
Abstract
Feline lymphocytic cholangitis (LC) has been commonly treated with prednisolone, and more recently with ursodeoxycholic acid (UDCA). Previously, we found that prednisolone treatment resulted in a statistically longer survival time than treatment with UDCA. In order to explain this difference, we compared the effects of prednisolone and UDCA treatment on hepatic tissue by evaluating consecutive liver biopsies. Archival serial biopsy materials from cats with LC treated with prednisolone (n = 5) or UDCA (n = 4) were evaluated. We employed haematoxylin and eosin staining to evaluate inflammation, and reticulin staining for fibrosis. Immunohistochemical stainings for Ki-67, K19 (Cytokeratin 19) and α-smooth muscle actin were used to evaluate cell type-specific proliferation and activation of hepatic stellate cells. Inflammation decreased more in the group treated with prednisolone, while the number of cholangiocytes, progenitor cells and fibroblasts did not differ between the treatment groups. Additionally, no difference was found for the amount of fibrosis in both treatment groups.
Introduction
The increasing popularity of pet cats has heightened the need for specific knowledge about lymphocytic cholangitis (LC), a common inflammatory hepatic disease in cats.1–3 Although bacterial DNA has been found in the bile of cats with LC, its aetiology remains enigmatic, and an immune-mediated component has also been suggested.4–7
Clinical signs include nausea and vomiting, changes in appetite, gradual weight loss and jaundice. 6 Blood analysis may reveal elevated activities of hepatic enzymes, such as alanine aminotransferase, reflecting damage to periportal hepatocytes, and increased levels of bile acids, while hypergammaglobulinemia is the most consistent finding.6,8,9 Usually, LC is a chronic disease that can affect the entire biliary tree and progresses slowly during months or years. Aggregates of lymphocytes in portal tracts and in and around bile ducts are a hallmark of the disease. 2 The chronic inflammation in the bile ducts, characterised by dilations, strictures and proliferation of bile ducts may eventually lead to fibrosis and cirrhosis. 2
Histopathology is considered the gold standard for diagnosing LC. 2 The lesions are characterised by inflammatory cells in portal tracts, variable portal fibrosis and proliferation of bile ducts, which are considered the hallmarks of LC.2,5 These histopathological features exhibit similarities to those found in human primary sclerosing cholangitis (PSC).5,6,10 To date, only a limited number of studies on the histological aspects of feline LC have been reported.3,5,6,11,12
LC is commonly treated with prednisolone or ursodeoxycholic acid (UDCA).13,14 The use of prednisolone has been warranted by the immune-mediated component suggested by the abundant presence of lymphocytes.2,5 UDCA has been proposed as supportive therapy based on its hepatoprotective properties.14–20 As promising results were reported initially for UDCA as a treatment for human PSC, it was welcomed as a potential new treatment for cats with LC between 1998 and 2008.21,22 However, more recent data indicate a lower efficiency of UDCA in human PSC patients.23–25
Clinical evaluation of these therapeutic interventions in cats with LC showed that prednisolone treatment resulted in a statistically significantly longer survival time than treatment with UDCA. 8 Yet it is undetermined if the improvement in clinical condition correlates with improvement in the underlying hepatic histological lesions.
The liver is capable of a remarkable and unparalleled regeneration, which is based on proliferation of both hepatocytes and cholangiocytes. 26 Only when regeneration capacity proves inadequate, progenitor cells (also known as ‘oval cells’ in rodents) will be activated.26–29 Fibrosis occurs when the injury takes on a more chronic character, and the amount of collagen subsequently increases. 30 The main source of collagen is Ito cells, also known as hepatic stellate cells (HSC), fat-storing cells, hepatic lipocytes or perisinusoidal cells, which are the main storage sites for vitamin A in non-diseased liver.31–34 Proliferating fibroblasts in the portal areas can also contribute to collagen deposits and fibrosis.
The purpose of this study was to evaluate liver histology during treatment with prednisolone or UDCA in cats with LC by analysing the proliferation of hepatocytes, lymphocytes, fibroblasts, bile ducts, activation of progenitor cells, fibrosis and the degree of inflammation.
