
Abstract
An 11-year-old cat was referred following vehicular trauma for evaluation and treatment of right thoracic limb lameness which was non-responsive to conservative management. Gait assessment revealed a severe weight-bearing right thoracic limb lameness, soft tissue swelling over the dorsal border of the scapula, crepitus upon direct palpation over the scapula and lateralisation of the scapula upon adduction of the distal limb allowing a diagnosis of scapular avulsion to be made. Computed tomography (CT) demonstrated a comminuted fracture of the right scapula and a tear of the serratus ventralis muscle. The scapular fractures involved the caudal scapular angle and therefore a circumcostal suture was not placed. Stabilisation was achieved through reattachment of the scapula to the serratus ventralis muscle with sutures placed through small holes in the dorsal and cranial borders of the scapula. Follow-up revealed resolution of lameness at 14 weeks postoperatively but non-union of the scapular fractures as evidenced by repeat CT. This case report details the medium-term outcome following this very unusual injury and contributes to the sparse literature regarding the progression of conservatively managed scapular fractures. It demonstrates that full return to function can occur following this injury even when radiographic union of the fracture is not achieved. To our knowledge this is the first report of this specific combination of injuries detailed with medium-term and advanced imaging follow-up.
Case Report
Scapular avulsion is uncommon. 1 The thoracic limb has no articulation with the skeleton and supports the trunk by deep and superficial muscles.2,3 The deep group holds the body up towards the scapula when the cat is standing and is composed of the serratus ventralis, trapezius and rhomboideus muscles. Rupture of this group causes the scapula to shift dorsally and prevents the cat maintaining normal posture. 2 The injury is caused by trauma.1,4 The characteristic dorsal displacement of the scapula is easily observed and palpable, 2 and the proximal part of the scapula displaces laterally if the distal limb is adducted. 5 While closed reduction and a Velpeau sling may facilitate a reasonable functional outcome, surgical repair is normally necessary for a full functional and cosmetic result. 5 Different stabilisation methods have been described, including circumcostal placement of a wire suture from the caudal margin of the scapula 5 and reattachment of the bone to the serratus ventralis muscle with sutures secured through holes in the scapula. 2 Healing is purportedly rapid with good function returning, 1 but follow-up of these cases in the literature is lacking.
