
Abstract
The aim of this study was to investigate the short- and long-term morbidity and mortality associated with urethral rupture in cats. Medical records were reviewed from four veterinary hospitals. Diagnosis was made from retrograde urethrography or direct visualisation during surgery. Location of rupture was categorised as pre-, intra- or post-pelvic. Follow-up data were collected from referring veterinarians. Sixty-three cats were included in the study of which, males predominated (88.9%). Trauma was the most common cause (n = 35; 55.6%) with the remainder due to iatrogenic injury. Forty-eight cats (88.9%) were treated surgically and six (11.1%) managed conservatively. Significant differences between cats suffering traumatic versus iatrogenic injury included the presence of musculoskeletal injuries (P <0.001); the location of rupture (P <0.001); the degree of rupture (P <0.001); definitive management (P <0.001) and short-term complications (P = 0.026). Short-term complications were significantly associated with the following: musculoskeletal injuries (P = 0.012); uroabdomen/uroretroperitoneum (P = 0.004); azotaemia (P = 0.021); postoperative urinary diversion (P = 0.036) and >1 surgery performed (P = 0.006). Forty-seven cats (74.6%) survived to discharge. Prognostic factors associated with survival to discharge included the presence of musculoskeletal injuries (P = 0.017); cause of rupture (P = 0.017); location of rupture (P = 0.039) and definitive management (P = 0.020). Twenty-four cats (57.1%) suffered short-term complications and 10 (27.0%) suffered long-term complications. Of those cats surviving to discharge 30 (71.4%) had a good outcome. Median follow-up was 16 months. Outcome was significantly associated with cause of rupture (P = 0.04); short-term complications (P = 0.03) and long-term complications (P <0.001). In conclusion, a significantly greater proportion of cats with iatrogenic injuries survived to discharge and had a good outcome compared with those that suffered trauma.
Introduction
Urethral rupture is uncommon in dogs and cats,1–3 and may occur as a result of vehicular trauma, pelvic fractures, bite wounds, penetrating injuries, urethral calculi and iatrogenic injury during urethral catheterisation or surgery.4–6 A previous report in cats found that the most common cause was iatrogenic injury from urethral catheterisation. 6 Clinical signs depend on the location, severity and duration of the injury, and the ability to urinate may or may not be affected. 5 Clinical signs include haematuria, dysuria, anuria, inguinal/perineal swelling, hind-limb skin necrosis, 7 abdominal distension, depression and anorexia. 8
Management of urethral injuries requires stabilisation of the animal with evaluation of haemodynamic status, correction of metabolic derangements and provision of urinary diversion. There are three options for treatment of urethral rupture: second-intention healing with temporary diversion of urine using a urethral catheter or cystostomy tube; primary repair; and permanent urinary diversion via an urethrostomy. 9 Primary repair may be challenging in cats owing to the small size of the urethra and is associated with complications such as stricture formation and urethral dehiscence. 4 Although permanent urethrostomies can be used as an alternative, complications such as recurring urinary tract infections (UTIs), stricture formation and incontinence can be frequent, and, in general, the rate of complications is greater following urethrostomy at more cranial sites.4,10
As urethral injuries are uncommon there is a relative paucity of information on these injuries in the literature, with most studies including case reports or retrospective analyses with a small number of cases. The purpose of this study was to describe the signalment, clinical findings, management and outcome of a large population of cats with urethral rupture. The study also aimed to investigate the factors associated with survival to discharge and outcome, and to compare and contrast traumatic urethral injuries and those attributable to iatrogenic damage. We hypothesised that cats with a traumatic injury and those with a more cranial site of urethral rupture would have a poorer survival and/or outcome.
