
Abstract
Objectives
The aim of the study was to evaluate the prevalence, size, location and appearance of mineralisations in feline stifle joints, and to evaluate their relationship with osteoarthritis and cranial cruciate ligament (CrCL) status.
Methods
Presence or absence, and size of mineralisations were determined from lateral stifle radiographs of 25 cats with CrCL rupture, and 44 cat cadavers without CrCL rupture. Mineralisations were classified as small, medium or large. Prevalence was compared between the clinically affected cats and the cadavers; the cadaver group was subdivided into an age-matched and an older group. Ten stifles with varying sizes of mineralisations were prepared as whole-knee specimens for histopathology. Location and appearance of the mineralisations, and degenerative changes in the cruciate ligaments, menisci, articular cartilage and joint capsule are described.
Results
Prevalence of articular mineralisations was 0.76 in stifles of cats with CrCL rupture (mean ± SD age 8.6 ± 4.5 years), 0.64 in stifles of age-matched cat cadavers and 0.74 in older cat cadavers (mean ± SD age 17.0 ± 2.4 years). Cats with CrCL rupture had a higher percentage of medium and large mineralisations than cats without CrCL rupture. Microscopically, small mineralisations were calcifications usually located in the cranial horn of the medial meniscus. Larger mineralisations were found to be ossifications, commonly located in the joint capsule and fat pad. Cats with larger mineralisations showed more signs of osteoarthritis, including degenerative changes in the CrCL.
Conclusions and relevance
Mineralisations in feline stifle joints were found to differ in size, appearance and location. Small mineralisations were usually confined to the medial meniscus, as described previously; larger mineralisations tended to be located in the tissues cranial to the menisci and seemed to be associated with osteoarthritis and CrCL pathology. Large mineralisations in feline stifles are ossifications in periarticular tissue and are associated with degenerative joint disease.
Introduction
Mineralisations in the cranial aspect of the stifle joint are a common radiographic finding in domestic cats. 1 They have been observed to be located within the cranial horn of the medial meniscus and are therefore referred to as meniscal mineralisations.1–3 Microscopically, two basically different appearances have been described. Whereas some mineralisations are calcifications or chondroosseus metaplasia with no organised bone structure,1,2 others are ossifications consisting of organised cancellous bone.1–3 The pathogenesis and clinical significance of meniscal mineralisations remains unclear, despite the high prevalence of the condition. In several large non-domestic cat species meniscal mineralisations are regarded as normal structures that develop during skeletal maturation.4–6 They commonly seem to be accidental findings without clinical significance in domestic cats. 1
Stifle pathology also may occur concurrently to meniscal mineralisations.1–3 Initial clinical reports described the presence of meniscal mineralisations in cats with cranial cruciate ligament (CrCL) rupture, although a cause and effect relationship could not be established.2,3 The authors of one study speculated that the medial meniscus loosens its normal compliance in the presence of calcification or ossification, which may predispose the stifle to CrCL rupture. 3 More recently, a large prospective clinical and cadaveric study was able to show that meniscal mineralisations in domestic cats are associated with older age and degenerative joint disease (DJD), especially of the medial joint compartment. 1 Association with CrCL pathology could not be established: cats with radiographically evident meniscal mineralisations had no clinical evidence of CrCL rupture, and there were no macroscopically detectable changes of the CrCL in the stifle joints of cat cadavers with meniscal mineralisations. 1 In cats, CrCL ruptures commonly result from traumatic events, although a subset of feline patients with similarities to canine degenerative CrCL disease has been described. 7
Meniscal mineralisations can differ markedly in size, shape and localisation, and in microscopic appearance. Whereas many are small and rounded and are located in the area of the cranial horn of the medial meniscus, others have a more triangular or irregular shape and reach substantial sizes that seem to exceed the cranial border of the medial meniscus. The goal of this study was to gain further insight into the association of meniscal mineralisations, DJD and CrCL pathology. We hypothesised that degenerative changes may be present in the feline CrCL prior to complete rupture, and that large mineralisations in the feline stifle joint are associated with CrCL pathology.
