
Abstract
The main aim of this retrospective study was to describe clinical and histopathological findings in cats with mucogingival lesions developed at the contact point of the premolar and molar teeth of the opposite quadrant. Cases were retrieved following manual review of the medical records, dental records and photographic documentation of all feline dental patients visited in the period between February 2001 and August 2011. Cats showing different lesions at different times were calculated as multiple cases. A total of 27 cats (31 cases) with 44 lesions (26 proliferations [59%], 11 clefts [25%] and seven foveae [16%]) were included. Mean age at the time of the first visit was 6.6 years. The lesion object of the study was the main reason for presentation in only five cases (16%). Proliferations showed two different histopathological patterns and had characteristics in common with human oral pyogenic granuloma. Successful treatment was achieved in all cases by removing the occlusal contact by dental extraction or coronal reduction, possibly associated with lesion excision. This study underlines the need for a thorough oral examination and evaluation of dental occlusion in all patients. Causes for the development of traumatic occlusion may include an acquired overbite (possibly secondary to selective dental extraction), congenital or post-traumatic malocclusion, abnormal latero-lateral mobility of the mandible, occlusal drift of the premolar and molar teeth, and/or alveolar bone expansion.
Introduction
In humans, reactive lesions of oral tissues are common.1,2 Depending on location and aetiology, tissue erythema, erosion, laceration, ulceration, hyperkeratosis, scaling or proliferation may develop. The most frequent causes include self-trauma (eg, chronic biting habits), sharp edges of grossly carious teeth, faulty dental restorations, incongruous prosthetics and orthodontic appliances, ingestion of chemicals or food at high temperatures, radiotherapy and chemotherapy treatments, and food impaction.1,3 Furthermore, lesions of iatrogenic origin secondary to improperly performed dental and surgical procedures are possible.
In the cat the potential causes of reactive oral lesions are also numerous and similar to those described in humans. Occlusal trauma (ie, an anomalous contact between teeth or between teeth and soft tissues of the opposite quadrant) may develop in case of congenital or acquired malocclusion. For example, distoclusion (ie, mandibular arch occluding caudal to its normal position relative to the maxillary arch) is frequently accompanied by the contact between the mandibular canine teeth and the hard palate mucosa. 4 Also, after alveolectomy and extraction of a maxillary canine tooth, even cats with normal occlusion may develop an abnormal contact between the mandibular canine cusp and the mucocutaneous junction of the upper lip, with the development of erosive or ulcerative lesions. 5
Gingival and mucosal lesions have been reported as a result of contact between the maxillary fourth premolar tooth and the mandibular tissues in cats.4,6–8 These have been described as granulation tissue, 5 inflammatory polyps 7 and pyogenic granulomas (PGs). 8 However, the histological and morphological description of these lesions is lacking in the literature.
The main aim of this retrospective study was to describe clinical and histopathological findings in cats with caudal mucogingival lesions developed at the contact point of the premolar and molar teeth of the opposite quadrant.
Materials and methods
Medical records review
Medical and dental records, and oral photographs of client-owned cats examined between February 2001 and August 2011 by one of the authors (MG) at different veterinary clinics in Northern Italy were reviewed. All patients presented because of an oral or maxillofacial problem, but not necessarily because of the lesion object of this study.
Type of lesions
Lesions were classified as proliferations (ie, broad-based plaques or exophytic lesions of oral mucosa), foveae (ie, mucosal or gingival depression without ulceration), and gingival clefts (ie, localised gingival recession with or without bone resorption). Shape, size and location of a cleft had to match the shape, size and location of the cusp of the opposite tooth at closed mouth evaluation.
Case selection
Patients were included in the study if they presented mucogingival tissue lesions at the point of contact with premolar or molar teeth of the opposite quadrant.
Cats with neoplastic lesions and proliferative stomatitis were excluded from the study because of the difficulty in identifying lesions of clear traumatic type.
Each patient that had visited on a certain date with one or more lesions was defined as a case. Therefore, cats showing different lesions at different times were calculated as multiple cases.
For all animals, a general physical examination and preoperative laboratory tests (including complete blood count and complete biochemistry profile) were performed. Depending on the medical condition and any other diseases present or suspected, the diagnostic investigation was variably extended (urinalysis; feline leukaemia virus and feline immunodeficiency virus enzyme-linked immunosorbent assay tests; feline calicivirus and herpesvirus type 1 polymerase chain reaction tests; serum protein electrophoresis; FT4 evaluation; faecal examination; abdominal or thoracic ultrasound; thoracic, abdominal or skull radiographs; and computed tomography scan of the head).
