
Abstract
Objectives
This study aimed to describe the length, internal and external diameters, cancellous bone volume and extent, and cortical thickness at predetermined locations in the radius and ulna of a cohort of skeletally mature, disease-free feline cadavers using radiography and computed tomography (CT).
Methods
Five feline cadavers were used (mean weight 3.31 kg, range 2.55–4.24 kg). Antebrachii (n = 10) were radiographed to confirm skeletal maturity and normal radiographic appearance prior to CT. Reconstructed CT images were used to measure bone length, cortical thickness, internal and external diameters, and cancellous extent. Cancellous bone volume was calculated automatically using OsiriX after manual segmentation (350–850 Hounsfield units window) from axial CT slices.
Results
CT images were used to measure bone length, cortical thickness, internal and external diameters, and cancellous extent and volume. Mean radial length was 95.89 mm (95% confidence interval [CI] 88.52–103.26 mm) and mean ulna length was 114.67 mm (95% CI 105.53–123.81 mm). The olecranon had the largest mean cancellous bone volume (94.16 mm3; 95% CI 72.09–116.23 mm3) and it extended a mean of 13.12 mm (95% CI 11.73–14.51 mm) distally. The radius at the level of the trochlea and the ulna at the level of the coronoid processes had the largest external diameters, respectively. The medullary canal narrowed at the level of the coronoid processes and became cranially eccentric at the proximal third of the diaphysis. The cranial cortex at the level of the coronoid processes and the caudal cortex of the olecranon were markedly thicker than other cortices at those levels.
Conclusions and relevance
Morphometry of the feline antebrachium was described using CT, and should be a useful reference for future research investigations and clinical applications.
Introduction
The anatomy and morphology of the feline antebrachium has been described,1–4 but bone morphometry has not. Bone morphometry is the measurement of quantitative three-dimensional properties of bone measured using manual or diagnostic imaging techniques.5–9 Morphometric analyses reported in normal dogs, cattle and humans are used as references for research into regional orthopaedic or neurological disease processes.5,7,8–13 The aim of this study was to describe the lengths, internal and external diameters, cancellous bone volume and extent, and cortical bone thickness at predetermined locations in the radius and ulna of mature cats. Radiography and computed tomography (CT) assessment was performed. Morphometric description of the feline antebrachium will provide information on the cortical and cancellous bone properties for future investigations, particularly orthopaedic research and clinical applications.
Material and methods
Cadavers
Four female skeletally mature cats of unknown desexing status, and one castrated male cat were euthanased for reasons unrelated to this study with intravenous sodium pentobarbital. Mean body mass was 3.31 kg (range 2.55–4.24 kg). The cadavers were kept frozen at −20°C and defrosted at room temperature prior to radiographic and CT imaging of their paired antebrachii.
Imaging
Radiographs of the forelimbs were obtained and reviewed by a board-certified radiologist to confirm normal radiographic appearance and skeletal maturity prior to CT. The cadavers were positioned by the same radiographer. Orthogonal radiographs (mediolateral and craniocaudal views) were obtained of each antebrachium. Each radiograph was centred over the mid-diaphysis of the antebrachium. The distal metaphysis of the humerus to the distal phalanges were included in the field of view. Radiographs were taken at 56 kVp and 3.2 mAs using a computed radiography system (CR X-35 AGFA system; Scoresby) and stored (AGFA IMPAX client; Scoresby) in a DICOM format.
CT (Emotion DUO; Siemens) was performed with the cadavers in sternal recumbency with both elbows extended and the olecranon in contact with and perpendicular to the gantry and the primary beam. The caudal aspect of the antebrachii were always in contact with the gantry, but remained unconstrained distally, as this would have altered the positioning of the elbow. The same foam positioning block was used for each cat. The foam block was placed under the mandible and between the humeri to provide a consistent distance between the limbs for all samples. The antebrachii of each cadaver were scanned from the phalanges to the distal metaphysis of the humerus. The parameters for each CT were as follows: 110 kVp, 100 mAs, 86 cm table height 0° gantry tilt, capture slice thickness 1.0 mm, 0.5 mm slice overlap, image matrix size 512 × 512 pixels and 0.95 mm focal spot. Fine bone and soft tissue window reconstruction algorithms were performed with a 0.5 mm slice thickness.
