
Abstract
Hyperextension injury to the feline carpus usually results in disruption of the palmar ligament support at the level of the carpometacarpal joint. Treatment options include pancarpal or partial carpal arthrodesis. Partial carpal arthrodesis preserves range of motion of the antebrachiocarpal joint, and pronation and supination of the forearm. The surgical technique and three cases of partial carpal arthrodesis using medially applied mini-plates are described. Partial carpal arthrodesis of the feline carpus using medially applied mini-plates may be a safe and effective treatment for hyperextension injury to the carpometacarpal joints.
Introduction
Carpal hyperextension injury is occasionally encountered in cats and is usually due to a fall from height. It is a result of disruption of the palmar ligament support. The level of injury in most cases is the carpometacarpal joints; however, the antebrachiocarpal and intercarpal joints may be affected. Treatment options include pancarpal and partial carpal arthrodesis. Pancarpal arthrodesis is indicated for hyperextension injuries involving the antebrachiocarpal joint. Either pancarpal or partial carpal arthrodesis may be elected for injuries involving the middle carpal and carpometacarpal joints. Case reports and clinical outcome studies of carpal arthrodesis procedures are scarce in cats and have focused on pancarpal arthrodesis.1–4 Long-term functional outcome in 18 cats with pancarpal and two cats with partial carpal arthrodesis was found to be satisfactory or excellent based on owner assessment but minor disabilities in jumping and climbing were commonly reported. 4 Both cats with partial carpal arthrodesis were reported to have an excellent outcome. 4
Partial carpal arthrodesis has the advantage over pancarpal arthrodesis of not only preserving range of motion of the antebrachiocarpal joint, but also allowing pronation and supination of the forearm. The latter seems to be functionally important in cats as the range of motion in pronation and supination is larger (115°) than in dogs (50°). 5 In dogs, reported surgical techniques to achieve partial carpal arthrodesis include cross pinning, intramedullary pinning, dorsal plating and medial plating.6–11 The small size of the carpal and metacarpal bones in cats limits implant options and there are currently no detailed descriptions of surgical technique for, and outcome following, partial carpal arthrodesis in cats. We report the use of medially applied mini-plates to achieve partial carpal arthrodesis in three cats with hyperextension injury of the carpometacarpal joint.
Case descriptions
Three cats with carpometacarpal hyperextension injury were treated by performing partial carpal arthrodesis using a medially applied mini-plate. The first patient was a 15-year-old female spayed domestic longhair cat with a body weight of 3.9 kg. The injury occurred when the cat got its left manus trapped in a closing door 1 day prior to presentation. The second cat was a 1.5-year-old female spayed domestic shorthair cat weighing 3.3 kg that had sustained a right carpometacarpal hyperextension injury due to an unknown trauma 9 days earlier. The third cat was a 9-year-old male neutered Burmese cat with a body weight of 5.0 kg. This cat sustained a left carpometacarpal hyperextension injury due to falling from a first floor balcony. It also had degenerative joint disease of the left elbow joint.
Hyperextension of the carpal joint was evident on palpation in all cats and was associated with swelling and pain. Stressed radiographs performed under general anaesthesia revealed dorsal deviation of the metacarpal bones relative to the distal carpal bones in all cats, indicating hyperextension injury at the level of the carpometacarpal joint (Figure 1). The first cat had concurrent fractures of the second and third carpal bones. The antebrachiocarpal joint was deemed unaffected in all three patients.

Lateral radiographic projection of the left manus of case 3. Dorsal stress has been applied to the paw to allow identification of instability at the level of the carpometacarpal joint
All cats were premedicated with an intramuscular injection of medetomidine (10 μg/kg) and methadone (0.3 mg/kg). Induction was achieved using alfaxalone intravenously to effect, and anaesthesia was maintained with isoflurane in oxygen via an endotracheal tube. The forelimb was clipped with a number 40 blade proximal enough to allow access to the proximal humerus for autogenous cancellous bone graft harvest. A brachial plexus block was performed using 1 mg/kg bupivacaine. The cats were placed in dorsal recumbency, and a hanging leg preparation using chlorhexadine and alcohol was performed. Perioperative cefazolin (30 mg/kg IV) was administered during limb preparation and continued at 90 min intervals throughout the surgery. A tourniquet was not used in any of the surgeries.