Head and oral examinations, including the evaluation of dental occlusion and complete periodontal examination, were performed in all patients under general anaesthesia. Dental occlusion was evaluated after the induction of anaesthesia but before endotracheal intubation. Any abnormal findings were annotated on a dental record. Most abnormalities were also photographed. A complete intraoral radiographical examination was performed in all patients. A complete dental treatment (ie, supra- and subgingival ultrasonic and hand scaling, dental polishing, dental extractions) was performed as necessary and, when considered appropriate, tissue biopsies were taken. When indicated (ie, whenever a surgical procedure was performed, including surgical biopsies and dental extractions), analgesia was administered with a multimodal approach, using a combination of systemic drugs and loco-regional blocks (ie, inferior alveolar nerve block and/or infraorbital nerve block). Anti-inflammatory and/or antibiotic treatments were administered according to the medical condition of the patient, type and duration of the surgical procedure.
Data collection
Data collected for each patient included signalment (breed, sex, age, weight); main reason for presentation and, when different, the main indication for the procedure, defined as primary reason for treatment; location and type of lesion; tooth/teeth in traumatic occlusion with the lesion; performed treatment; histopathological findings (for biopsied proliferations); and outcome (Table 1). In addition, when possible, the speed of development of the lesion, defined as the time elapsed between a previous clinical examination (performed under general anaesthesia or not) and the time of diagnosis, was recorded. Furthermore, the dental history (ie, any previous dental treatment, oral or maxillofacial surgical procedure) was reviewed.
Data from 27 cats with caudal traumatic mucogingival lesions

Modified Triadan numbering system (if tooth missing). †Time since previous visit: number of days between previous visit and diagnosis
EX = extraction of tooth in contact with the lesion; EXO = extraction of tooth next to the lesion; WS = coronal adjustment of tooth in contact with the lesion; ExL = surgical excision of proliferative lesion; PS = periodontal surgery on tooth next to the lesion; SS = Scottish Straight; DSH = domestic shorthair; MC = male castrated; F = female intact; FS = female spayed; M = male intact; P = proliferation; Fo = fovea; C = cleft; Buc = buccal; Pal = palatal; Dis = distal; Dis-Buc = distobuccal. N/FU = no follow-up information
Outcome of treatment
Treatment outcome was classified as complete healing if, at the time of follow-up, the surgical area was free from signs of inflammation or any type of lesion. If, following complete healing, a new lesion similar to the one previously treated developed after a certain amount of time, a recurrence was recorded. The persistence of a lesion following treatment was defined as absence of healing. Finally, a lesion was described as progressive if it changed in time from one type to another (eg, from fovea to proliferation).
Results
Number of cases
Twenty-seven cats were included in the study: 16 European Shorthairs, five Persians, two Exotics, and one each of Scottish Straight, Carthusian, Sphynx and Maine Coon. Of these, 11 were males (one intact and 10 castrated) and 16 were females (four intact and 12 spayed). The age at the time of the first visit ranged from 1.0 to 13.8 years (mean 6.6 years, median 7.1 years), and the weight from 1.8 kg to 7.1 kg (mean and median 4.5 kg). Weight was not recorded in one case.
Two cats developed multiple lesions over time. In particular, one cat presented four times over 2 years and 3 months for seven different lesions, and another cat presented twice within 9 weeks for two different lesions. Thus, the total number of cases was 31.
Reason for presentation and primary reason for treatment
The main reasons for presentation are listed in Table 2. The lesion object of the study was the main reason for presentation in five cases (16%): four cases with a single proliferation and one case with two gingival clefts. The symptoms reported in these patients included pain when closing the oral cavity, anorexia, bleeding from the oral cavity and persistent nose rubbing.
Main reasons for presentation. A single patient may have been presented for more than one reason

The oral mucosal lesion represented the primary reason for treatment in 17/31 cases (55%) (Table 3). Of these, 12 cases had proliferative lesions, two had clefts, one had foveae, one had both one proliferation and one fovea, and one had one proliferation and two clefts.
Primary reasons for treatment
In the remaining 14 cases (45%), the lesions were diagnosed only during the oral examination performed under general anaesthesia. Eight of these cases had proliferative lesions, three had clefts and three had foveae.
Clinical presentation
Clinically, proliferations appeared as broad-based plaques or exophytic lesions, round or irregularly elongated, from pink to deep red in colour, sometimes with yellowish discolouration, often with superficial ulceration, ranging in size from 2 to 10 mm in diameter, with a soft or friable consistency, and bleeding easily (Figure 1). Often, a concavity was evident in the centre of the lesion, which corresponded to the tip of the cusp of the tooth in traumatic occlusion.

