
Abstract
Radioiodine therapy is commonly used in hyperthyroid cats and has a high success rate, ranging from 85–95%. As in humans, thyroid volume has been reported to influence radioiodine therapy outcome in hyperthyroid cats. The purpose of this study was to relate total thyroid volume, calculated by a newly constructed formula for feline patients (0.438 × length × width²), to the outcome of radioiodine therapy. To search for a correlation between total thyroid volume and therapy outcome, 167 hyperthyroid cats were included. Patients were categorised according to the administered radioiodine dose and therapy outcome. Our analysis did not show a significant relationship between an increasing total thyroid volume and the odds for a final low total thyroxine concentration (TT4; P = 0.3930) or a final hyperthyroid outcome (P = 0.0901). A significant relationship was found for an increase in the odds for a final low TT4 outcome with an increase in the number of foci detected on the pertechnetate thyroid scan (P = 0.0238). This was not true for a final hyperthyroid outcome (P = 0.7435). The number of detected foci was also significantly associated with the total thyroid volume (P = 0.0006). Findings indicated that the presence of multiple affected foci influences therapy outcome towards a low TT4 outcome. Bilateral hyperthyroidism and its potential effect on a final low TT4 outcome should therefore be addressed when informing owners of the possible outcomes of radioiodine therapy for their cat.
Introduction
Radioiodine therapy in hyperthyroid cats has a high success rate, reported in literature as hypo- or euthyroid, ranging from 85–95%.1–6 In this study therapy failure is described as a hyperthyroid or low total thyroxine concentration (TT4) outcome. The term ‘low TT4’ rather than hypothyroid was chosen for patients with a serum TT4 below the reference interval, given the difficult diagnosis of hypothyroidism in cats and the lack of extensive diagnostic work-up in the patient follow-up in this study.
Therapy failure is accompanied by considerable drawbacks, justifying further research on possible causes. A final low TT4 outcome has a potentially negative effect on renal function and may create the need for thyroxine supplementation, meaning daily medication and an additional cost for the owner.7–11 Persistent hyperthyroidism results in the need for a second radioiodine therapy or another form of treatment. The relationship between a large thyroid volume and a persistent hyperthyroid outcome has been reported in human medicine by different authors,12–20 although this has been disputed by others. 21 Total thyroid volume in hyperthyroid cats, determined ultrasonographically, was reported to be significantly different from the normal mean total thyroid volume in euthyroid cats. 22 Therefore, it is reasonable to consider an effect of thyroid volume on therapy outcomes. Most studies in humans have not found any relationship between thyroid gland size and a hypothyroid outcome,23–25 although one study reported that smaller goitres were a risk factor for developing hypothyroidism. 26 Thyroid size estimation by palpation, as a scoring factor of dose determination, has been used in hyperthyroid cats treated with radioiodine.1,4 In two other studies, thyroid volume estimation was taken into account for dose calculations in hyperthyroid cats; however, the method of volume estimation was not mentioned.2,27 Only a single study described the effect of thyroid volume on therapy outcome in hyperthyroid cats, concluding that persistent hyperthyroidism after a single treatment was seen more often in cats with larger total thyroid volumes, as estimated by scintigraphy. 5
In a previous study by our group, eight different formulas to estimate thyroid volume by scintigraphy were compared. 28 One formula, derived from human medicine, showed no statistical difference between the volume estimated by ultrasound and the volume estimated by scintigraphy (volume = 1.08 × [π /6] × length × width² or volume = 0.565 × length × width²). Furthermore, this formula was based on a single scintigraphic acquisition and therefore was selected for volume estimation in this study. Further optimisation of this formula led to the determination of a corrective factor of 0.438 for feline use (volume = 0.438 × length × width²). The goal of this study was to relate the total calculated thyroid volume to the outcome of the subsequent radioiodine therapy. We hypothesised that larger volumes would result in a higher percentage of persistent hyperthyroidism and smaller volumes would be at risk for receiving too much radioactive iodine thus resulting in a low TT4 outcome.
