
Abstract
A 13-month-old female domestic shorthair cat presented with a 10-month history of polyuria and polydipsia that began after having been hit by a car. Neurological examination revealed visual deficits and an absent bilateral menace response. Hematological and serum biochemical analyses were within reference values, but hyposthenuria was identified. Failure to concentrate urine during the water deprivation test followed by an increase in urine specific gravity after administration of synthetic antidiuretic hormone (ADH) suggested a diagnosis of central diabetes insipidus. Subcutaneous or oral administration of synthetic ADH was effective in central diabetes insipidus treatment during the 19-month follow-up.
Case Report
Central diabetes insipidus (CDI) is a rare condition in cats 1 caused by loss or destruction of antidiuretic hormone (ADH)-secreting neurons in the supraoptic and paraventricular nuclei within the hypothalamus, 2 or by any impairment to hormone transport or release. 3 Most cases of CDI are idiopathic, but isolated reports of congenital,4,5 traumatic, 6 parasitic and neoplasitic etiology7,8 have also been described. Diagnosis of CDI is based on the results of hematology, serum biochemistries, urinalysis and hormone evaluation,5,9 but confirmed with a water deprivation test (WDT)–desmopressin 10 response test to confirm the diagnosis.3,9–12
This article reports a case of CDI following head trauma in a cat successfully treated with oral desmopressin.
A 13-month-old female domestic shorthair cat presented with a 10-month history of polyuria and polydipsia (PU/PD). Four weeks prior to onset of PD, the cat sustained head trauma after being hit by a car. At the time of trauma, the animal was semi-comatose, hypothermic, and exhibited epistaxis and left-sided otorrhagia. Owing to constant lateral recumbency, postural assessment, gait and postural reactions were not performed. Neurological examination revealed increased spinal reflexes in all limbs with crossed extensor reflexes in hind limbs. Cranial nerve examination revealed mild miosis and lack of a menace response oculi uterque (OU). Direct and consensual pupillary light reflexes (PLR) were normal. After the first 24 h, the animal exhibited complex partial seizures, characterized by licking and tonic-clonic movements of the right forelimb. During emergency care, 2 mg/kg dexamethasone (Dexavet; Bravet Laboratory) q24h and 4 mg/kg furosemide (Furosemida; Sanofi-Aventis Pharmaceuticals) q6h were administered for 3 and 5 days, respectively, to treat cerebral edema. Thoracic and abdominal radiographs were unremarkable. A week following the trauma, the cat presented signs of vestibular syndrome, characterized by walking in circles to the left side. Thirty days after trauma, the owner reported a significant increase in water consumption, which was not observed prior to the accident.
On re-check evaluation, 10 months later, the cat was alert, responsive and in good physical condition. Neurological examination revealed normal gait, posture and postural reactions, except for absent visual placing response. Moreover, the animal had abnormal interaction with a strange environment, reluctance to jump and to move, and could not discriminate obstacles, indicating severe visual impairment. 13 The cat could detect objects introduced into the lateral visual field of the left eye with absent bilateral menace response, intact palpebral reflex, and normal direct and consensual pupillary light reflexes OU.
Hematological, biochemical (alanine amino transferase, aspartate aminotransferase, alkaline phosphatase, urea and creatinine) and blood glucose evaluations were within normal ranges, and excluded kidney failure, liver failure and diabetes mellitus. Urinalysis showed decreased urine specific gravity (USG) [1.004, reference interval (RI) 1.025–1.0359]. Daily water intake measured by the owner for 3 days ranged between 162 ml/kg/day and 212.5 ml/kg/day (RI 20–90 ml/kg/day 9 ). Urine production was evaluated by taking the urine from the cat’s bare sandbox and ranged between 120.3 ml/kg/day and 134.7 ml/kg/day (RI 20–45 ml/kg/day 9 ). These results are consistent with previous findings in cats with CDI, 14 although nephrogenic diabetes insipidus (NDI) and psychogenic polydipsia (PP) were also differential diagnoses.