The cat was moved into theatre and the affected limb was free draped so that the proximal humerus was accessible. The proximal humerus was approached via a craniolateral incision through the skin and subcutaneous tissue. The acromion head of the deltoid was retracted caudally exposing the craniolateral metaphysis. A hole was drilled through the cortical bone and cancellous bone was collected using a small curette. The cancellous bone graft was stored on a saline-soaked gauze until it was required for the arthrodesis.
A medial skin incision was performed from the medial styloid process of the radius to the base of the second metacarpal bone, dorsal to the first digit. The tendon of the abductor pollicis longus muscle was identified and used as a proximal and palmar landmark. The deep tissue and joint capsule were sharply incised with a number 15 scalpel blade, longitudinal to the limb, to expose the middle carpal and carpometacarpal joints. Care was taken to preserve the medial collateral ligament of the radiocarpal joint, which courses in a cranioproximal to palmarodistal direction below the tendon of the abductor pollicis longus muscle. 6 The dorsal joint capsule of the carpometacarpal joints was further incised horizontally, as lateral as the exposure allowed. Hyaline cartilage in the carpometacarpal and middle carpal joints was debrided with a small bone curette or pneumatic burr. Access to the fourth carpometacarpal joint was difficult and it was not possible to access the fifth carpometacarpal joint, resulting in an in-ability to debride the articular cartilage at this locale. The previously collected autogenous cancellous bone graft was placed in the joint spaces of the carpometacarpal and middle carpal joints.
A five-hole mini-plate was applied medially so that one screw could be inserted into the radial carpal bone, one screw through the distal carpal bones and three screws into the metacarpal bones (Figure 2). The proximal end of the plate was positioned just dorsal to the articulation of the first digit and the insertion of the abductor pollicis longus tendon. The