Materials and methods
Demographics
The study consisted of 167 hyperthyroid cats (81 males, 86 females), with a mean age of 12 years and 5 months (range 7–18 years). All cats were diagnosed with hyperthyroidism based on their clinical signs and measurement of the serum TT4 by the referring veterinarian. The first group of 39 cats was presented at our facility between December 2003 and October 2008, and these patients were retrospectively included. The second prospective group of 128 cats was presented between October 2011 and November 2012. As a first inclusion criterion, a control TT4 measurement 6 months after the radioiodine therapy was required. These final outcomes, solely based on the control TT4 value, were categorised as low TT4, euthyroid or hyperthyroid. Only those cats with scans that showed unilateral disease or clearly discernible hyperactive thyroid tissue foci in cases of bilateral disease, or the presence of additional ectopic thyroid tissue, were included.
Thyroid scintigraphy
All cats underwent a diagnostic planar thyroid pertechnetate (99mTcO4–) scan. The cats were scanned on a dual-head camera (GCA 7200A; Toshiba) with a low-energy high-resolution (LEHR) collimator. The average 99mTcO4– activity injected into the cephalic vein was 95.3 MBq and acquisitions were performed, on average, 30 mins after injection. The cats were anaesthetised with propofol (4–8 mg/kg to effect, IV, Propovet, 10 mg/ml; Ecuphar) and were positioned in ventral recumbency with the g camera located underneath the table. Zoomed 25.6 × 25.6 cm field-of-view planar images were acquired on counts (200 kcounts), in a 256 × 256 matrix, with a 0.1 cm pixel size. All scans were processed using multimodality software (Hermes V5.0; Nuclear Diagnostics AB). After the diagnostic scan, patients were treated by intravenous injection of an individually adapted dose of radioiodine (131I), depending on the severity of clinical signs, TT4 and the thyroid-to-salivary gland ratio as determined on the 99mTc-scan. Patients that were on prior medicinal treatment were taken off antithyroid medication for a minimum of 10 days before the radioiodine therapy. This dose scoring method is similar to what has been reported previously. 4 The median dose of radioiodine administered was 117.71 MBq (range 69.56–372.22 MBq).
Thyroid volume
To quantify thyroid volume, a formula based solely on the length and width of each lobe (volume = 1.08 × [π /6] × length × width²) was elected as the most suitable. 28 This formula assumes an ellipsoid shape of the thyroid gland and equates height (ie, the dorsoventral dimension) to width (ie, the mediolateral dimension), and a corrective factor of 1.08 was applied. The formula did not show a significant difference between the ultrasonographically and scintigraphically estimated volumes and has the additional advantage that only a single ventral planar image is needed. As the correction factor was derived for human patients, we first determined a factor for feline use. The assumption of an ellipsoid shape was dismissed, and a correction factor of 0.438 was calculated based on a mathematical comparison of thyroid length and width measurements that were made by ultrasound and planar thyroid scintigraphy for a group of 28 cats (unpublished data). The correction factor was introduced in the formula as follows: thyroid volume = 0.438 × length × width².
The thyroid volumes of 167 hyperthyroid cats were then calculated using this new formula. Length (ie, the craniocaudal dimension) and width (ie, the mediolateral dimension) measurements were made with automatically applied regions of interest, based on a 30% threshold of the activity of the lobe considered (Figure 1). 28 All measurements were made by the same author (VV). The volume of each thyroid focus was calculated and summed in the case of bilateral disease or the presence of ectopic thyroid tissue. Next, a correlation between the total thyroid volume and therapy outcome was investigated. Given that the activity of radioiodine used in our facility was individually adapted, a dose correction was needed to model the relationship between total thyroid volume and therapy outcome. To correct for the administered dose, the cats were divided into three groups: group 1 (low dose, 74–148 MBq, n = 114), group 2 (medium dose, 148–259 MBq, n = 41) and group 3 (high dose, >259 MBq, n = 12).
