
Abstract
Practical relevance:
Hypersensitivity dermatitis (HD) is often suspected in cats and is mostly caused by insect bites, food or environmental allergens. Cats with non-flea induced HD are reported to present frequently with one or more of the following cutaneous reaction patterns: miliary dermatitis, eosinophilic dermatitis, self-induced symmetrical alopecia or head and neck excoriations/pruritus.
Clinical challenges:
None of the above patterns are, however, pathognomonic for non-flea induced HD and the diagnosis of this condition is based on exclusion of diseases presenting similarly and an adequate response to treatment. Therapeutic approaches to affected cats include use of immunomodulatory drugs (ciclosporin, glucocorticoids, antihistamines), hypoallergenic diets and allergen-specific immunotherapy.
Evidence base:
This review provides an update on the clinical signs, diagnosis and treatment of feline non-flea induced HD. It draws on the findings of a recent large-scale study that described the clinical signs of numerous cats with non-flea HD and has proposed criteria to facilitate the diagnosis of the condition.
Broad scope of hypersensitivity dermatitis
Hypersensitivity dermatitis (HD) is often suspected in companion animals and includes flea (and other insect) bite hypersensitivity dermatitis, cutaneous adverse food reactions, urticaria, angioedema and atopic dermatitis. 1 In feline medicine, the term ‘atopic dermatitis’ is considered inappropriate because the importance of IgE in the pathogenesis of the condition has not been conclusively demonstrated.2,3 Therefore, for the purpose of this discussion, and more generally, the more generic term of ‘non-flea HD’ (ie, non-flea bite associated HD) is used in place of feline atopic dermatitis.
The diagnosis of feline non-flea HD is usually based on exclusion of other pruritic conditions such as ectoparasitic disease and bacterial infections.4 –7 Additionally, and depending on the clinical pattern, other conditions may need to be ruled out (eg, psychogenic alopecia for symmetrical self-induced alopecia, viral diseases for head and neck excoriations, mast cell hyperplasia or tumours for eosinophilic dermatitis). As non-flea HD may be caused by various allergens, cats should undergo an elimination dietary trial and allergy tests may be beneficial in some cases, especially when allergen-specific immunotherapy is planned.
It is usually accepted that cats with non-flea HD will exhibit pruritus and at least one of the following patterns: head and neck excoriations/pruritus, self-induced symmetrical alopecia, eosinophilic diseases (eosinophilic plaques or granulomas, indolent ulcers) or miliary dermatitis.4 –7 None of these signs or patterns are considered pathognomonic for non-flea HD in cats. For this reason, criteria have been developed to facilitate the diagnosis in the context of a thorough work-up, 5 and these are a key focus of this article.
Treatments for non-flea HD include diets, antigen-specific immunotherapy, glucocorticoids, antihistamines and ciclosporin.6,8
Clinical features of feline non-flea HD
Epidemiology
Feline non-flea HD (including food hypersensitivity with cutaneous manifestations) is recognised as a frequent condition even though the incidence and prevalence have never been studied. A familial predisposition has been observed by some authors and a breed predisposition (Abyssinian) has been suggested.6,7,9 These data collectively suggest a hereditary background associated with HD, but specific genetic studies have not been carried out in allergic cats. A gender predisposition has not been demonstrated, though females represented 59% of a panel of 161 cats with non-flea HD. 7 The majority of cats with HD seem to exhibit the first clinical signs before 3 years of age, although some studies suggest a wider range of age at onset of disease.2,6,10 In one recently published study, the mean age at onset was 3.4 years, with cats demonstrating food HD being slightly older (mean 4 years old) than those with non-flea, non-food HD. 7 In the same study, seasonality was a feature of the disease in fewer than 10% of cats.