Left mandibular proliferative lesion (arrow) in contact with the mesiobuccal cusp of the maxillary fourth premolar tooth (asterisk) (case C). (a) Closed mouth; (b) open mouth
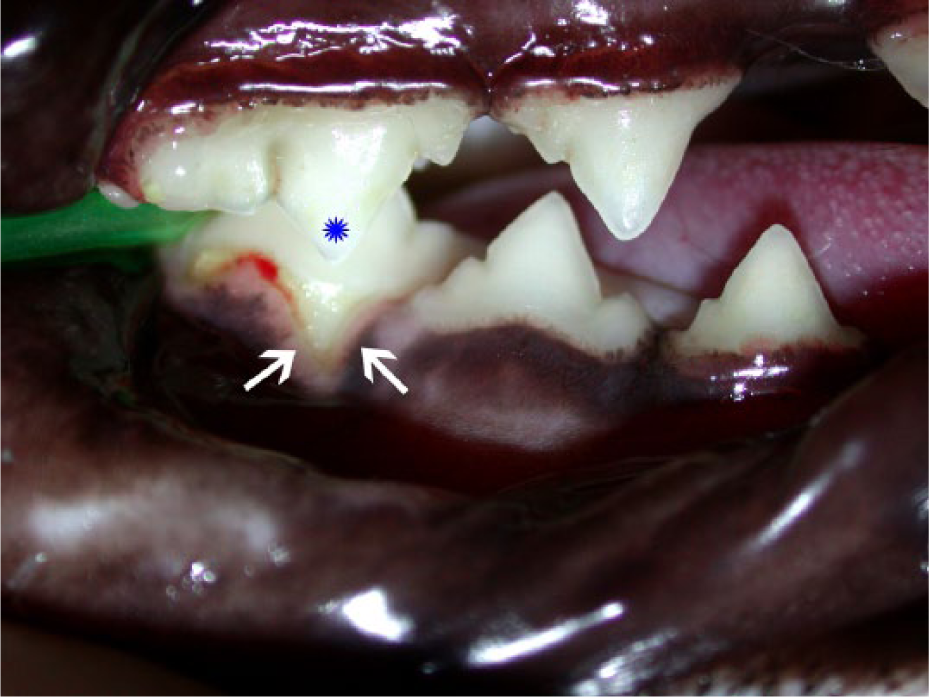
Foveae were non-ulcerated indentations on the gingival, alveolar, buccal/vestibular or palatal mucosa. They were circular to oval in shape, 2–3 mm in diameter and relatively shallow (except a single palatal lesion) (Figure 2).

Foveae (arrows) on the gingiva of the mesial root of the right mandibular first molar and fourth premolar teeth in contact with the mesiobuccal cusp of the maxillary fourth premolar (red asterisk) and the middle cusp of the maxillary third premolar tooth (blue asterisk), respectively (case Alfa 1–2)
Gingival clefts were typically V-shaped, 1–3 mm in disto-mesial dimensions and apical extension. In a few cases the lesion extended beyond the mucogingival junction (Figure 3). The margins of the defects were often inflamed, and there was variable plaque and calculus accumulation on the affected tooth surface. The shape of the defect was an accurate impression of the cusp of the tooth in traumatic occlusion. At closed mouth, the tip of the opposing tooth cusp reached the apical margin of the defect.
Buccal gingival cleft (arrow) at the mesial root of the right mandibular first molar tooth, in contact with the mesiobuccal cusp of the maxillary fourth premolar tooth (asterisk). Ten-year-old, female spayed, domestic shorthair cat (case not included in the current series)
Number and distribution of lesions
A total of 44 lesions were diagnosed in 27 cats: 26 proliferations (59%), 11 clefts (25%) and seven foveae (16%). Eighteen cats (67%) had only proliferations, four (15%) only gingival clefts and three (11%) only foveae. Two cats (7%) presented proliferations, as well as other types of lesions.
Seventeen cats (63%) presented only one lesion and 10 individuals (37%) presented bilateral, multiple lesions either concomitantly or successively. With the exception of two cases, concomitant lesions were always of the same type.
Side distribution of the lesions was similar, with 23 lesions (52%) localised on the right side, and 21 (48%) on the left side of the mouth.
The great majority of the lesions (93%) affected the mandibular tissues and only three lesions (two proliferations and one fovea; 7%) were located on the upper jaw. One cat had a right mandibular and a left maxillary lesion at the same time. In all other cases, the lesions were either maxillary or mandibular only.
Most of the lesions (80%) were on the buccal side of the affected tooth. The two maxillary proliferative lesions were distobuccal to the fourth premolar tooth. The only maxillary fovea was palatal to the fourth premolar tooth.