The DICOM images were stored for analysis.
Image analysis and data collection
Image analysis of the radiographic and CT DICOM images was performed by the same investigator using OsiriX (OsiriX 64 v 5.7.1, http://www.OsiriX-viewer.com/index.html). All measurements were taken in triplicate by the same investigator at the same time and the average of these three measurements was reported. The review sequence of the images was not randomised.
Each antebrachium was measured separately using multiplanar reconstruction (MPR) of the CT images acquired. The measurements were made from the two-dimensional images. The length of the radius was measured from the centre of the head of the radius (caput radii) to the most proximal aspect of the distal radial articular concavity in the saggital plane. The radial head measurements were taken from the first complete proximal radial axial slice through which all cortices of the head could be visualised when the axial images were oriented perpendicularly to the cranial cortex of the radius in the saggital plane. The centre of the radial head was defined as the point equidistant from the cranial and caudal cortices in the saggital plane. The radial diaphysis was divided into three levels at which measurements would be taken – the proximal third, mid-point and distal third. These levels were calculated for each radius, respectively, from the measured radial length using the technique described above. The proximal third level was located one-third of the calculated length of the radius, distal to the radial head. The mid-point level was located equidistant from the proximal and distal articular surfaces of the radius. The distal third level was located two-thirds of the calculated length distal to the radial head. The other measurement sites for the radius included the radial head, radial neck (collum radii) and trochlea (Figure 1a). The landmark for the radial neck was the narrowest point distal to the radial head and proximal to the radial diaphysis in the saggital plane. The landmark for measurement of the trochlea was the widest point passing through the radial styloid process in the frontal plane (Figure 1a). The length of the ulna was measured from the craniocaudal mid-point of the olecranon (tuber olecrani) to the most distal aspect of the styloid process in the sagittal plane. The olecranon measurements were taken from the first complete proximal ulna axial slice through which all cortices of the olecranon could be visualised when the axial images were oriented perpendicularly to the cranial cortex of the olecranon in the saggital plane. The craniocaudal mid-point of the olecranon was determined to be the point equidistant between the cranial and caudal cortices of the ulna in the saggital plane. The diaphysis of the ulna was measured at the calculated levels of the proximal third, mid-point and distal third, as for the radius. The other measurement site for the ulna was the proximal aspect of the medial coronoid process (processus coronoideus medialis) (Figure 1b). Internal diameter, external diameter and cortical thickness were measured at each of the described levels on the radius and ulna.

(a) Measurement levels for the radius, cranial view. 1 = head; 2 = neck; 3 = proximal third; 4 = mid-point; 5 = distal third; 6 = trochlea. (b) Measurement levels for the ulna, lateral view. 1 = olecranon; 2 = coronoid processes; 3 = proximal third; 4 = mid-point; 5 = distal third
Cortical thickness and internal diameter were measured along the radius and ulna separately using the standard OsiriX bone algorithm (window level: 300; window width: 1500). Measurement levels for the radius were the head, neck, proximal third, mid-point, distal third of the diaphysis and the trochlea (trochlea radii) at landmarks described above. Measurement levels for the ulna were the olecranon (tuber olecrani), coronoid processes (processus coronoideus), proximal third, mid-point and distal third of the diaphysis at landmarks described above. At each site on the respective bones the axial CT slice was manually oriented and marked using the region of interest tool to determine the relative cranial, caudal, medial and lateral aspects of the bones. This is a modification of methods previously described,14,15 and was performed to take into account the changing relative spatial relationship between the radius and the ulna with respect to the absolute craniocaudal and mediolateral planes. The internal diameter of the bone was measured along the same relative craniocaudal and mediolateral axes (Figure 2). The relationships between bone measurements were calculated by obtaining a percentage of the measured components for each cat. These percentages were then averaged for the cohort and confidence interval (CI) calculated.

