
Abstract
Objectives
Heartworm-associated respiratory disease (HARD) is a recently recognised pathological manifestation in cats caused by Dirofilaria immitis exposure. This study aimed to estimate the percentage of cats at risk of developing HARD in a heartworm-endemic area (Taipei, Taiwan), and to test the correlation of heartworm exposure and the presence of lower airway/lung clinical signs (LA/L signs).
Methods
This was a prospective case-control study. The study design called for the enrolment of at least 80 cats with LA/L signs and at least 80 cats without such clinical signs in a 1 year period. The D immitis antibody seroprevalence of the two cohorts was compared.
Results
From February 2014 to January 2015, 187 client-owned cats were prospectively enrolled: 83 clinical cases with LA/L signs and 104 cats without such signs. Antibody seropositivity was approximately twice as frequent in cats with LA/L signs (13.3%) than in cats without signs (7.8%) (odds ratio [OR] 1.814); nevertheless, no statistically significant difference between the two cohorts (P = 0.22) was found. We used 41 frozen samples from free-roaming cats to examine the possibility of different exposure rates to mosquito bites between client-owned cats and stray cats, finding the seroprevalence to be 7.5% in free-roaming cats – a result not statistically different to that in client-owned cats (P = 0.60). Outdoor access was a significant risk factor for heartworm exposure in client-owned cats (OR 3.748; P = 0.03); however, living entirely indoors did not provide complete protection from exposure/infection.
Conclusions and relevance
Our results did not show statistically significant differences in antibody seroprevalence between cats with and without LA/L signs. LA/L signs were not always present under conditions of natural exposure. However, exposure to D immitis is not rare among client-owned cats, suggesting that heartworm prophylactics should be a part of routine care in all cats living in areas endemic for canine heartworm.
Introduction
Clinically, heartworm disease (HWD) is seen much less frequently in cats than in dogs. Cats are thought to be more naturally resistant to heartworm infection because of the commonly found low worm burden or failure of mature worm development in cats exposed to Dirofilaria immitis.1–4 However, a previous necropsy study of shelter cats showed that pathological changes in the pulmonary arteries could be present with heartworm exposure, even when lacking adult heartworms in the heart and lungs. 5 An experimental model revealed that cats inoculated with heartworm can develop a pulmonary parenchymal and airway pathology with the arrival of immature worms at 70–90 days postinfection. 6 As a result, the term ‘heartworm-associated respiratory disease (HARD)’ has come to describe cats with the presence of lung histological and radiographic lesions, with corresponding clinical findings, despite the lack of adult heartworms existence.1,7–9 The clinical signs associated with HARD include laboured breathing, chronic coughing and tachypnoea,2,3,9 similar to many other common respiratory diseases, such as feline asthma.10,11
Taiwan has long been recognised as a heartworm-endemic endemic area, with a reported canine heartworm infection prevalence of 13–57% in different studies of dog populations.12,13 During the period 2011–2013, D immitis antibody status was examined in 27 chronic coughing cats in Taiwan by some of the authors of this study (C-H L, H-J T, OF H); only one case was positive. Furthermore, some of these cats received bronchoalveolar lavage, and all the cases with lower airway eosinophilic inflammation showed negative results for the D immitis antibody test. These observations raise some questions. First, from a clinical point of view, what is the prevalence of clinically identifiable HARD in cats presenting for lower airway/lung clinical signs (LA/L signs) in a canine heartworm endemic area? Is the seroprevalence of D immitis antibody higher in cats with LA/L signs than in cats without the associated signs?
To answer these questions, we designed the present study to include cats with possible differential diagnoses including HARD in a heartworm-endemic area. Our objectives were to estimate the percentage of cats at risk of developing HARD in a canine heartworm-endemic area, and to test the correlation of heartworm exposure and the presence of LA/L signs.