Out of 24 mandibular proliferations, one was on the buccal mucosa next to the mandibular fourth premolar tooth. The other 23 lesions developed on the mucosa buccal (n = 16), distal (n = 4) or distobuccal (n = 3) to the mandibular first molar tooth.
Out of six mandibular foveae, one was on the buccal gingiva of the mandibular fourth premolar tooth. All other foveae developed on the buccal mucosa or gingiva of the mandibular first molar tooth.
All gingival clefts were located on the buccal side of the affected mandibular teeth (four fourth premolar teeth, and seven first molar teeth).
Six of 44 lesions (14%) (one proliferation, one fovea, four clefts) were buccal to the mandibular fourth premolar tooth. In these six cases, the tooth in contact with the lesion was the ipsilateral maxillary third premolar tooth (central cusp) for four lesions and the ipsilateral maxillary fourth premolar tooth (mesiobuccal cusp) for two lesions.
Twenty-eight lesions (64%) (16 proliferations, seven foveae, five clefts) were buccal to the mandibular first molar tooth. All of these lesions were in contact with the ipsilateral maxillary fourth premolar tooth (mesiobuccal or distal cusp).
Three lesions (7%) were distobuccal and four (9%) were distal to the mandibular first molar tooth. These proliferations were in occlusal contact with the ipsilateral maxillary first molar tooth and/or with the distal cusp of the maxillary fourth premolar tooth.
Two lesions (5%), both proliferative, were distobuccal to the maxillary fourth premolar tooth and in contact with the ipsilateral mandibular first molar tooth (distal cusp). In both cases a posterior crossbite developed secondary to severe maxillofacial trauma.
One fovea (2%) was palatal to the maxillary fourth premolar tooth, in occlusal contact with the ipsilateral mandibular first molar tooth (distal cusp).
Speed of development
The lesions were diagnosed from 20 days to more than 3 years after a previous clinical examination or surgical procedure. In seven cases the tooth adjacent to the lesion had been recently extracted (from 28 days to 90 days earlier), whereas in two cases the extraction occurred 210 and 600 days earlier, respectively. One cat developed two proliferations 28 and 22 days after the previous visit. It then developed two clefts within 9 months of the previous re-examination (approximately 2 years from the previous surgical treatment). Finally, it developed another proliferative lesion 20 days after the last surgical procedure. There was no difference in speed of development for proliferations and clefts in this patient.
Treatment
Treatment options (as individual procedures or in combination) included coronal reduction of the tooth/teeth in occlusal contact with the lesion with the use of aluminum oxide abrasive burs (17 lesions; Dura-White Stones, Shofu Dental GmbH) (Figure 4), extraction of the tooth/teeth in occlusal contact with the lesion (performed in case coronal reduction caused pulp exposure; 23 lesions), extraction of the tooth/teeth next to the lesion (performed mostly in case of concomitant periodontal or other dental disease; 16 lesions), periodontal surgical procedure (one cleft), and surgical excision of the lesion (20 proliferations; Tables 1 and 4). One cat was not treated and was euthanased at the time of diagnosis for other medical reasons.

Reduction of the mesial cusp of the maxillary fourth premolar tooth in contact with a gingival cleft developed on the buccal side of the right mandibular first molar tooth (case not included in the current series). (a) Preoperative image. (b) After dental scaling, polishing and radiographical examination, the portion of crown to be removed is marked with a pen. (c) Postoperative image. The exposed dentine may be protected with a layer of unfilled resin
Elected treatment options based on type of lesion

EX = extraction of the tooth/teeth in occlusal contact with the lesion; EXO = extraction of the tooth/teeth next to the lesion; ExL = surgical excision of the lesion; PS = periodontal surgical procedures; WS = coronal reduction of the tooth/teeth in occlusal contact with the lesion
Histopathology
Seventeen of 20 excised proliferations were submitted for histopathological examination. The remaining three excised lesions were not examined because of economical restraint. Six proliferative lesions were not surgically removed or analysed.
Histologically, two microscopic patterns were noted: one predominantly inflammatory, classified as chronic focal lymphoplasmocytic mucositis (type 1; seven lesions [41%]), and one predominantly hyperplastic, classified as chronic focal fibrovascular hyperplastic mucositis (type 2; 10 lesions [59%]) (Table 1). The type 1 pattern was mainly characterised by a slightly elevated plaque-like lesion with diffuse interstitial infiltrate, consisting of lymphocytes and plasma cells (Figure 5). At times, superficial perivascular neutrophils associated with ulceration were present. A variable degree of epithelial hyperplasia, often associated with focal, multifocal or diffuse ulceration, was observed. The interstitial stroma was generally inconsistent. Moderate fibrovascular hyperplasia was observed only in one sample. In some cases, granulation tissue was noted below the ulcer. In some samples, salivary gland tissue was present, with the same lymphoplasmacytic interstitial infiltrate. Rarely, mild necrosis was present.
