
Abstract
This case report describes the successful treatment of a Persian cat diagnosed with intra-abdominal fungal pseudomycetoma causing hypercalcaemia and constipation due to an extra-luminal mechanical obstruction of the colon. Treatment included surgical excision, supportive care and itraconazole for 6 months.
Case Report
An adult male castrated Persian cat of unknown age and weighing 3.5 kg was referred to the Hebrew University Veterinary Teaching Hospital with a chief complaint of constipation of 1 month duration and intermittent vomiting. The cat was adopted as an adult stray 5 years prior to presentation. At the time of adoption he suffered from hind limb lameness and skin lesions, which were tentatively diagnosed as dermatophytosis. Prior to the referral the constipation was treated with antibiotics, deworming, subcutaneous (SC) fluids, frequent enemas, canned food, laxatives, pro-motility drugs and gastrointestinal protectants, with no resolution.
On presentation, the cat was bright, alert and responsive, with a body condition score of 3/9. Physical examination was unremarkable. Complete blood count, serum biochemistry and urinalysis were unremarkable, except for a total (tCA; 13.9 mg/dl) and ionised hypercalcaemia (iCa; 1.819 mmol/l, range 0.9–1.35 mmol/l). Thoracic radiographs were unremarkable; however, a single, smooth soft tissue density mass, 3 cm in diameter, ventral to the seventh lumbar vertebra and causing narrowing of the colon at the pelvic inlet was seen on the abdominal radiographs. Abdominal ultrasound was performed, and a heterogenic mass 3 cm in diameter with peripheral vascularisation was seen in the caudal abdominal and cranial pelvic cavities.
A rectal examination under sedation confirmed the presence of a sub-lumbar mass compressing the colon with no intra-luminal obstruction.
Ultrasound-guided fine needle aspirates were obtained from the mass, the spleen and the liver. Cytology of the mass was consistent with a pyogranulomatous-to-granulomatous reaction. Pyknotic neutrophils, phagocytising neutrophils, highly reactive macrophages, red blood cells and cellular debris were seen on direct smears made from a fine needle aspirate of the mass. Cytology of the spleen and liver was unremarkable. As the underlying cause was not identified, the main differential diagnoses were poorly exfoliating neoplasia (eg, sarcoma), or an unusual bacterial or fungal granuloma. Foreign body migration or feline infectious peritonitis were considered less likely given the hypercalcaemia.
Treatment with laxatives [lactulse (Laevolac; Fresenius-Kabi) 670 mg/ml, 1.5 ml PO, q8h] and pro-motility agents [metoclopramide (Pramin; Rafa Laboratories) 0.5 mg/kg, PO, q8h,and cisapride suspension (Prepulsid; Janssen Pharmaceuticals) 1 mg/ml, 0.5 mg/kg PO q8h] was continued; however, vomiting and diarrhoea persisted, and calcium levels remained high (iCa: 1.819 mmol/l; tCa: 13.92 mg/dl). Computed tomography was performed 1 week later to further assess the mass and to assist in surgical planning (Figure 1). Exploratory surgery of the abdominal and pelvic cavities was performed, including pubic osteotomies. A 6 cm × 3 cm irregular mass attached to the sacrum was found. The mass was de-bulked as complete excision was impossible without compromising vital structures, and the excised tissue was submitted for histopathology. The specimen consisted of fibrous tissue embedded with numerous round mats composed of fungal hyphe, suspected to be fungal pseudomycetoma. Unstained tissue sections of 4–6 μm were mounted on Superfrost-Plus slides (Thermo Scientific) for immunohistochemistry. The immunohistochemical staining was performed by the indirect peroxidase anti-peroxidase technique with a panel of mono- and polyclonal antibodies reacting specifically with the aetiological agents of aspergillosis, candidosis, cryptococcosis, dermatophytosis, fusariosis, scedosporiosis (pseudallescheriosis), geotrichosis and zygomycosis, as previously described.1–4 Reactivity of fungal elements in this case was obtained only by a heterologously absorbed, dermatophyte-specific antibody raised against Tricophyton mentagrophytes and reacting only with Trichophyton and Microsporum species (Figure 2). Treatment with itraconazole [Sporanox (Janssen Cilag) 10 mg/kg, PO, q24h) was initiated.