Materials and methods
Two cohorts of client-owned cats with and without clinical signs of coughing, open-mouth breathing or laboured breathing (LA/L signs) were recruited. The study design called for a prospective enrolment of at least 80 cats with LA/L signs and at least 80 cats without such clinical signs during a 1 year period (February 2014 to January 2015). The cases were collected from five sources: one veterinary teaching hospital that was receiving referral cases from all areas and four private veterinary hospitals in different administrative districts in Taipei. The exclusion criteria were cats <6 months of age and those having received monthly heartworm preventive medication in the 6 months before enrolment. Attending veterinarians acquired information about the signalment, clinical condition, lifestyle and environmental status of each case. Serum or plasma samples were collected to test circulating IgG antibodies against D immitis, using an in-house lateral flow immunoassay kit (Solo Step FH, Feline Heartworm Antibody Test Kit; Heska). The test was performed either immediately after blood collection or frozen for later evaluation. Samples were frozen based on the manufacturer’s instructions, being refrigerated for up to 72 h or stored at or below −20°C for longer storage.
Different exposure rates to mosquito feeding may exist between client-owned cats and stray cats. Thus, we planned to test at least 40 frozen samples from free-roaming cats of a previous epidemiological study on the influenza virus in Taiwan in 2013. Samples were tested for antibody against D immitis, allowing an estimate of seroprevalence in stray cats.
Statistical analysis
Gaussian distributions were assessed with the Shapiro–Wilk test. The seroprevalence of antibodies against D immitis was reported with descriptive statistics. The χ 2 test was used to examine the statistical difference in antibody seroprevalence between different cohorts. Logistic regression analysis was used to examine the relationships between antibody seropositivity and multiple risk factors, obtained through published epidemiological studies and case reports. The odds ratio (OR) was calculated to represent the magnitude of the association between antibody seropositivity and individual risk factor. Statistical software (SPSS Statistics 19.0.0; IBM) was used for all analyses, and the level of statistical significance was defined as P <0.05.
Results
A total of 228 samples were tested for antibody against D immitis during the 1 year study period; this included samples from 187 client-owned cats and 41 free-roaming cats. The client-owned cats (n = 187) included 125 domestic shorthairs, 25 Persians, 10 American Shorthairs, 10 Persian crosses, four Scottish Fold crosses, two Russian Blues, two Siamese, two Scottish Folds, two Himalayan crosses, one British Shorthair, one domestic longhair, one Exotic Shorthair, one American Shorthair-cross and one Siamese cross. The median age of the client-owned cats was 8.0 years (interquartile range [IQR] 3.1–12.0 years). Median body weight was 4.4 kg (IQR 3.6–5.5 kg), and the median nine-point body condition score was 5 (IQR 4–7). 14 Ninety-four of the cats were male (70/94 were neutered) and 93 were female (85/93 were neutered). The exact ages, body weights, detailed clinical conditions and presence of LA/L signs were unknown for the 41 free-roaming cats included in the study.
The results of the D immitis antibody test and the comparisons of seroprevalence between the different cohorts are listed in Table 1. Two cases were excluded because of invalid results. Sixty-three of the client-owned cats had a D immitis in-house antigen test; all results were negative. We observed cats with LA/L signs for D immitis exposure vs absence of D immitis exposure; the OR was 1.814 (95% confidence interval 0.694–4.742).