Materials and methods
All procedures were approved by the responsible ethical committees as required under Dutch legislation. All liver biopsies were taken for diagnostic purposes between 1998 and 2008. No tissue was taken for research or scientific purposes only.
Case selection
Twenty sequential archival biopsy materials (fixed in 10% neutral buffered formalin and embedded in paraffin) from nine cats diagnosed with LC were identified from the registration system used by the Department of Pathobiology, Faculty of Veterinary Medicine at Utrecht University (The Netherlands). The diagnosis of LC was based on the presence of typical histopathological findings combined with clinical signs, and elevated levels of bile acids and/or activities of liver enzymes. 2 The characteristics of the cats are shown in Table 1. The archives further showed that cats were treated with prednisolone (1–2 mg/kg/day) or UDCA (15 mg/kg/day).35,36 On average, biopsies were taken every two months (mode; range, 1–9 months) (Table 2). As a rule, a minimum of two biopsies was taken at any time from each patient by the attending clinician. Only cats with a diagnosis of LC that had serial biopsies taken were considered eligible for inclusion in this study.
Characteristics of nine cats with lymphocytic cholangitis
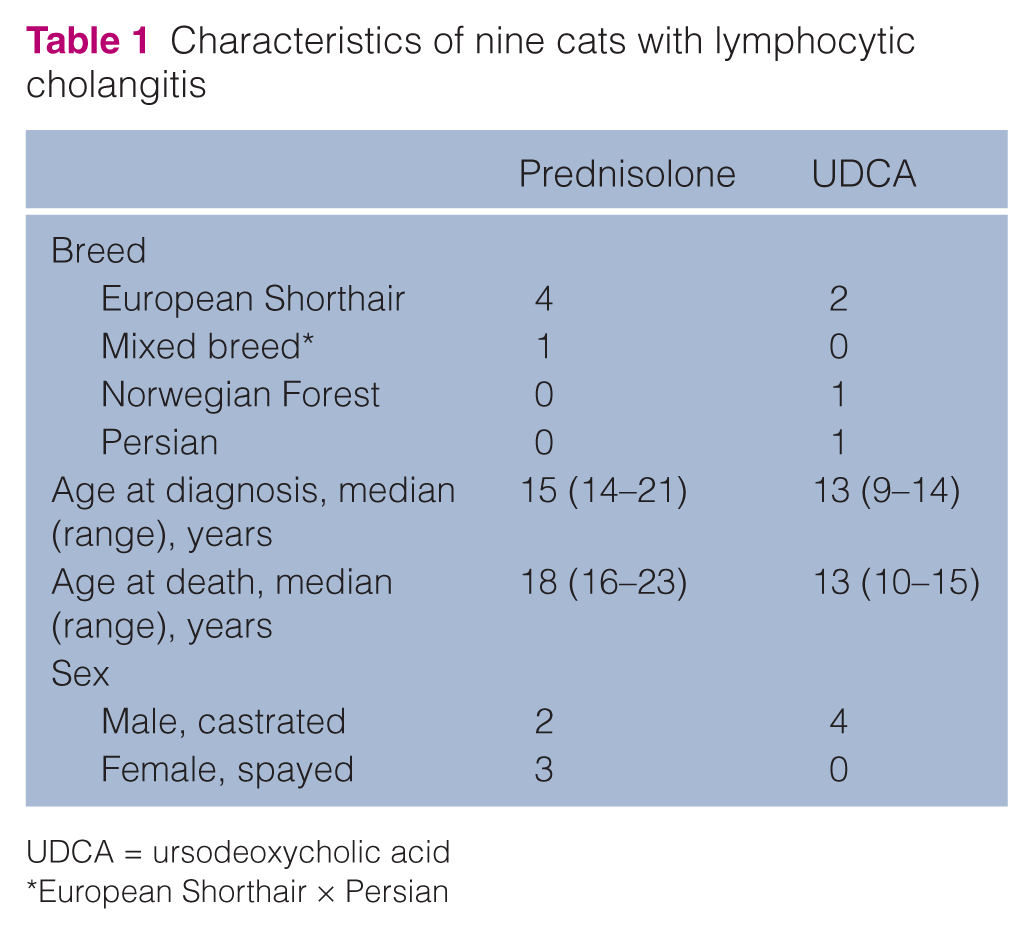
UDCA = ursodeoxycholic acid
European Shorthair × Persian
Description of biopsies and therapies in the different cats
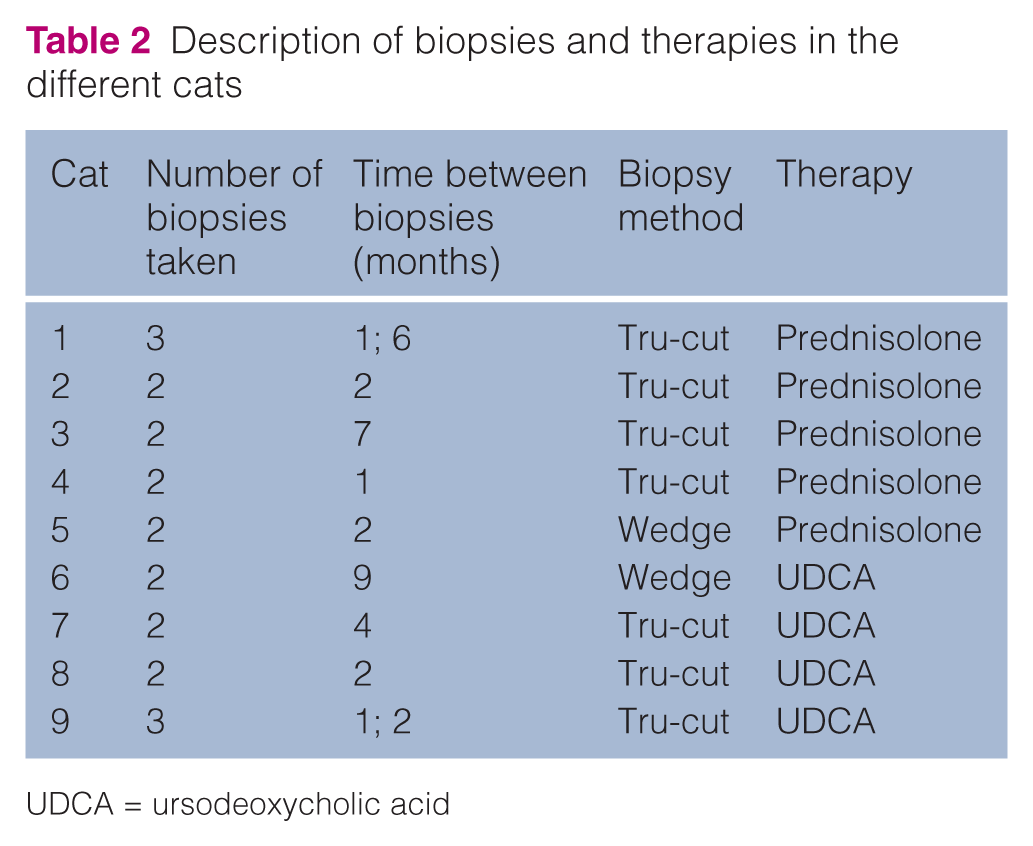
UDCA = ursodeoxycholic acid
Additionally, tissue samples from dogs and cats that did not suffer from LC were included to verify the correctness of the immunohistochemical staining processes.