Materials and methods
The medical records of all cats treated for urethral rupture were reviewed between March 2002 and February 2012 from the following referral hospitals: The Queen Mother Hospital for Animals at the Royal Veterinary College, The Queen’s Veterinary School Hospital at the University of Cambridge, the Langford Small Animal Hospital at the University of Bristol and the Rosemary Lodge Hospital at the Bath Veterinary Group. Urethral disruption was confirmed by positive contrast radiography and/or direct visualisation during surgery. Location of urethral rupture was divided into the following three categories from radiographic studies: pre-pelvic (defined as the length of urethra from its origin at the neck of the bladder to the cranial aspect of pubis); intra-pelvic (defined as the length of urethra from the cranial aspect of the pubis to the caudal aspect of the ischial tuberosity); post-pelvic (defined as the length of urethra from the caudal aspect of the ischial tuberosity until its termination). The following information was recorded: signalment, cause of urethral rupture, presence of concurrent injuries, presence of azotaemia (urea >10 mmol/l and creatinine >140 μmol/l) and hyperkalaemia on admission, anatomical location of rupture (pre-, intra- or post-pelvic), extent of rupture as assessed by visualisation at surgery (complete or partial), duration of injury prior to diagnosis, definitive management (final management used to treat the urethral rupture, including either a surgical procedure or conservative management with urinary diversion), method and duration of pre-operative and/or postoperative temporary urinary diversion, presence of complications and survival to discharge. In those cats that were euthanased, the reason for euthanasia was recorded, if available.
Follow-up data were collected by telephone conversations with the referring veterinarians and were divided into short- (STC) and long-term urinary complications (LTC). STCs were defined as those that occurred within 10 weeks of definitive management (including immediate postoperative complications). LTCs were defined as those that occurred after 10 weeks after definitive management. Overall outcome was considered to be good if the cat had no complications, fewer than two occurrences of mild complications that were either easily treatable or required no treatment. Overall outcome was considered to be poor if the cat had had severe complications compromising its ability to urinate, recurrent (more than two) complications or had been euthanased for reasons relating to its lower urinary tract.
Statistical analysis
Statistical analysis was performed using a statistical software package (PASW Statistics 18.0.0; Education SPSS). Data were assessed graphically for normality. Median and range was reported for non-normally distributed data, which was compared with the Mann–Whitney U-test. Categorical data were reported as proportions and compared with the χ2 or Fisher’s exact tests, as appropriate. Statistical significance was set at P <0.05.
Results
Signalment
Sixty-three cats were included in this study. Fifty-six cats (88.9%) were male (53 neutered; three entire) and seven (11.1%) were female (all neutered). Forty-seven cats (74.6%) were domestic short- or longhair, with 16 cats (25.4%) represented by the following pedigree breeds: British Shorthair (four); Burmese (three); Birman (two); Persian (two); and one each of the Ragdoll, Somali, Siamese, Cornish Rex and Exotic Shorthair. The median age was 36 months (range 4 months to 12 years).
Clinical findings
Thirty-five of 63 cats (55.6%) suffered urethral rupture due to trauma. Seen, or suspected, vehicular trauma was the cause in 33 cats and bite wounds in the remaining two. Twenty-eight cats (44.4%) suffered urethral rupture due to iatrogenic damage. Damage was due to attempted urethral catheterisation in 25 cats, failed perineal urethrostomy (PU) in two cats and inadvertent damage during ovariohysterectomy in one cat.
Information on ability to urinate was available for 13 cats. One cat (7.7%) was reported to urinate normally, whereas the rest exhibited stranguria, dysuria, oliguria, or anuria.
Twenty-five cats had concurrent musculoskeletal trauma with the following injuries: multiple pelvic fractures (13), hind-limb fractures (six); open wounds (five); and a caudal vertebral fracture (one). Other concurrent injuries included uraemic cellulitis (28); uroabdomen (12); neurological deficits (four); bladder rupture (three); abdominal wall rupture (three); uroretroperitoneum (three); pleural effusion (one); pneumothorax (one); urothorax (one); hydronephrosis (one); rectal tear (one); and penile thrombosis (one).