Fractures of the scapula account for 0.5–2.4% of all fractures observed in small animals6–8 and are normally the result of vehicular trauma. 7 Scapular fractures can either be managed surgically or conservatively depending upon the type of fracture, with surgical management being reserved for cases with loss of congruity of the articular surface or a change in the angulation of shoulder joint articulation, as is seen with many fractures of the scapular neck. 4
This case report details the presentation, case management and follow-up for a case of scapular avulsion and concomitant comminuted fracture of the scapula.
An 11-year-old male neutered domestic shorthair cat was referred for evaluation of right thoracic limb lameness following vehicular trauma sustained 1 week earlier. No response had been noted to cage rest and medication with meloxicam (Metacam; Boehringer Ingelheim: 0.05mg/kg PO q24h). Radiographs suggestive of fracture of the caudo-dorsal border of the scapula prompted referral (Figure 1a and b).
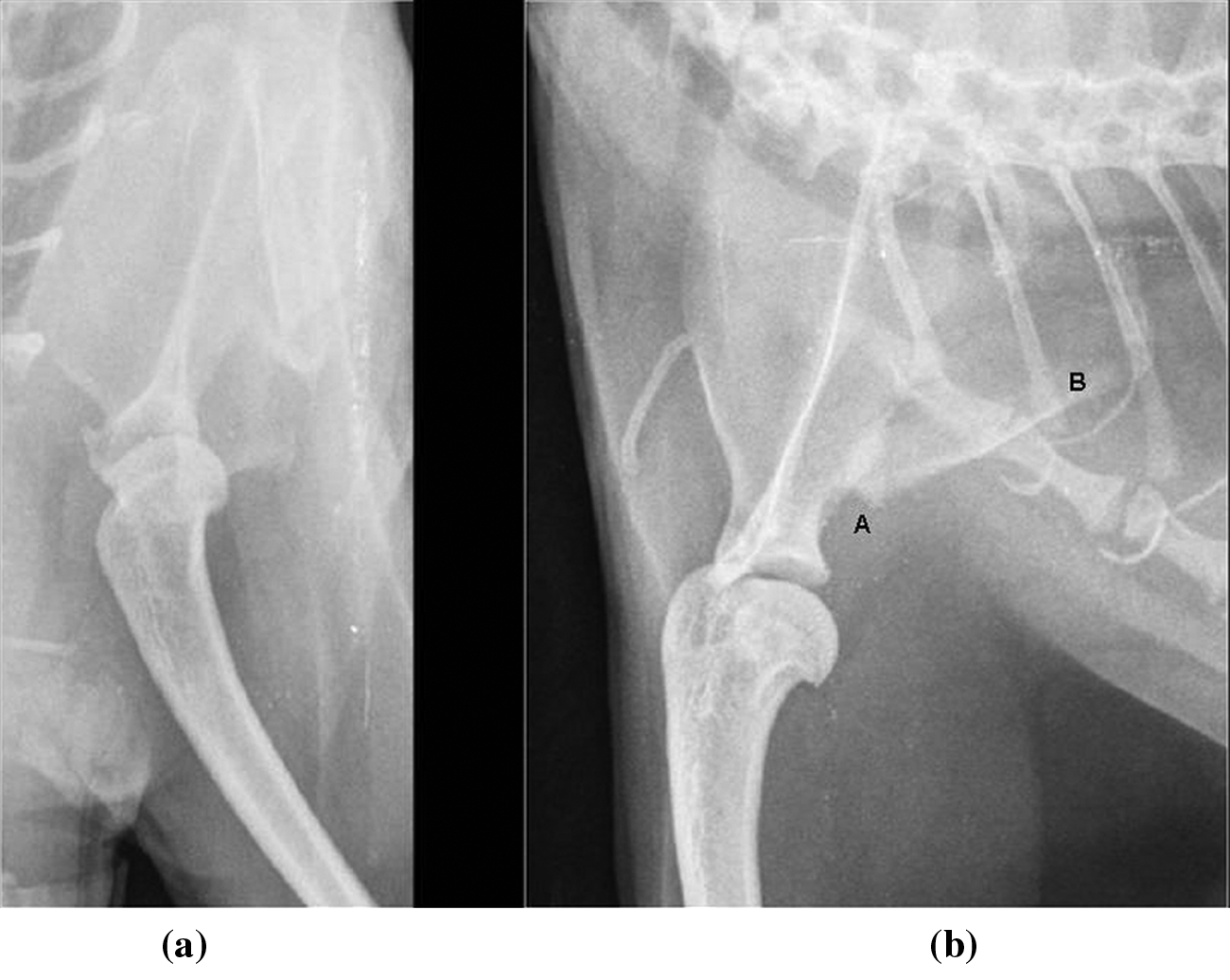
Caudo-cranial and medio-lateral views of the right shoulder taken one week following original trauma. Note the discontinuity of the caudal border of the scapula (a) with additional fragment adjacent (b)
Upon presentation, the cat was quiet but alert and responsive. The body condition score was 7.5/9 and weight was 7.18 kg. Examination revealed a severe weight-bearing right thoracic limb lameness and a 2.5 cm × 2 cm soft tissue swelling over the dorsal border of the scapula. Crepitus was palpable when pressure was applied directly over the scapula. Upon adduction of the distal limb the scapula was felt to lateralise abnormally and it could be displaced dorsally by simulating weight bearing.
Pre-anaesthetic sedation was achieved using acepromazine (ACP; Novartis Animal Health: 0.01 mg/kg, IV) and methadone (Physeptone; Glaxosmithkline: 0.2 mg/kg, IV). Anaesthesia was induced with alfaxalone (Alfaxan; Vetoquinol: 2–3 mg/kg, IV, titrated to effect) and maintained using isoflurane (Isoba; MSD Animal Health: 1.5%) in 100% oxygen. Fluid therapy with compound sodium lactate (5 ml/kg/h, IV) was administered throughout.
Computed tomographic (CT) scan of the right thoracic limb revealed a comminuted fracture of the scapula; the main fracture line started at the level of the scapular neck. It extended proximally through the infraspinous fossa before changing orientation cranially to include the dorsal border. Moderate ventral, medial and cranial displacement of the caudoventral segment was evident. A small sliver was also separated from the dorsal border (Figure 2a–c). The serratus ventralis muscle was identified in cross section and appeared discontinuous with bunching of the muscle and moderate soft tissue swelling. A round soft tissue-attenuating structure was present dorsal to the scapula within the subcutis with an attenuation of 74 Hounsfield units, consistent with haemorrhage (Figure 2d). Right scapular avulsion with a serratus ventralis tear, subcutaneous haematoma and scapular fracture were diagnosed.