To rule out CDI, NDI and PP, a WDT combined with desmopressin administration was performed.15,16
After 6 h of fasting (the cat was allowed free access to water) the bladder was emptied manually and body weight was checked (3.2 kg). Prior to the test and every 30 mins, after water was withheld, USG, mental and hydration status, pulse rate, respiratory rate and body weight were assessed, and water was withheld. Before the test and 1 h after water deprivation, the urine was hyposthenuric (USG 1.006, RI 1.025–1.0359) (Figure 1).
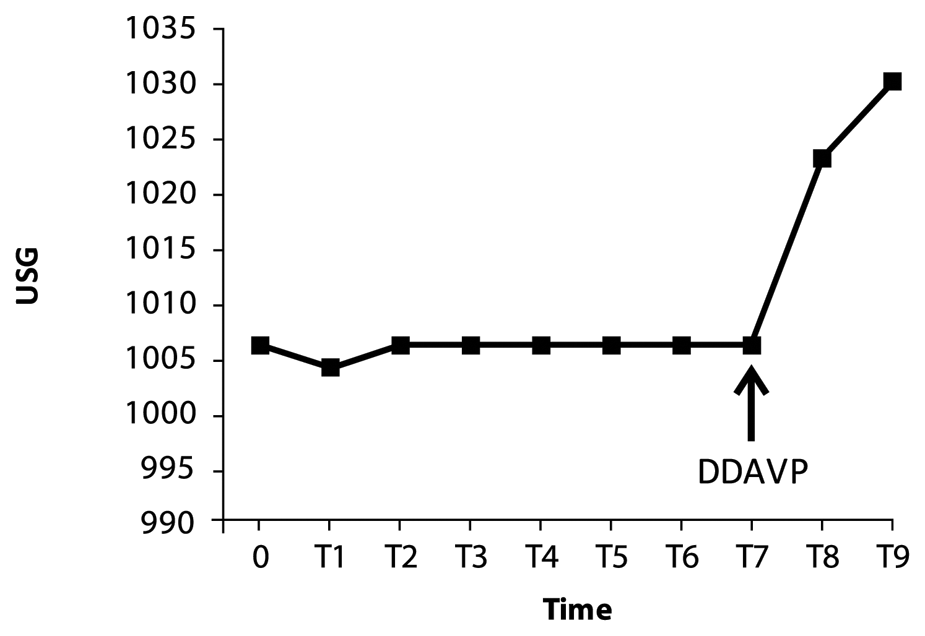
Urine specific gravity (USG) during water deprivation test (WDT) performed on a 13-month-old neutered female domestic shorthair cat suspected of central diabetes insipidus secondary to head trauma. WDT started at time zero (T0). Four hours later (T7), 2 μg/animal desmopressin acetate was administered subcutaneously. DDAVP = desmopressin acetate
Four hours later, a 5% reduction in body weight (3.04 kg), a 36% increase in heart rate, persistent hyposthenuria (1.006) and cat stress (characterized by irritability and growling) were determined at the time of administration of 2 μg/cat desmopressin acetate (DDAVP 4 µg/ml; Ferring Pharmaceuticals) subcutaneously.15,16 After administration of DDAVP, 2.5–3 ml/kg 9 water per hour was supplied for 5 h. Over the following 8 h, USG increased to 1.023 (RI 1.025–1.0359) (Figure 1), water intake (Figure 2A), and urine production (Figure 2B) reduced significantly as, has been reported previously in CDI. 12

Water intake (A) and urine production (B) 3 days before and 2 days after desmopressin acetate administration (DDAVP)
The cat was initially treated with 2 µg desmopressin subcutaneously, once a day for 7 days. An increase in USG (1.030) was observed at the end of this period. To facilitate drug administration, conjunctival sac drops were prescribed. Nasal solution desmopressin (DDAVP 0.1 mg/ml) at a dose of 5 µg/eye (one drop) was administered twice a day for 7 days and water intake was monitored. This protocol failed to attenuate PD even at higher doses (up to 15 µg/eye). Thus, oral desmopressin tablets (DDAVP 0.1 mg) were initiated at 12.5 µg q12h. Decreases in water consumption and urine production were observed thereafter. Dose adjustments were performed by increasing the dose to 50 μg q12h which eliminated the PU/PD on the majority of days during the 19-month follow-up.