Axial computed tomography slices. (a) Proximal third of the radius. (b) Middle of the radius. (c) Distal third of the radius. Top of images is cranial; left of images is medial. Radius is marked with cross-hairs. Solid orange = craniocaudal plane; solid blue = mediolateral plane; solid green = cranial and caudal cortical thickness; dotted light green = internal diameter in craniocaudal plane; solid red = medial and lateral cortical thickness; dotted light orange = internal diameter in mediolateral plane
Each axial CT DICOM image had cancellous bone manually segmented from other tissues using a window level of 350 and window width of 850 Hounsfield Units (HU) using OsiriX.16–20 The volume of cancellous bone was calculated automatically and recorded after segmentation of the DICOM images for each bone. 17 The proximal and distal extents of cancellous bone from the articular subchondral bone were measured using MPR after segmentation.
Results
Bone length
Bone length measured from CT had a mean of 95.89 mm (95% CI 88.52–103.26 mm) for the radius and 114.67 mm (95% CI 105.53–123.81 mm) for the ulna.
Cancellous bone
Cancellous bone extended a mean of 3.60 mm (95% CI 3.28–3.92 mm) distally from the articular subchondral bone of the radial head. The calculated cancellous bone volume of the radial head was a mean of 13.13 mm3 (95% CI 9.35–16.91 mm3).
The cancellous bone of the distal radius extended a mean of 10.37 mm (95% CI 9.72–11.02 mm) from distal articular surface. The total calculated cancellous bone volume of the distal radius was a mean of 76.88 mm3(95% CI 62.15–91.61 mm3).
Cancellous bone extended a mean of 13.12 mm (95% CI 11.73–14.51 mm) distally from the olecranon. The total calculated cancellous bone volume proximal ulna was a mean of 94.16 mm3 (95% CI 72.09–116.23 mm3).
The cancellous bone of the distal ulna extended a mean of 10.71 mm (95% CI 9.71–11.71 mm) from the styloid process. The mean total calculated cancellous bone volume of the distal ulna was 17.49 mm3 (95% CI 13.79–21.19 mm3).
External diameter of bone
The external diameters of the radius and ulna at the measurement levels are reported in Tables 1 and 2, respectively.
Computed tomography external diameter measurements of the radius at the measurement levels reported as mean (95% confidence interval)

CC = craniocaudal; ML = mediolateral
Computed tomography external diameter measurements of the ulna at the measurement levels reported as mean (95% confidence interval)

CC = craniocaudal; ML = mediolateral
The radial head was ovoid in shape. The mean craniocaudal plane external diameter was 63% of the mediolateral plane. The radial neck was narrower than the head in both planes. The neck was, on average, 85% and 81% of the radial head in the craniocaudal and mediolateral planes, respectively. The external diameter of the radial diaphysis varied little throughout its length. The radial trochlea was the widest part of the radius in both planes, and was, on average, 133% and 130% wider in the craniocaudal and mediolateral planes compared with the radial head, which was the next widest part.
The olecranon’s mediolateral external diameter was, on average, 46% of its craniocaudal plane. The level of the coronoid processes represented the widest external diameter on the ulna in both planes, respectively. Throughout the ulna diaphysis, the external diameter remains widest in the craniocaudal plane, and narrows consistently from the proximal third to the distal third.
Internal diameter of bone
The internal diameters of the radius and ulna at the measurement levels are reported in Tables 3 and 4, respectively.