Serum biochemistry was performed in 36 cats at the time of hospital admission. Twenty-nine of these cats (80.6%) were azotaemic. Information on potassium concentration was available for 31 cats: 13 (46.4%) were hyperkalaemic and three (10.7%) were hypokalaemic. In the remaining 15 cats potassium concentration was within the reference interval.
Urethral rupture was confirmed by contrast radiography in 62/63 cats and by exploratory surgery in one cat. The location of rupture was recorded for 61/63 cats. Of the 55 male cats, 26 suffered intra-pelvic ruptures (47.2%), 26 suffered post-pelvic ruptures (47.2%) and three suffered pre-pelvic ruptures (5.6%). Of the six female cats, four suffered intra-pelvic ruptures (66.7%) and two suffered pre-pelvic ruptures (33.3%). A description of the extent of the urethral rupture was available for 24 cats, with 14 suffering partial rupture (58.3%) and 10 suffering complete rupture (41.7%).
The median time from injury to diagnosis was 2 days (range 0–20 days).
Management of urethral discontinuity
Seven cats were euthanased prior to definitive management. The reasons for euthanasia included the owner declining treatment owing to the diagnosis of urethral rupture (three); the owner declining a pre-pelvic urethrostomy (PPU) (one); the presence of multiple injuries alongside neurological deficits (one); the development of sepsis (one); and the urethra being too short to repair (transection at the bladder neck) (one). One cat died prior to definitive management owing to the development of septic shock. One cat did not require any definitive management for the urethral injury as it was very minor and resolved by itself.
Fifty-four cats underwent definitive management for their urethral injuries, with six (11.1%) managed conservatively with temporary urinary diversion and 48 (88.9%) undergoing surgical correction. The median duration of temporary urinary diversion in the conservatively managed cases was 6 days (range 3–25 days). Twenty-six cats had temporary urinary diversion provided pre-operatively for a median duration of 7 days (range 2–21 days). The methods of urinary diversion used were as follows: cystostomy tube in 19 (73.1%); urethral catheter in five (19.2%); urethral catheter and cystostomy tube in two (7.7%). The method chosen for urinary diversion was at the discretion of the clinician. In those cases where both a cystostomy tube and a urethral catheter were used, the urethral catheter was used, in part, to act as a ‘splint’. All cystostomy tubes were surgically placed. The reason for providing pre-operative urinary diversion was recorded in 11 cats and included the following: conservative management attempted initially but failed (five); the cat was considered too unstable for surgical correction (four); to allow injured soft tissues to heal prior to definitive urethrostomy (two).
In the male cats, the surgical procedures included PU in 20 cats (47.6%), PPU in 18 (42.9%) and urethral anastomosis in four (10.0%). In the female cats, the surgical procedures included urethral anastomosis in three cats (50.0%), PPU in two (33.3%) and vaginourethroplasty in one (16.7%). Nine cats (18.8%) underwent more than one surgical procedure. The cat treated with vaginourethroplasty has been previously reported. 4
Twenty-nine cats had temporary urinary diversion provided postoperatively for a median duration of 7 days (range 1–37 days). Seventeen of these cats had also received pre-operative urinary diversion. The methods of urinary diversion used were as follows: urethral catheter in 15 (40.5%); cystostomy tube in 12 (32.4%); urethral catheter and cystostomy tube in 10 (27%). The method chosen for urinary diversion was at the discretion of the clinician. As previously, in those cases with both types of urinary diversion, the urethral catheter was also placed, in part, to act as an urethral ‘splint’.
Seven cats were euthanased after definitive management. The reasons for euthanasia were recorded for six cats, and included failure of conservative management and the owner declining surgical correction (two); development of an aortic thrombo-embolism 24 h postoperatively (one); development of sepsis (one); the presence of severe anaemia and multiple injuries (one); and the development of extensive urethral necrosis after attempted conservative management (one). One cat died after definitive management owing to suffering a cardiac arrest approximately 12 h following a PPU.
The median duration of hospitalisation was 19 days (range 3–60 days).