Miliary dermatitis

Head excoriations

Neck excoriations

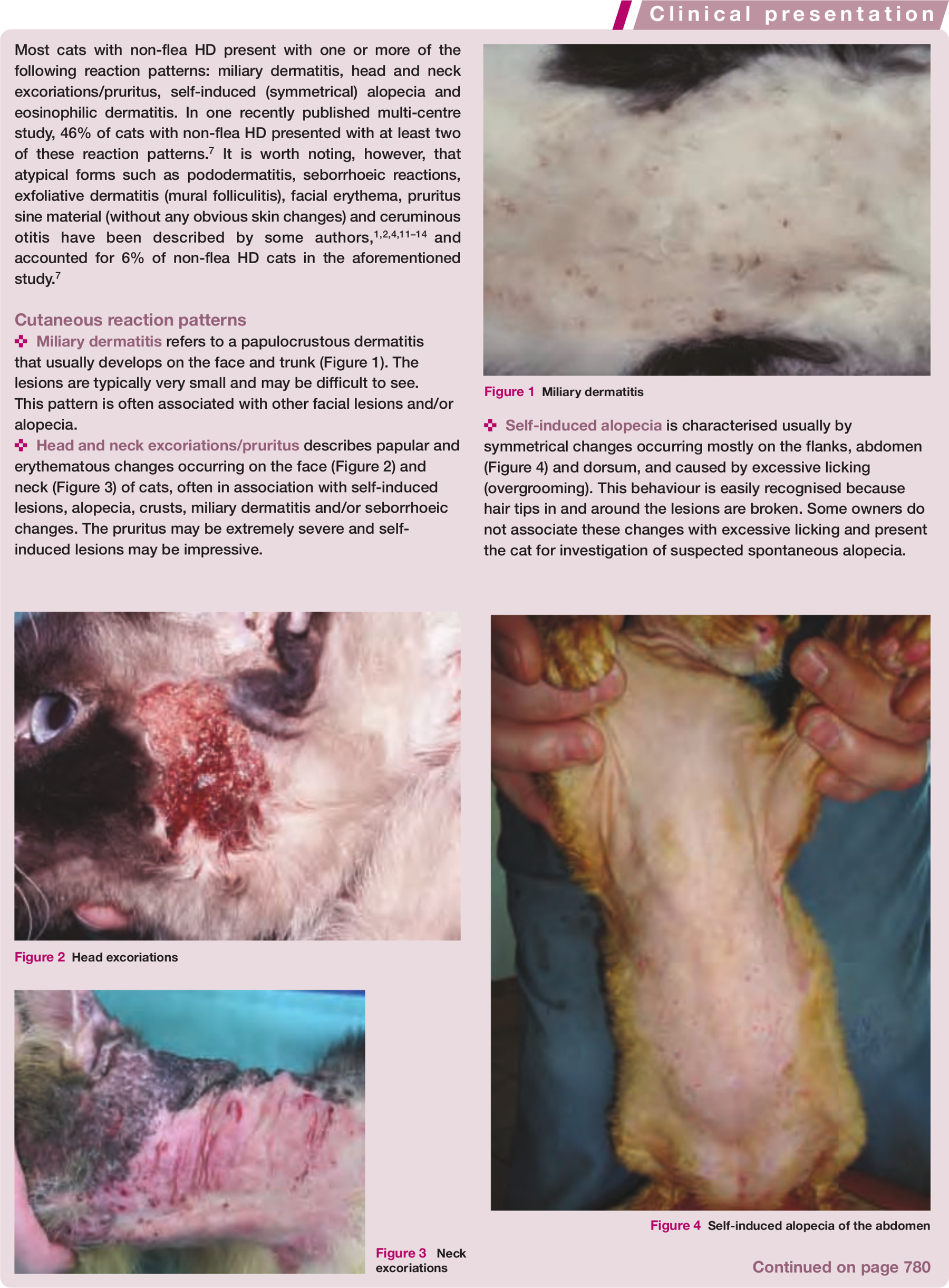
Self-induced alopecia of the abdomen

Ulcerative lesion of the upper lips

Eosinophilic plaques on the abdomen

Linear eosinophilic granulomas on the caudal thigh

Interdigital eosinophilic granulomas

Eosinophilic granulomas on the chin (‘fat chin’)
Clinical presentation
The typical cutaneous reaction patterns and other signs that may be associated with feline non-flea HD are summarised in the boxes on pages 779 and 780.