Internal diameters of the radius at the measurement levels reported as mean (95% confidence interval)

CC = craniocaudal; ML = mediolateral
Internal diameters of the ulna at the measurement levels reported as mean (95% confidence interval)

CC = craniocaudal; ML = mediolateral
The radial head’s mean internal diameter was, on average, 216% wider in the mediolateral axis than the craniocaudal. The internal diameter tapered by approximately 2 mm through the radial neck in the mediolateral axis but changed little in the craniocaudal axis before joining the diaphysis. The radial medullary canal remained mostly ovoid throughout its length, but narrowed midway to a mean of 1.58 mm (95% CI 1.07–2.09 mm) in the craniocaudal axis before flaring out again to a mean of 1.82 mm (95% CI 1.26–2.38 mm) at its distal third. The mean mediolateral internal diameter of the radial diaphysis was 2.50 mm (95% CI 1.71–3.28 mm) at the proximal third, which widened by an average of 117% between the proximal third and mid-point, and by 110% between the mid-point and the distal third. The internal diameter of the radial trochlea was consistently the widest point in both mediolateral and craniocaudal planes.
The caudal ulna surface in the cat was convex from proximal to the mid-shaft and then concave distally. The internal diameter of the ulna at the olecranon was widest in the craniocaudal axis. The mediolateral internal diameter at the olecranon was on average 40% of the craniocaudal measurement. The medullary canal narrowed at the level of the coronoid processes to a more ovoid shape (viewed in cross section) and measured a mean of 3.16 mm (95% CI 2.57–3.75 mm) craniocaudally and 2.37 mm (95% CI 1.91–2.82 mm) mediolaterally. The mediolateral internal diameter at the proximal third of the ulna diaphysis was, on average, 44% of the craniocaudal plane. At this level of the diaphysis, the medullary canal was cranially eccentric. The medullary canal widened distal to the proximal third of the ulna by a mean of 145% at the mid-point and 134% at the distal third of the ulna in the mediolateral plane. In the craniocaudal plane, the internal diameter of the diaphysis tapered gradually. The mid-point was, on average, 90% of the proximal third internal diameter. The mean distal third internal diameter was 79% of the mid-point internal diameter and 70% of the proximal third, respectively.