Dirofilaria immitis antibody seroprevalence in the cats of the present study
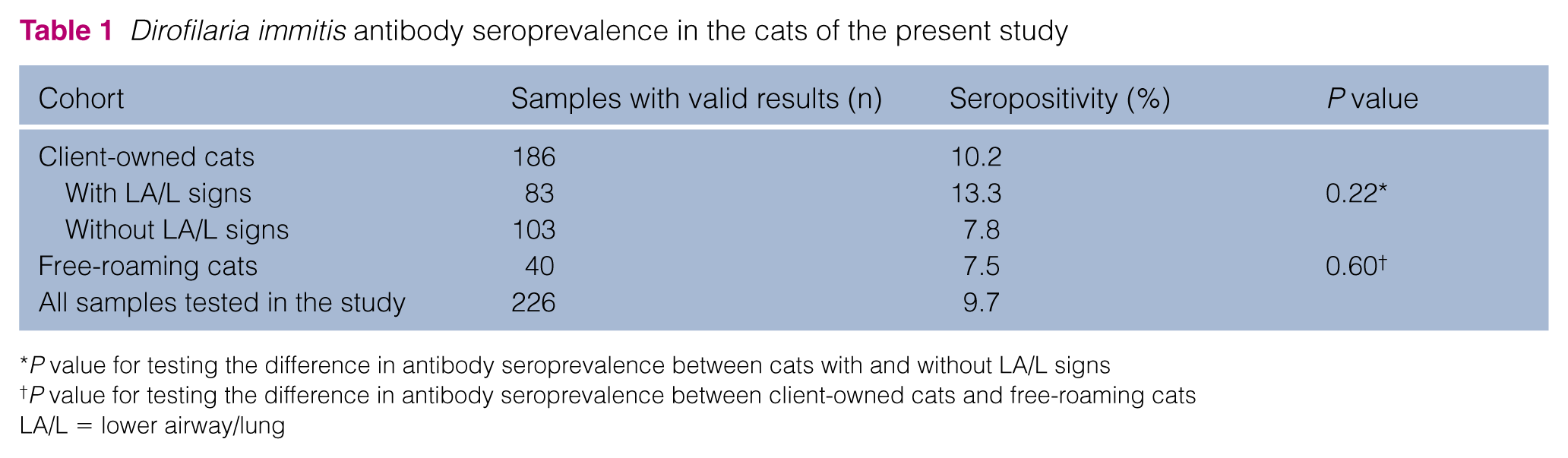
P value for testing the difference in antibody seroprevalence between cats with and without LA/L signs
P value for testing the difference in antibody seroprevalence between client-owned cats and free-roaming cats
LA/L = lower airway/lung
Among all client-owned cats, 17.8% lived with dogs and 11.9% had outdoor access (this included absolute outdoor and mixed indoor/outdoor lifestyle). Among client-owned cats showing LA/L signs, the clinical signs observed by the owners included coughing (89.2%), open-mouth breathing (22.9%), laboured breathing (21.7%), vomiting (18.1%), diarrhoea (3.6%) and syncope (2.4%). Table 2 shows the results of our multiple logistic regression model for the risk factors of D immitis antibody seropositivity. After adjusting for the effects of age, sex, presence of a dog, laboured breathing and vomiting, we found cats with outdoor access to be 3.748 times more likely to have D immitis antibody seropositivity than cats living exclusively indoors (P = 0.031).
Results of multiple logistic regression on potential risk factors for Dirofilaria immitis antibody seropositivity in the present study

OR = odds ratio; CI = confidence interval
Discussion
This study showed client-owned cats with evidence of exposure to D immitis to be 1.814 times more likely to have LA/L signs than cats without exposure to D immitis. Exposure to D immitis does not necessarily confirm the diagnosis of HARD. Heartworm-exposed status may, however, be used as a rough estimate for the possible risk of HARD in a cat population. 1 In our study, the cats with LA/L signs were, indeed, nearly twice as likely to be antibody seropositive. However, the difference between cats with and without LA/L signs in antibody seropositivity was found not to be statistically significant. If HARD was easily and commonly induced in naturally exposed cats, the antibody seroprevalence should be significantly higher in cats with LA/L signs compared with cats without LA/L signs in a heartworm-endemic area. Nevertheless, the results of our study did not support this hypothesis, implying HARD may not be frequently seen in clinical cases.