Differential diagnoses
Given that none of the clinical signs or reaction patterns described for non-flea HD (see pages 779 and 780) are pathognomonic, ruling out of resembling diseases is a compulsory step in the case work-up. Ectoparasites such as fleas, lice, Otodectes, Notoedres, Demodex and Neotrombicula species, as well as bacterial and fungal diseases, will need to be ruled out in virtually all cats.2,6,7,10,15,17 Additionally, and depending on the clinical presentation, some other differential diagnoses should be considered and confirmatory tests carried out (Table 1).
Hypersensitivity dermatitis: differential diagnoses and confirmatory tests

Diagnostic work-up
In ruling out diseases that may look clinically like non-flea HD, ectoparasites (ie, fleas, Otodectes, Notoedres, Demodex, Trombicula, etc) and dermatophytosis should be a particular focus of attention. Consequently, flea combing, scrapings, fungal cultures and cytological examination (if the skin is inflamed) should be regarded as the absolute minimum work-up in patients with a suspicion of non-flea HD. Note that Wood’s lamp examination, trichoscopy and culture on dermatophyte test medium can be associated with false-negative results.
Malassezia dermatitis and superficial pyoderma can complicate feline HD in some instances and should be treated appropriately. Exclusion of fleas and other parasites often requires treatment of the affected cat, other animals living in the household and the house, even if parasites are not found on the animal. Special attention should also be paid to Demodex gatoi infestations if this mite is present in the area in which the cat lives, or if the cat has a history of travel.
If the presentation pattern suggests the possibility of other conditions, such as viral or neoplastic diseases, then skin biopsies and polymerase chain reaction (PCR) may additionally be indicated to rule out these disorders. However, the histology associated with non-flea HD is not substantially different from any other pruritic skin disorder and not generally very helpful in determining the aetiology of the pruritus.
Rarely, symmetrical alopecia can be associated with psychogenic causes and a specific work-up should be carried out, especially in patients with self-induced alopecia. 18
Diagnostic criteria
The Dermatology Department at the University of Zurich has recently developed criteria for the diagnosis of non-flea HD (see box below). 5 It is extremely important that these criteria are not considered a replacement for a proper work-up but, rather, tools to evaluate the probability of non-flea HD before this work-up or to confirm a suspicion thereafter. The importance of this work-up is best illustrated by comparing the specificity and sensitivity of the criteria before (sensitivity: 75%, specificity: 76% when five out of the eight criteria are met) and after (sensitivity: 90%, specificity: 83% when six of the 10 criteria are met) ruling out fleas. The fact that the sensitivity and specificity are markedly higher when fleas are ruled out supports flea control as the first mandatory step in the work-up of pruritic cats.
Elimination diet
As food induced HD and non-flea, non-food HD are virtually indistinguishable, even after conducting a proper clinical examination and using the criteria discussed above, it is mandatory to carry out a elimination dietary trial in all cats with non-flea HD.
An elimination diet consists of feeding a cat for 6–8 weeks with a source of protein and a carbohydrate source that have never previously been provided. Hydrolysed foods, in which the proteins have been broken down into small pieces, making them less allergenic, have not been proven superior to date.19,20 In addition, some reports of allergy reactions to preservative suggest that a home-cooked diet may be the best option, though studies have not been carried out in cats. 21 As none of the possible diets can be regarded as 100% anallergenic, if a food allergy is strongly suspected, a further dietary trial with another protein source should be considered in patients not responding to an elimination diet. 4 It is worth noting that owners of cats with outdoor access should be instructed to keep their pet indoors during the whole trial.

Some cases of late improvement have been seen as long as 12 weeks after the start of a trial. Consequently, extending the duration of the trial should be considered in a patient with a high index of suspicion that fails to respond within 8 weeks.
Last, but not least, any improvement during the trial should be confirmed by a challenge with the original diet; in the case of food induced HD, recurrence of the clinical signs is usually seen within 7–10 days.
Allergy tests
Allergy testing is not appropriate for establishing or confirming a diagnosis of non-flea HD because of the high number of false-positive and false-negative results associated with these tests. Allergy testing should, however, be carried out when antigen immunotherapy is planned. In the experience of most dermatologists, allergens implicated in intradermal and serological tests are mainly from dust mites, which does not rule out any role of pollen allergens.2,6 Interpretation of these tests in cats is often regarded as more difficult than in other animals, and intravenous injection of fluorescein with subsequent interpretation with Wood’s lamp has been advocated. 22

Footnotes
Key Points
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The author does not have any potential conflicts of interest to declare.