
Abstract
Practical relevance:
The ability to perform a complete eye examination in the cat is critically important for patients with an ocular disorder or a systemic disease, as well as for the geriatric cat.
Clinical challenges:
Cats may need short breaks between portions of the eye exam in order to minimize stress. For the clinician, use of ophthalmic equipment and interpretation of normal vs abnormal findings may take some practice in order to develop proficiency.
Audience:
This review is aimed at veterinary practitioners and outlines all the steps and equipment necessary to perform a complete ophthalmic examination in the cat.
Equipment:
Although some specialized equipment is required, a complete eye exam can be performed with a modest investment in equipment and supplies.
Evidence base:
This article draws on published references for normal parameters measured in the feline eye exam, as well as the experience of the authors.

Proficiency in performing an eye examination in the cat is critical for the patient presented with ocular disease, as well as for the patient that may have a systemic disorder. Although veterinary ophthalmologists use specialized equipment, a thorough eye exam can be performed with relatively simple equipment (Figure 1). Practice leads to proficiency, especially when performing fundic examinations.

Basic equipment needed for an ophthalmic exam (clockwise from top left): Optivisor loupe (x 3.5 magnification at 4 inches), 20 diopter indirect lens, direct ophthalmoscope and Finoff transilluminator
Vision and neuro-ophthalmic tests
Assessing vision in the cat can sometimes be more difficult than in the dog. Cats tend not to move around a strange room as a dog might, making assessments of visual behavior more tenuous.


The best assessment of a cat’s vision comes from the results of multiple tests.
Adnexal and anterior segment examination
The adnexa consists of the eyelids, third eyelid and conjunctiva. The anterior segment includes the cornea, anterior chamber, iris, ciliary body (which cannot be visualized) and lens. All of these structures (other than the ciliary body) can be adequately examined with a transilluminator, an Optivisor loupe (x 3.5 magnification at 4 inches) and a direct ophthalmoscope set on the slit beam. A slit lamp biomicroscope is the ideal instrument for anterior segment examination but is typically only utilized by ophthalmologists.

The anterior chamber depth can be evaluated with the slit beam and one eye compared with the other. A shallow anterior chamber with a normal cornea and iris may indicate lens instability or aqueous misdirection syndrome. In the latter, aqueous humor is abnormally diverted into the vitreous body, resulting in vitreous expansion which causes the lens and iris to be displaced anteriorly. This condition often leads to glaucoma. By contrast, a shallow anterior chamber with a corneal wound may indicate a perforated, leaking eye.

Examination of the anterior chamber for aqueous flare using the slit beam of the direct ophthalmoscope and an Optivisor for magnification


The major arterial circle (arrow), located in the iris, is a large vessel varying in prominence from cat to cat
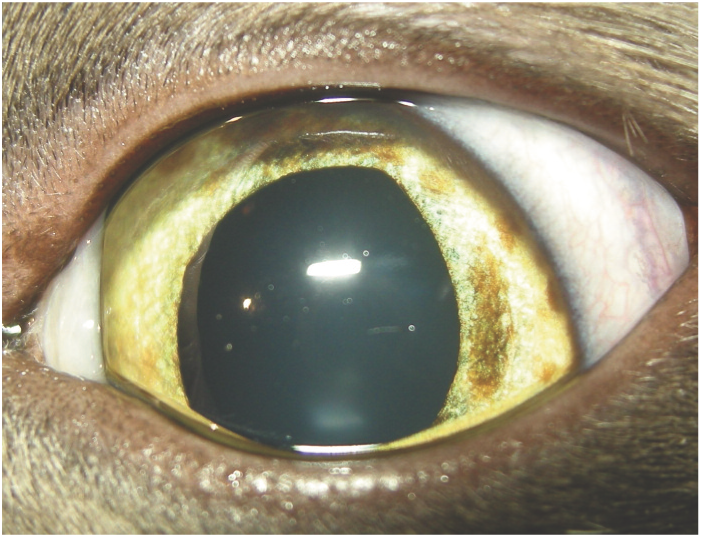
The edge or equator of the lens is not visible in a normal eye. If the edge of the lens is visible, along with an aphakic crescent, the lens is subluxated. A fully luxated lens will tend to fall either into the anterior chamber, where it is easy to visualize, or posteriorly into the vitreous cavity. If the lens appears not to be present, it is likely in the ventral-most portion of the vitreous cavity.

