
Abstract
A 6-year-old neutered female domestic shorthair cat weighing 3.1 kg was referred to the clinic owing to a 2 day history of anorexia. On physical examination, a pectus excavatum (PE) was apparent, and a cranial abdominal mass was palpated. Serum biochemical analysis showed severely elevated liver enzymes. On radiography, the PE was graded as moderate, and a 5 × 3 cm soft tissue density mass was detected in the cranial abdomen. Using duplex ultrasonography, the mass was identified as an enlarged liver lobe with vascular thrombosis. The diagnosis of liver lobe torsion (LLT) was confirmed surgically, and the affected left lateral lobe was resected. On follow-up, performed 1 and 6 months postoperatively, no further abnormalities were found on clinical examination or serum biochemical analysis. At follow-up examination, the PE did not appear to cause any additional clinical signs, indicating that treatment of moderate PE in older animals is not obligatory. This is the first reported case of LLT with concurrent PE, and the second feline case of LLT treated surgically. Animals with anatomical malformation of the diaphragm caused by PE may be at higher risk of developing LLT. Early diagnosis and surgical intervention of LLT can produce a good clinical outcome without further repercussions.
Case Report
Pectus excavatum (PE) and liver lobe torsion (LLT) are rare findings in veterinary patients. PE is a thoracic malformation found mostly in cats that causes dorsoventral narrowing of the thoracic cavity, displacement of the heart and anatomical changes in the diaphragm.1–4 In contrast to PE, LLT is more frequently reported in dogs, and only two feline cases of LLT have been published.5–9 The cause of LLT is unclear, but damage, and congenital absence or laxity of liver ligaments reportedly predispose an animal to LLT.5,6,8,10,11 Resection of the affected liver lobe is the treatment of choice for LLT and is well described in the literature.5,8,9 The present case report describes the first feline case with PE and left lateral LLT, treated with lobectomy of the affected liver lobe and without treatment of the PE.
Case description
A 6-year-old neutered female domestic shorthair cat weighing 3.1 kg was referred from a private veterinarian owing to a 2 day history of lethargy and anorexia. The cat had been absent for 2 days before the owners noticed the clinical signs. On physical examination, the cat was lethargic and mildly dehydrated, but in good body condition (body condition score 5 [scale 1–9]). The abdomen was tense and painful on palpation, and a mass was palpable in the cranial abdomen. A PE was evident on palpation; no respiratory abnormalities or signs of trauma were observed. A complete blood count (CBC) and serum biochemistry analyses were performed. The CBC showed a mild leukocytosis (13.7 × 103 cells/µl; reference interval [RI] 5.5–11 × 103 cells/µl]) and anaemia (packed cell volume 23.9% [RI 27–47%]). Serum biochemistry revealed a normal total protein concentration (8.0 g/dl [RI 6.5–8.5 g/dl]), elevated total bilirubin concentration (17.1 μmol/l [RI <3.4 μmol/l]), and severely elevated lactate dehydrogenase (>4000 IU/l [RI <70 U/l]), aspartate transaminase ([AST] >1000 IU/l [RI ⩿83 IU/l]) and alanine transaminase (ALT; >1000 IU/l [RI ⩿78 IU/l]) activity. A lateral radiograph of the thorax and cranial abdomen showed a PE with moderate dorsal to ventral narrowing (Figure 1). The frontosagittal index and the vertebral index were measured as prev-iously described and were 2.5 (RI 0.7–1.3) and 5.9 (RI 12.6–18.8), respectively, grading the PE as moderate. 2 All other skeletal structures appeared normal. A loss of detail in the cranial abdomen was present, but the caudal abdomen appeared normal. A soft tissue density mass (5 × 3 cm) was identified in the mid-cranial abdomen. On abdominal ultrasonography, a 5.6 × 2.1 cm hypoechoic mass caudal to the liver was observed and connected to liver; mild peritoneal nearly anechoic effusion was also present. The unique vasculature architecture of the liver enabled identification of the mass as a liver lobe, and coloured duplex ultrasonography confirmed the absence of blood flow within the mass. The diaphragmatic surface of the liver and the diaphragm itself were flattened. All other liver lobes and abdominal organs appeared normal on ultrasonography. Based on the non-specific clinical and laboratory findings, and the major ultrasonography findings in the liver, our differentials were LLT, lymphoma, liver neoplasia or metastasis. However, the sonographically normal liver pattern without any parenchymal changes was not consistent with neoplasia. Based on these findings, LLT was suspected. To confirm this diagnosis, an exploratory laparotomy was performed.