Computed tomography of the caudal abdominal cavity of an adult Persian cat with intra-pelvic fungal pseudomycetoma. A single, 3 cm × 2.5 cm × 2 cm diameter, smooth soft tissue density mass (arrow head) located in the caudal abdominal and cranial pelvic cavities, causing ventral displacement and narrowing of the descending colon (white arrow), is present. No invasion into adjacent structures was seen. On post-contrast study (iohexol 350 mg/ml), no enhancement was seen
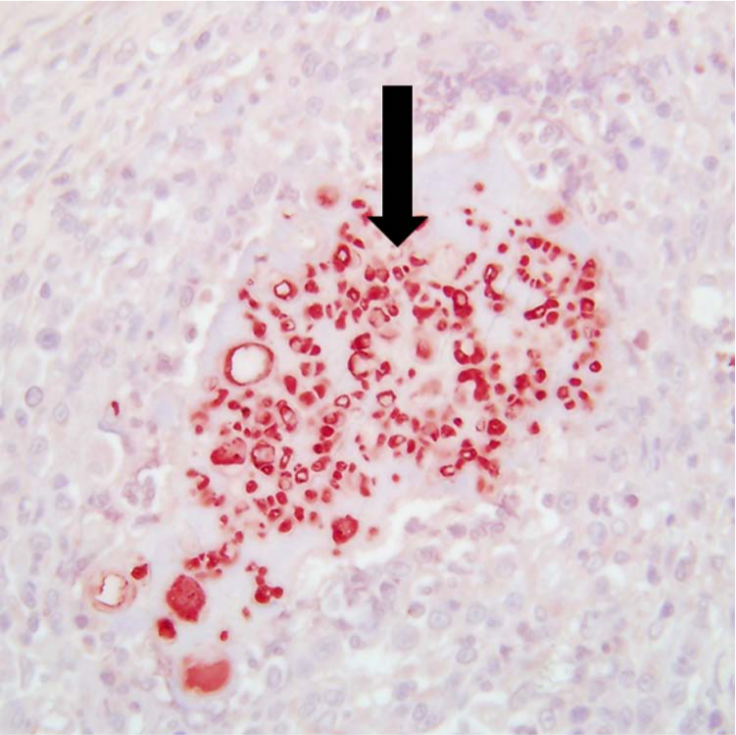
Immunohistochemistry of an excised pelvic mass in an adult Persian cat presented for constipation. Within the excised tissue, all fungal elements were stained strongly and uniformly only by using a dermatophyte-specific antibody as the primary (black arrow). The positive reactivity resulted in a specific and uniform red colouration of the fungal elements, consistent with a pseudomycetoma
Three days after surgery the cat became anorectic, dysuric and developed a mild azotaemia (creatinine 2.8 mg/dl). Physical and neurological examinations were unremarkable. Repeat urinalysis showed no abnormalities, and a urine culture was negative. Initially, postoperative pain, neuropraxia or urethral edema was suspected. Treatment was symptomatic and consisted of intravenous fluids, pain control, frequent bladder expressions, phenoxybenzamine [Dibenyline (Dallas Pharmaceuticals) 2 mg, PO, q12h] and diazepam [Assival (Teva Pharmaceuticals) 0.5 mg/kg, IV, pro re nata]. Three days later the anorexia, azotaemia and hypercalcaemia resolved, but stranguria persisted and the bladder became difficult to express. An indwelling urinary catheter was placed and maintained for 3 days in order to decompress the bladder; however, the problem persisted when the catheter was removed. A positive contrast, retrograde urethrogram was performed, and narrowing of the distal urethra was seen. A urethral stricture was suspected and a percutaneous tube cystostomy was placed, via celiotomy, to divert the urine. A repeat rectal examination was performed under anaesthesia and the area of the previously excised mass was inspected during surgery and touch smears were made from the area. No evidence of recurrence was seen and fungal hyphae could not be demonstrated on the smears. Ionised calcium 8 days after surgery was normal (1.28 mmol/l).
The cat was discharged 12 days after the initial surgery with the tube cystostomy still in place. Urine culture and susceptibility while the cystostomy tube was in place grew resistant strains of Escherichia coli and Pseudomonas species, and the cat was treated with ticracillin [Timentin (GlaxoSmithKline) 15 mg/kg, IV, diluted, SC q8h] for 4 weeks. Over the next 2 weeks the cat improved significantly, gained weight and began urinating independently. The tube cystostomy was removed 26 days after insertion. Repeat urine culture was negative. The cat went on to receive itraconazole for 6 months and is still doing well 1 year after discontinuation of the drug.