Rubeosis iridis, or neovascularization on the iris surface, in a cat with chronic uveitis. Courtesy of Michigan State University Ophthalmology Service
Iris melanosis. Note the individual areas of hyperpigmentation that are flat with the iris surface

Iris melanoma, a potentially life-threatening neoplasm. Note the extensive hyperpigmentation with areas raised from the iris surface
Schirmer tear test
The Schirmer tear test (STT) involves placing the test strip in the lower conjunctival sac for 60 seconds and measuring the amount of wetting in millimeters during this time. This test assesses only the aqueous portion of tears, and not the lipid or mucin component. Normal STT values for cats range from 7–34 mm/min.3,4

Keratoconjunctivitis sicca (KCS) is uncommon in cats compared with dogs. In fact, excess tearing is a more frequent clinical finding and thus the STT can often be omitted from the eye exam in a cat without losing vital information.
If the STT is performed, it must be prior to placing any fluid on the ocular surface. It has previously been speculated that stress in cats can increase sympathetic tone, causing a temporary decrease in tear production.3,5 However, a more recent study of normal cats did not substantiate this. 4 Instead, this study suggested that an STT <9 mm/min is consistent with KCS, and no normal cat was found to have an STT <7 mm/min. It was also found that cats that were stressed actually seemed to wet the STT paper more rapidly. 4
Due to variability among cats, a low STT value must be interpreted carefully. Low STT values must be found in conjunction with clinical signs such as corneal ulceration, lusterless cornea and mucoid discharge before making a diagnosis of KCS.

Tonometry
Tonometry is a non-invasive diagnostic tool commonly used to approximate the intraocular pressure (IOP). Accurate estimations of IOP play an essential role in diagnosing glaucoma (high IOP) as well as helping to confirm acute uveitis (low IOP). The normal range of IOP in cats is 12–19 mmHg. There is a normal circadian rhythm to IOP, with the highest values occurring at night. 7

There are two types of tonometers in general use in practice today – applanation and rebound tonometers; the most common examples being the Tono-Pen and the TonoVet, respectively (Figures 7 and 8). These instruments differ in the way they obtain an estimation of IOP. Applanation tonometry measures the force needed to flatten an area of the cornea with the instrument’s footplate. In comparison, rebound tonometry measures the probe deceleration as it is propelled from the instrument, contacts the cornea and returns.8,9 One study in cats comparing these two indirect measuring devices with the gold standard of manometry, reported that the readings of the TonoVet were closer to the true IOP than those of the Tono-Pen, especially at IOPs above 20 mmHg. 10

The Tono-Pen applanation tonometer works by flattening the cornea with the instrument’s footplate

