
Abstract
A 5-year-old, male neutered domestic shorthair cat was referred for investigation of lethargy, weight loss, pyrexia and upper respiratory tract signs. On computed tomography, an expansile, osteodestructive lesion in the right tympanic bulla was identified. A soft tissue mass extended from the bulla into the nasopharynx, cranium and subcutaneous tissues. The nasopharyngeal mass ruptured during handling, liberating purulent material from which Pasteurella multocida was isolated in pure culture. The lesion was most likely an atypical, abscessated nasopharyngeal polyp. The cat was treated with bulla osteotomy and antibiotics, and made a complete recovery.
Case Reports
A 5-year-old, male neutered domestic shorthair cat was presented for partial anorexia, lethargy and noisy breathing. A mild stertor had been present since kittenhood, but the noise had increased significantly in the week prior to presentation coincident with the development of nasal discharge. On physical examination, stertor, right-sided nasal discharge and elevated rectal temperature (39.3°C) were noted. Laboratory abnormalities included mild hyperglycaemia (10.64 mmol/l; reference interval [RI] 4.11–7.94 mmol/l) and hyperglobulinaemia (57 g/l; RI 25–45 g/l). Serology for feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV) (SNAP FIV/FeLV Combo; IDEXX Laboratories), and cryptococcal antigen (Crypto-LA Test; Inverness Medical Innovations) were negative. On presentation at referral to the Valentine Charlton Cat Centre 2 weeks later, complete anorexia for 1 week was reported. The cat had lost 330 g in body weight in 2 weeks (body condition score 2/5) A loud inspiratory stertor and increased inspiratory effort were present at rest. There was a copious, right-sided, mucoid nasal discharge, and the rectal temperature was 39.2°C. The cat was assessed as having right-sided caudal nasal cavity or nasopharyngeal disease. A nasopharyngeal polyp, nasopharyngeal stenosis, infection, foreign body and neoplasia were the major differential diagnoses.
Computed tomography (CT) of the head was performed under general anaesthesia using a 16-slice scanner (Philips Brilliance), 0.8 mm slice thickness, bone and soft tissue filters, an 11 cm image field of view and a 512 matrix. The cat was premedicated with methadone (0.3mg/kg; Physeptone, Aspen Pharmacare) and acepromazine (0.2mg/kg; ACP 2, Delvet) by intramuscular injection and induced with alfaxalone (1.3mg/kg; Alfaxan, Jurox) by intravenous (IV) injection and maintained on isoflurane in oxygen with spontaneous ventilation. Pre-contrast and 1 min post-contrast (7 ml iohexol, 350 mgI/ml, IV) images were acquired. Images were viewed using bone (WL 500, WW 3500), nasal (WL 480, WW 2500) and soft tissue (WL 25–60, WW 250–350) windows. The right tympanic bulla was markedly enlarged (Figure 1a) and filled with soft tissue attenuating material (Hounsfield units 20–30) that passed through three defects in the bulla wall (Figure 1b). The soft tissue attenuating material had moderate-to-marked rim enhancement and contained several small gas-filled cavities and centrally located, circular non-enhancing areas, suggesting fluid-filled cavities or focal necrosis (Figure 1c). A large defect was present in the craniolateral wall of the right tympanic bulla. The soft tissue attenuating material followed the course of the Eustachian tube into the nasopharynx where it filled the nasopharyngeal lumen causing ventral displacement of the soft palate and lateral displacement of the right hyoid bones. A large defect was present in the petrosal part of the right temporal bone caudal to the cochlear, which resulted in communication between the right tympanic cavity and right caudal fossa of the cranium. Soft tissue attenuating material passed through this defect caudally on the right caudal floor of the caudal fossa, extending to the level of the foramen magnum where it formed a right-sided 3 × 7 mm crescent-shaped mass with marked contrast enhancement that caused moderate leftward extra-axial displacement of the brainstem (Figure 1d). A third large defect was present in the lateral wall of the bulla through which soft tissue attenuating material passed into the subcutaneous tissue compressing the right external ear canal. Other regions of the wall of the right tympanic bulla were thin and incomplete with multiple, 1–2 mm focal areas of lysis. The septum dividing ventromedial and dorsolateral compartments of the tympanic bulla was destroyed (Figure 1b). The ventral regions of both nasal cavities, the choana and the left sphenoid sinus were filled with fluid and soft tissue attenuating material consistent with mucosal thickening. The right medial retropharyngeal lymph node was moderately enlarged and had heterogeneous contrast enhancement.