Histological examination of a slightly elevated plaque-like mucosal lesion showing ulcerations and diffuse, superficial and deep, interstitial infiltrate, consisting of lymphocytes and plasma cells (type 1 histological pattern; case M) (haematoxylin and eosin stain; bar = 200 μm, x 4). Inset: magnified area (x 40)
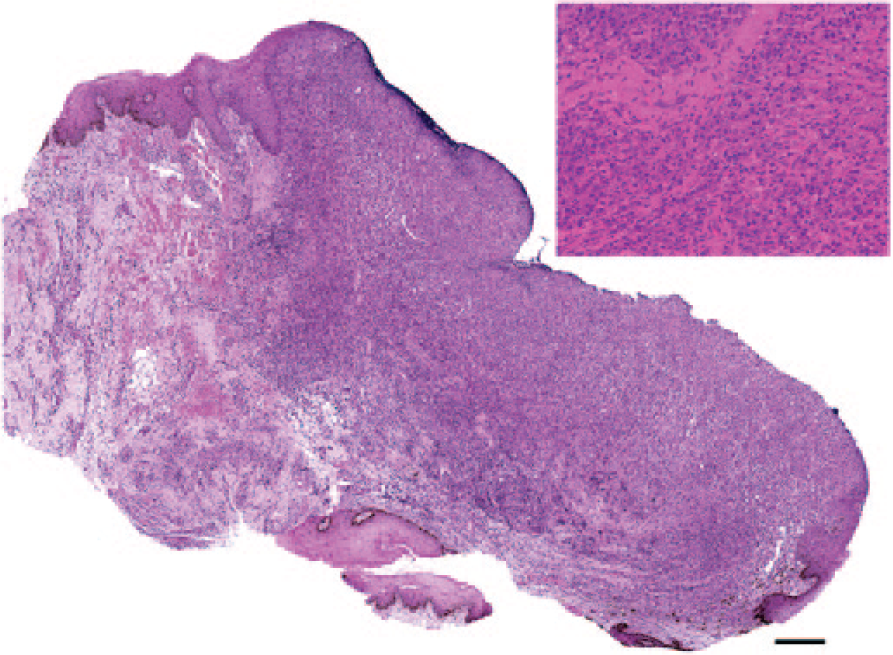
The main feature of the type 2 pattern was the presence of hyperplasia of the fibrous and vascular components, with neovascularisation ascribable to granulation tissue (Figure 6). Endothelial cells and activated fibroblasts were embedded in variable amounts of interstitial collagenous stroma. A variable degree of mixed perivascular infiltrate with lymphocytes, plasma cells and neutrophils was observed. Epithelial hyperplasia and ulceration were focal, multifocal or diffuse, and generally of moderate-to-severe intensity. In some samples mild necrosis was present.

Histological examination of an exophytic mucosal lesion characterised by massive fibrovascular hyperplasia (type 2 histological pattern; case A4) (haematoxylin and eosin stain; bar = 500 μm, x 4). Inset: magnified area showing granulation type tissue (x 40)
Follow-up and outcome
Follow-up visits were performed for 19 cats (70%), from 3 weeks to more than 3 years after the surgical procedure. All showed complete healing, without recurrence. In some cats (with proliferations) healing was rather slow, with the persistence of a certain degree of inflammation for a period ranging from 3 to 6 weeks, and for up to 3 months after surgery in one cat. Four cats had long-term follow-up visits (16 months–3 years after surgery), confirming the absence of any recurrence. Seven patients were lost to follow-up. One cat was euthanased at the time of diagnosis.
The progression from one type of lesion to another was never demonstrated.
Discussion
This study underlines the need for a thorough oral examination and evaluation of dental occlusion in all patients. Only five cases were presented for veterinary care because of the studied lesion. Four of these had proliferations, possibly easier to spot by the owners and also possibly causing more discomfort than other lesion types. Clinical examination performed in awake (non-anaesthetised) patients resulted in diagnosis of 12 additional cases. However, 20 lesions were diagnosed only after induction of general anaesthesia in patients presented for other oral conditions. If dental occlusion is not accurately evaluated, clefts could be incorrectly allocated to primary periodontal disease and foveae could easily go undetected.