Traumatic versus iatrogenic urethral rupture
There was no statistically significant difference in the sex, breed or age of cats between the two groups. A summary of the significant results are shown in Table 1.
Summary of significant findings with P-values shown
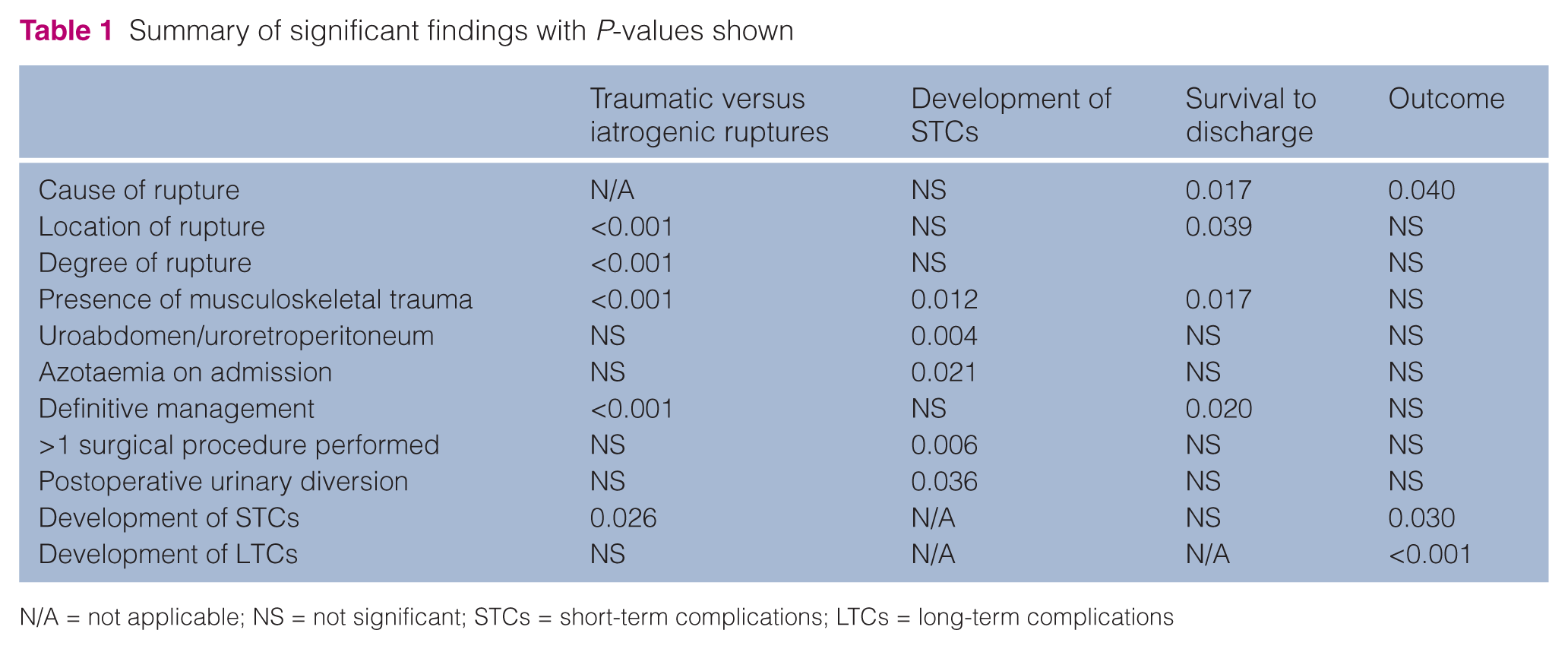
N/A = not applicable; NS = not significant; STCs = short-term complications; LTCs = long-term complications
The presence of concurrent musculoskeletal trauma was significantly different between the two groups (P <0.001), with 23/34 cats (67.6%) in the trauma group suffering concurrent musculoskeletal injury compared with 2/28 cats (7.1%) in the iatrogenic group. Both of these cats had a wound on the hind-limb with concurrent uraemic cellulitis. Thirteen of the cats with trauma (37.1%) had concurrent pelvic fractures.