Histopathology and immunohistochemistry
A routine haematoxylin and eosin (HE) staining was used to evaluate the degree of inflammation during therapy. Proliferation of cells was determined with Ki-67, a commonly used proliferation marker. 37 The activation of progenitor cells and proliferation of bile ducts was evaluated with immunohistochemical staining protocols for cytokeratin 19 (K19) as described previously. 38 Fibrogenesis was evaluated by applying a reticulin stain (Gordon and Sweet) to stain type III collagen (reticulin).2,39 Furthermore, we evaluated the activation of HSC, the main producers of collagen in the chronically injured liver, with a stain against α-smooth muscle actin (α-SMA).26,40–44
Staining protocols
Archival formalin-fixed liver tissues were routinely processed to produce slides with freshly cut sections (3 µm) that were stained with HE. Additionally, freshly cut sections were mounted on silane-coated slides (Starfrost; Waldemar Knittel) and stained for reticulin according to Gordon and Sweet, Ki67, K19 and α-SMA. For these stainings, tissue sections were deparaffinised and rehydrated in a series of xylene, alcohol and aqua dest baths (5 mins each) before application of the following protocols.
Ki-67
Sections were incubated in pre-heated citrate buffer (10 mM, pH 6.0) in a microwave oven. Endogenous peroxidase activity was blocked with 1% hydrogen peroxide (H2O2) in methanol. Sections were incubated with 10% normal horse serum to reduce background staining. Next, the sections were incubated with mouse anti Ki-67 (MIB1 clone, 1:50; Dako) overnight at 4°C in a humidified chamber in a refrigerator. After washing in phosphate-buffered saline (PBS) with Tween-20, sections were incubated in horse anti-mouse biotinylated immunoglobulin G (1:125; Vector Laboratories). Subsequently, avidin–biotin complex binding (ABC method; Vector Laboratories) and visualisation, with haematoxylin as counterstain, and 3-amino-9-ethylcarbazole (AEC; Dako) were performed according to the manufacturer’s instructions. Jejunal samples from dog and cat were used as positive controls to check for the correctness of the staining protocol used.
K19
Tris-buffered saline (TBS; 0.01 M, 1.5 M sodium chloride, pH = 7.6) with Tween was used to wash sections before treating them with ready-to-use Proteinase K (Dako). Endogenous peroxidase activity was blocked with 0.1% H2O2 in TBS. Sections were then incubated with 10% normal goat serum to reduce background staining. Subsequently, sections were incubated with the primary antibody mouse anti human K19 (clone b170, 1:100; Leica Microsystems). After washing in TBS with Tween-20, sections were incubated with Envision (goat-anti-mouse; Dako). Visualisation with haematoxylin as a counterstain and AEC (Dako) were performed according to the manufacturer’s instructions. Positive staining of bile ducts served as internal controls.
α-SMA
The ABC/peroxidase (PO) method for mouse anti-α-SMA was used. Endogenous peroxidase activity was blocked with 1% H2O2 in methanol. PBS with Tween-20 was used to wash sections in between steps. Sections were then incubated with 10% normal horse serum to reduce background staining, and then with the primary antibody mouse-anti-SMA (MU128-UC, 1:1200; BioGenex Laboratories). After washing in TBS with Tween-20, sections were incubated with horse anti-mouse biotin (1:125; Vector Laboratories) for 30 mins. Then, the ABC method (Vector) and visualisation with AEC (Dako) were performed according to the manufacturer’s instructions. HE was used as a counterstain. Arterial smooth muscle cells were used as internal controls.
Histological scoring and grading methods
HE and reticulin staining
A modified version of the grading system introduced by Gagne et al 3 for the number of lymphocytes, and fibrosis and bile duct proliferation was used to evaluate the biopsies (Tables 3 and 4).
Grading scheme for inflammation and fibrosis of haematoxylin and eosin- and reticulin-stained specimens

Scoring and grading scheme for immunohistochemically stained specimens

The percentage of the specimens infiltrated with inflammatory cells obscuring normal hepatic structure was measured. Two calibrated high-resolution microscopical images of randomly selected areas in the biopsies were made using Cell^B software (version 3.0; Olympus Soft Imaging Solutions) with an Olympus ColorviewIIIu (Olympus) digital camera and an Olympus BX41 microscope at × 200 magnification. The average percentage of inflammation was calculated with Cell^B software (version 3.0; Olympus) (Table 5).