The distal cusp of the mandibular molar tooth normally occludes on a concavity of the palatine process of the maxillary bone, palatal to the distal root of the fourth premolar tooth. No data exist on the normal depth of this concavity, and in the absence of obvious abnormalities (ie, inflammation and ulceration) the definition of pathological fovea in this location is very subjective. In the single case of palatal fovea included in this population, the depths of the maxillary right and left concavities were clearly asymmetrical. However, for these reasons and owing to the retrospective nature of this study, it is possible that the true prevalence of foveae and clefts was greater than reported.
The development of proliferations, foveae or clefts may depend on the type of tissue contacted by the offending tooth, as different tissues may show different reactivity in response to specific trauma.9–12 When the occlusal contact occurred at the gingiva, a fovea or a cleft developed. Gingival recession may be caused by periodontal disease rather than trauma. 13 However, we consider that a traumatic component played a major role in the clefts included in this study. This view is supported by the fact that, even if dental scaling and polishing may have contributed to the resolution of mild lesions, after the extraction of the tooth in contact with the lesions, the clefts (and periodontal status of the involved teeth) did not worsen or even improved. The development of foveae rather than clefts (gingiva) or proliferations (alveolar and buccal mucosa) may be secondary to a different degree of contact between the tooth and the soft tissues.
Despite a clinically indistinguishable appearance, in this study proliferations showed two different microscopic patterns, one dominated by a lymphoplasmacytic inflammatory component and one by a fibrovascular proliferation. They both showed non-specific histopathological features, and the final diagnosis should therefore always be based on both histological and clinical appearance. Factors affecting the development of histological pattern 1 or 2 are unknown. We hypothesise that they represent two different stages of the same lesion. In the oral mucosa, inflammation is almost inevitably of lymphoplasmacellular type, and when there is chronic ulceration, an attempt to repair with fibrovascular granulation and hyperplastic tissue occurs. 10 Immature tissue is characterised by neovascularisation with endothelial-activated cells, and the fibrous component with higher quantities of collagenous matrix is prevalent in mature tissues. 10
As previously reported, 8 the proliferative lesions observed in this study had clinical and histopathological characteristics similar to human PG, and, in particular, to the so-called non-lobular capillary haemangioma (PG non-LCH type). PG is a very common reactive tumour-like lesion affecting humans. It represents a productive response to low-grade inflammatory stimuli of different nature.14,15 The name is a misnomer, as it is not a granulomatous lesion and does not have a bacterial component.16,17 PG developing in women during pregnancy seems to have a hormonal cause and is defined as granuloma gravidarum. 14 The most common location for PG is the gingiva, irritation resulting presumably by the presence of dental calculus or other material in the gingival sulcus, dental exfoliation or eruption, and local trauma.14,15,18 Other possible locations include the tongue, lower lip and buccal mucosa. 14 Clinically, it is a red or pink mass, and it predominantly consists of granulation tissue. 15 However, the histological appearance may be predominantly inflammatory or fibrous. 14 One type of PG, characterised by a number of capillaries arranged in a lobular way, is called LCH. A second type, represented by a fibrovascular proliferation that resembles granulation tissue, is called non-LCH. The surface may ulcerate secondary to trauma. The size varies from a few millimetres to a few centimetres. The growth rate is variable, and the maximum size is reached in a few weeks or months.14,17 An initial period of growth may be followed by a period of stabilisation and, occasionally, regression of the lesion. 17 Treatment includes the excision of the proliferation and the removal of any irritating factor.
In our feline population, the lobular pattern was absent and the fibrovascular tissue had an orientation similar to granulation tissue. The vessels were generally perpendicular to the surface. However, as noted in PG non-LHC type, some lesions (pattern type 2) showed a predominant fibrous component, possibly suggesting a process of fibrous tissue maturation.
Interestingly, two proliferations with histological pattern 2 were initially diagnosed as neoplastic malignancies. In one case a diagnosis of poorly differentiated spindle cell sarcoma was based on the presence of a predominant spindle cell population with moderate morphological atypia (anisocytosis, anisokaryosis and some mitosis), without a specific architectural organisation (Figure 7). The immunohistochemistry assay with anti-cytokeratin and anti-vimentin antibodies revealed an ordered and repeated pattern characterised by numerous vessels perpendicular to the surface, and delimited by fibrous hyperplastic cells. Serial sections allowed the identification of an area of central necrosis. At the periphery, fibrovascular proliferation was observed. These findings were interpreted as immature granulation tissue. Therefore, the final diagnosis was severe chronic hyperplastic stomatitis with areas of central necrosis.