first screw was inserted into the radial carpal bone and the second screw into the base of the metacarpal bones before the other screw holes were filled. The proximal metacarpal screws were aimed to engage at least two metacarpal bones, the most distal screw just the second metacarpal bone. In the first case, a 1.5 mm veterinary cuttable plate was used with 1.5 mm screws. In the other two cases, a 1.7 mm titanium hand plate (Stryker) was combined with 1.3 mm screws, also from a hand set (Synthes) (Figure 3). Postoperative radiographs revealed adequate implant positioning in all cases with no violation of the radiocarpal joint.
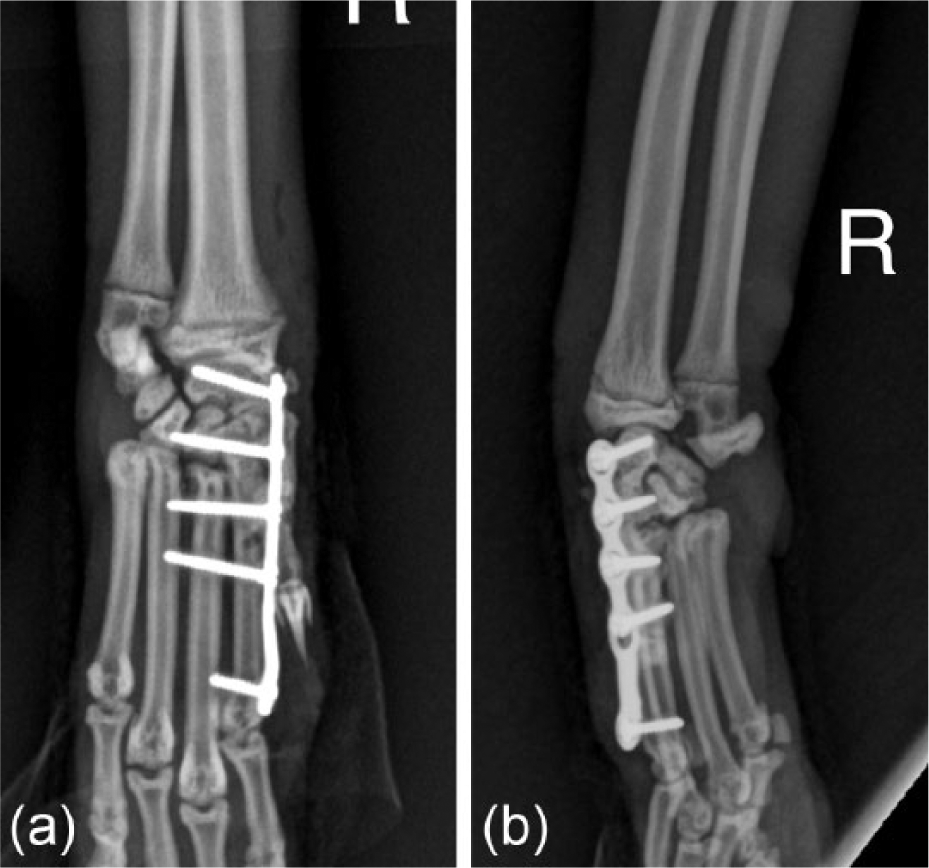
(a) Dorsopalmar and lateral postoperative radiographs of case 2 illustrating implant positioning. (b) Dorsopalmar and lateral postoperative radiographs of case 2 illustrating implant positioning

A range of mini-plates considered suitable for medial application to the feline carpus. From left to right: 1.5 mm veterinary cuttable plate, Stryker 1.7 mm titanium hook plate (modified by removing the hook), Synthes 1.3 mm finger plate
All cats were placed on intravenous Hartmann’s solution at induction and remained on fluids until they were eating postoperatively. A splinted bandage was applied to all cats for 5–7 weeks. All cats received a course of cephalexin for 5–20 days. Analgesia was provided using methadone or buprenorphine injections as needed while in hospital, and buccal buprenorphine and/or oral meloxicam for 3–5 days following discharge. The cats were discharged between 3 and 9 days after surgery. In two cats moderate swelling of the foot occurred postoperatively, necessitating daily bandage changes initially. Thereafter, bandages were changed weekly.
Follow-up examinations and radiographs were performed after 5–7 weeks, prior to removal of the splinted bandage, and again after 3 months in one cat. Carpal hyperextension could not be elicited in any of the cats. Carpal range of motion in flexion was only noted in the medical records for one cat where it was reported to be 90°. Implants remained stable