Cortical bone thickness
The cortical thicknesses of the radius and ulna at the measurement levels are reported in Tables 5 and 6, respectively.
Cortical thickness of the radius at the measurement levels reported as mean (95% confidence interval)
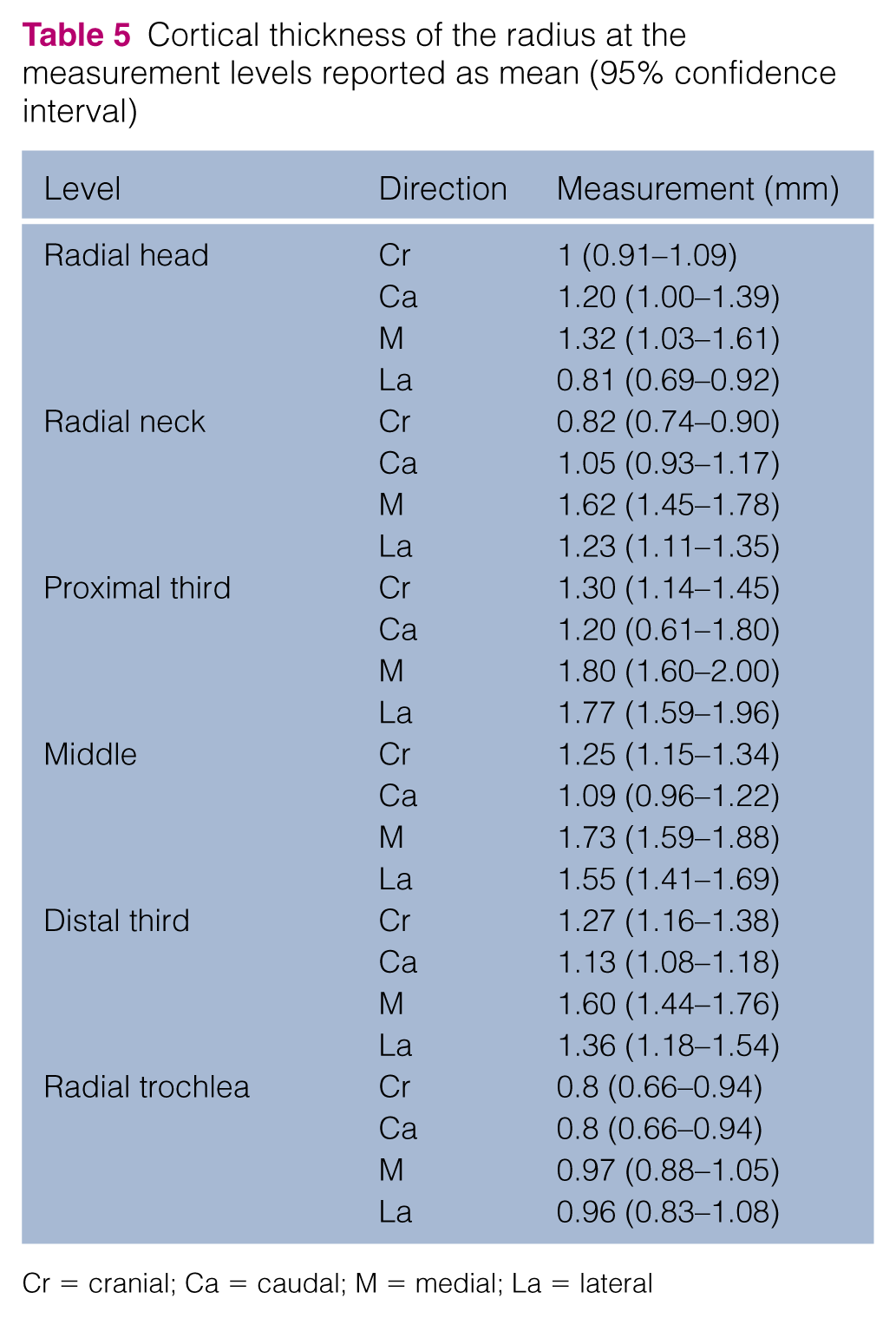
Cr = cranial; Ca = caudal; M = medial; La = lateral
Cortical thickness of the ulna at the measurement levels reported as mean (95% confidence interval)

Cr = cranial; Ca = caudal; M = medial; La = lateral
The radial head caudal and medial cortices were thicker than the cranial and lateral cortices. The radial neck had thicker medial and lateral cortices than the cranial and caudal cortices. The medial and lateral cortices were consistently thicker throughout the radial diaphysis and radial trochlea compared with the cranial and caudal cortices at each respective level.
The olecranon cortices were relatively similar thicknesses, except for the caudal cortex, which was at least a mean of 241% thicker than the rest. The cranial cortex at the level of the coronoid processes were, on average, 150% thicker than the caudal cortex and 390% and 132% thicker than the medial and lateral cortices, respectively. The caudal cortex at the level of the proximal third of the ulna diaphysis was the thickest. It was a mean of 168% thicker than the cranial cortex and approximately three times as thick as the medial and lateral cortices. At the middle of the ulna diaphysis, the caudal cortex was a mean of 203% thicker than the lateral cortex and 176% thicker than the cranial cortex, respectively. The caudal cortex was a mean of 171% thicker than the medial cortex. The cranial cortex at the distal third of the ulna diaphysis was a mean of 142%, 122% and 142% thicker than the lateral, medial and caudal cortices, respectively.