Biopsy results for inflammation in nine different cats
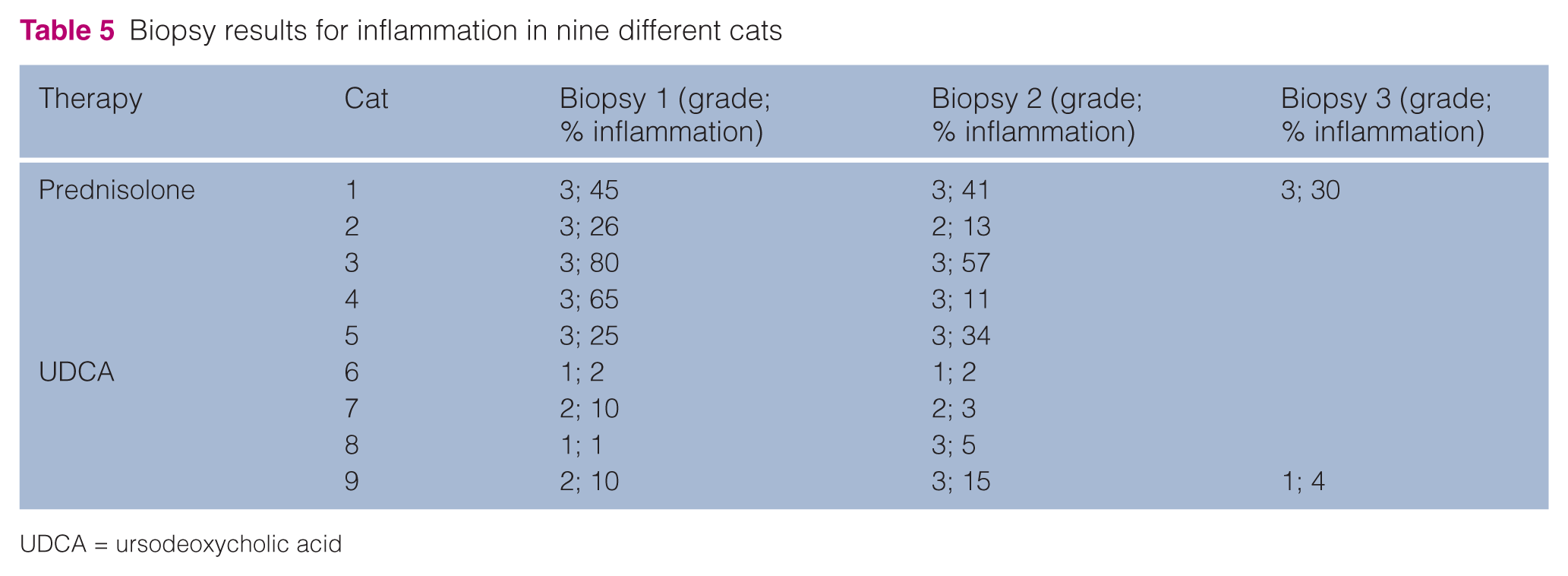
UDCA = ursodeoxycholic acid
Immunoreactivity for Ki-67 was evaluated by counting the number of cells per high-power field (HPF; magnification × 400) and calculating the average of three HPFs (Table 4). K19 allowed for the enumeration of bile ducts and periportally located progenitor cells.
Immunoreactivity against α-SMA was evaluated by expressing the number of α-SMA positive cells graded as absent, mild, moderate or strong.
Results
Inflammation
The percentage of the specimens infiltrated with inflammatory cells (Figures 1a,b) decreased in four and increased in one of the five cats treated with prednisolone. In contrast, the results for UDCA were less consistent (Table 5). As can be seen, the grade (ie, the number of lymphocytes per infiltrate) did not change, in the most part. Therefore, the largest contribution to changing the severity of inflammation was made by the total part of the liver biopsy being affected by inflammation (ie, percentage of biopsy). Overall, when comparing the two treatment groups, the group treated with UDCA was less severely affected by the disease than the group treated with prednisolone.