Materials and methods
This study was conducted at the Vetsuisse Faculty of the University of Zurich, Switzerland, and consisted of two parts. First, radiographic prevalence of different sizes of mineralisations between a group of cat cadavers without CrCL rupture and clinical cats with CrCL rupture was compared. Second, stifle joints of cat cadavers with various sizes of mineralisations were examined histopathologically, describing the appearance and localisation of the mineralisations and degenerative changes in various articular structures, including the CrCL. Stifle joints were prepared in toto, allowing evaluation of intra- and periarticular structures in their normal anatomical relationship.
Cadaver group
Hindlimbs of cats that had been euthanased or had died from causes unrelated to this study were collected. Each stifle joint was examined for the absence or presence of positive cranial drawer signs and a lateral radiograph was taken. Both hindlimbs were disarticulated at the hip joint, packed in plastic bags, marked with a number that allowed later identification and stored at −18°C. The cat cadavers needed to have a known age of >2 years and absence of a positive cranial drawer test to be included in the radiographic prevalence study. This resulted in a group of 44 cats (88 stifle joints). Ten stifle joints were prepared for histopathology as described later.
Clinical patients with CrCL rupture
Consecutive medical records and orthogonal radiographs of clinical cats with CrCL rupture were recruited from the clinic database. Radiographs of cats with known age and body weight that had been presented for hindlimb lameness and had a diagnosis of CrCL rupture based on positive cranial drawer test and/or visualised ruptured CrCL in surgery were included. Cats with injuries to multiple ligaments of the stifle joint were excluded. The first 25 cats matching inclusion and exclusion criteria going back in time were evaluated. Mean ± SD age of the 25 cats with CrCL rupture was calculated using Excel for later comparison with the cadaver group.
Radiographic evaluation
The presence or absence of meniscal mineralisations, and the size of mineralisations when present were evaluated on lateral radiographs of both the clinical patients and the cadaver stifles. Length and width (mm) of the mineralisation was measured (PK) with a common ruler at the longest and widest points of the mineralisation and were then multiplied with each other. Mineralisations ⩽2.25 mm2 were classified as small, mineralisations between 2.25 and 6.25 mm2 as intermediate, and mineralisations ⩾6.25 mm2 as large (Figures 1–3).

Lateral radiograph of a cat with a small round mineralisation in the area of the cranial horn of the medial menisci (arrowhead)

Lateral radiograph of a cat with an intermediate-sized mineralisation in the cranial stifle joint. This mineralisation is irregularly shaped and seems to be located along the cranial border of the meniscus

Lateral radiograph of a cat with a large mineralisation, located in the area of the fat pad. There is another mineralisation in the caudal aspect of the joint capsule
DJD was evaluated on the orthogonal radiographs of the clinical cats with CrCL rupture, but not in the cadaver limbs as only lateral radiographs were available. DJD was assessed by two observers (PK and KV) as being absent or present, based on presence or absence of osteophytosis and on presence or absence of subchondral bone changes. Absence or presence and size of articular mineralisations were not considered in the DJD assessment.
Radiographic prevalence of meniscal mineralisation
Radiographic prevalence of meniscal mineralisations and their sizes was evaluated in the group of clinical cats with CrCL rupture (n = 25) and the cadaver group (n = 44). The cats of the cadaver group were sorted according to their age, in order to recruit an age-matched group to the clinical cats. This was achieved by stepwise exclusion of the oldest cats until the mean age of the cadaver group was the same as in the clinical group. The older cat cadavers formed their own group. Prevalence of meniscal mineralisations and their sizes is reported for the clinical patients with CrCL rupture, the age-matched group of cadavers and the group of older cats in the cadaver group. Because only radiographs of the affected stifle joint were available for the clinical patients with CrCL rupture, whereas both stifle joints had been radiographed in the cadavers, comparison of prevalence between groups was performed by including only one stifle joint of the cats in the cadaver group; the left stifle joint was evaluated in the first half of the cat cadavers (n = 22) and the right stifle joint in the second half of the cadavers (n = 22).