Lateral radiograph showing a moderate pectus excavatum (big arrow) and an abdominal mass (small arrows)
The cat was premedicated with dexmedetomidine (10 µg/kg, Dexdomitor; Pfizer) and methadone (0.1 mg/kg, Heptadon; Ebewe Pharma), and induced with propofol (2 mg/kg, Propovet; Vana). Anaesthesia was maintained with isoflurane (Vetflurane; Virbac) in oxygen and an intravenous bolus of fentanyl (2 µg/kg, Fentanyl; Janssen). The patient was placed in dorsal recumbency, and a cranial midline coeliotomy was performed. On entry to the abdomen, a sinistrodorsal inclination of the xyphoid cartilage and an approximately 180° counter-clockwise torsion of the left lateral hepatic lobe were visible, with no adhesions noted (Figure 2). The diaphragm was flattened owing to a shortened central tendon but otherwise showed normal ventral muscular development. A circumference strangulation ligature was made at the torsion site with monofilament suture (2/0 Monosyn; B Braun Melsungen AG), and the lobe was resected. The abdomen was closed routinely. Buprenorphine (10 μg/kg q8h, Bupaq; Richter Pharma) was administered for 24 h and meloxicam (0.1 mg/kg q24h, Metacam; Boehringer Ingelheim) for 7 days to provide postoperative analgesia. Clinically, the cat recovered well postoperatively and was discharged the following day. One week after surgery, the previous clinical abnormalities had resolved and the comprehensive blood test values normalised, with two exceptions (AST 89 IU/l; ALT 961 IU/l). These changes were likely caused by liver injury due to the LLT, but possible differentials include hypoxic damage; hepatolipidosis owing to the reported period of anorexia; and inflammatory hepatic injuries (hepatitis, cholangiohepatitis, pancreatitis, triaditis complex). Histological examination of the resected lobe revealed haemorrhagic infarction and multifocal areas of neutrophilic infiltration within the liver.
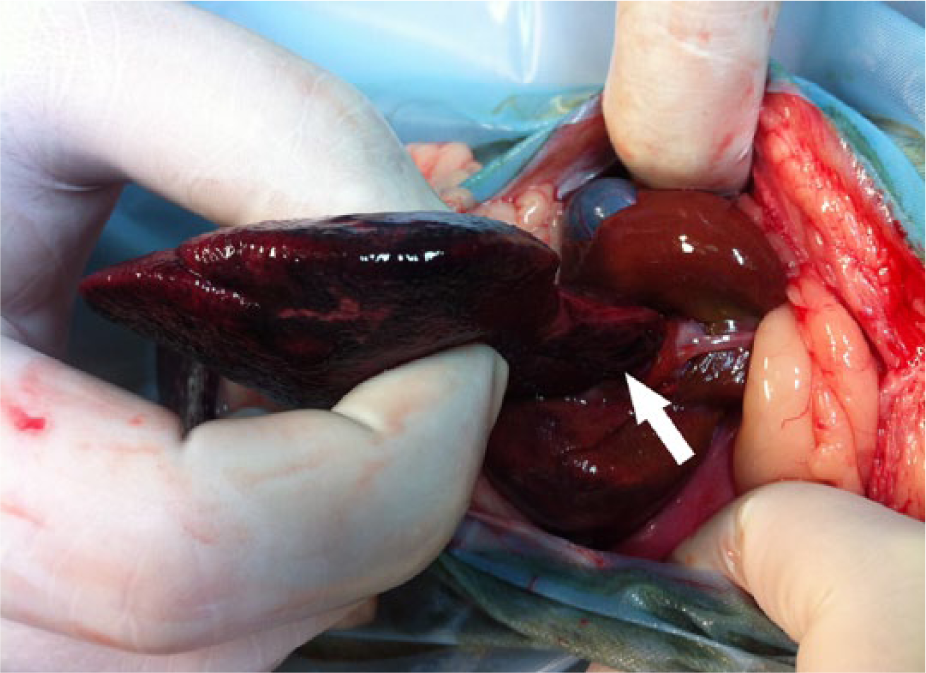
Intraoperative view showing torsion of the left lateral liver lobe (arrow)
On follow-up examination at 1 and 6 months postoperatively, the clinical appearance of the patient was unremarkable, and the serum biochemistry values were within normal limits. Surgical repair of the PE in a second surgery was considered but was declined by the owner owing to the lack of associated clinical signs.