The location of the rupture was significantly different between the two groups (P <0.001). Of the 34 cats in the trauma group four (11.8%) suffered a pre-pelvic rupture, 25 (73.5%) suffered an intra-pelvic rupture and five (14.7%) suffered a post-pelvic rupture. Of the 27 cats in the iatrogenic group one (3.7%) suffered a pre-pelvic rupture, five (18.5%) suffered an intra-pelvic rupture and 21 (77.8%) suffered a post-pelvic rupture. The degree of rupture was also significantly different between groups (P <0.001), with all cats suffering a partial rupture in the iatrogenic group, but only 3/13 cats (23.1%) in the trauma group.
The definitive management was significantly different between the two groups (P <0.001) (see Figure 1). Of the 28 cats in the trauma group, three (10.7%) underwent a PU, 17 (60.7%) underwent a PPU, five (17.9%) underwent an anastomosis, two (7.1%) underwent conservative management and one (3.6%) underwent vaginourethroplasty. Of the 26 cats in the iatrogenic group 17 (65.4%) underwent a PU, three (11.5%) underwent a PPU, two (7.7%) underwent an anastomosis and four (15.4%) underwent conservative management.

Bar chart demonstrating the difference in definitive management between the traumatic urethral ruptures and those attributable to iatrogenic damage. PU = perineal urethrostomy; PPU = prepubic urethrostomy; VU = vaginourethroplasty
There was a significant difference in the development of STCs between the two groups (P = 0.026), with 17/23 cats (73.9%) in the trauma group developing STCs in comparison to only 11/26 cats (42.3%) in the iatrogenic group. There was no significant difference in the development of LTCs or overall outcome between the two groups.
Survival and outcome
Forty-seven cats (74.6%) survived to discharge, 14 (22.2%) were euthanased prior to discharge and two (3.2%) died prior to discharge. Twenty-five of 28 cats (89.3%) with an iatrogenic rupture and 22/35 cats (62.9%) with a traumatic rupture survived to discharge. There was a statistically significant difference in survival to discharge between these two groups (P = 0.017). Fifteen of 25 cats (60%) with concurrent musculoskeletal trauma and 32/37 cats (86.5%) without concurrent musculoskeletal trauma survived to discharge. There was a statistically significant difference between these two groups (P = 0.017). Twenty-three of 26 cats (88.5%) with post-pelvic ruptures, 21/30 (70.0%) with intra-pelvic ruptures and 2/5 (40.0%) with pre-pelvic ruptures survived to discharge. There was a statistically significant difference in survival to discharge between the different categories of rupture (P = 0.039). All cats treated with PU, 17/20 cats (85.0%) with PPU, 4/6 cats (66.7%) with conservative management, 4/7 cats (57.1%) with anastomosis and one cat with vaginourethroplasty survived to discharge. There was a statistically significant difference in survival to discharge between the different categories of treatment (P = 0.020).
Twenty-four/42 cats (57.1%) suffered STCs occurring within a median duration of 3 weeks (range 1–10 weeks). These complications included the following: UTI confirmed by urine culture and sensitivity (14); stricture (eight); incontinence (five); peristomal skin necrosis (four); urine extravasation (three); urine scalding (two); detrusor atony (one); uroabdomen (one). Four of 14 UTIs (28.6%) were multidrug resistant. One of the cats that developed peristomal skin necrosis has previously been reported. 11 Short-term complications were statistically significantly associated with the following: presence of musculoskeletal injuries (P = 0.012); presence of uroabdomen/uroretroperitoneum (P = 0.004); azotaemia on arrival (P = 0.021); more than one procedure carried out (P = 0.006); and postoperative urinary diversion (P = 0.036). The specific type and duration of postoperative urinary diversion were not found to be significant, however.