on all follow-up radiographs. Bony fusion was incomplete in all cases at 5–7 weeks, but was more advanced at 3 months in the cat with later radiographs (Figure 4). There was a tendency for only the medial aspect of the carpometacarpal joint to fuse. Only metacarpal II was fused to the distal carpal bones in the cat with radiographs 3 months postoperatively.

(a) Dorsopalmar and lateral radiographic projections of case 3 at 12 weeks postoperatively. Note the failure to achieve bony fusion on the lateral aspect of the intercarpal and carpometacarpal joints. (b) Dorsopalmar and lateral radiographic projections of case 3 at 12 weeks postoperatively. Note the failure to achieve bony fusion on the lateral aspect of the intercarpal and carpometacarpal joints
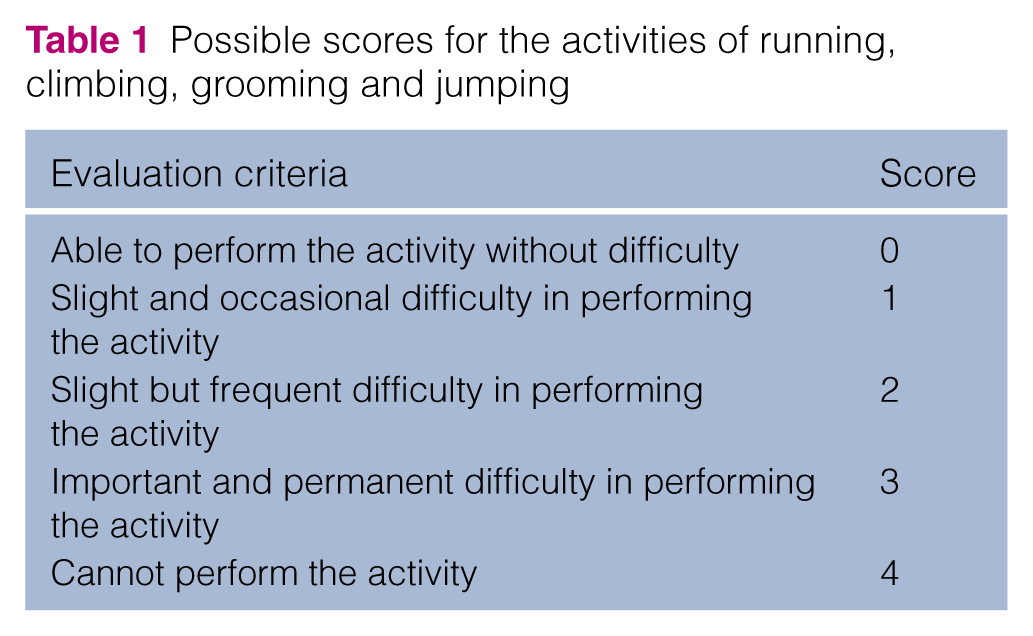
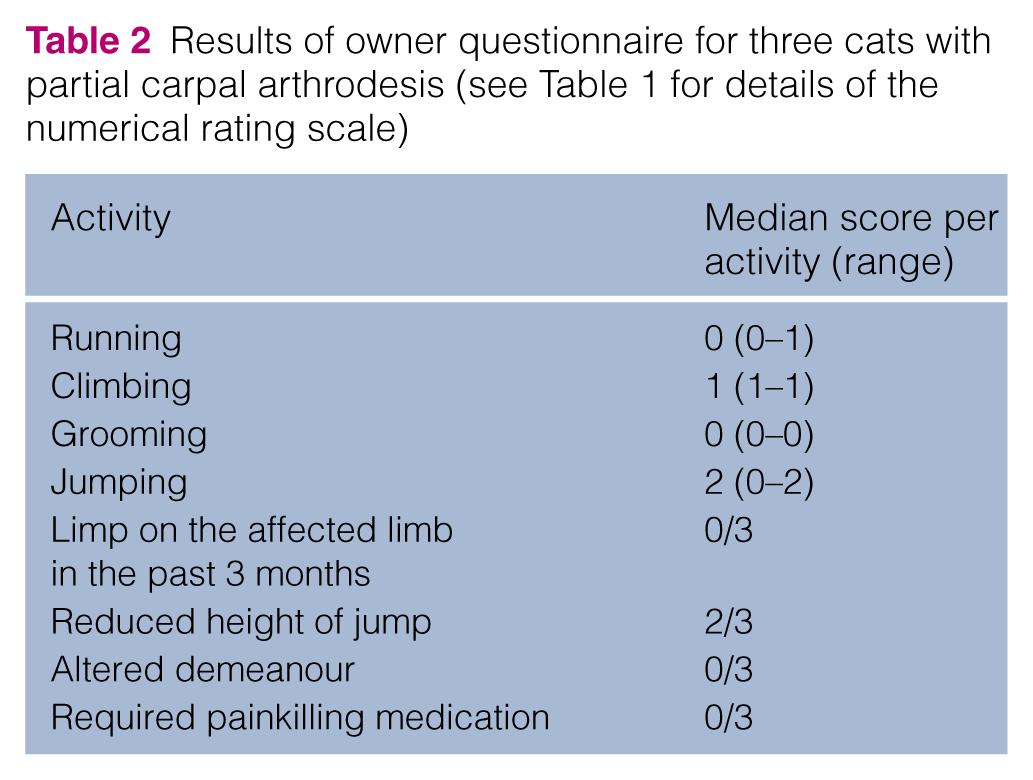
Owner-assessed long-term functional outcome was evaluated via a telephone questionnaire. The first cat had died 11 months after surgery, as a result of unrelated causes, 1 year prior to the telephone call. The other two cats were still alive at the time of questioning (12 months postoperatively). Questions from a previously used questionnaire were used to obtain the owner-perceived scores regarding the activities: running, climbing, grooming and jumping (Table 1). 4 The median scores for each activity are summarised in Table 2. Additionally, owners were asked whether they had observed a limp in the affected front leg in the past 3 months, whether they perceived a reduced height of jump, an altered demeanour (eg, aggression, seeking seclusion, resentment of handling) and whether the cat required painkilling medication. Reduced height of jump was reported in two cats. The answer to all other questions was no. All owners would have the surgery performed again. A cumulative score of <2 was considered to be an excellent outcome, and a cumulative score of ≥2 was considered satisfactory. Based on the results of the owner questionnaire, two cats were considered to have a satisfactory outcome and one cat was considered to have an excellent outcome.
