
Abstract
This report describes a case of bile peritonitis and bilothorax associated with diaphragmatic laceration secondary to gunshot wounds in a cat. Surgical treatment comprising cholecystectomy, placement of a chest tube for thoracic lavage and tube feeding led to an uneventful recovery. Bilothorax and bile peritonitis are a rare presentation in cats. There are only four cases reported in the literature and combined bilothorax and bile peritonitis secondary to gunshot lesion has not been documented before. This report describes positioning of the chest tube for pleural lavage through the diaphragmatic defect created by a pellet’s trajectory. The tube was then allowed to exit the laparotomy incision instead of exiting the thoracic wall.
Case Report
A 3-year-old, male neutered, domestic shorthair cat was presented as an emergency to the Centre for Small Animal Studies of the Animal Health Trust for sudden deterioration of his demeanour secondary to multiple gunshot wounds. The cat was shot 5 days earlier and was assessed by the referring veterinarian for anorexia and multiple skin wounds. Upon presentation to the Animal Health Trust the cat was pyrexic (temperature = 39.9°C) and depressed. Physical examination revealed 10% dehydration, dyspnoea, mild jaundice and pale mucosal membranes. Pulse was weak, heart rate was 140 beats/min and respiratory rate was 60/min.
Haematology showed anaemia (packed cell volume 21%) and biochemistry was consistent with hypoalbuminaemia (20.9 g/l; reference interval (RI) 28–40 g/l), hyperbilirubinaemia (total bilirubin 58 μmol/l; RI 0–15 μmol/l) and alanine transaminase 1284 μ/l (RI 5–70 μ/l).
Intravenous fluid therapy with Hartmann’s solution (Aquapharm; Animal Care) at 6 ml/kg/h and intravenous cefuroxime 20 mg/kg/q8h (Zinacef; Glaxo Smithkline) was initiated.
Dorsoventral and lateral radiographs of skull, thorax and abdomen showed numerous pellets scattered throughout the body, with reduction in abdominal serosal detail and moderate pleural effusion. Thoracic radiographs also revealed the presence of a focal soft tissue opacity extending from the diaphragm into the thorax (Figure 1). Abdominal and thoracic ultrasonography confirmed pleural and peritoneal effusion, multiple hepatic pellet tracts were detected and the gall bladder had a sunken appearance with concave walls.