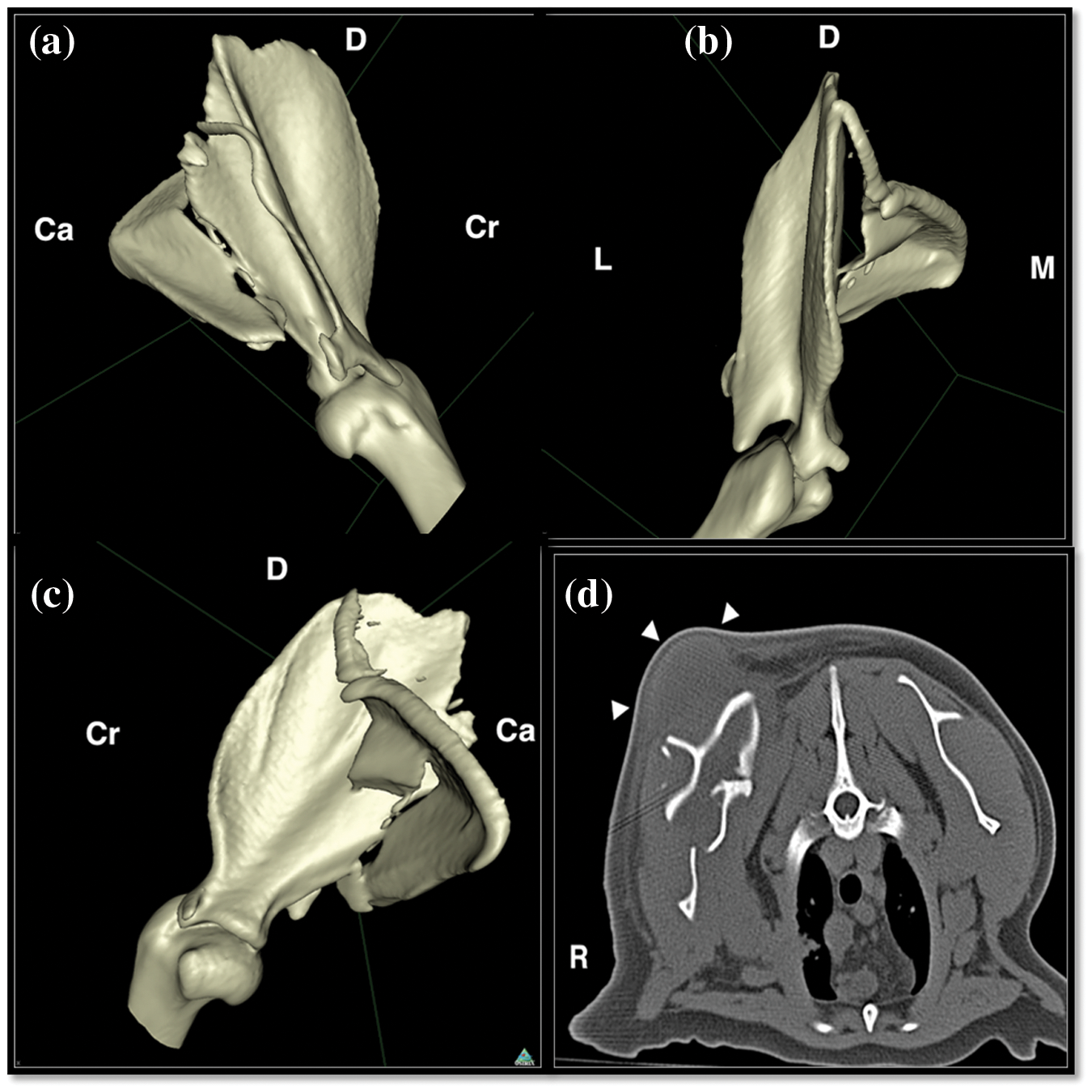
Lateral, medial and dorsal 3D reconstructions and a single transverse image demonstrating the configuration of the comminuted right scapular fracture and the presumed haematoma (arrowheads). Cr = cranial, Ca = caudal, L = lateral, M = medial, R = right
Under anaesthesia the shoulder laxity was more pronounced (Figure 3). Local anaesthesia was achieved using a paravertebral block with bupivacaine hydrochloride (Marcain; Astrazenaca) at 0.5% (1.3 mg/kg) and the rate of fluid administration was increased to 10 ml/kg/h intravenously (IV). The scapula was approached through a T-shaped incision. A defect in the musculature overlying the dorsal scapula of 2 cm in diameter was evident. The dorsal portion of the scapula protruded through this defect. The dorsal margin of the serratus ventralis had become detached from the facies serrata and the small avulsed segment from the dorsal border of the scapula was palpable within this musculature. The fracture caudal to the scapular spine was palpated and observed to be moderately displaced but stable. The caudal scapular angle was involved in the fracture such that a circumcostal suture was unlikely to ameliorate the instability due to the scapular avulsion. Owing to the palpable stability of the fracture site, surgical repair of the fracture was not felt to be justified as, while alignment may have been improved, an extensive approach would have been required, which may have exacerbated instability, and achieving adequate implant purchase would have been challenging. Surgical repair of the fracture was not felt to be necessary. The supraspinatus and infraspinatus muscles were elevated slightly to reveal the cranial angle and remaining dorsal border of the scapula. Three 1.5-mm holes were drilled through the cranial angle and dorsal border approximately 7 mm apart. Three interrupted sutures of 3 metric polypropylene (Prolene; Ethicon) were placed through these holes (Figure 4) and through the detached serratus ventralis muscle to close the defect. Closure was routine. Upon manipulation the stability of the right scapula was comparable with that on the left. Postoperative analgesia was maintained with methadone (0.1 mg/kg, IV q6h) for the first 48 h and with buprenorphine (0.02 mg/kg, IV q8h) thereafter. Meloxicam (0.05mg/kg, PO q24h) was also administered for 7 days postoperatively.