Histological examples of feline lymphocytic cholangitis. (a) Large infiltrates of small lymphocytes are present in portal areas (asterisk) extending to portal–portal bridging inflammation. Haematoxylin and eosin (HE) staining. (b) Portal areas are infiltrated by moderate numbers of small lymphocytes with moderate bile duct proliferation. HE staining. (c) Concentric bands of collagen surround the bile duct (asterisk). Collagen stain according to Gordon and Sweet. (d) Positive staining against α-smooth muscle actin is present around the bile ducts, in the arterial tunica media and in the wall of the portal veins. In addition, the perisinusoidal spaces throughout the parenchyma are moderately stained, which is most likely due to activated stellate cells. Immunohistochemistry (IHC). (e) Positive staining for K19 is present in the cytoplasm of bile duct (arrowhead) cells and other cells (most likely liver progenitor cells) located in the periportal parenchyma (arrow). IHC. (f) Positive Ki-67 staining is present in nuclei of proliferating lymphocytes (arrow), fibroblasts (arrowhead) in portal areas and in hepatocytes (asterisk). IHC
In two biopsies from cats treated with prednisolone, follicle formation of B-lymphocytes was seen. Seventeen biopsies were negative for follicle formation and one liver specimen could not be judged unambiguously.
Fibrogenesis and activation of HSC
The fibrosis score increased more frequently during treatment with UDCA (Table 6).
Results for fibrosis in nine cats with lymphocytic cholangitis
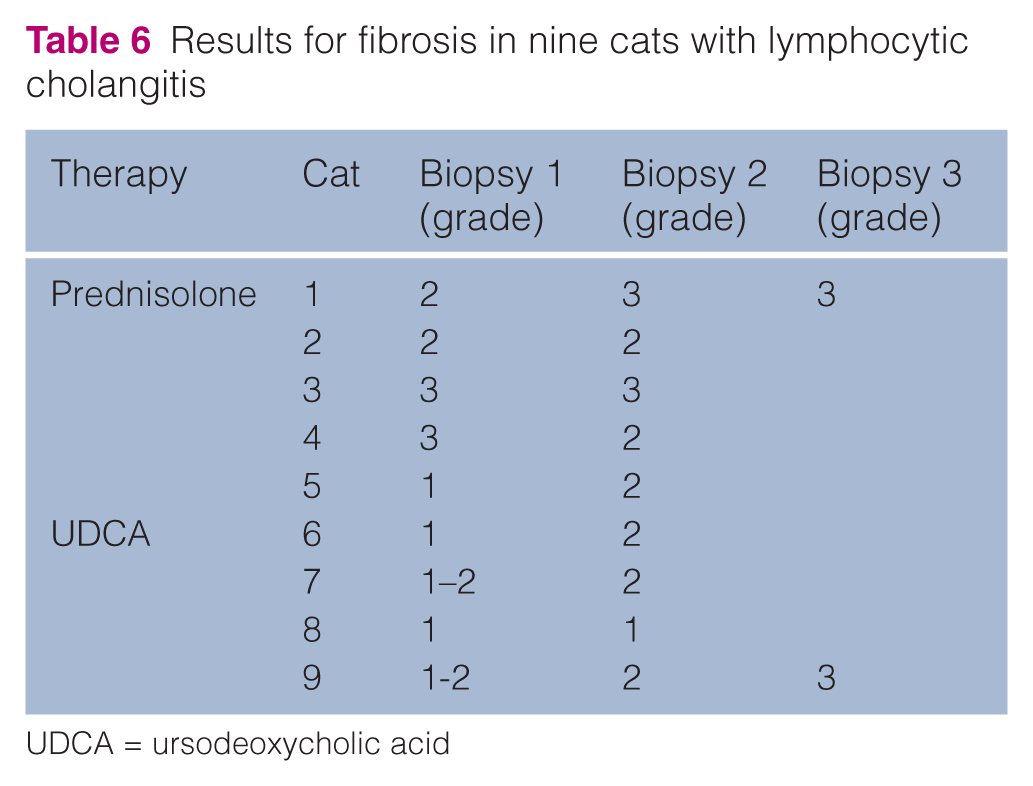
UDCA = ursodeoxycholic acid
Sixteen of 20 biopsies were successfully stained against α-SMA. However, except for the positive results in blood vessel walls, no other cells stained positive in the needle biopsies (grade 0). The two wedge biopsies did contain α-SMA positive cells, that is, HSC (grade 1) (Figure 1d).