Mycetomas are pyogranulomatous nodules that contain tissue grains or nodules, and can be fungal (eumycetoma) or bacterial (actinomycetoma) in origin. 5 Clinically, the three distinguishing features of mycetoma are formation of nodular inflammatory lesions with secondary fibrosis, formation of fistulae, and the presence of bacterial or fungal grains in the affected tissue and exudates. 6 The dermatophytes within these lesions may aggregate into clusters that resemble the tissue grains of eumycetoma. These clusters of dermatophytes are not considered true grains because individual fungal elements may often be found in the tissue as well. Therefore, some prefer the term pseudomycetoma to distinguish the dermatophytic lesions from those of other fungal mycetoma. 5
The initial lesion is typically a painless scratch or small papule. Because little discomfort is associated with early lesions, mycetomas are usually insidious, and human patients generally present late in the course of the disease. As the disease progresses, affected tissue is replaced by a tumourous-like mass of chronic inflammation and fibrosis that may clinically resemble neoplasia. 7 In humans, trauma has been reported as a cause for slow penetration of fungal infections into the abdominal cavity, with lesions developing over months-to-years. 8 In this report, there was evidence of trauma to the pelvic region when the cat was adopted, at least 5 years prior to presentation, and we suspect that this was the site of fungal penetration.
Dermatophyte penetration into body cavities is extremely rare and, to date, only three cases of intra-abdominal pseudomycetoma in cats have been reported in the veterinary literature.7,9,10 In the first case the cat died 3 weeks after a therapeutic trial with itraconazole; however, the cause of death was unknown, as post-mortem examination was not allowed. The other cats were euthanased owing to financial constraints or poor prognosis. Although it is unknown if Persian cats are predisposed to this fungal infection, it is interesting that three of the four reported cats thus far are Persian. In addition, cutaneous fungal pseudomycetoma is reported almost solely in Persian cats.11–15 This case report is the first to document successful treatment of an intra-abdominal pseudomycetoma with a combination of surgical excision, supportive care and prolonged antifungal therapy.
Hypercalcaemia secondary to pyogranulomatous diseases caused by fungal16,17 or bacterial 18 organisms is rarely reported in cats, and persistent hypercalcaemia due to pseudomycetoma has not been previously reported. The suggested mechanism for hypercalcaemia in fungal infections is activation of monocytes and macrophages by interferon-γ or Toll-like receptor agonists, causing expression of 25-hydroxyvitamin D3 1α-hydroxylase, leading to hypervitaminosis D. 19 Another possible mechanism is expression of parathyroid hormone-related protein by cells within the granulomas. 19
In this case, histopathology provided a tentative diagnosis, and fresh tissue was not available for fungal culture as infectious causes were considered less likely. When only fixed tissue is available or when cultivation attempts have been unsuccessful, in situ identification is the only feasible diagnostic option for obtaining a definitive diagnosis.2,3 Immunohistochemistry, however, provides identification to the level of the genus; identification to the species level in most cases is not possible.
The cause of the stranguria in this cat remains unclear. The main differential diagnoses include transient neuroprxia, stress-related urethral spasm and urethral stricture. Although the mass was anatomically located near the origin of the pudendal and pelvic nerves, the cat maintained a normal anal reflex and did not exhibit faecal incontinence; however, its bladder was difficult to express, rendering lower motor neuron nerve injury less likely. A stricture was suspected based on the contrast study. However, the cat regained full ability to urinate 4 weeks after discharge; therefore, urethral oedema and spasm secondary to inflammation, along with stress and pain, were most likely the causes of the stranguria.
We suspect that pseudomycetomas that are not excised, or at least radically debulked, will respond poorly to supportive care and antifungal therapy as fungal granulomas are poorly vascularised, limiting drug penetration into the target site. Therefore, treatment should most likely consist of a combination of radical surgical debulking or, if possible, complete excision and prolonged antifungal therapy. It is unknown how long treatment with antifungal therapy should persist, but, based on the slow response in humans, several months of treatment seem reasonable.
Conclusions
Intra-abdominal fungal pseudomycetoma should be considered a differential diagnosis in any cat, especially Persian cats, presenting with an abdominal mass and hypercalcaemia. Aggressive debulking, where complete excision is impossible, in combination with antifungal systemic medications, resulted in a good quality of life and remission for at least 1 year in this case.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.