The TonoVet rebound tonometer works by measuring the speed with which the probe returns to the instrument following contact with the cornea
Regardless of the method used to assess IOP, it is important to ensure that pressure is not being placed around the cat’s neck or on the globes as the eyelids are held open. Restraint under the chin and behind the head will help to prevent movement of the cat without affecting the IOP. A topical anesthetic must be used when utilizing applanation tonometry, but is not necessary for rebound tonometry due to the short contact time between the probe and the cornea.
The most important thing when checking patients over time is to utilize the same measuring device so that trends in IOP are more easily assessed. 11
Collection of cytology sample
See box on page 707.
Fluorescein staining
Fluorescein is a water-soluble dye and is thus absorbed by hydrophilic tissue (corneal and conjunctival stroma) but not by lipophilic tissue (conjunctival and corneal epithelium and Descemet’s membrane).
Placing a drop of topical anesthetic on the eye and waiting 30 s before fluorescein staining will make the cat more tolerant of rinsing. Because the fluorescein strips are highly concentrated, only a small drop of eye wash is needed to partially wet the strip. While retracting the upper lid, touch the wetted fluorescein strip to the bulbar conjunctiva rather than to the cornea itself. Allow the patient to blink, which distributes the dye across the surface of the cornea. Rinse excess stain from the cornea with eye wash.
Any exposed corneal stroma (indicating loss of corneal epithelium) will absorb fluorescein. If a deep ulcer with no stain uptake at its base is present, this is most likely a descemetocele. If aqueous humor mixed with fluorescein is seen running from the surface of a cornea with an ulcer this would be considered a positive Seidel test and indicates a corneal perforation. The cobalt blue filter on the direct ophthalmoscope along with a source of magnification should be used for enhanced visualization of small areas of fluorescein uptake.
Fluorescein can also be utilized to assess patency of the nasolacrimal system. For this assessment, a large amount of stain is placed on the ocular surface, but not rinsed, and then the nares are observed for appearance of the dye. This test is known as the fluorescein passage or Jones test. In cats, the time it takes for fluorescein to reach the nares is quite variable, typically ranging from a few seconds to a few minutes. One study reported a range of 4–1800 s. 13 Some cats may also have a nasolacrimal duct opening into the oral cavity. Therefore, it is important to observe the oropharynx for dye if fluorescein is not observed at the cat’s nares.

Microbrushes are ideal for collecting ocular surface samples for cytology
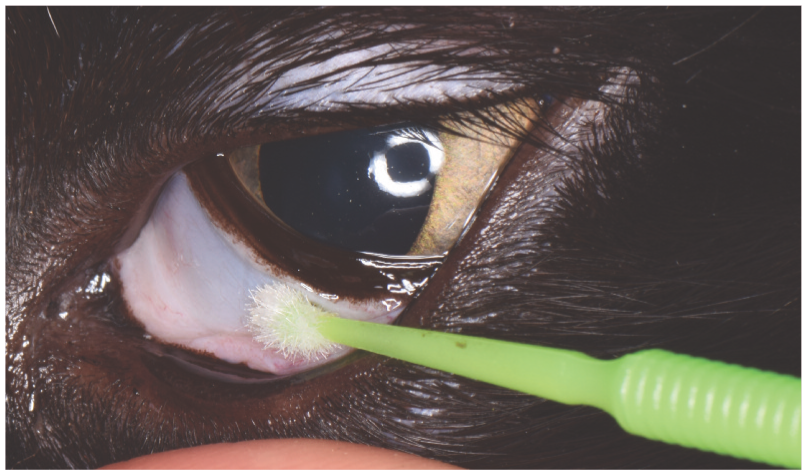
The Microbrush should be rolled firmly across the conjunctiva or cornea several times. The brush is then rolled on a glass slide to transfer the cells