Preparation of stifle joints for histopathology
Limbs were thawed at room temperature for 14–18 h. Nine stifle joints without cranial drawer instability were prepared, out of which two had no mineralisations on lateral radiographs, two had small mineralisations, one had an intermediate-size mineralisation and four had large mineralisations. One cat cadaver with a large mineralisation on radiographs also had a positive cranial drawer test unilaterally. This stifle joint was examined additionally.
Skin and musculature were removed, and femur and tibia were sectioned in their distal, and proximal third, respectively. The whole joints were immersed for at least 4 days in a solution consisting of 2.5% glutaraldehyde in phosphate buffer and 1.3% formaldehyde. This mixture was individually prepared before use. Solution (4–5 ml) was injected intra-articularly before immersing the specimen, for improved fixation of intra-articular structures. After fixation, the specimens underwent dehydration in an ascending alcohol series over 4 days and defatting in xylol for 3–5 days. Specimens were finally infiltrated under vacuum in a non-polymerising methyl methacrylate (MMA) mixture (89 g MMA stabilised [ACROS Organics]; 10.5 g dibutylphthalat [Merck Schuchardt OMG]; 0.5 g Perkadox 16 [Dr Grogg Chemie AG]) at 4°C for 7 days before being imbedded in the polymerising MMA mixture (89 g MMA, 10 g dibutylphthalat, 1 g Perkadox 16). The specimens were initially cooled to reduce the risk of heat-induced bubble formation during polymerisation. After the first 3–5 days they were kept at room temperature.
Sagittal slices with a thickness of approximately 800 μm were cut using a diamond-coated saw (Exakt; Firma Haslab) (Figure 4). After fixation of the slices on a polyacryl slide with glue (Cementit CA 10; Merz + Benteli AG), they were then milled to a thickness of 500–600 μm (Leica SP 2600; Leica Microsystems). Sections were stained using a Giemsa surface stain.

Whole feline stifle joint embedded in a methyl methacrylate block and undergoing sagittal slicing with a diamond-coated saw
Histopathological evaluation
The slides were first evaluated under a stereomicroscope (Leica MZ16) and for exact investigation of the cellular structures under a light microscope (Leica DM LB2) using ranges of magnification from × 10 to × 400. Microscopic appearance, localisation and extent of the articular mineralisations were evaluated. A microscopic score reflecting degenerative changes was formulated by two independent observers (PK and HG) for the cranial cruciate ligament, the caudal cruciate ligament, both menisci, the joint cartilage and the joint capsule. Each structure was graded in 0.25-point increments on a scale from 0–3. A score of 0 indicated no degenerative changes, scores of 0.25–1.00 low-grade degenerative changes, scores of 1.25–2.00 intermediate severity of degenerative changes, and scores of 2.25–3.00 were assigned to severe degenerative changes. A consensual score was formulated at a repeat examination if observer disagreement existed in the initial scoring. The mean of the individual scores was defined as the global joint score. Scores of stifle joints with no or small mineralisations (n = 4) were compared with scores of stifle joints with medium and large mineralisations (n = 5), excluding the stifle joint with palpable joint instability. Scores were also compared between stifle joints with a CrCL score of <1.5, and stifle joints with a CrCL score of ⩾1.5, regardless of the presence and size of articular mineralisations.