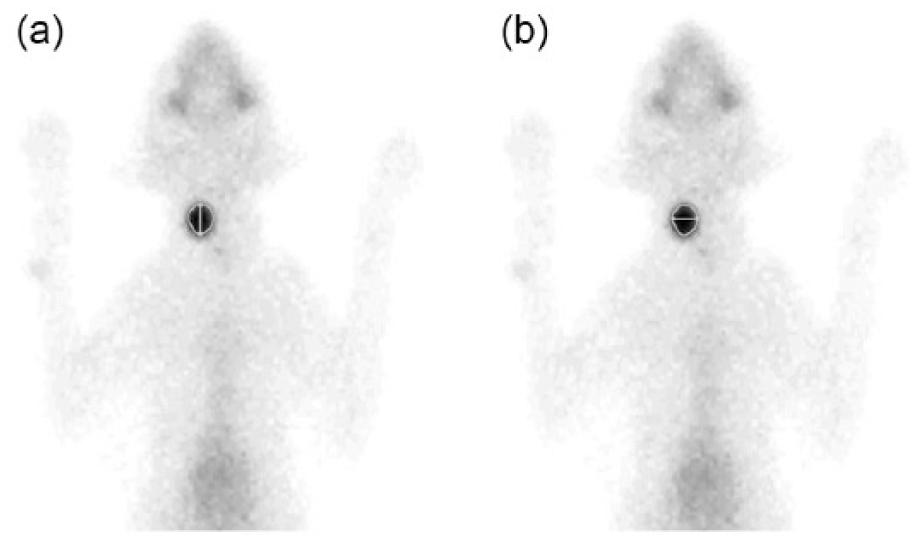
Planar pertechnetate scan demonstrating (a) length and (b) width measurements based on a 30% threshold region of interest in a unilaterally affected hyperthyroid cat
The effect of total thyroid volume and number of foci on the final outcome was modelled by a logistic regression model using the euthyroid group as a reference category, and using dose as categorical and volume and the number of foci as continuous fixed effects. Additionally, a linear regression model was fitted to assess the effect of the number of foci on total thyroid volume.
Results
The findings for each of the different dose categories are summarised in Table 1. Of the 167 cats treated with radioiodine, 111 (66.5%) demonstrated a TT4 value within the normal reference interval at 6 months after therapy. Forty (24.0%) cats showed a TT4 value below and 16 (9.5%) showed a TT4 value above the normal reference interval. Ninety-six (57.5%) cats had bilateral thyroid disease, 52 (31.1%) were unilaterally affected and 19 (11.4%) had unilateral or bilateral disease with additional ectopic foci. Of the 111 euthyroid cats, 62 (55.9%) were bilaterally affected, 40 (36.0%) were unilaterally affected and nine (8.1%) showed the presence of additional ectopic thyroid tissue. Two of these cats showed a single focus in the cervical region and two intrathoracic foci. They were classified as bilateral with ectopic tissue, although the question remains if both intrathoracic foci were ectopic tissue or if one of them was an enlarged, descended thyroid lobe. The seven other cats all showed bilateral disease with additional ectopic thyroid tissue. Of the 40 final low TT4 cats, 24 (60.0%) were bilaterally affected, eight (20.0%) were unilaterally affected and eight (20%) were bilaterally affected with additional ectopic thyroid tissue. Of the 16 persistent hyperthyroid cats, nine (56.25%) were bilaterally affected, five (31.25%) were unilaterally affected and two (12.5%) showed ectopic foci. One of the latter showed an enlarged thyroid focus in the cervical region and a smaller focus intrathoracically; this cat was classified as unilaterally affected with additional ectopic thyroid tissue. Again, whether this should be defined as bilateral disease with one lobe descended or as unilateral disease with additional ectopic tissue is not certain. The other cat with ectopic thyroid tissue was bilaterally affected with an additional ectopic focus. The mean thyroid volume of unilaterally affected cats was 1130.4 mm³ ± 748 mm³; the mean total thyroid volume of bilaterally affected cats was 1418.1 mm³ ± 1044.5 mm³; patients either unilaterally or bilaterally affected, but with additional thyroid tissue, showed a mean total thyroid volume of 1742.28 ± 1486.8 mm³. The median dose of radioiodine and range of doses for the final euthyroid group was 116.81 MBq (range 69.56–372.22 MBq); for the final low TT4 group this was 129.5 MBq (range 79.40–346.76 MBq); and for the final hyperthyroid group this was 110.63 MBq (range 82.14–319.20 MBq). The median doses of radioiodine with their range for each dose category were as follows: group 1 (102.12 MBq; range 69.56–142.3 MBq), group 2 (179.04 MBq; range 148.74–255.67 MBq), group 3 (318.07 MBq; range 262.7–372.22 MBq).