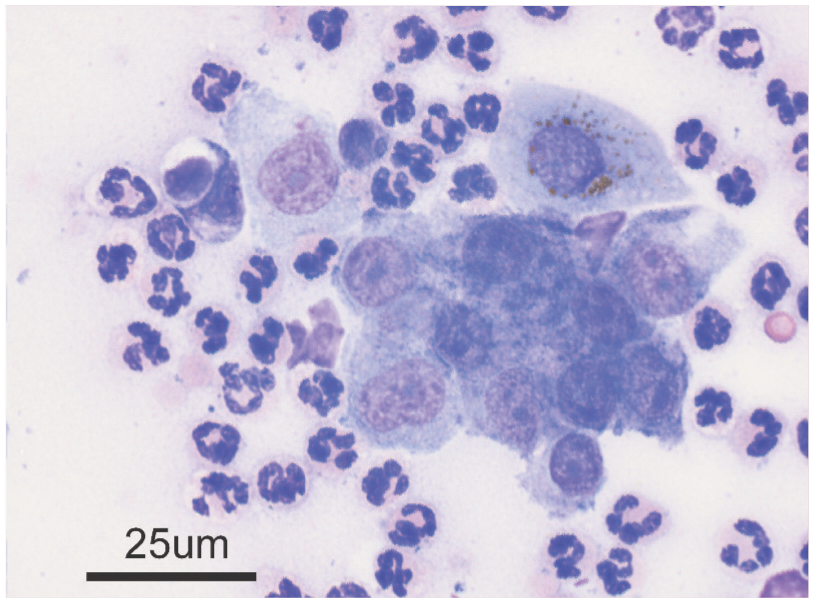
Cytologic preparation from a kitten with conjunctivitis. Purulent inflammation is present as well as a cytoplasmic inclusion body within an epithelial cell (arrow), consistent with Chlamydia felis. Wright’s stain, x 100

Cytologic preparation from a cat with a raised pinkish-white plaque and corneal vascularization. Purulent inflammation with eosinophils (arrow) and a mast cell (arrowhead) is present, confirming eosinophilic keratitis. Wright’s stain
Cytologic preparation from a cat with conjunctivitis. Purulent inflammation is present, a finding consistent with, but not diagnostic for, herpesvirus infection. Wright’s stain

Fundic examination
Fundic examination is critically important in geriatric cats or any cat with systemic illness. The fundus can be examined by direct or indirect ophthalmoscopy. While a standard direct ophthalmoscope produces an image that is right side up, it is magnified approximately x 15 and provides only a 5° angle view, making visualization of the entire fundus difficult. Conversely, indirect ophthalmoscopy produces an image that is upside down and inverted but with a magnification of only about x 3, making visualization of large portions of the fundus possible. Intermediate between the two is the Welch Allyn Panoptic direct ophthalmoscope which provides a 25° upright image view.
Several technical aspects of indirect ophthalmoscopy are important to appreciate in order to obtain the best view of the fundus. Indirect lenses are biconvex although the curvature of each side is different. The flatter side (usually marked by a silver ring on the rim) should always be positioned towards the patient. A transilluminator should be held next to the observer’s eye. To start, rest the hand holding the lens gently on the cat’s head with the lens pointed away from the eye. Attain the best tapetal reflection possible, then drop the lens into place to observe the fundus (Figure 14). The observer’s eye, the light beam, the lens and the cat’s eye should all be in a straight line. The indirect lens should be held with the observer’s arm fully extended (do not bend the elbow and lean forward).

Indirect ophthalmoscopy using a Finoff transilluminator and a 20 diopter indirect lens
The lens needs to be at the correct distance from the cornea, so that the image of the fundus entirely fills the lens. If eyelids or iris are seen within the lens, then the lens is too close (usually) or too far from the cornea. An assistant looking from the side can help the examiner learn correct placement by indicating when the light spot on the cornea is very small and focused (correct focal point).


Note the dorsal tapetal and ventral melanotic portions in the normal feline fundus. The optic disc is non-myelinated and has three main arteriole–venule pairs extending from it, along with a few other small vessels

Normal fundus in a blueeyed, color-dilute cat. No tapetum or pigment is present, allowing Visualization of choroidal vasculature and sclera in addition to retinal blood vessels
A cat will tend to retract its globe when a very bright light is shone into the eye. This leads to elevation of the third eyelid and loss of the fundic image. The examiner should stop, let the cat relax and try again. This is mitigated to some extent by using light of just sufficient brightness to provide a good image and avoiding excessive illumination. Another helpful maneuver in some cats is to have an assistant hold the cat toward the edge of the table, as often this prompts it to lift its eyes such that the third eyelid retracts.