Results
Radiographic prevalence and size of meniscal mineralisations in clinical cats with CrCL rupture
Twenty-five clinical cats (13 male, 12 female) with CrCL rupture were presented from 1998–2007. Mean ± SD age was 8.60 ± 4.52 years (range 2–18 years). Mean ± SD body weight was 5.50 ± 1.48 kg (range 2.6–8.1 kg). Twenty-three cats were domestic shorthair, one was a Persian and one a German Rex. Radiographic DJD was deemed absent in 18 and present in seven cats. Out of the seven cats with DJD, only two had a history of lameness of more than 3 weeks’ duration. All seven cats with CrCL rupture and concurrent DJD had medium or large mineralisations. Medium or large articular mineralisations were additionally observed in five cats without radiographic DJD. The overall prevalence of articular mineralisations was 76%, out of which most mineralisations were of intermediate size or large (Table 1).
Prevalence of articular mineralisations in cats with cranial cruciate ligament (CrCL) rupture, an age-matched group of cat cadavers and an older group of cat cadavers
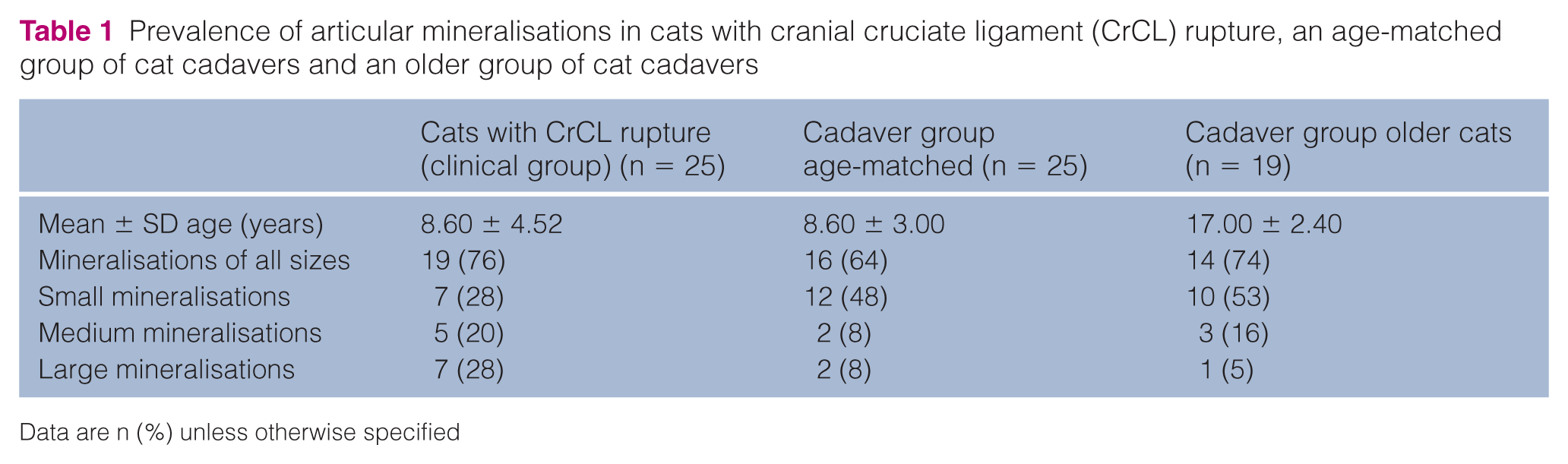
Data are n (%) unless otherwise specified
Cadaver group
The mean ± SD age of the 44 cats in the cadaver group was 12.2 ± 5.0 years. The overall prevalence of articular mineralisations in the cadaver group was 82% when both stifle joints were considered, with only 8/44 cats (18%) having no mineralisation in either stifle joint. Six cats (13.6%) had unilateral stifle mineralisations, all of which were small, and 30 cats (68.2%) had bilateral mineralisations. As mentioned earlier, only either the left or the right stifle of the cadavers were considered for comparison of prevalence with the clinical cats with CrCL rupture (Table 1): the prevalence of meniscal mineralisations of the 25 cats in the age-matched cadaver group (mean ± SD age 8.6 ± 3.0 years) when only including one limb was 64%, and was 74% in the group of 19 older cats. Both age groups had predominantly small mineralisations (Table 1).
