus measurement (P = 0.034) and right cranial BV ratio (P = 0.029). However, no difference was detected in any other measurements or ratios.
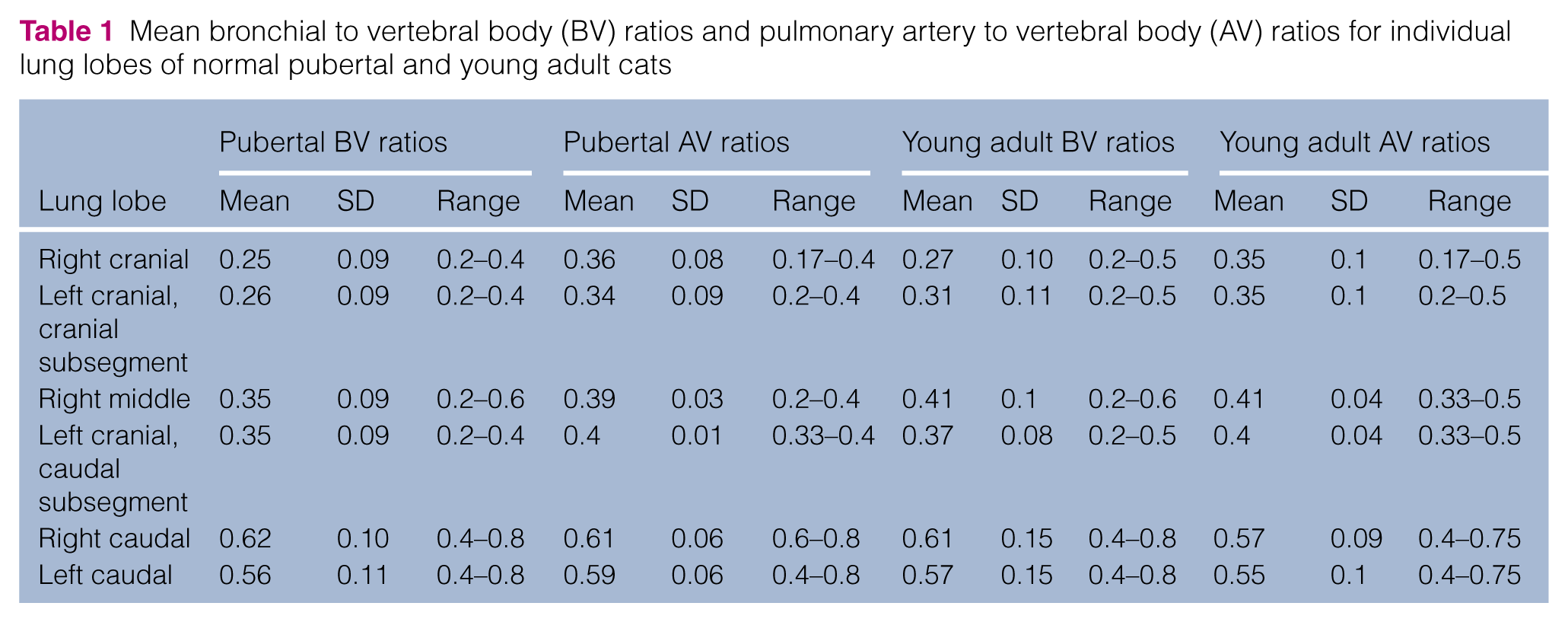
Normal mean BV and AV ratios were determined for each lung lobe for pubertal and young adult cats (Table 1). No significant difference was noted in BV ratios between pubertal and young adult cats in any lung lobe. Further, BV ratio analysis was completed by combining these age groups. Combined age group analysis of BV ratios revealed a significant difference between lung lobes (P <0.001; Figure 3). Therefore, BV reference intervals were established accordingly (Table 2). Only the left and right caudal lung lobe AV ratios demonstrated a significant difference between young adult and pubertal cats (right caudal P = 0.038; left caudal P = 0.028; Figure 4). No significant difference was noted in vertebral body diameter between young adult and pubertal cats (P = 0.616); however, there was a significant difference inpulmonary artery diameter between young adult(left = 0.29 ± 0.03; right = 0.28 ± 0.04) and pubertal cats (left = 0.31 ± 0.03; right = 0.3 ± 0.03) in both the left and right caudal lung lobes (left lobe, P = 0.026; right lobe,P = 0.026). In both young adults and pubertal cats, the left and right caudal lung lobe AV ratios were significantly different from all other lung lobes (P <0.001) but not from each other (Figure 2). No significant differences were detected between all other lung lobes. Reference intervals for AV ratios were established for pubertal (Table 3) and young adult (Table 4) cats, accounting for differences noted between lobes.