We also identified concentric fibrosis in three LC patients (Figure 1c).
Proliferation and regeneration
Eighteen out of 20 biopsies of feline patients were successfully stained for Ki-67 (Figure 1f). Increased proliferation of fibroblasts was seen in the UDCA group compared with the prednisolone group (Table 7).
Proliferation of different cell types in the different treatment groups based on Ki-67 staining

UDCA = ursodeoxycholic acid
Overall, 15 biopsies were successfully stained with K19 (Figure 1e). In both the prednisolone and UDCA treatment groups, the number of bile ducts and liver progenitor cells remained stable. Furthermore, there was no difference in absolute numbers of bile ducts or progenitor cells between the two treatment groups.
Discussion
In liver disease, different cells (hepatocytes and cholangiocytes) can proliferate, and hepatocytes are the first to do so. 26 Only when regeneration capacity proves inadequate, progenitor cells (oval cells) residing in the canal of Hering will be activated.26–29 All cats with LC showed proliferation of cholangiocytes and bile ducts, which may be considered a hallmark of LC.
The group treated with UDCA was less severely affected by LC than the group treated with prednisolone. As the treatment grouping was based on period in time and not on severity of the disease, this is not due to selection of cases and must be attributed to serendipity.
When LC was first reported, knowledge of the disease was scarce, and it is possible that only very severe cases were referred to the academic veterinary hospital after veterinarians tried to treat their patients and did not succeed. When, later on, more was learned about LC, referring veterinarians might have able to recognise the disease at an earlier stage. Furthermore, owners may have been more willing to be referred because of increased prosperity and their desire to obtain the best possible health care for their pets. As the cause of the disease is still unknown, we can also not rule out an external, yet unknown, factor that has diminished the severity of the disease over time. Owing to these differences in the two treatment groups, it may have been easier to score improvement or deterioration in the prednisolone group.
The suppression of proliferation of lymphocytes by prednisolone has been described previously. 45 One earlier study reported no effect of UDCA on the proliferation of lymphocytes in mice. 46 Follicle formation of B-lymphocytes was seen in two biopsies from cats treated with prednisolone. Newly formed lymphoid structures have often been associated with chronic inflammatory processes and have been previously observed in LC.5,47 Similarly, these structures have been detected in PSC.48,49 However, lymphoproliferative disorders have been linked to the prolonged use of immunosuppressive drugs in human research.50,51 More research is needed to establish the nature of the follicle formation, and specifically the role of prednisolone in this process.
Despite treatment with UDCA, the fibrosis score increased or remained stable in all cats. This may be explained by the fact that the number of fibroblasts increased in 50% of the cats treated with UDCA, while these numbers did not increase in any felines treated with prednisolone. Fibroblasts actively contribute to liver fibrosis. 52 Historically, HSC were considered to be the main source of fibroblasts, but epithelial-to-mesenchymal transition from hepatocytes or biliary epithelial cells has been shown to be actively involved in accumulation of fibroblasts.52,53 Perhaps the main fibrotic component in cats with LC is not formed by HSC, but fibroblasts. Future research is needed to answer this question. Furthermore, the fixation method used does influence the quality of the liver tissues sampled as demonstrated before. 36 This might explain why no α-SMA-positive cells were identified in the needle biopsies of our feline patients. As a consequence, we were not able to confirm the positive correlation between the degree of fibrosis and α-SMA demonstrated previously. 54 Additionally, differences between diagnoses based on wedge biopsies or needle biopsies have been reported.55–58 Although no definitive agreement on required biopsy size has been reached, pathologists seem to agree that a diagnosis can be based on a specimen containing 4–10 portal triads.56–58 Furthermore, chronic liver disease in rats has been shown to be equally well represented by needle biopsies as larger samples of tissue taken by laparotomy. 57 Wedge biopsies offer more material to be evaluated, but may misrepresent a disease when taken from a superficial part of the liver. Needle biopsies are smaller, but do also take tissue from the inner parts of the organ. In judging fibrosis, researchers found that the extent of fibrosis was overestimated in 40 cases, underestimated in 50 cases, and equally scored in 21 cases when compared with wedge biopsies when evaluating hepatic biopsies in both dogs and cats. 55 Based on these previous findings, we conclude that we may have encountered differences between the samples taken by needle biopsy and the samples taken by wedge biopsy. However, these differences may be small as LC is a chronic disease affecting the whole organ, and the fact that the wedge samples were equally distributed among both treatment groups. Comparisons of needle and wedge biopsies in larger numbers for LC specifically can be considered a much needed subject for future research.