Descriptive histopathological findings (n = 10 stifles)
Mineralisations
Mineralisations were found to be either calcifications or ossifications. The two radiographically small mineralisations were calcifications located as well-circumscribed calcified nodules within the cranial horn of the medial meniscus and surrounded by fibrous cartilage (Figure 5). Medium and large mineralisations represented ossifications consisting of well-organised woven bone that was usually surrounded by a thin layer of fibrous tissue. These ossifications were either located between the cranial horn of the medial meniscus and the joint capsule (Figure 6) or in the infrapatellar fat pad (Figure 7). A meniscal calcification was confluent with an ossification extending into the fat pad in one case. In another case, an intrameniscal calcification and a seemingly separate ossification in the infrapatellar fat pad were found. Fibrosis of the fat pad was present in seven joints. This was regarded as mild in one joint with a small intrameniscal calcification. The fat pads of stifles with medium or large mineralisations were moderately or severely fibrosed (Figure 7).

Sagittal section of a feline stifle joint with a small round and well-circumscribed calcification in the cranial horn of the medial meniscus. The fat pad, joint capsule and cartilage have a normal appearance (magnification × 8)

Sagittal section of the cranial aspect of a feline stifle joint with an ossification (magnification × 16). The ossification consists of mature cancellous bone, containing fat centrally. It is located between the cranial horn of the medial meniscus and the fat pad and is delineated by a band of calcified fibrous cartilage. The fat pad is fibrosed

Sagittal section across the infrapatellar fat pad of a specimen with multiple ossifications and high-grade fibrosis of the infrapatellar fat pad (magnification × 10). There is marked proliferation of synovial villi originating from the joint capsule adjacent to the fat pad
Menisci
Low-grade meniscal degeneration was mainly located in the centre of the meniscal fibrocartilage. With continuing degeneration, disaggregation of fibres reached the meniscal periphery and the surface started to show roughness. The fibres in the cranial horns of the menisci tended to be most severely affected. Severely degenerated menisci had a roughened surface with clefts or tears. Normal architecture of fibres was lost and chondrocyte appearance changed; their nuclei became bigger and vacuolated. Chondrocytes were subjectively reduced in numbers, with some areas being completely acellular. Meniscal degeneration was generally more severe in stifles with mineralisations but did not seem to be consistently and directly associated with the size of the mineralisation. Minor changes were found in two stifles without calcification, and in one cat with an intermediate-sized mineralisation. Intermediate grade of meniscal degeneration was observed in the two cats with small calcifications and in three cats with large mineralisations. Severe changes were found in two cats with large mineralisations and in the cat with complete CrCL rupture.
Cranial and caudal cruciate ligaments
Degenerative changes were seen in both the cranial and caudal cruciate ligament but were more pronounced in the CrCL (Figure 8). Low-grade cruciate ligament degeneration was seen as localised areas of fibres that had lost their orientation, with the majority of the ligament having a normal appearance. There was some cleft formation between fibres in larger areas of degeneration, but the basic structure of the ligament was still intact. With increasing degeneration of the ligament, fibrocytes showed more evidence of chondroid metaplasia in that they appeared rounded, had an increased volume and formed lacunae around them. Non-degenerated cruciate ligaments typically were poorly stained with the Giemsa surface stain and appeared yellow. Degenerated fibres stained differently and became blue. High-grade CrCL degeneration was found in one specimen with a large ossification. Complete rupture and severe degeneration was evident in the cat cadaver with complete CrCL rupture.