In human medicine, causes of CDI include damage to the hypothalamic–neurohypophyseal region related to head trauma, surgery, primary or metastatic tumors, or idiopathic and genetic situations. 3 In veterinary medicine, CDI is a rare condition, 15 classified as primary (idiopathic or congenital) or secondary (head trauma or neoplasia), as in humans. 11 In this case report, head trauma preceded the appearance of PU/PD, suggesting that the etiology of the CDI was traumatic.
Diagnostic criteria for CDI vary and are based on plasma sodium concentration, the presence of PU, appropriate response to a water deprivation test/ADH response test, urine osmolality or USG,17,18 and lesion identification via magnetic resonance imaging (MRI). 19 Resolution of CDI has been reported in dogs and humans secondary to head trauma, and typically occurs within a few weeks. 20 In the present report, spontaneous recovery was not observed during the 19-month follow-up, so future resolution in this case is unlikely. 21
In this patient, persistent visual impairment, associated with intact PLR, suggested a partial lesion of the central visual pathway, from the lateral geniculate nucleus (LGN) to the visual cortex of the occipital lobes.22,23 As this area contains no neurons responsible for the PLR pathway, lesions there cannot interfere with the reflex. Most prosencephalic lesions that are involved with coma or semicoma, as seen in this case, will disrupt the central visual pathway, and will cause loss of the menace response with normal pupil size and light response. 24 In addition, experimental bilateral removal of the visual cortex in the occipital lobes can cause visual deficits with a persistent visual orienting response in the lateral visual field, as seen in this case, presumably via the rostral collicular projection in the midbrain.24,25 Moreover, focal seizures might occur from lesions in the occipital cortex presenting limb tonic-clonic movements, as in this cat in its right forelimb, indicating that the lesion is in the opposite cerebral hemisphere.24,26 Besides that, the cranial trauma may produce vestibular signs and the patient tends to circle towards the affected side.24,27 In the present case, left side otorrhagia and circling to the same side indicated cranial trauma.
Focal thalamic lesions in dogs and cats are uncommon and often difficult to localize based on neurological examination. Clinical features of thalamic lesions can include altered behavior and consciousness disturbances, hearing deficits, vestibular ataxia, and visual deficits if the rostral thalamic nucleus, the thalamic reticular system, medial geniculate nucleus and LGN, respectively, are damaged.23,24 In the present case, the cat was semi-comatose at presentation, with complex partial seizures (psychomotor seizures), vestibular ataxia and visual impairment. These abnormalities suggest injury to different regions of the thalamus. Owing to its proximity to the thalamus, the hypothalamus was also affected in this case. Hypothalamic lesions can lead to decreased ADH synthesis and water reabsorption associated with increased urinary excretion of free water.3,5 As discussed earlier in this report there is a multifocal problem in this case, probably involving occipital lobe, vestibular, thalamic and hypothalamic regions.