Histological examination of a proliferative mucosal lesion (case G). (a) Areas of hypercellular compact fibrous tissue with scant inflammation. (b) Hyperplastic fibrous tissue, low cellularity and abundant myxoid matrix. A mitotic figure is evident (arrow). Haematoxylin and eosin stain (bar = 40 μm, x 40)
In another case, malignant spindle cell carcinoma was initially suspected based on the presence of elongated cells with moderate characters of anisocytosis and anisokaryosis, frequent mitosis and some atypia. These cells were apparently in continuity with the superficial epithelium and infiltrating the submucosa in absence of the underlying basement membrane. The immunohistochemical assay with anti-cytokeratin and anti-vimentin antibodies, together with deeper histological serial sections, showed two distinct cell populations: epithelial cells, located above the basement membrane (which was actually present), referring to the surface epithelium; and deep subepithelial cells of mesenchymal origin. A specific distribution pattern, characterised by neovascularisation associated with fibrous proliferation and interstitial matrix deposition, was revealed. The final diagnosis was then chronic, moderate, focal, fibrovascular hyperplastic mucositis.
In both cases, the initial evaluation was probably influenced by artefacts mainly due to superficial cuts of the tissue samples. Deep biopsies and serial sections at different depths should always be performed and analysed.
Lesions clinically similar to the proliferations described here have been previously reported in the literature.4,6 In particular, they have been described as lesions secondary to interference between the maxillary fourth premolar tooth and the mandibular fourth premolar and first molar teeth.4,8 This study confirms that in the majority of cases the traumatic occlusal contact occurred in this location. However, different locations are also possible. In descending order of frequency, the lesions developed near the mandibular first molar tooth (35 lesions), the mandibular fourth premolar tooth (six lesions) and maxillary fourth premolar tooth (three lesions). The tooth most frequently in contact with the lesions was the maxillary fourth premolar tooth (34 lesions), followed by the maxillary first molar tooth (six lesions), the maxillary third premolar tooth (four lesions) and the mandibular first molar tooth (three lesions).
The majority of cats included in this study were mesaticephalic. Sex distribution was similar between males and females. Unfortunately, the data of the general feline population visited during the same period at the same veterinary clinics is not available, and it is therefore difficult to statistically demonstrate any breed or sex predisposition.
The exact pathogenetic mechanisms leading to traumatic occlusion in the study population is unknown, but some causes may be hypothesised. Lyon and Okuda described mucosal proliferations of unknown origin (defined as inflammatory polyps) adjacent to the mandibular first molar tooth and listed as possible causes bruxism, chronic inflammation and local tissue irritation. 7 In the cases described in the current study, bruxism was never reported or detected.
The occlusal contact with a proliferative lesion could theoretically be secondary to an increase in volume of the soft tissue, and thus be a consequence of the proliferation rather than its cause. However, different aetiological factors responsible for the exophytic lesions could not be demonstrated. Furthermore, if the soft tissue lesions were primary, they would have possibly developed not only in contact with a tooth cusp, but also in other locations, which was not the case.
Traumatic occlusal contact may also be secondary to congenital or post-traumatic malocclusion, an abnormal latero-lateral mobility of the mandible, an acquired deep bite (overbite), an occlusal drift and/or alveolar bone expansion. Congenital malocclusion is considered an unlikely aetiological factor in this population. Four cats showed neutroclusion unlikely to influence the anatomical area of interest, and only three brachycephalic cats showed a typical mesioclusion. Furthermore, the mean age at the time of diagnosis was 6.6 years. Given the high speed of development of some lesions (just a few weeks in some individuals), in cases of a congenital component the study population would be expected to be younger.
In only four cats the lesions developed following severe oral and maxillofacial trauma and post-traumatic malocclusion. This is therefore a possible, but uncommon, cause for the development of the described lesions.
Cats are anisognathic, with the mandible narrower and shorter than the maxilla. The maxillary third and fourth premolar teeth (the most common teeth in contact with the lesions in our study) occlude buccal to the mandibular teeth, completely overlapping the mandibular crowns. 19 The tip of the large cusps of the maxillary teeth normally lightly touches the mandibular soft tissues. A slight increase in latero-lateral mobility of the mandible may therefore favour the contact between the maxillary teeth and the mandibular tissues. Increased mandibular mobility was not recorded in any of these patients, but this possibility was not specifically and objectively evaluated prospectively.