Discussion
We documented the lengths, internal and external diameters, cancellous bone volume and extent, and cortical bone thicknesses in the feline radius and ulna using CT in a cohort of normal cats. Anatomical texts only describe the surface anatomy of the domestic feline antebrachium,1,2,4,21 and although previous studies have compared the length of the radius and ulna of domestic cats with those of other felids,15,22 none have described the morphometry of the feline antebrachium or the volume and distribution of the cancellous bone using CT. CT measurement of bones using OsiriX MPR has previously been validated as an accurate and repeatable measurement tool that was non-inferior to digital Vernier calliper measurements of bone manually.6,23 Those studies were performed using 16 and 256 slice CT machines capable of isotropic resolution in reformatted multiplanar images and may not be replicated in less advanced machines. A study on the agreement and repeatability of single-slice CT imaging in measuring vertebral body lengths in three canine cadavers compared with calliper measurements found that vertebral body length measured from single-slice CT images overestimated vertebral body length by a mean 2.2 mm when compared with callipers. 24 That study was limited in that only three dogs were measured. Furthermore, the CT images obtained in that study had a slice thickness of 4 mm with no slice overlap, which limited the spatial resolution and increased the effect of partial volume averaging. In contrast, our study utilised a slice thickness of 1 mm with an overlap of 0.5 mm, which has previously been demonstrated to decrease the effects of partial volume averaging.25,26 Similar technology has been used to accurately assess CT reconstructions of joint spaces in the canine elbow, which strongly agreed with frozen section calliper measurements, with a mean variation of 0.15 mm. 27
Our findings were similar to reports in anatomical texts,1,2,4,21 which showed that cancellous bone distribution was concentrated around the metaphyses of the radius and ulna in cats. There were considerable volumes of cancellous bone in the distal radius and proximal ulna. Interestingly, there was almost a cm of cancellous bone extending from the ulna styloid process, although this still represented a small volume of cancellous bone. Inserting intramedullary pins into this distal ulna cancellous bone may be clinically useful. It has been proposed that cancellous bone provides a high friction, high surface area pin–bone interface that may decrease the risk of pin loosening and migration.28,29
We found the cancellous bone volume in the radial head was small compared with the other metaphyseal regions measured, and extended only 3.60 mm (3.28–3.92 mm) from the articular surface, which corresponds to the start of the radial neck. The radial neck is small but rather prominent in cats and attaches the head to the shaft of the radius in cats. It is located a few mm distal to the radioulnar (articulatio radioulnaris proximalis), humeroulnar (articulatio humeroulnaris) and humeroradial (articulatio humeroradialis) joints. The distal border of the radial neck was delineated by the radial tuberosity (tuberositas radii), which flared from the caudolateral aspect of the bone and represents the insertion point of the biceps brachii muscle.1,2
The cortical thickness of the radius was relatively homogeneous throughout its length. For the orthopaedic surgeon, this finding suggests that in mature cats, the radial diaphyseal cortices should provide predictable and consistent purchase for orthopaedic implants along its entire length. In contrast, ulna cortical thicknesses varied markedly by location, which is likely a reflection of the shape of the ulna and insertions of soft tissue attachments. It has been shown that areas of cortical and trabecular bone under dynamic physiological loads, such as subchondral bone and ligamentous or tendinous insertions have the capacity to remodel in response to use.30,31 Trabecular bone remodels in response to forces acting on the bone in accordance with Wolff’s law.32,33 We have observed that the cortices of the feline antebrachium were generally thicker in regions of high dynamic loads and points of ligamentous or tendinous attachments. The olecranon cortical thicknesses were similar except for the caudal cortex, which was at least a mean of 241% thicker than the other cortices and coincides with the insertion point of the triceps tendon, which is subjected to higher tensile forces. The cranial cortex at the level of the coronoid processes was a mean of 150% thicker than the caudal cortex, and a mean of 390% and 132% thicker than the medial and lateral cortices, respectively. We observed that the caudal cortices of the ulnar diaphysis were generally thicker than the other cortices. This finding is likely representative of the triangular cross section of the ulna at these levels, which has its apex caudally and is the origin of the ulnar head of the deep digital flexor (musculus flexor digitorum profundus, caput humerale) muscle.1,2,4,21
This study was a preliminary descriptive study of the feline antebrachial morphometry and has several limitations. The data reported here are representative of a specific cohort of cadaveric, mature, domestic shorthair cats, and does not provide findings for juvenile or geriatric cats. Data from other cohorts are expected to be different and thus age may create distinctive cohorts for comparison. Our data will provide anatomic information useful to researchers, particularly for orthopaedic research on mature cats. Visual and radiographic inspection of the animals prior to inclusion in this study eliminated animals with skeletal disease or that were immature. All of the cats used in this study were skeletally mature but the exact age, reproductive and nutritional status were not known. These factors can affect bone quality, bone development and cancellous bone volume, and is a limitation of this study.