Discussion
The clinical signs, physical examination and CBC findings in the present case were consistent with those documented in case reports of LLT in the veterinary literature; however, they were non-specific for the diagnosis of LLT.5,8 Although high serum hepatic enzyme activity indicates hepatic injury, these parameters are not limited to LLT. 5 The blood value changes normalised within 30 days, consistent with previous reports (10–60 days).5,7 Previously described radiographic findings of dogs with LLT were non-specific for the diagnosis of LLT, indicating that additional diagnostic modalities such as abdominal ultrasonography, computed tomography (CT) or exploratory surgery are required.5,7–9,12 In veterinary medicine, duplex ultrasonography and contrast CT have proved to be useful diagnostic tools for this purpose.7,8,12 In the present case, duplex ultrasonography effectively diagnosed LLT.
The most interesting aspect of the present LLT case was the simultaneous occurrence of PE. PE is generally congenital, but the exact underlying mechanism remains unknown.1,2,4 Common theories for its development include a thickened substernal ligament that helps in elevating the caudal sternum, a shortened central tendon and deficient muscular development of the ventral diaphragm. 4 Central tendon shortening, which reportedly results in a flattened diaphragm, 4 was observed intraoperatively in this case. In healthy dogs, the liver is tethered within the abdomen by ligaments. 13 Damage, congenital absence or laxity of these supporting structures reportedly predispose an animal to LLT.5,6,8,10,11 In theory, any liver lobe can twist on its pedicle; however, the left lateral lobe is believed to be predisposed because of its size and range of mobility, and because it is relatively separated from the other lobes.5,9 Including this case, the left lateral liver lobe is most commonly affected in both cats and dogs with LLT.5,6,8,9,14 In one feline case report, LLT was associated with liver neoplasia in the affected lobe. 5 In previous reports, hepatic masses were suspected to exert stress on the liver ligaments, causing their elongation and increased mobility of the liver lobes.5,8 However, a previous case series of 41 cats suffering from hepatic neoplasia did not report any case of LLT. 15 In the second feline case, LLT was also mass-associated, but the mass was suspected to be secondary to chronic LLT. 9 In the present case, no mass or related adhesions were present, but the left triangular ligament was stretched. We hypothesise that the flattened diaphragm induced by PE enabled excessive mobility of the liver lobes, subsequently causing elongation of the left triangular ligament and twisting of the liver lobe. However, anatomical changes in the liver ligaments were not found during necropsy in a previous feline case report of PE; 4 therefore, this needs to be addressed in future studies in order to prove this hypothesis. Clinical signs of trauma were not observed, and it remains unclear whether the LLT in this case was caused or promoted by trauma. In the present case, the untreated moderate PE did not cause any complications after liver lobe resection or generate any further clinical abnormalities.
Conclusions
The present case is the first known case of LLT with concurrent PE reported and the second feline case of LLT treated surgically. Animals with anatomical malformation of the diaphragm caused by PE may be at higher risk of developing LLT. Early diagnosis and surgical intervention of LLT can produce a positive clinical outcome without further repercussions.
Footnotes
Conflict of interests
The authors do not have any potential conflicts of interest to declare.
Funding
The authors received no specific grant from any funding agency in the public, commercial or non-profit sectors for the preparation of this case report.