(a) Three-dimensional, volume-rendered computed tomography (CT) image of the caudoventral aspect of the skull (WL 344, WW 390) showing multiple, round-to-oval focal areas of lysis (black arrows) in the wall of the right tympanic bulla. The right epihyoid and stylohyoid bones (white arrow) are displaced laterally and ventrally by the enlarged right tympanic bulla. Crop and sculpt post-processing functions have been used to remove the image of the endotracheal tube that was superimposed on the tympanic bullae and hyoid bones in this view. The endotracheal tube is marked with a white asterisk. (b) Transverse, pre-contrast CT image of the skull at the level of the tympanic bullae made using a bone filter and viewed in a bone window (WL 500, WW 3500). The wall of the enlarged right tympanic bulla is thin and incomplete with a large defect in the lateral wall (white arrowhead) and multiple smaller defects in other regions of the wall. A defect is present in the right petrous temporal bone (white arrow) resulting in loss of the bony wall between the right tympanic cavity and the caudal fossa of the cranium. The right tympanic cavity is filled with soft tissue attenuating material and several small regions of gas. Soft tissue attenuating material is seen bulging into the nasopharynx (black asterisk), the right external ear canal is compressed and the right hyoid bones are displaced ventrolaterally (black arrow). (c) Transverse, post-contrast CT image at the level of the temporomandibular joints made using a soft tissue filter and viewed in a soft tissue window (WL 166, WW 545). Soft tissue attenuating material (white arrows) with moderate peripheral and ring-shaped regions of enhancement is seen filling the nasopharynx and causing severe ventral displacement of the soft palate. The endotracheal tube (white asterisk) is seen passing through the left side of the oropharynx. (d) Transverse, post-contrast CT image at the level of the caudal skull made using a soft tissue filter and viewed in a soft tissue window (WL 166, WW 545). The soft tissue attenuating material in the right tympanic bulla has a moderate heterogeneous contrast enhancement, with peripheral enhancement and multiple ring-shaped regions of enhancement (black arrows). A linear region of contrast enhancement is seen passing through the large defect in the right petrous temporal bone into the right ventral region of the caudal fossa of the cranium and there is mild leftward displacement of the brainstem (white arrow). Contrast-enhancing tissue is also seen passing ventromedially from the right tympanic bulla into the retropharyngeal region (white arrowhead). The endotracheal tube is marked with a white asterisk. R = right, L = left, white asterisk = endotracheal tube
Bilateral otoscopic examination was unremarkable. The soft palate was retracted to reveal a smooth, fluctuant, yellowish, glistening mass bulging into the nasopharynx (Figure 2). During biopsy, the mass collapsed, releasing yellow, mucoid fluid and revealing a thin wall. The cat was placed in dorsal recumbency, and the ventral area of the head and neck was aseptically prepared for access to the tympanic cavity through a ventral bulla ostectomy. The ventral surface of the enlarged bulla was easily palpable and was approached between the digastric and mylohyoid muscles. The tympanic cavity was opened using a Steinmann pin followed by a small bone rongeur to remove the thin bone. Yellow, mucoid fluid, similar to that observed during biopsy of the nasopharyngeal mass, drained from tympanic cavity. After taking samples for cytology, culture and histopathology, the bulla was carefully debrided using a small bone curette, flushed with 0.9% saline, and suctioned. No drain was placed, but the incision was closed only partially to allow for temporary drainage should the mucoid content of the bulla prove to be an infectious exudate. The wound was covered with a loose bandage. On initial extubation, the cat developed an obstructive respiratory pattern. Following re-induction with alfaxalone (1.4 mg/kg IV), re-intubation and administration of dexamethasone sodium phosphate (0.6 mg/kg IV; Dexadresson, Intervet) to reduce nasopharyngeal mucosal inflammation, the cat recovered uneventfully. Methadone (0.1 mg/kg IV) was administered every 4 h until discharge. Treatment with amoxicillin–clavulanic acid (24 mg/kg SC then 20mg/kg PO q12h × 5 days [Clavulox, Zoetis]), and marbofloxacin (3.5 mg/kg PO q24h × 28 days [Zeniquin, Zoetis]) was initiated while results were pending. The cat was bright and eating well, and the stertor had resolved at discharge from hospital the next day.