Based on the site of injury, endocrine disorders may develop and complicate the effects of traumatic brain injury (TBI) and its prognosis. Pituitary dysfunction secondary to TBI may be partial or complete, with clinical presentations ranging from mild to severe, depending on which pituitary hormones are affected.17,28,29 As changes in the neurohypophysis occur rarely and may lead to CDI, only 18 cases have been reported in cats.5,6,10,21,30
In this case, initial signs of PD, PU and nocturia, which began a month after the trauma, raised the possibilities of renal, liver disease, and diabetes mellitus, as well as diabetes insipidus. These were felt to be excluded based on the absence of alterations on hematology and serum biochemistry. Owing to financial constraints, the owners declined additional testing to definitively rule out other disorders that may result in severe PU/PD, such as underlying hyperthyroidism, hepatic insufficiency, hyperadrenocorticism and hypercalcemia. In an optimal situation, these parameters should have been evaluated, but, based on the history, response to water deprivation/ADH response testing and long-term follow-up, CDI secondary to trauma was the most likely diagnosis. 15
CDI, primary or secondary NDI, and PP still persisted as differentials.5,9,10,11,30,31 WDT and desmopressin, an analogue of ADH,9,30 administration were used to evaluate the ability of hypothalamus and neurohypophysis to produce and secrete ADH in response to dehydration and the ability of the kidney to respond to the hormone. 30 In this case, an increase in heart rate and reduction in body weight were used to determine the timing of desmopressin (2 μg SC/animal) administration.14–16 During the test, water was provided only for maintenance (2.5– 3 ml/kg/h) 9 owing to the risk of over-hydration and brain edema if offered ad libitum. It was observed that, even during WDT, the animal was unable to concentrate its urine, suggesting the absence of ADH or ADH receptors.15,16 PP was excluded because an expected increase in USG should be observed during WDT. 16 A gradual water restriction, for 3 days before this test, is necessary to diagnose PP. A chronic polyuria, even in high concentrations of ADH, leads to an impairing ability of renal tubules to concentrate urine, causing a misunderstood diagnosis. 9 NDI, an impaired responsiveness of the kidney to ADH, can be congenital or secondary to renal or metabolic disorders that alter the normal interaction between ADH and renal tubular receptors. 30 In NDI or CDI, USG remains low during water deprivation test, but very little, or no, rise in USG is observed after desmopressin administration in NDI.9,15 Therefore, CDI was suggested by a marked increase in USG from 1.006 to 1.023, which demonstrated normal renal tubular responsiveness to ADH,9–11,31 along with a dramatic drop in daily water consumption 8 h after hormone administration. The diagnosis of a lesion, traumatic or neoplastic, in the hypothalamic/neurohypophyseal region requires advanced brain imaging techniques. Owing to the unavailability of MRI, this procedure was not performed. The fact that the cat was young and remained neurologically normal over the 10-month period suggested that significant brain pathology was unlikely.
Desmopressin is the initial treatment of choice for CDI. It is available as an injection, intranasal spray and oral tablet. It can be difficult to establish the best therapeutic dose in order to control clinical signs and avoid an overdose, which can lead to hyponatremia, fluid overload, cerebral edema and seizures. 14 Moreover, attempts to control the fluid balance without desmopressin using fluids alone is too hazardous. 18
Starting doses of 1.5–4 µg of intranasal or conjunctival desmopressin twice a day and water availability ad libitum has been reported to result in good control of PD and PU in most animals. 11 However, the conjunctival desmopressin failed to control CDI in this case, even with increasing doses. The intranasal route is difficult to use in cats owing to the discomfort of drug administration because of nasal mucosa irritation. 32
Desmopressin may also be given subcutaneously (0.5–2 μg/cat) or orally (12.5 µg/cat) at night, adjusting the dose as necessary, 9 aiming to decrease water consumption to normal. 3 In this case, the effective oral dose was 50 μg q12h. Side effects include headache, fatigue, nausea and stomatitis, but have not been reported in the veterinary literature.
Other therapies for CDI include chlorpropamide, thiazide diuretics and, less commonly, carbamazepine and clofibrate, which act through different mechanisms.3,9,33 The chlorpropamide, an anti-diabetes drug, acts by sensitizing the renal tubules to the antidiuretic effect of ADH, being effective only in forms of partial CDI. Thiazide diuretics exert their effect by decreasing sodium and chloride absorption in the distal tubule, therefore allowing more sodium absorption and, consequently, the water absorption in the proximal tubule.9,33 The therapeutic effect of carbamazepine, an anti-convulsvant, is to reduce the sensitivity of the osmoregulatory system of ADH secretion and simultaneously raises the sensitivity of the collecting duct to the hydro-osmotic action of the hormone. Clofibrate, a lipid-lowering agent, stimulates residual ADH production in patients with partial CDI. 3
Prognosis depends on the underlying cause of the CDI. Idiopathic cases and those secondary to head trauma may have favorable long-term results with appropriate medication, free access to water and periodic monitoring.31,34
Conclusions
Although a complete work-up was not possible owing to financial constraints, in this case report diagnosis of CDI was confirmed through WDT and response to desmopressin administration. Successful treatment was achieved through subcutaneous and oral administration of desmopressin twice a day, allowing the cat to remain asymptomatic during the 19 months of follow-up.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.