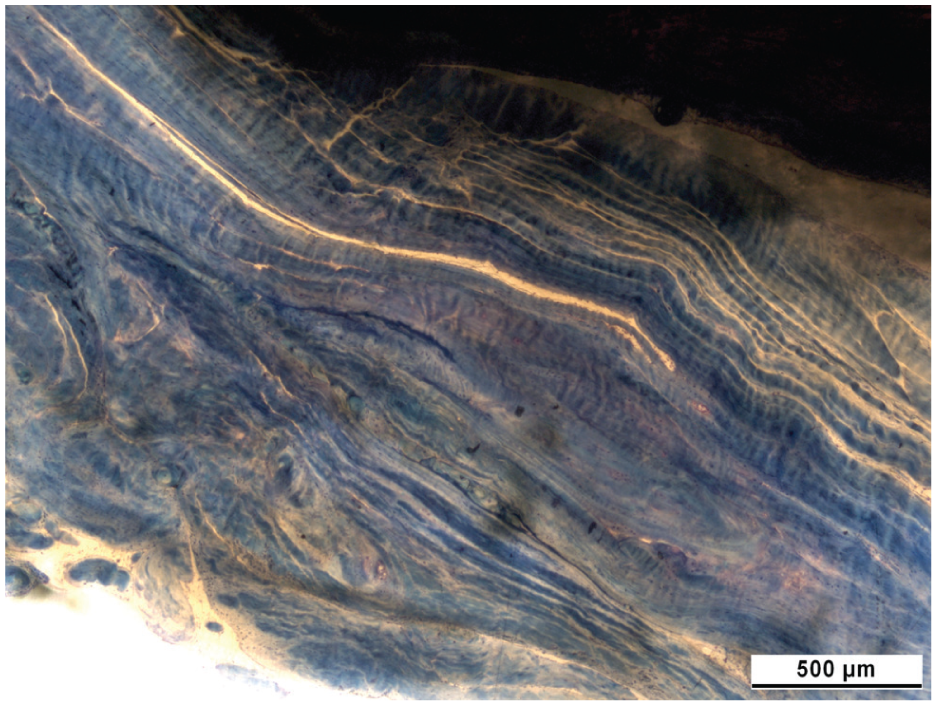
Sagittal section through a cranial cruciate ligament displaying severe signs of degeneration (magnification × 400). There is loss of the parallel arrangement and swelling of fibres. Note the curly course of fibres, the cleft formation reaching the ligament surface, and the hypertrophy of the synovial lining
Articular cartilage
Low-grade degenerative changes were mainly located superficially in the tangential layer. Intermediate changes consisted of erosion of the cartilage surface in greater areas and changes extending as clefts into the transitional or radial zone. Severe cartilage degeneration was only found in the cat cadaver with an unstable knee and involved extensive erosion of the superficial layers and in parts complete erosion of all layers onto the subchondral bone, accompanied by loss of architecture and chondrocyte death.
Joint capsule
Low-grade changes consisted of elongated and/or thickened synovial villi and an increase in synovial cell layers. Samples that were classified as having intermediate changes had similar changes to the synovial membrane and additional thickening of the fibrous joint capsule. Two joints with radiographically large mineralisations had high-grade changes with severe fibrosis of the joint capsule and in one case there was an additional ossification in the caudal part of the joint capsule.
Relationship of articular mineralisations and histopathological scores
Degenerative changes of all individual intra-articular structures, as well as the global degenerative joint score, were higher in joints with radiographically medium or large mineralisations than in joints with no or small mineralisations (Table 2). The largest increase in degenerative scores between cats with no or small mineralisations compared with those with medium or large mineralisations were found in the joint capsule, which was mainly owing to increased severity of capsule fibrosis. Also, CrCL scores were higher in cats with medium or large mineralisations than in stifles with no or small mineralisations. When grouping cats (excluding the cat with positive cranial drawer test) according to the status of their CrCL (score of <1.5 or >1.5) a corresponding increase in degeneration scores of all other intra-articular structures, especially the caudal cruciate ligament, the joint capsule and the global score, was found. The mean global score was 0.73 in cats with a CrCL score of <1.5 and 1.24 in cats with a CrCL score of >1.5.