As the presence of the teeth likely contributes to maintain upper and lower jaws at a certain distance, we consider possible the development of an acquired overbite in patients that lose important teeth such as the large mandibular and maxillary premolar and molar teeth. Sixteen cases were missing one or more of these teeth, and 10/33 mucosal foveae and proliferations developed after the tooth adjacent to the lesion was lost or extracted. In particular, one cat developed seven lesions over time (one fovea, two clefts and four proliferations). Initially, the cat had a mandibular proliferation next to the right mandibular first molar tooth (tooth 409), in contact with the mesial cusp of the right maxillary fourth premolar tooth (tooth 108), and a deep fovea palatal to the left maxillary fourth premolar tooth (tooth 208) in contact with the distal cusp of the ipsilateral mandibular first molar (tooth 309). Teeth 409 and 108 were extracted, the proliferative lesion was surgically excised and the height of the distal cusp of tooth 309 was reduced. At the 18 day follow-up, the cat showed two mucosal proliferations at the contact point of the right maxillary first molar (tooth 109) and third premolar teeth (tooth 107). Coronal reduction of the central cusp of tooth 107 and surgical excision of the proliferative lesions were effective in treating these lesions. Two years later, the cat developed two gingival clefts at the right mandibular fourth premolar (tooth 408) and left first molar teeth (tooth 309), in contact with tooth 107 and 208 respectively. Teeth 107 and 208 were extracted, and the cleft at tooth 309 was treated with a lateral sliding flap. About 5 weeks later, a proliferative lesion developed on the mandibular mucosa in contact with the left maxillary first molar tooth (tooth 209), which was then extracted. The mass was surgically excised. At the last follow-up visit, 2 years after surgery, no other lesions were present.
In another patient tooth 108, in contact with a proliferative lesion vestibular to the missing tooth 409, was extracted and the proliferation excised. At the 2 month follow-up, a similar lesion was present on the left side, in contact with tooth 208.
However, scientific data relative to the normal depth of the bite in cats and the influence that the extraction of certain teeth may have are not available. In addition, several individuals had complete dentition or were missing teeth (incisors and maxillary second premolar) that unlikely have any influence on the depth of the bite. The role of extraction and dental overbite on the development of these lesions remains therefore speculative.
Occlusal drift (teeth migration in coronal direction) may also be hypothesised as a cause of acquired traumatic occlusion. In humans, occlusal drift is a physiological phenomenon accentuated in case of loss of the opposing teeth. It is also considered necessary to maintain the normal occlusal and interproximal contact after dental abrasion and continued facial growth.20,21 It is unknown if similar phenomena occur in cats. However, alterations of the periodontal ligament and cement of the mandibular premolar and molar teeth, indicative of a possible distal drift, have been reported in feline patients. 22 Another study also showed hypercementosis, narrowing of the periodontal space and alveolar bone expansion of the premolar and molar teeth (as well as maxillary canine teeth) in cats. 23 Alveolar bone expansion may be explained by the so-called periodontal growth (or segmental alveolar bone growth), which, in humans, refers to growth of the periodontal tissues in a coronal direction, and results in movement of the entire tooth in the same direction. 23 Interestingly, in seven cases partial extrusion and buccal alveolar bone expansion of the maxillary canines was recorded on the dental chart (data not shown). Slight occlusal drift of premolar and molar teeth may be very difficult to detect clinically, and its potential role in the development of an acquired occlusal trauma in the caudal region of the mouth remains hypothetical.
Another possible factor influencing occlusion and depth of the bite may be the physiological skull growth. Even if cranial growth in the cat is prevalent in the early months of life, 24 bone turnover of the maxillofacial bones may lead to occlusal changes during life. However, given the rapid development of the lesions in several cases, this is an improbable cause of acquired malocclusion in this study population.
The elimination of traumatic contact by extraction or coronal reduction of the tooth in contact with the lesion was always efficacious and prevented the development of local recurrences. As discussed earlier, however, the extraction of an offending and/or offended tooth may favour the occlusal contact between other teeth and the soft tissues, causing the development of new lesions.
Conclusions
Although we strongly support the surgical excision of proliferative lesions, as it favours healing, promotes more rapid resolution of symptoms and allows the obtaining of a histopathological diagnosis, in three cases with four different lesions, in which only coronal reduction or extraction of the offending tooth was performed, the lesions healed spontaneously and were not present at the follow-up visit. One case treated similarly was lost to follow-up.
The real need for treatment (coronal reduction or extraction of the tooth cusp in traumatic occlusion) for foveae remains to be proven. These are, in fact, likely asymptomatic lesions, and progression to proliferation or cleft was not supported by this study. Long-term monitoring may therefore be the right approach for these types of lesions.
Two individuals developed a proliferative mucosal lesion after and next to a gingival cleft. However, retrospective data are not unequivocal (initially the occlusion was not recorded in these patients), and progression from one type of lesion to another could not be demonstrated.
Footnotes
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no grant from any funding agency in the public, commercial or not-for-profit sectors.