Long-term follow-up (>10 weeks) was available for 37/47 cats (78.7%). The median duration of follow-up was 16 months (range 3–100 months). Ten of 37 cats (27.0%) suffered LTCs occurring within a median duration of 38 months (range 6–78 months). These complications included the following: UTIs (six); incontinence (three); recurrent lower urinary tract disease (non-obstructive) after a traumatic urethral injury (one); stricture (one). Thirty-four cats were alive at follow up; one cat was euthanased at 9 months owing to a urethral stricture following PPU and one cat was euthanased at 6 months for unrelated reasons (gastric neoplasia).
Overall outcome was determined for 42/47 cats. Four cats were lost to follow-up and there was no follow-up for one cat, which was treated at the end of the study period, and therefore records were only available until discharge. Overall outcome was good in 30 cats (71.4%) and poor in 12 (28.6%). Of these 12 cats, five had been euthanased within 10 weeks of discharge. The reasons for euthanasia were as follows: one as a result of ongoing urinary tract problems, two owing to severe urethral strictures and two for unknown reasons. Overall outcome was statistically significantly associated with cause of rupture (P = 0.04), STCs (P = 0.03) and LTCs (P <0.001). Eighteen of 21 cats (85.7%) who suffered an iatrogenic rupture had a good outcome compared to only 12/21 (57.1%) who suffered a traumatic rupture. Sixteen/18 cats (88.9%) that did not suffer STCs had a good outcome in comparison to 14/24 cats (58.3%) with STCs. All cats without LTCs had a good outcome compared to 3/10 cats (30%) with LTCs.
Discussion
In this study the majority of cats sustained traumatic urethral ruptures (55.6%), with the most common cause being seen, or suspected, vehicular trauma. This is in contrast to previous reports where an iatrogenic aetiology has been reported in 73.7–79.3% of cases.5,6 Only 44.4% suffered an iatrogenic urethral rupture, and most were attributable to damage from catheterisation due to urethral obstruction. The smaller proportion of iatrogenic ruptures could reflect a different population. Cases in previous studies were obtained from referral veterinary hospitals, similarly to this study; however, one of the referral hospitals from this study has a large first opinion and emergency service, which may have influenced the results. The previous studies reported populations of cats from the USA 6 or France. 5 We sampled a population of cats from the UK and also analysed a larger number of cats (n = 63) in comparison to the other studies (n = 29; n = 11, respectively). Therefore, it may be more representative of the total population.
Urethral injury has been reported to occur more commonly in male cats, consistent with the results of this study. One possible explanation is the anatomy of the urethra. The male urethra is attached to the ischium via the ischiocavernosus and ischiourethralis muscles;12,13 therefore, it may be less able to tolerate traction or shearing forces resulting from abdominal trauma. The male urethra has a smaller diameter, which can predispose to urethral obstruction and thus require treatment by catheterisation. Temperament may also contribute with increased roaming behaviour in males, subsequently leading to a higher risk of vehicular trauma. 7
In dogs, traumatic urethral rupture is frequently associated with pelvic fractures,2,3,6 with a reported incidence of 85.7% 6 of urethral injuries presenting with concurrent pelvic fractures. However, only 37.1% of trauma cases in this study had concurrent pelvic fractures. This indicates that, unlike dogs, blunt trauma without pelvic fractures can commonly lead to significant urethral injury in cats. This finding, in combination with the fact that urination may not necessarily be affected, 5 highlights the difficulty in identifying urethral injuries in cats unless they are actively investigated. Therefore, urinary tract injury should be suspected in any cat with abdominal or caudal trauma and positive contrast radiography should be considered, regardless of the presence or absence of pelvic fractures.
This study identified several significant differences between cats suffering traumatic urethral rupture and those suffering iatrogenic rupture. The presence of musculoskeletal injuries was significantly different between the two groups, with a higher proportion of animals with these injuries in the trauma group. This finding is expected as vehicular trauma can cause multiple injuries simultaneously, with musculoskeletal trauma one of the most commonly reported. 2 Iatrogenic damage to the urethra is less likely to be associated with musculoskeletal injury; however, significant wounds can develop in association with uraemic cellulitis, as seen in two cats in this study.