Summary of the findings for each dose and outcome category

The SD could not be calculated as data from only one cat were available
Category 1 = low dose; category 2 = medium dose; category 3 = high dose; UL = unilateral, BL = bilateral, E = ectopic thyroid tissue
A possible influence of the calculated total thyroid volume on therapy outcome was investigated. The odds ratio (OR) per 100 mm³ increase in thyroid volume of hyperthyroidism, relative to euthyroidism, was 1.04257 (95% confidence interval [CI] 0.99252–1.09514), thus not significantly different from 1 and clinically not relevant (P = 0.0901). The OR per 100 mm³ increase in thyroid volume of the final low TT4 group, relative to the final euthyroid group, was 1.01628 (95% CI 0.97857–1.05544), which is even closer to, and not significantly different from 1 (P = 0.3930). Regarding the effect of the number of foci on final outcome an OR of 1.9906 (95% CI 1.08288–3.67914) was observed for the odds of a low TT4 outcome relative to the odds of a euthyroid outcome. This means that an increase of 1 unit for the number of foci doubles the odds of a final low TT4 outcome relative to a euthyroid outcome (P = 0.0238). However, the number of foci did not significantly increase the odds for a final hyperthyroid outcome relative to a euthyroid outcome (OR = 1.16216; 95% CI 0.46381–2.91197; P = 0.7435). Finally, the relationship between the number of foci counted on the 99mTcO4– scan and the total thyroid volume was fitted by a linear regression model, and this analysis demonstrated a significant effect of an increasing number of foci on the total thyroid volume (P = 0.0006).
Discussion
Although full agreement has not been reached, the majority of human studies found indications for a relationship between a large thyroid volume and persistent hyperthyroidism.12–20 The largest volumes in our study were observed in the persistent hyperthyroid outcome group (Table 1); however, no significance was reached regarding the odds of hyperthyroidism, relative to euthyroidism, with an increasing thyroid volume. In the study by Forrest et al, 5 11% of the hyperthyroid cats treated with radioiodine remained hyperthyroid, an outcome comparable to ours (9.5%). The persistent hyperthyroid cats in this study all showed significantly larger volumes of thyroid tissue; however, the method of volume calculation was different from our study and the number of cats included was much lower (n = 80). 5 A possible reason for the lack of statistical significance in our study might also be the small number of cats in the final hyperthyroid group (n = 16). The formula that was designed to estimate thyroid volume might also have been not accurate enough in estimating the true total thyroid volume.
One other reason for persistent hyperthyroidism is the possibility of malignant disease. Thyroid carcinomas are considered uncommon in hyperthyroid cats, occurring in only 1–5% of the cases. The scintigraphic imaging features that have been described for thyroid carcinomas are a heterogeneous uptake pattern with irregular, spiculated margins, a multifocal pattern with uptake outside the normal thyroid lobe margins, and a linear multifocal uptake pattern secondary to tumour extension along the fascial planes.29,30 Although these imaging features are not highly reliable in differentiating malignant from benign disease, 30 none of the 16 persistent hyperthyroid cats in our study were suspected of malignant disease, based on their scans and follow-up. However, as no biopsies or fine-needle aspirates were taken, no final conclusions can be drawn. Aside from the obvious limitations of this study, it must be borne in mind that other factors may play a role in defining the final outcome after therapy. Both in human and feline studies, multiple factors influencing radioiodine therapy outcome, for example the administration of antithyroid drugs and severity of disease, have been proposed and argued.6,12,13,16,19,20,24,26,31,32
An interesting finding was the larger total thyroid volume in cats with a low TT4 outcome compared with those with a euthyroid outcome in dose categories 2 and 3 (Table 1). The majority (32/40 [80%]) of these final low TT4 cats were either bilaterally affected or bilaterally affected with additional ectopic thyroid tissue. This was confirmed in our statistical analyses demonstrating a significant relationship between the number of foci and the total thyroid volume, and a doubling of the odds for a final low TT4 outcome when one extra focus was observed on the 99mTcO4– thyroid scan. Nykamp et al reported a two-fold higher chance of final hypothyroidism in cats with bilateral disease, similar to our results. 27 Seventy-eight percent of their final hypothyroid patients had bilateral disease, whereas 1/6 cats with multifocal disease became hypothyroid. 