Lateral radiograph of thorax and abdomen showing numerous pellets scattered throughout the body with reduction of abdominal serosal detail, pleural effusion and focal soft tissue opacity extending from the diaphragm into the thorax
Peritoneal and pleural effusion centesis yielded bright green and yellow fluid, respectively. Total bilirubin was 477 μmol/l (RI 0–15 μmol/l) in both effusions. Cytological evaluation showed degenerated neutrophils without intracellular bacteria (Figure 2) and bacteriology culture did not yield growth. The elevated bilirubun in the effusions compared with serum was consistent with bile peritonitis and bilothorax.
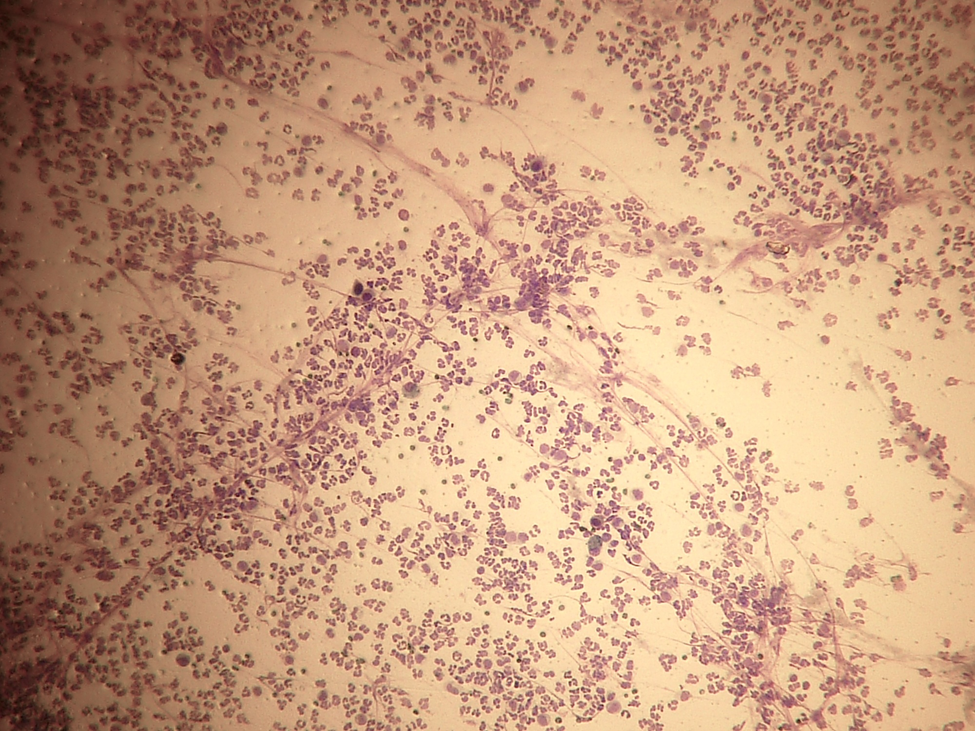
Cytological image of the peritoneal biliary effusion: degenerated neutrophils without intracellular bacteria
The day after admission, the cat was anaesthetised and prepared for midline exploratory coeliotomy. During exploration a 2 mm × 2 mm defect in the dorsal left diaphragm was found and debrided (Figure 3). A 1 mm × 2 mm defect in the cystic duct, 2–3 mm distal from its junction with the common bile duct was detected. Retrograde flushing with 0.9% saline solution from the body of the gall bladder highlighted biliary leakage (Figure 4). Exploration also confirmed the presence of multiple hepatic pellet tracts (Figure 5). A cholecystectomy was performed. The pleural effusion was aspirated via the diaphragmatic defect, and lavage of the thoracic and peritoneal cavity with pre-warmed 0.9% saline was performed. A silicone chest tube (14 Fr × 38 cm Mila International) was positioned in the thoracic cavity through the diaphragmatic defect, which was then closed with simple interrupted sutures of 3-0 polydioxanone (PDS; Ethicon) (Figure 6). The tube was allowed to exit the laparotomy incision for pneumothorax evacuation in the immediate postoperative period and for pleural lavage. Closure of the coeliotomy incision was routine. Pleural lavages with 10 ml/kg pre-warmed Hartmann’s solution and aspiration were performed every 3–4 h for the first 24 h and than every 8 h via the thoracostomy tube. Repeat thoracic radiographs confirmed pleural effusion resolution on the fourth day and the chest drain was removed.

A 2 mm × 2 mm defect in the dorsal left diaphragm with bile pigmentation on the lesion borders

A 1 mm × 2 mm perforation of the cystic duct, 2–3 mm distal from its junction with the common bile duct. Retrograde flushing from the gall bladder body highlighted bile leakage from the defect