Summary of histopathological scores in 10 stifle joints of cats. Shades of grey indicate low-grade, intermediate or high-grade degenerative changes in different articular structures. There is an increased tendency for intermediate and high-grade changes in cats with medium or large articular mineralisations. The fat pad showed various degrees of fibrosis, most severe in the stifle joints with large mineralisations

Stifle joint with positive cranial drawer test and complete CrCL rupture
CrCL = cranial cruciate ligament; CaCL = caudal cruciate ligament
Discussion
Results of this study confirm the previously reported high prevalence of meniscal mineralisations in domestic cats. 1 The preparation of the stifle joints in toto showed that larger mineralisations frequently extended into soft tissues cranial of the medial meniscus, mainly the joint capsule and fat pad, rather than being confined to the meniscal fibrocartilage itself. Differences also seem to exist between small and large mineralisations with regard to concurrent DJD and CrCL degeneration. Cats with CrCL rupture had a higher prevalence of larger mineralisations than the age-matched control group, and histopathologically the presence of larger mineralisations was associated stifle DJD, including degenerative changes of the CrCL. This likely indicates that larger mineralisations are part of a degenerative process in the stifle joint, and that CrCL degeneration can also precede complete CrCL rupture in cats.
Meniscal mineralisations are known to occur in several species, including domestic and non-domestic cats,1–6 guinea-pigs, 8 pigs, 9 dogs3,10 and humans.11–13 Prevalence, assumed aetiopathogenesis and clinical relevance vary between species. Whereas meniscal mineralisations are rare in dogs and humans and generally regarded to be a pathological finding secondary to trauma or meniscal degeneration,3,11–13 they are common in non-domestic cats where they are thought to be a normal anatomical feature or a vestigial anomaly without clinical significance.4–6 The high prevalence of meniscal mineralisations in ageing domestic cats may implicate that they are a normal feature in the ageing feline stifle, even more so because many affected domestic cats seem to be free of clinical signs. 1 In one study, approximately 70% of stifle joints with meniscal mineralisations had no other signs of stifle pathology on radiographs, and there was no difference in pain response on palpation of the stifle joints between cats with and without meniscal mineralisations. 1
The prevalence of articular mineralisations was even higher in our cadaver population than reported previously. Mineralisations were observed in one or both stifle joints of 82% of cats in this study, whereas only 46% were affected in a previous study. 1 This difference may be partially owing to the older age of the cats in this study (12 years) as compared with 9 years in the previous study, 1 but also differences between groups in geographical location, genetic background, breed distribution or outdoor/indoor lifestyle could be responsible for the discrepancy in prevalence.
The main focus of this study was to evaluate whether there were differences in the size of the articular mineralisations regarding histopathological appearance and location, and association with DJD and CrCL pathology. The preparation of whole-stifle specimens allowed determination of both the anatomical location and histopathological appearance of the mineralisations. Small mineralisations were located within the cranial horn of the medial meniscus and were well-circumscribed calcified bodies surrounded by otherwise normal- or near-normal-appearing meniscal fibrocartilage. Large mineralisations were found to be ossifications consisting of mature cancellous bone, which seemed to origin at the cranial border of the meniscus or within the joint capsule in some specimens, and appeared to be located within the fat pad without evident connection to the menisci in other cases. Meniscal calcifications and para-articular ossifications can be present simultaneously. In contrast to our findings, ossifications have previously been described to be always located in the cranial horn of the medial meniscus.1–3 It is possible that routine sampling of the menisci and ossifications may have made it difficult to determine the exact localisation of the ossifications in the absence of visualisation of surrounding structures.