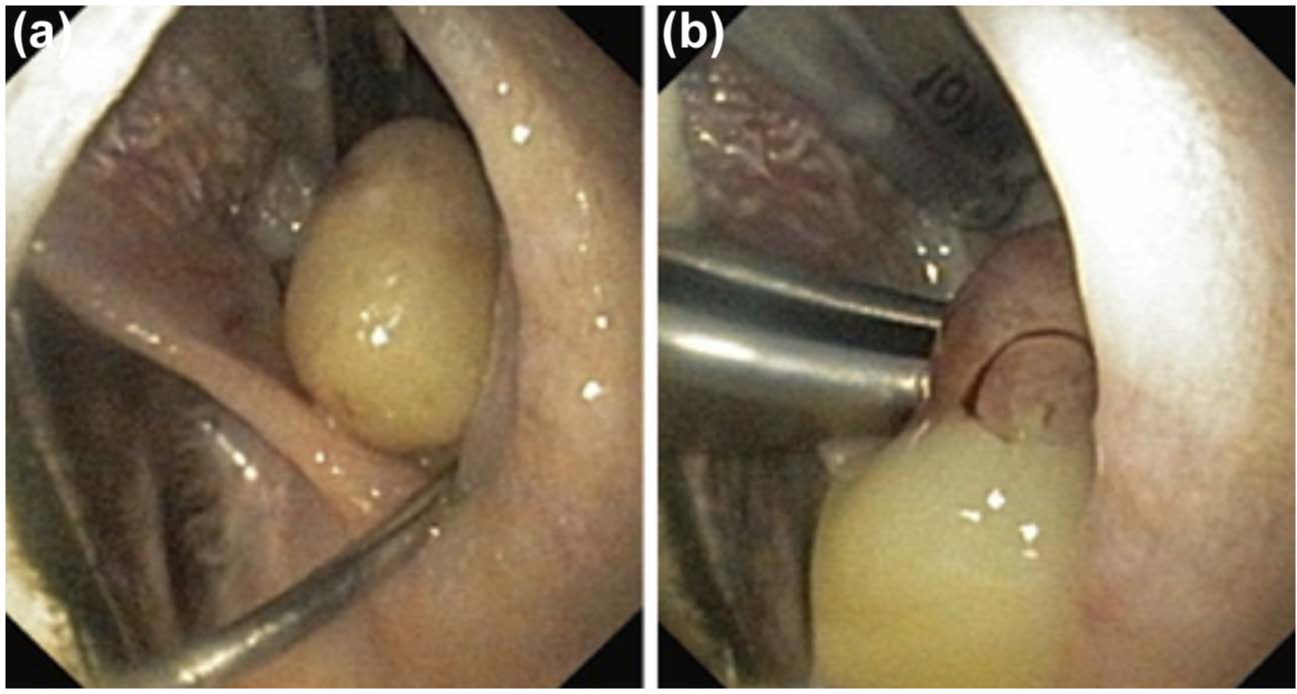
(a) The soft palate has been retracted using a spey hook revealing the polypoid mass in the nasopharynx. (b) Rupture of the abscessated polyp during handling
Cytological examination of fluid from the nasopharyngeal lesion and the tympanic bulla were similar, demonstrating mucus, numerous inflammatory cells (97% lytic neutrophils, 2% small lymphocytes, 1% macrophages) scattered clumps of large, plump, uniform, ciliated epithelial cells and occasional squamous epithelial cells and intra- and extracellular Gram-negative rods. Pasteurella multocida was isolated on aerobic culture of fluid from the nasopharyngeal lesion and from the bulla. Histopathological examination of biopsies from the wall of the nasopharyngeal lesion and the tympanic bulla were similar. There were elements of intact pseudostratified ciliated respiratory epithelium overlying a dense irregular connective tissue with a marked inflammatory infiltrate dominated by sheets of plasma cells and scattered small lymphocytes. Where epithelial surfaces were present, scattered neutrophils were interspersed in the superficial submucosa and epithelium with small pockets of luminal neutrophils, epithelial cells and haemorrhage evident. Occasional dilated modified apocrine glands containing amorphous to slightly vacuolated eosinophilic material and nuclear debris were present in the specimen from the external ear canal. The cat gained 750 g in 3 months. The owner reported no further clinical signs and no abnormalities were detected on physical examinations. The cat remains clinically normal at the time of writing 31 months after presentation.
The lesion in this case is presumed to be an atypical nasopharyngeal polyp. The acute illness is not typical for a nasophayryngeal polyp and is likely to be a consequence of P multocida infection. Another unusual feature is the extensive lysis of the bulla wall. Pathological expansion of the tympanic bulla has been described as a CT feature of feline nasopharyngeal polyps being present in all 13 cats studied. 1 However, in that study, thickening of the bulla wall was common. Bony proliferation of the bulla was also reported in a case of unilateral bulla expansion in a cat with upper respiratory tract (URT) signs. 2 In that case, the nasopharyngeal obstruction was attributed to direct compression by the bulla itself, rather than a soft tissue mass extending from the bulla, as was seen in the case reported herein.
The bony lysis of the bulla wall in our case may have been associated with the P multocida infection. Certain strains of P multocida produce a toxin, which has been demonstrated to inhibit osteoblast differentiation in vitro 3 and to be responsible for destruction of the nasal turbinates in atrophic rhinitis in pigs. 4 The bony lysis reported here permitted intracranial extension of the lesion through a large defect in the petrous temporal bone. In a previous description of intracranial extension of otitis media, the route taken by nasopharyngeal polyps was via the internal acoustic meatus. 5 Interestingly, clinical signs of intracranial involvement were not seen, despite extension of the lesion into the caudal fossa, presumably because the brainstem was displaced but not yet compressed.
Conclusions
This case highlights the importance of early advanced imaging in the investigation of URT disease in cats. It informs endoscopic investigation, sometimes rendering it unnecessary, as in this case, and identifies selection of sites for biopsy, which can be performed under the same anaesthetic.
Footnotes
Supplementary material
Video 1: Three-dimensional volume rendered CT movie of the caudoventral aspect of the skull (WL 344, WW 390) showing the large defects in the rostral and lateral aspects, and the multiple round-to-oval-shaped focal areas of lysis in the wall of the right tympanic bulla. The right epihyoid and stylohyoid bones are displaced laterally and ventrally by the enlarged right tympanic bulla. Crop and sculpt post-processing functions have been used to remove the image of the endotracheal tube that was superimposed on the tympanic bullae and hyoid bones in this view.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.