Location of rupture and definitive management were also significantly different between the two groups. Intra-pelvic rupture was most common in the trauma group and post-pelvic rupture most common in the iatrogenic group. Previous studies have reported that damage from urethral catheterisation commonly damages the penile urethra, 14 which would be classified as post-pelvic in our study. This is likely to be owing to the urethral anatomy in this region, with the presence of the sigmoid flexure and the relatively smaller diameter of the lumen. 15 The difference in the definitive management between the two groups reflects the difference seen in the location of the rupture, which naturally will affect what surgical treatments are possible. Thus, the majority of cats in the trauma group underwent a PPU and those in the iatrogenic group underwent a PU.
This study identified that traumatic injury was more likely to be associated with complete rupture of the urethra in comparison to iatrogenic injuries. The vast majority of cases in the iatrogenic group were due to damage from attempted catheterisation, and it is unlikely that complete transection of the urethra would result with passage of a catheter. In traumatic incidents, larger or shearing forces would be involved in the initial urethral injury; therefore, complete rupture would be more likely. However, degree of rupture was not found to be associated with survival to discharge or outcome. This suggests that if complete tears are managed appropriately then these animals should still be able to have a favourable outcome.
The presence of STCs was significantly different between the two groups, with significantly more STCs reported in the traumatic group. In this study all musculoskeletal injuries affected the hindquarters of the cats. Trauma to this area can lead to bruising and haematoma formation, inflammation, tissue oedema and open wounds. These factors could reduce the healing potential of the tissue, 16 which is a concern, particularly when considering treatment by urethrostomy. Indeed, pre-operative urinary diversion was provided and surgery was delayed in two cases in this study in order to allow healing of this region and improvement in the future urethrostomy site. Whether the presence of compromised soft tissue during definitive management increases the risk of developing a STC is uncertain, but this factor may warrant further investigation.
The types of STCs were similar between the two groups, with UTIs most frequently identified. A large number of animals had pre-operative and/or postoperative urinary diversion, and UTIs are a recognised complication of the use of cystostomy tubes 17 and urethral catheters.18,19 Indeed, the use of postoperative urinary diversion was significantly associated with the development of STCs. UTIs are also a recognised complication of permanent urethrostomy techniques.10,20 Although 28.6% of UTIs were multidrug resistant, all short-term UTIs resolved with appropriate antibiotic therapy.
STCs were significantly associated with the presence of uroabdomen and uroretroperitoneum. Interestingly, 6/8 cases (75%) that developed urethral strictures in the short-term period (<10 weeks) presented with uroabdomen. Exposure of the urethra to urine is known to delay urethral healing and increase periurethral fibrosis, 21 which could lead to increased stricture formation. However, it was not possible to define any relationship between uroabdomen and subsequent stricture formation with the present data.
Prognostic factors associated with survival to discharge included cause of rupture, presence of musculoskeletal injuries, location of rupture and definitive management. In agreement with our hypothesis, cats with traumatic urethral injuries were less likely to survive to discharge. These animals tended to have multiple injuries, and a previous study identified that the presence of multiple injuries is a negative prognostic factor. 6 This study was able to show that specifically concurrent musculoskeletal trauma was associated with reduced survival. Multiple injuries may lead to a more compromised animal with a poorer overall prognosis. The cat may require more intense management and treatment for several different injuries, which would increase the overall cost of treatment. This can lead to euthanasia before treatment is attempted, and in the current study three cats were euthanased before definitive management because of the diagnosis of urethral rupture. These cats were included in the data analysis because financial issues and the overall prognosis for recovery are important factors that the owner must take into consideration before embarking on treatment of their pet.