In heartworm-endemic regions, the seroprevalence of antibodies against D immitis in cats has been reported to be in the range of 2.8–33%.2,15–19 The overall antibody seropositivity was 10.2% in our client-owned cats, representing exposure to D immitis without the regular use of heartworm-preventive medications. Cats that are naturally exposed to D immitis may not necessarily develop lung pathology, but clinically the evidence of antibody presence would increase the suspicion of HARD in cats with LA/L signs. The threat of developing HARD exists in exposed cats. There are diagnostic challenges because of the lack of a gold standard for the confirmatory diagnosis of HARD in clinical cats. Airway eosinophilia found on bronchoalveolar lavage is not specific for HARD,10,20 and a more invasive procedure, such as lung histopathological evaluation, 21 is not generally acceptable for client-owned cats. Abnormalities in bronchial reactivity and pulmonary function have been reported both in vitro and in vivo in cats with HARD.7–9 Some authors believe that the findings of LA/L signs in antibody-positive cats, without other disease and without evidence of mature HWD, allows a provisional diagnosis of HARD. 1 The best method for differentiating asthma, the most likely of the differential diagnoses, is still unclear. Because of difficulties in diagnosis and the potential risk of developing HARD and HWD, the best strategy is to pursue heartworm preventives in all cats residing in canine heartworm endemic regions.
Outdoor access was a significant risk factor for D immitis antibody seropositivity in our investigation, a result similar to the findings of other studies.15,18,19 However, the seroprevalence in the free-roaming cat population was not higher than in client-owned cats, a result of note. One previous study cited high average and median ages for heartworm-infected cats, indicating that the risk of infection might be higher if a cat lives longer in a risk area. 22 We expect the life span of these free-roaming cats from relatively rural areas of Taiwan to be shorter than client-owned cats that are well cared for, and this might reduce the chance of exposure. Furthermore, many client-owned indoor cats in our study still developed D immitis antibody seropositivity, as found in previous studies.15,19,23 Although a lifestyle with outdoor access can significantly increase the risk of heartworm exposure in cats, living entirely indoors did not provide adequate protection from exposure.
This study has limitations. First, the statistical power of the study was limited owing to the relatively small number of cats enrolled. Therefore, a real difference in antibody seropositivity between cats with and without LA/L signs might have gone undetected. Second, heartworm-exposed status can be underestimated with the use of D immitis antibody seroprevalence. All of the following factors can contribute to an underestimation of heartworm exposure in cats: undergoing an antibody test <60 days postinfection; failure to develop antibodies after exposure; having an insufficient amount of detectable IgG antibody; and becoming antibody negative over time.2,3,7,17,23–25 Third, the risk of HARD can be overestimated based on antibody seropositivity. Owing to the risk or concerns over cost, not all cats with a positive antibody result received bronchoalveolar lavage to prove an eosinophilic inflammation. Furthermore, an airway eosinophilia is not capable of making the diagnosis of HARD, as cats with concurrent feline asthma or Toxocara cati infection also show eosinophilic inflammation in the lower airway.10,11,20
Conclusions
Through the screening of antibody seropositivity as an estimation of heartworm-exposed status, exposure to D immitis was approximately twice as frequent in cats with LA/L signs (13.3%) as in cats without these signs (7.8%). However, the difference in seropositivity between cats with and without LA/L signs did not reach statistical significance. LA/L signs were not always present under conditions of natural exposure. Although the differences between HARD and various eosinophilic airway/lung diseases have not yet been fully elucidated in clinical cases, HARD can be prevented with monthly heartworm prophylactics. Based on a 1 year seroprevalence of D immitis antibodies of 10.2% in client-owned cats, a regular heartworm prophylactic plan as part of routine healthcare should be advocated in cats living in areas endemic for canine heartworm.
Footnotes
Acknowledgements
We thank Professor Ching-Ho Wang for sample size consultation; Dr Chung-Ling Liu for her effort to make the antibody test routinely available at the National Taiwan University Veterinary Hospital; biostatistician We-Ting Hung for statistical consultation; Dr Hui-Ting Lin for the handling of samples from the free-roaming cats; and veterinary student Shih-Jung Yen for help with sample collection. We also appreciate all of the dedicated cats owners who pursue better feline health in Taiwan.
Conflict of interest
Within the past 3 years, Chung-Hui Lin, Pei-Ying Lo, Han-Ju Tsai and Olivia F Hsieh have received lecture fees and/or royalties from Zoetis Taiwan, manufacturers of heartworm preventives; however, Zoetis Taiwan did not involve or provide financial support for any part of the present study. The other authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.