Mean bronchial to vertebral body (BV) ratios and pulmonary artery to vertebral body (AV) ratios for individual lung lobes of normal pubertal and young adult cats
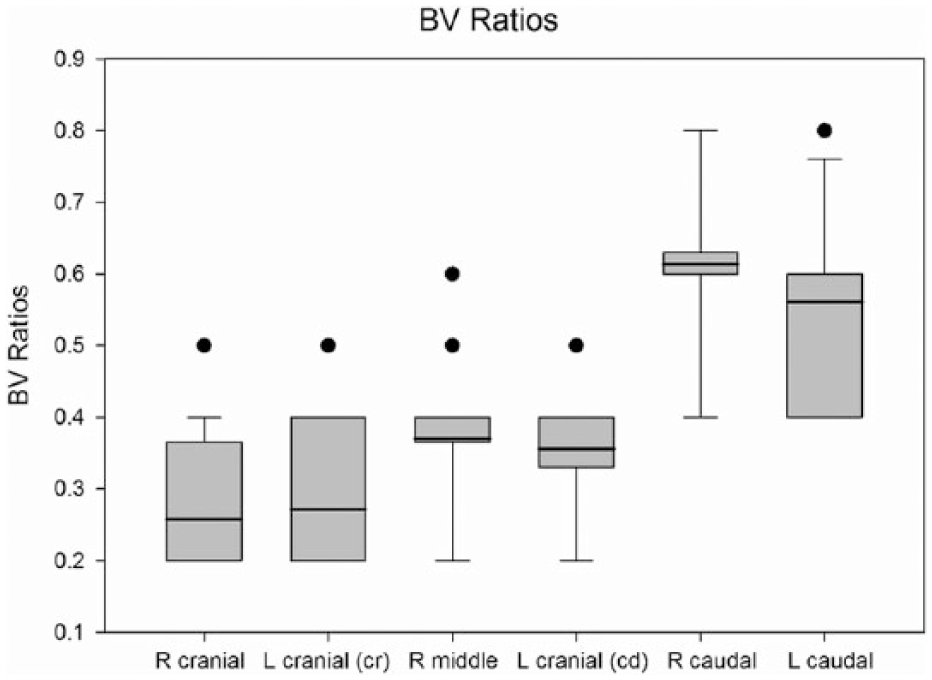
Combined bronchial to vertebral body (BV) ratios of normal cats. Significant difference in mean BV ratio was noted between pairs of lung lobes. R = right; L = left
Combined mean bronchial to vertebral body (BV) ratios, SD and suggested reference intervals
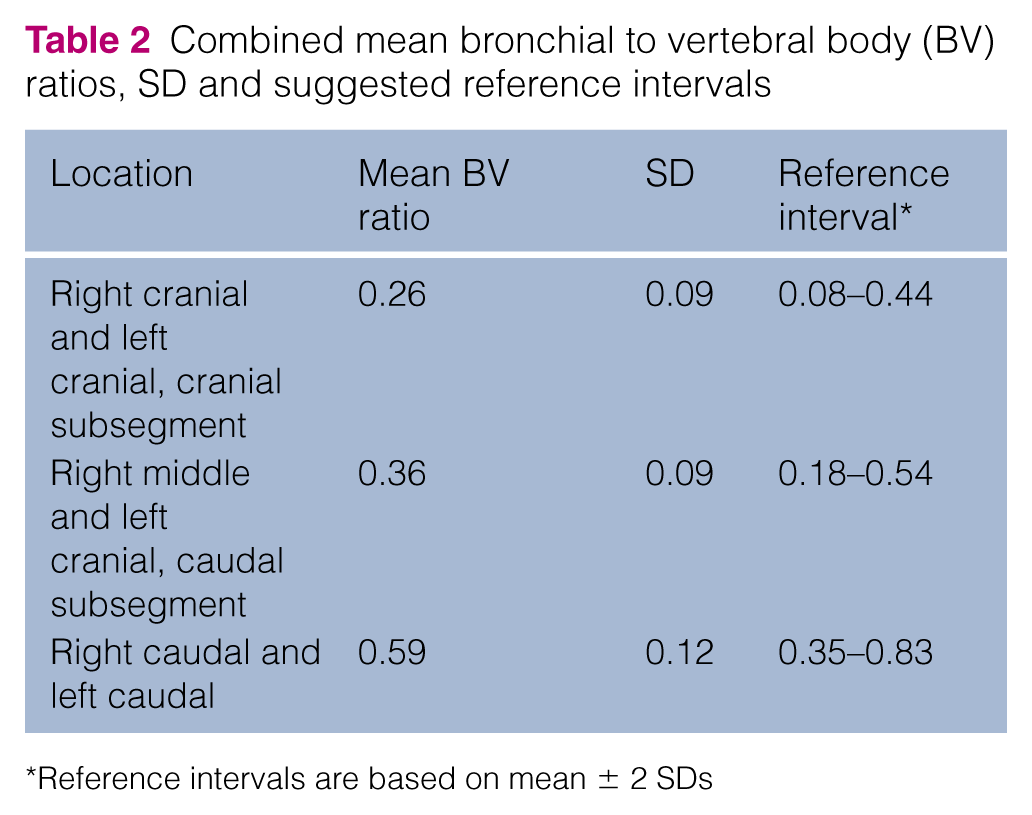
Reference intervals are based on mean ± 2 SDs

Pulmonary artery to vertebral body (AV) ratios of normal cats. (a) AV ratios for young adult cats, (b) AV ratios for pubertal cats. The mean caudal lung lobe AV ratios were significantly different for the caudal lung lobes compared with all other lobes. Mean AV ratios were significantly different in caudal lung lobes of young adults compared with pubertal cats. R = right; L = left
Combined mean pulmonary artery to vertebral body (AV) ratio, SD and suggested reference intervals for pubertal cats

Reference intervals are based on mean ± 2 SDs
Combined mean pulmonary artery to vertebral body (AV) ratio, SD and suggested reference intervals for young adult cats

Reference intervals are based on mean ± 2 SDs
Discussion
Vertebral body diameter measurement is a consistent variable in cats >7 months of age. The predictability of vertebral size provided a unit of comparison for the denominator for BV and AV ratios. Clinically significant variability was not noted on repeat measurements performed by the same or multiple investigators. Similar BV measurements were found between the two age groups that were evaluated, suggesting that one set of reference intervals can be established for cats >7 months. Differences observed in BV ratios between the cranial lung lobes, the middle and caudal subsegment of the left cranial lobes and the caudal lobes suggest that different reference intervals should be considered for each pair of lobes. A single set of AV ratio reference intervals can be established for the cranial lung lobes, right middle lobe and caudal subsegment of the left cranial lobe inclusive of both age groups. The caudal lobes require a separate reference interval from other lobes as well as between age groups. Reference intervals presented in this study could be utilized to evaluate changes in bronchial and pulmonary artery diameter with high-resolution CT images independent of one another. This could be useful in patients with concurrent diseases that affect both bronchi and pulmonary vasculature.