Possible scores for the activities of running, climbing, grooming and jumping
Results of owner questionnaire for three cats with partial carpal arthrodesis (see Table 1 for details of the numerical rating scale)
Discussion
A satisfactory-to-excellent outcome after partial carpal arthrodesis for treatment of carpometacarpal hyperextension injury using a medially applied mini-plate was observed in this small case series of three cats. Intraoperative or postoperative implant-related complications were not observed.
Reports of carpal arthrodesis techniques in the feline literature are limited to pancarpal arthrodesis, and include one cat with a dorsally applied 1.5 mm mini- plate, three cats with a medially applied 2.0 mm locking plate, one cat with arthrodesis wire and external skeletal fixation, and 18 cats predominantly treated with dorsal plates (veterinary cuttable plates, dynamic compression plates, hybrid pancarpal arthrodesis plates) or crossed pins.1–4 Outcome after pancarpal arthrodesis in cats has been described as satisfactory-to-excellent using subjective outcome evaluation and owner questionnaires. Reported problems included limited ability to jump and climb, minor gait abnormalities and changes in demeanour. 4 Complications occurred in 25% of the cats with pancarpal arthrodesis. 4 In the previously reported cases, pancarpal arthrodesis was performed to treat carpometacarpal injuries where partial carpal arthrodesis could have been possible.1,4
Complications associated with external coaptation or bandaging are commonly reported in cases of carpal arthrodesis. 12 All cats in this case series had a splinted bandage applied for between 5 and 7 weeks. In one case bandage complications resulted in pressure sores and dermatitis that required antibiotic therapy. In this case the course of cephalexin was continued for 20 days postoperatively.
Pancarpal arthrodesis does not only eliminate flexion and extension of the carpus, but also interferes with supination and pronation of the forearm. Cats have a higher range of motion in supination and pronation than dogs and use this during playing, climbing and grooming. 5 Although it would seem important to maintain the most physiological function, only two cats with partial carpal arthrodesis have been described in the veterinary literature to our knowledge; these were included in the study by Calvo et al. 4 Both cats received partial carpal arthrodesis with cross pins and both were reported to have an excellent outcome despite complications such as pin migration and metacarpal fracture. It is possible that surgeons tend to choose pancarpal over partial carpal arthrodesis owing to fear of previously reported suboptimal limb function and development of antebrachiocarpal osteoarthritis after partial carpal arthrodesis in dogs. 9 However, other studies in dogs have shown favourable results following partial carpal arthrodesis.8,11,13 In a clinical study of 45 dogs with partial carpal arthrodesis, 70% of dogs returned to full function. 8 Objective outcome evaluation in dogs using force plate analysis has shown no difference in vertical limb loading between dogs with partial carpal and pancarpal arthrodesis. 13
It is also possible that partial carpal arthrodesis is uncommonly performed in cats owing to the small size of bones and the perceived difficulty of inserting implants that are rigid and stable enough. Pinning techniques, such as cross pinning or intramedullary pinning, can be used but pin migration is a common complication.4,11 Intramedullary pinning involves insertion of intramedullary pins into the metacarpal bones in a distal to proximal direction, followed by advancing the pins across the distal and middle carpal joint until they are seated within the radial carpal bone. Inserting the pins into the medullary cavities of the metacarpal bones without going through the transcortex of the metacarpal bones or the radiocarpal joint is technically demanding and pin size is limited by the small diameter of the intramedullary canal of feline metacarpal bones. Dorsal plating, arguably the most commonly used technique for partial carpal arthrodesis in dogs, would likely result in interference of the proximal end of the plate with the distal radius due to the small height of the radial carpal bone.
Medial plating has been described in dogs and cats for pancarpal arthrodesis.2,14 Applying a plate medially has the biomechanical advantage of the plate being loaded along its width. This increases the area moment of inertia and therefore the resistance to bending compared with a dorsally applied plate. Medial plating for partial carpal arthrodesis also avoids the risk of the proximal end of the plate irritating the antebrachiocarpal joint during extension. These were the reasons we chose to apply the plates on the medial aspect of the carpus in these cases. It was also hypothesised that the medial approach might spare the soft tissue from extensive dissection, which may decrease postoperative swelling and aid in healing of the arthrodesis.
Simpson and Goldsmid measured the dimensions of the feline distal radius, carpal and metacarpal bones to estimate screw sizes for dorsal plating in pancarpal arthrodesis. 1 In that study the third metacarpal bone had a mean mediolateral dimension of 3.68 mm and the authors concluded that a 1.5 mm diameter screw is the upper threshold for safe insertion. 1 The dorsopalmar width of the metacarpal bones is narrower than the mediolateral width so we elected to use 1.3 mm screws from a human hand set in two of the described cases.