Concentric fibrosis has been alternately absent and present in reports on feline LC and is considered to be a hallmark of the disease in humans.5,6,59
Ki-67 has mainly been used for the evaluation of neoplasms, but it has also been used successfully on inflammatory bile ducts and chronic liver injuries in humans.60,61 Historically, feline studies have employed the MIB-1 clone for Ki-67, but, recently, SP6 was judged to be equal or even superior to MIB-1 in human research.62,63 Unfortunately, our studies found that the SP6 clone did not work on feline hepatic and intestinal control samples. We used additional tissue samples from dogs’ jejunum to verify our staining protocols, and these canine control samples were positive. Both feline and canine tissue samples were positive when the MIB-1 clone was used. Therefore, this study shows that the MIB-1 clone can be used successfully on feline hepatic tissue to evaluate the proliferation of several cell types.
Although this is, to our knowledge, the first study of the effects of therapeutics for LC on the histopathological features of the liver, several limitations apply. First, the small number of cats and biopsies limits the study’s power. Liver biopsies were taken to diagnose LC, but only a limited number of owners allowed multiple biopsies to be taken. In general, owners were primarily interested in the clinical improvement of their pet, and not in the histological development of the disease. The costs associated with taking liver biopsies might have attributed to this, as well as the perceived burden for the cat, including full anaesthesia. Second, low case numbers is a drawback observed in numerous feline studies, possibly associated with similar reasons as outlined above.64–66 Extrapolation or generalisation of data must therefore be undertaken with caution. However, publications based on low numbers can still be beneficial for the clinician, owner and animal, for instance to prevent expensive overtreatment. Furthermore, it provides directions for future research with larger multi-centred studies and facilitates meta-analyses.
Additionally, unequal numbers of sequential biopsies were available for various cats. Follow-up biopsies were also taken at different stages following the start of the therapy regimens. This complicates the process of comparison between the patients, biopsies, and efficacy of both treatment options. It would have been preferable to have identical groups of patients, with equal numbers of biopsies per patient, taken at set times from initiating the therapy in order to eliminate unwanted bias from the analyses. However, the retrospective nature of our research prevented this standardised set-up. Therefore, we must interpret the findings with caution as the duration of the therapy may have influenced the histopathological scores.
Unintentionally, all cats treated with UDCA had lower scores on percentage of inflammation at the start of the therapy than the cats treated with prednisolone. This, and the age difference between the two groups, might have biased outcomes. The retrospective character of the study further limits the possibilities for collecting additional data.
Based on the outcomes of this study, future research could help in collecting sequential biopsies at set times in order to fully compare the effect of therapeutics on liver tissue in prospective randomised studies. Furthermore, more feline patients are needed to clarify the effects of therapeutics on liver histology.
Conclusions
Inflammation decreased more in the group treated with prednisolone, while the number of cholangiocytes, progenitor cells and fibroblasts did not differ between the treatment groups. No difference was found for the amount of fibrosis between the groups treated with either prednisolone or UDCA.
Footnotes
Acknowledgements
We would like to thank Ronald Molenbeek, Ronald Kisjes and Ted van den Ingh for valuable advice and assistance on the immunohistochemistry stainings.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.