Earlier studies have described the BA ratio in dogs and cats without pulmonary disease,9,10 and this ratio was shown to be significantly larger in dogs with bronchiectasis. 2 The BA ratio and ABR have been utilized in human medicine to evaluate images from patients with bronchiectasis, asthma, chronic pulmonary embolism, pulmonary hypertension and congestive heart failure.1,6,7,11,12 Utilization of the ABR in the study evaluating pulmonary hypertension presents the relationship between the arterial and bronchial measurements slightly differently than the BA ratio; however, the study found that the sensitivity of the ABR for detecting pulmonary hypertension was decreased in patients with lung disease, specifically those with bronchiectasis. Aging in people is also shown to increase the BA ratio.3,4 This has not been evaluated in geriatric dogs and cats, but this could be a concern in geriatric patients with concurrent arterial or airway disease. For these reasons, we have evaluated a bronchus to vertebral body ratio and artery to vertebral body ratio. The comparison of each element with a consistent parameter allows for independent comparison that would be useful in these complex scenarios. Utilizing a standardized location of a single vertebral body diameter allows for a consistent variable within the ratio with which all other measurements can be compared. Results of this study are supportive of the vertebral body diameter measured mid-body at T6 being a stable and repeatable variable.
Repeat measurements by a single observer revealed good agreement between measurements. The difference in the right cranial bronchus measurement between two observers did not exceed two SDs, and therefore this is unlikely to be clinically significant. In addition, the measurement calipers in the viewing software rounds to the nearest 0.1 mm. This could result in a slight difference between observers. The authors compared measurements using this tool with handheld electronic calipers (data not shown), and there was no significant difference noted in the resultant ratios. Therefore, we elected to use the viewing software calipers to better reflect what is routinely clinically available and convenient.
In comparison with the BA ratio, which obtains measurements from paired structures at the same level for each measurement, it was demonstrated in the present study that BV and AV ratios result in differences between lobes of the lungs. Although this was observed in both the BV and AV ratios, significant differences were observed between all three pairs of lobes in the BV ratio and only in the caudal lobe AV ratios in comparison with all other lobes. It appears that the bronchial diameter varies more with lung lobe than does the arterial diameter. Arterial diameter within the caudal lobes is larger compared with other anatomically smaller lung lobes. As would be expected considering the relative anatomical symmetry of the lung lobes, there was no difference noted between right and left lobes of similar orientation (ie, right cranial/cranial segment of left cranial; right middle/caudal segment of left cranial; right caudal/left caudal).
A difference between AV ratios of young adult and pubertal cats was another intriguing finding in our study. Further evaluation of this indicated that while there was no significant difference in vertebral body diameter, the pulmonary arteries were slightly larger in the pubertal age group. It is important to recall that only five cats had serial images measured that spanned both the pubertal and young adult cat age groups; therefore, this could represent simple variation within the population. One study has demonstrated an effect of aging on the BA ratio in people, but this study involved young adult subjects. 3 There is limited information regarding bronchial and arterial measurements in children. One study evaluating pediatric patients found that the BA ratio was lower in childrenwhen compared with the standard ratio of >1. 13 The authors focused on the BA ratio and did not provide information about the component measurements in comparison with young adults. The effect of age on bronchial or pulmonary artery diameter has not been described in cats. To investigate this further, repeated measurements of the AV ratio in a large population of the same cats over time would be needed.
Utilization of serial CT images obtained from the same cat at different time points could be a potential limitation in this study as outliers could disproportionally skew the data. Clinical validation of these data for other breeds, male cats and cats less than 7 months ofage could identify potential diversity of these ratios. Measurements in the present study were acquired utilizing the anesthetic and ventilation techniques established for BA ratio reference intervals in cats. 9 Significant differences were identified between full inspiratory and expiratory images for the canine BA ratio. 14 The same data were collected during fixed pressure inspiration and differences would be expected for the airways at end expiration. Lastly, the inability to obtain repeat measurements in a large number of the same cats over time as they aged limits our ability to evaluate change in pulmonary artery size and better determine if aging played a role in pulmonary artery diameter differences.
Conclusions
The vertebral body diameter is a stable variable for which to compare bronchial and pulmonary artery diameter. Clinically significant intra-observer or inter-observer variability of the BV and AV ratios was not noted, demonstrating that these are reliable ratios. Reference intervals suggested allow for application of this technique to animals with complex pulmonary disease affecting both the airways and pulmonary arteries. Further investigation of these ratios in the diseased lung may allow for determination of a more defined cut-off range.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.