Multifocal small retinal hemorrhages in a cat with systemic hypertension and hypertensive retinopathy
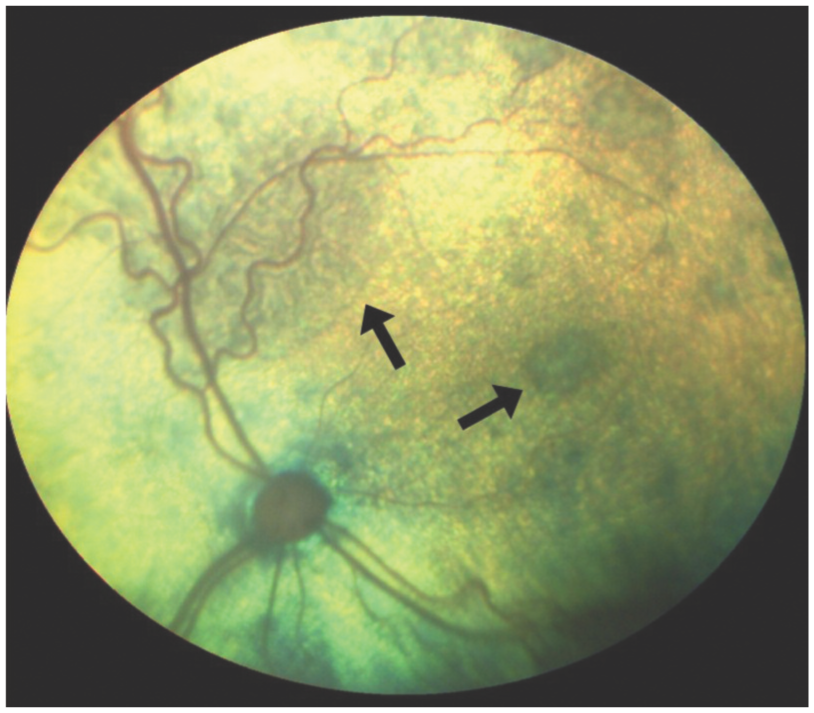
Multifocal areas of intra- and subretinal fluid accumulation (arrows) in a cat with systemic hypertension and hypertensive retinopathy

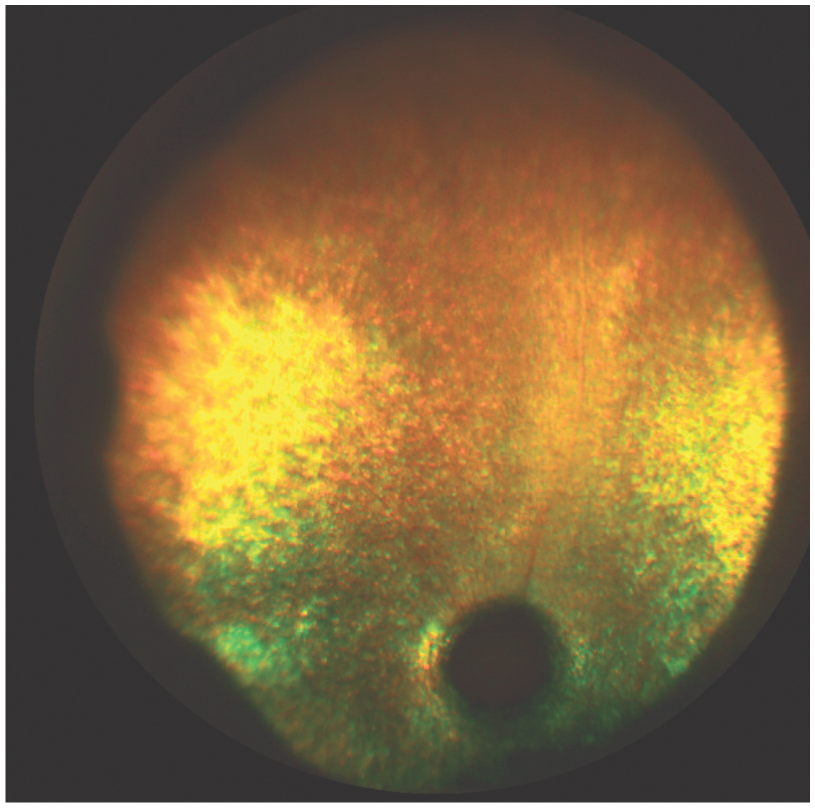
Large areas of hemorrhage within the retina and in the vitreous in a cat with systemic hypertension and hypertensive retinopathy