It remains unknown whether the calcifications and ossifications represent the same disease process at a different stage or if they are caused by different factors. In general, dystrophic tissue calcification and heterotopic ossification are caused by different mechanisms. Dystrophic calcification tends to occur in degenerate tissue low in blood supply and oxygen. Small mineralisations within the medial meniscus were more common in older cats in this and in a previous study, 1 and it seems likely that calcifications in the medial meniscus occur secondary to age-related meniscal degeneration and have no clinical significance. Heterotopic ossification represents formation of bone in soft tissues where bone usually does not exist. Formation of bone requires angiogenesis and migration and activation of osteogenic precursor cells. In human medicine para-articular heterotopic ossifications have been described to occur after trauma, or joint and spinal surgery.14,15 Assuming that large mineralisations in feline stifle joints represent heterotopic ossifications in the joint capsule and fat pad these should then be considered pathological, even more so as they were usually accompanied by significant joint capsule and fat pad fibrosis. Calcified bodies in the joint capsule can also represent synovial osteochondromatosis, a condition characterised by primary or secondary formation of osteochondral nodules in the synovial lining of the joint capsule. Synovial osteochondromatosis in cats has been described in several case reports.16–18 However, radiographically it is difficult to differentiate between synovial osteochondromatosis and osteoarthritis, and histology was only performed in one of the reports. 18 In synovial osteochondromatosis the osteochondral nodules originate in the synovial lining and frequently detach from the joint capsule to become loose joint bodies. 18 This was not observed in the present study.
A relationship between meniscal mineralisation and cartilage degeneration has been demonstrated previously; cadavers with meniscal mineralisations had higher cartilage degeneration scores, especially of the medial compartment of the stifle, based on India ink evaluations, than cats without meniscal mineralisations. 1 Furthermore, the size of the meniscal mineralisations correlated with the severity of cartilage degeneration. 1 This is consistent with the findings of the present study that degenerative scores, not only of the articular cartilage, but also of all articular structures, were higher in joints with larger articular mineralisations. Degenerative changes in stifle joints without and with small mineralisations were mild and more likely to represent wear-and-tear changes. We did not include the presence and size of mineralisations as a radiographic feature in the subjective DJD assessment, but all cats with pre-existing DJD also had medium or large mineralisations, indicating them to be a feature of feline stifle osteoarthritis.
CrCL degeneration is the most common cause for stifle osteoarthritis in dogs, but in cats it is generally assumed that CrCL rupture is usually caused by trauma. Only one retrospective clinical study on feline CrCL ruptures describes a subgroup of cats assumed to suffer from a degenerative process of the CrCL similar to dogs. 7 These cats tended to be older and heavier than cats with traumatic CrCL and can be affected bilaterally. 7 The finding that some cats within our CrCL rupture group had pre-existing radiographic DJD at the time of presentation supports these previous clinical observations. Histopathological evaluation of our cadaver stifles also clearly demonstrated that degenerative changes can be present in feline CrCL prior to complete rupture. Additionally, the severity of degeneration in the CrCL mirrored the severity of degeneration of other articular structures, including cartilage and joint capsule.
This study has several drawbacks, and further studies are needed to clarify the cause and effect relationship of articular mineralisations, DJD and CrCL in feline stifle joints. We only provide a descriptive histopathological study of 10 feline stifle joints, which may not reflect the normal population, especially as selection of which stifle joints of the cadaver group were processed for histopathology was not randomised. Although the preparation of stifle joints in toto had advantages in localising the radiographically visible mineralisations within the stifle joint, the thick slices and the embedding in polymethyl methacrylate (PMMA) somewhat limited the information about single cell constitution and extracellular matrix. We were also unable to evaluate radiographic DJD in the cat cadavers, as, owing to cost constraints, only lateral radiographs were available.
Conclusions
Small mineralisations in feline stifle joints were found to be calcifications in the cranial horn of the medial meniscus, with only minor, likely age-related, degenerative joint changes. In contrast, large mineralisations were mainly located in the joint capsule and fat pad and were associated with joint capsule fibrosis and stifle osteoarthritis. The CrCL in affected stifles showed signs of degeneration, similar to dogs with degenerative CrCL disease.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.