27 The idea behind these findings is that the more thyroid tissue is destroyed, the less normal functioning tissue remains after therapy. Although a large overlap was observed, the mean thyroid volume of all unilaterally affected cats in our study was smaller (1130.4 mm³ ± 748 mm³) than the mean total thyroid volume of bilaterally affected cats (1418.1 mm³ ± 1044.5 mm³). Patients either unilaterally or bilaterally affected, but with additional thyroid tissue, showed a mean total thyroid volume of 1742.28 ± 1486.8 mm³. In human medicine this effect of large thyroid volume on hypothyroidism has not been reported.23–25 As far as the patients with a low TT4 outcome in dose category 1 of this study are concerned, a possible explanation could be that their smaller volumes increase the risk of radioiodine overdose and therefore the risk of a low TT4 outcome. However, this is only a hypothesis and, to our knowledge, there are no previous reports of this phenomenon in the literature. In three cats, two with a euthyroid and one with a hyperthyroid outcome, there was doubt over whether to define a high uptake focus in the thorax as a descended thyroid lobe or as ectopic thyroid tissue. In all three cats it was subjectively decided, based on the position of the focus, to define it as ectopic tissue. Although the possibility exists that these cats were categorised erroneously, the influence on our results was considered negligible. The percentage of cats with a successful outcome (66.5%) in our study was substantially lower than what is commonly reported in the literature.1–6 However, some studies only considered persistent hyperthyroidism as therapy failure, 5 or included clinical signs alone or along with TT4 as a factor to categorise the patient’s thyroid disease status.1–4 Moreover, the time of follow-up after therapy varies among studies. In our study, a TT4 value from 6 months after therapy was chosen as a reliable outcome. Not all cats with a low TT4 outcome in this study demonstrated clinical signs of hypothyroidism and therefore could potentially have been categorised as successful.
As the majority of our clients originate from neighbouring countries and often have to travel far, follow-up of patients was consistently performed by the initially referring veterinarians. Six months after the radioiodine therapy, veterinarians and owners were consulted by phone or by e-mail to obtain the results from the blood test and to provide an update on the condition of the patients. Unfortunately, not all data obtained from these enquiries proved to be reliable to evaluate potential clinical signs related to hypothyroidism. We therefore decided not to include clinical signs as a factor to define therapy success. A second drawback to these follow-ups by the referring veterinarians is the lack of consistency among laboratory reference values. This might raise questions concerning the significance of these measurements, particularly for values near the reference interval. Moreover, TT4 fluctuations have been reported in hyperthyroid cats before and after treatment,4,33–36 and could possibly also account for the borderline subnormal TT4 values in clinically normal cats after therapy. However, given the potentially negative effect of a decreased thyroid function on renal function, as described in both humans and cats,9–11 we chose to consider this low TT4 outcome as not successful. A low TT4 concentration can exacerbate renal disease and shorten the patient’s life span, especially in cats with underlying chronic kidney disease, which might not have been detected before therapy.37–40 Furthermore, the diagnosis of true hypothyroidism in cats is difficult and requires more than a single TT4 measurement, 41 as was available in our study. The fact that only a single blood sample was evaluated in this study could therefore also account for low values in some clinically normal cats. Finally, the effect of non-thyroidal illness creating an artificially low TT4 is a considerable contributing factor in this population, consisting mostly of older patients, and given the lack of a thorough clinical complete biochemical follow-up.
Conclusions
Although the largest thyroid volumes were observed in the persistent hyperthyroid group, no statistical significance was reached in the relationship between total thyroid volume and persistent hyperthyroidism. Remarkably, the majority of patients with a low TT4 outcome also presented larger total thyroid volumes compared with the final euthyroid group and the odds for a final low TT4 outcome were significantly increased in the case of multifocal disease. Therefore, the presence of multiple foci and their effect on a final low TT4 outcome could also be taken into consideration when informing owners of the possible outcomes for their cat. Finally, it has to be kept in mind that the influence on therapy outcome is most likely multifactorial, with different degrees of contribution and likely mutual interactions between several factors. This could explain the disagreement present in the literature and the lack of significance in our study, and justifies further research on this subject as data regarding factors influencing radioiodine therapy outcome in cats are severely lacking.
Footnotes
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.