Mini-plates with a small distance between plate holes must be used to be able to position screws appropriately. Spacing of the plate holes of three different mini-plates is shown in Figure 3. The 1.5 mm veterinary cuttable plate and the 1.3 mm Synthes hand plate have a very similar hole spacing, which is slightly less than in the 1.7 mm Stryker hand plate. Although the spacing of the plate holes is appropriate for the described use in all plates, the 1.3 mm Synthes hand plate is palpably weaker than the other two plates and was therefore not used. All three plates can be used with the 1.3 mm screws of the Synthes hand set if their designated screws are considered inappropriately large for the bone diameter. This claim is not substantiated by any biomechanical data but only based on clinical experience with the two cases described here and other use of the 1.5 mm veterinary cuttable plates with 1.3 mm screws for other indications.
The major limitation of this technique is that it is very difficult, if not impossible, to access and debride the articular cartilage at the lateral aspect of the feline carpus via the described medial approach. The consequence of this inability to debride the articular cartilage laterally was apparent on postoperative radiographs where bony fusion was only observed on the medial aspect of the joint. Clinically, this did not seem to cause any adverse effects; however, concern as to whether the limited medial carpal arthrodesis achieved in this case is robust enough in the long term remains. Ideally, a more extensive arthrodesis would have been achieved. When evaluating why a more extensive arthrodesis did not occur, the principles of arthrodesis (that is the removal of all articular cartilage, stable fixation and the provision of autogenous bone graft), need to be considered. 15 In the reported cases, difficulty accessing the articular surface of the fourth and especially the fifth carpometacarpal joints was experienced. This inhibited removal of the articular cartilage in these joints and was likely the reason that arthrodesis was not achieved in these locales. Exposure of these joints may be improved by locating the medial skin incision more dorsally to allow improved access to the carpometacarpal joints or by approaching the lateral aspect of the carpus through a limited lateral approach.
Failure to provide stable fixation across the carpometacarpal joints may also be a reason why the arthrodesis was not achieved in the lateral joints. In the case that had 12 week radiographs available, there is only a single screw engaging metacarpal III. This may not have provided sufficient stability to allow arthrodesis to occur at the third carpometacarpal joint. This may highlight a need to engage this metacarpal with more than one screw. In the other two cases this was achieved but the limited radiographic follow-up does not allow us to comment on whether this difference in implant positioning improved this feature of the arthrodesis. All of the cases had autogenous cancellous bone graft placed within the joint spaces, fulfilling this principle.
A major limitation of this case series is the limited radiographic follow-up. Follow-up radiographs were performed 5–7 weeks postoperatively at splint removal. As expected, there was no radiographic evidence of osseous union at this time. Limb alignment, bone apposition, implant position and implant integrity are the only factors that could be realistically assessed at this time point. Healing in a feline arthrodesis case could not be expected to have progressed to the point of radiographic union in this time period. More extensive radiographic follow-up was unable to be obtained owing to one cat dying and another moving to a different state. Without radiographic follow-up we cannot be sure that the treatment resulted in an arthrodesis rather than a stable ankylosis. However, no reports of implant complications were received on owner questioning 1 year postoperatively.
Conclusions
At approximately 1 year after surgery owners reported a satisfactory-to-excellent outcome after partial carpal arthrodesis using a medially applied mini-plate. No lameness, no change in demeanour, and normal grooming and running activities were observed. Owners reported a decreased ability to jump, characterised by a reduced height of jump and, on occasion, difficulty climbing. This is similar to what was previously reported following pancarpal arthrodesis. 4 Although the perception and satisfaction of owners is an important outcome measure, the ability to perform specific activities, such as the ability to pronate and supinate the affected paw, may not be recognised through questionnaires. More cases with longer clinical and radiographic follow-up times are needed to evaluate fusion, carpal range of motion and complication rates. Only bandage-related complications were experienced in this small case series. The duration of bandaging was extrapolated from recommendations in dogs but shorter bandaging times would reduce the risk of complications and potentially help maintain carpal range of motion.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case series.
Conflict of interest
The authors do not have any potential conflicts of interests to declare.