Previous studies looking at the effect of gonadectomy on cat skeletal development are contentious. One study found no significant differences between the sexes or between the time of gonadectomy on the mature length of the radius, although physeal closure was delayed in gonadectomised animals. 34 Another study found that gonadectomised cats had longer radial lengths compared with intact controls at 24 months of age. 35 All of the cats used in this study were skeletally mature, and although the reproductive status of the female cats was unknown, this may have contributed some variability to our results.
It has been reported that cats have a paw preference, similar to handedness in people.36–40 It is feasible then, that continual preferential use of a limb may affect bone quality and size; however, this effect is likely to be insignificant in normal cats that weight bear symmetrically between left and right sides. Previous studies on paw preference in cats have used reaching tests to determine the effect of sex on limb use with conflicting and contradictory results,38–40 which suggests that the effect is small, if present at all. One kinetic study of cat limb use measured by a pressure-sensitive mat found that there was no significant difference between males and females on preferential use of left or right limbs. 41 The study also found that while males had longer limbs, which correlated with longer stride length, it was cat body size and not sex that influenced limb use. Therefore, the physical size of the cats in this study, rather than sex, ‘handedness’, reproductive or nutritional status, should be considered the most important physical modifier of limb length, although these attributes undoubtedly contribute to each individual’s phenotype. Without knowing the history of each cat, it would be difficult to speculate on the effect of these attributes on the measurements obtained in this study. While the number of cats in this study was small, there was no difference between left- and right-sided measurements, and, as such, the data were pooled to describe the bone morphometry for this cohort. Attempts at discerning left- and right-sided differences were not made as there is no reason to believe it would be different, and without knowing any paw preference of the cats, this would be a presumptive, arbitrary division at best.
The data reported are absolute measurements rather than a normalised proportion, which makes interpretation and extrapolation straightforward and of use for future reference. While it would have been feasible to normalise the data to a specific regional structure (eg, vertebral length) or measurement such as weight, we believe that the utility of the data would have been limited by such manipulation.
One technical limitation of this study was the CT slice thickness. We found that a reconstructed 0.5 mm CT slice limited resolution of the subchondral bone owing to the adjacent anatomy and curvature of the articular surfaces. Micro-CT would offer slice thickness as small as 40 µm and has been used in cats to study auditory ossicles in situ. 42 This modality could have facilitated the accuracy of measuring the juxta-articular bone diameter.
Obtaining bone density measurements would have enhanced our study. Although dual-energy x-ray densitometry has been performed in cats with metabolic and storage disease,43,44 there are currently no data for normal cats.
Conclusions
Our study has described the lengths, internal and external diameters, cortical bone thickness, and bone volume and extent for the radius and ulna from a cohort of mature feline cadavers. Our morphometric description of the radius and ulna provides information that can serve as a useful reference for future studies into regional anatomy and pathology, or for orthopaedic research and clinical applications.
Footnotes
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
Funding for this research was provided as part of the Research Masters with Training postgraduate scholarship from Murdoch University.