Location of rupture and definitive management were also associated with survival. Pre-pelvic rupture and primary repair had the worst survival, with only 40% and 57.1%, respectively, surviving to discharge, which is in agreement with our hypothesis. Cranial urethral injuries are difficult to repair, with options including a PPU, 10 sub-pubic urethrostomy 22 or transpelvic urethrostomy 23 if the urethra is long enough, or urethral anastomosis. 24 One cat was euthanased as the urethra was too short to repair as it had ruptured at the site where it joins the bladder.
Literature regarding optimal treatment for urethral rupture in the cat is relatively limited. Extrapolation from the canine literature suggests that injuries to the pelvic urethra should be managed by urethral anastomosis over a urethral catheter with concurrent urinary diversion, 4 and this is how seven cats were managed in this study. A further two cats had anastomosis for their first surgical procedure, but surgical revision was required and so their definitive management differed. Follow-up information was available for 7/9 of these cats. Stricture formation can be common with this management; however, clinical signs of dysuria are generally only seen when narrowing of the urethral diameter exceeds 60%. 25 In this study, the stricture rate was 21.4% (9/42 cats). Three of these cats underwent urethral anastomosis, meaning that, overall, 3/7 cats (42.8%) which had anastomosis developed a clinically significant stricture. In the human literature there has been a shift away from primary anastomosis as it has led to unacceptable rates of impotence and incontinence, favouring, instead, suprapubic urinary diversion with delayed urethroplasty 3–6 months later or early endoscopic realignment of the damaged section of the urethra.26,27 However, in this study, urinary incontinence was not reported as a complication for any cat that underwent anastomosis; therefore, incontinence may not be as important a complication after this type of management in cats in comparison to humans.
Overall outcome was good in 71.4% of cases. Factors significantly associated with outcome included cause of rupture and the presence of STCs and LTCs. Location of rupture was not associated with outcome, however, refuting this part of our hypothesis. The finding that traumatic cases had a poorer outcome is expected, as these cases tended to be more severely affected with a greater proportion having concurrent musculoskeletal trauma and developing STCs. Some STCs and LTCs can be severe and considerably affect the animal’s quality of life, necessitating further treatment or euthanasia, which can ultimately lead to a poor outcome. Indeed, the post-discharge mortality rate was 14.3%. Overall 5/6 of the cases euthanased after discharge were euthanased in the short-term period (<10 weeks), which may suggest that STCs have a greater effect on outcome than LTCs.
Limitations include the retrospective nature of the study, where not all information could be gathered from all the medical records available. A certain amount of variability was introduced owing to the recruitment of cases from numerous hospitals; therefore, multiple clinicians were involved in the management of these cats. This study also includes male and female cats. Female cats with urethral injuries have not been reported in the literature, which may mean that the results of this study are not comparable to previous studies. There are gender differences in location of rupture and definitive management. In female cats the urethra enters the vestibule at the caudal aspect of the pubic symphysis 28 and therefore it is not possible for a female cat to suffer a post-pelvic urethral rupture. Furthermore, female cats cannot be treated with PU and vaginourethroplasty cannot be performed in male cats for obvious reasons. Therefore, the two genders have been described separately in these sections of the descriptive statistics and this factor was taken into account during the statistical analysis to avoid bias.
Conclusions
Urethral rupture is most commonly caused by traumatic injury and is most often seen in male cats. Significant urethral injury can occur despite the absence of pelvic fractures; thus, urethral rupture should be suspected in any cat which has suffered abdominal trauma. STCs are seen in the majority of cases and may have a greater effect on outcome than LTCs. The results indicate that with appropriate treatment the prognosis for urethral rupture is good; however, a significantly greater proportion of cats with iatrogenic injuries survived to discharge and had a good outcome compared with those that suffered trauma.
Footnotes
Acknowledgements
We would like to thank the veterinary hospitals approached in this study for inclusion of their cases, and the veterinary surgeons, nurses and students involved with their management.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Elena Addison received the 2013 JFMS Resident Best Paper Award for this study.