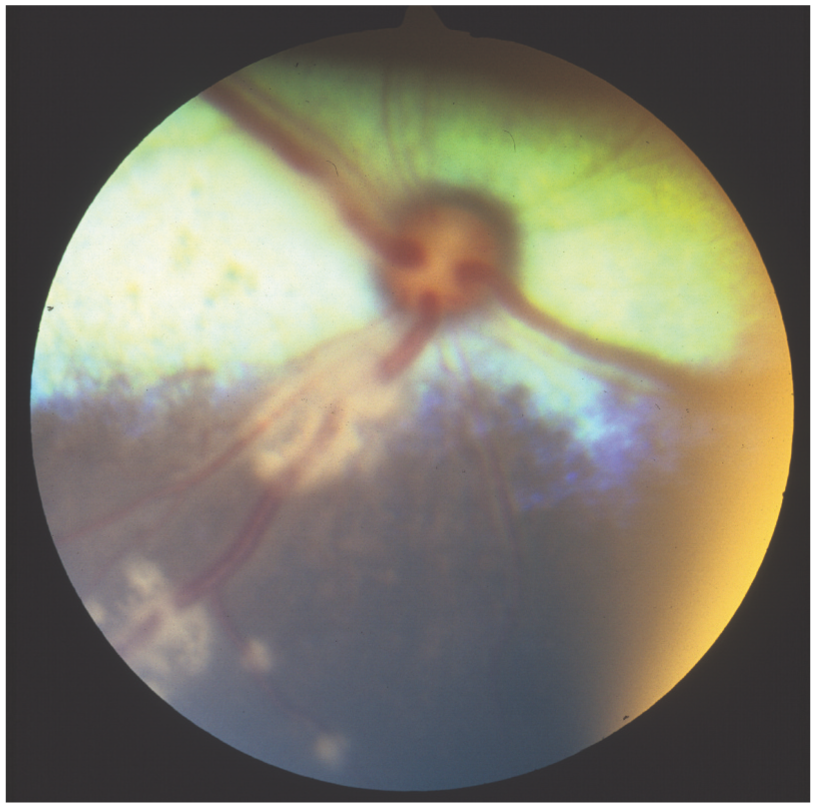
Complete serous retinal detachment in a cat with systemic hypertension and hypertensive retinopathy. Note that no hemorrhages are present in this cat
Advanced retinal degeneration in a cat. Note the tapetal hyperreflectivity, loss of retinal blood vessels and optic nerve degeneration
Retinal vasculitis in a cat with feline infectious peritonitis. Note the perivascular cuffing of inflammatory cells

Focal chorioretinitis (arrow) in a cat with cryptococcosis
Any patient in which chorioretinitis is identified should undergo a thorough systemic work-up in an attempt to determine an underlying cause.
Key points
A complete eye exam is critical for the cat presented for ocular disease or a systemic illness.
Many normal cats will have a weak menace response and poor visual placing. The cotton ball test often elicits the best visual response.
When performing tonometry it is important that no pressure is placed on the cat’s neck or on the globes when holding open the eyelids.
Hypertensive retinopathy is the most common cause of vision loss in older cats.
Fundic examination should be performed on every geriatric cat, regardless of the reason for the veterinary visit. Early signs of hypertensive retinopathy may be identified before the cat goes blind.
It takes practice to master the technique of indirect fundic examination, as well as to distinguish normal and abnormal findings.
Footnotes
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.