Parenchymal hepatic pellet tract

Placement of the thoracostomy tube through the diaphragmatic defect
To support the patient’s nutritional needs, a silicone oesophagostomy tube (14 Fr × 60 cm; Surgivet, Smiths Medical) was placed. The cat was tube-fed 214 ml Enteral Care KC Feline (Veterinary Formula, PetAg) (0.83 kcal/ml) daily, divided in five meals for 8 days, after which the tube was removed. The cat recovered uneventfully and was discharged.
Discussion
Bile peritonitis and bilothorax is exceedingly rare in cats. To my knowledge, only four cases have been described previously. Three cats developed bile peritonitis secondary to trauma. Two sustained injury from gunshots and one was hit by a car. One had perforation of the gall bladder; the second and the third suffered avulsion of the common bile duct from the duodenum. 1 A cat with bilothorax secondary to placement of a thoracostomy tube for treatment of a pyothorax was also reported. 2
In this case a pellet trajectory perforated the diaphragm and the cystic duct, creating a direct communication between the peritoneal and the pleural cavity. The communication between the two cavities permitted the passage of the leaked bile from the abdomen into the thorax. The cat was presented with bile peritonitis and bile pleuritis.
Diagnosis of biliary effusion was based on the concentration of effusion bilirubin compared to serum bilirubin. If the ratio is greater than 1, then a diagnosis of bile peritonitis/pleuritis can be made. 1
In dogs, stab or bite injuries, and penetrating wounds from gunshots can lead to tears in the extrahepatic biliary tract; however, this type of injury is usually associated with blunt trauma, such as motor vehicle accidents.1,3 When leakage occurs as a result of blunt trauma, the location of the tear is usually within the common bile duct or hepatic duct. 3 Iatrogenic injury sustained during abdominal surgery, associated with gall bladder expression, cholecystectomy, cholecystotomy, choledochotomy or incision of the hepatic ducts, may also result in biliary leakage and peritonitis. Rarely, leakage from the gall bladder has been reported.3–5
In blunt traumas, rapid cranial movement of the liver away from the well-fixed duodenum produces a traction force that can result in tearing or avulsion lesions. 6 The most common site of common bile duct rupture is just distal to the entrance of the last hepatic duct. 7 Knowledge of the distribution of these lesions is important so that close examination of these areas is performed during exploration surgery.
Penetrating injury is a less common cause of extrahepatic biliary tract trauma. With gunshot wounds to the abdomen and thorax, tissue within the trajectory of the projectile undergoes crush injury. Kinetic energy transferred to the body when the projectile hits its target leads to the formation of shock waves that radiate to more distant tissues. 8
Spillage of bile into the peritoneal and pleural cavity causes permeability changes, inflammation, haemolysis and tissue necrosis, which encourage bacterial growth. 7
The toxicity of bile acids depends not only on the amount of bile in the cavity, but also on the concentration of bile salts in the bile. 7 Bile peritonitis is more lethal in dogs than in humans because of the higher content of taurocholic acid in canine bile. 7 To my knowledge there are no equivalent studies in cats.
Bile acids are toxic to tissue and their hyperosmolarity leads to fluid shift from the vascular space into the cavities, resulting in dehydration and hypovolaemic shock. 2 This, together with a negative acute phase reaction, is thought to be the cause of the reduced serum albumin concentration on presentation in this case. 2 Bile is normally sterile; in penetrating injuries, however, bacterial infection can be introduced via direct inoculation or may be secondary to gastrointestinal tract penetration. 6 Animals with septic biliary effusion have a significantly higher mortality rate compared with those with sterile effusion. 1 In this case, anaerobic and aerobic culture of both pleural and peritoneal effusion yielded no bacterial growth, probably owing to the previously initiated treatment with antibacterials.
Bilothorax and bile peritonitis can occur in humans for a variety of reasons. Bilothorax is commonly associated with bilopleural fistulae, but can also occur with bile leakage into the abdomen in the face of an intact diaphragm. 2 The suspected mechanism of action in the latter scenario is that the bile acids and pigments are carried across the diaphragm in the lymphatics, and then cause damage to the lymphatic walls, subsequently leaking into the pleural space along with fluid. 2 Bilothorax in dogs, with an intact diaphragm, resolved with time. 2 Humans with sterile biliary effusion may have vague symptoms that last for an average of 30 days before surgical treatment and have a mortality rate of less than 10%. 7 In veterinary medicine, many studies have also identified a prolonged period (3–30 days) from rupture to presentation for bile peritonitis. The onset of clinical signs in animals with a ruptured biliary tract and the degree of peritonitis present depends on the volume of liquid bile, concentration of bile salts and bacteriobilia. 7
A study on the prediction of injury caused by penetrating wounds to the abdomen in humans showed that among the patients undergoing abdominal exploratory surgery, 89% were positive for intra-abdominal wounds. 9 Mandatory exploration of penetrating gunshot wounds is therefore recommended. 9 Similarly, animals with evidence of peritoneal penetration require an exploratory coeliotomy. 10 However, animals with thoracic injury can usually be managed with conservative treatment, or thoracocentesis and pleural lavage. 10 Generally, dogs and cats with abdominal gunshot wounds have a worse prognosis than with thoracic wounds. 10
Conclusions
My recommendations for managing cats presenting combined bile peritonitis and bilothorax are exploratory coeliotomy with prompt identification of an underlying cause, aerobic and anaerobic effusion culture, pleural and peritoneal lavage. A thoracostomy tube for pleural cavity lavage could be placed through the diaphragm during abdominal exploration and allowed to exit the laparotomy incision. It is generally recommended that drains are not placed through the primary incision because of proposed healing delay. 11 I have used this technique of thoracostomy tube placement for diaphragmatic hernias in cats for 12 years and have not encountered any complications. This technique reduces the morbidity of tube placement through the thoracic wall and the invasiveness of the procedure, sparing anaesthesia time. Moreover, nutritional support via enteral nutrition is of extreme importance in these debilitated and dehydrated patients, which present frequently with hypoalbuminaemia and anorexia.
Footnotes
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The author does not have any potential conflicts of interest to declare.