Cat in lateral recumbency (head towards right of image) demonstrating displacement of the scapula and overlying soft tissue swelling, presumed haematoma
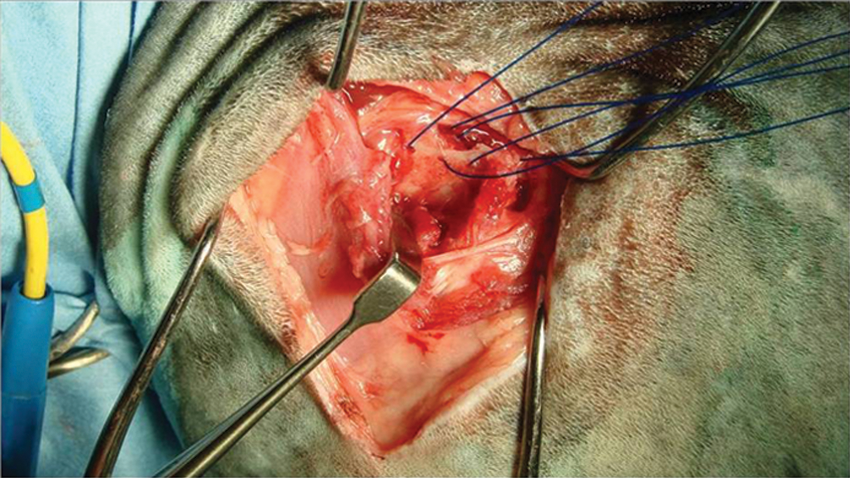
Intraoperative picture demonstrating the three 1.5 mm holes drilled in the dorsal margin of the scapula with polypropylene sutures in place (dorsal is to the top of the picture). The defect in the dorsal margin following detachment of the small sliver of bone is also evident
The cat was weight bearing on the first day postoperatively with a similar degree of lameness to that noted pre-operatively and was discharged 5 days postoperatively. Cage rest with periods of harness walking and passive range of motion physiotherapy were advised.
Reassessment was performed 7 weeks postoperatively. The cat had not tolerated physiotherapy or harness walking. Gait assessment revealed a barely discernible right thoracic limb lameness. No crepitus was palpable upon palpation over the scapula. Upon adduction of the distal limb, the scapula remained stable and dorsal displacement was not possible. The swelling had resolved but mild infraspinatus and supraspinatus muscle atrophy was evident.
Sedation was achieved using medetomidine (Seda-start; Animalcare: 0.02 mg/kg, IV) and butorphanol (Torbugesic; Pfizer Animal Health: 0.2 mg/kg, IV) and repeat CT was performed. The margins of the scapular fracture were smoother and more rounded, but configuration of the fragments overall was unchanged. Mild callus formation was evident only at the most dorsal fragment. The defect in the serratus ventralis muscle was no longer evident, but slight irregularity in the contour and thickening of the muscle persisted compatible with healing (Figure 5). The cat was discharged with instructions for one room rest.

Lateral 3D reconstruction of right scapular fracture 7 weeks postoperatively demonstrating unchanged positioning of fragments but rounding of fracture edges compatible with chronicity. The 1.5 mm drill holes in the dorsal border are evident and it appears that one of the sutures has pulled through (arrow). D = dorsal, Cr = cranial, Ca = caudal
At reassessment 14 weeks postoperatively the cat remained on house rest. Gait assessment revealed resolution of lameness. The scapula remained palpably stable with no crepitus palpable. Muscle atrophy had resolved.
Sedation and CT were repeated to assess progression of osseous union prior to allowing an increase in exercise intensity. There were minimal changes compared with previously: the ventral scapular fragment had rotated slightly to be more in alignment with the scapular body; the scapular fragments were more rounded and slightly thicker with poor mineralisation of callus present — the appearance of which was consistent with a non-union. There was increased attenuation of the subcutaneous tissue dorsal to the scapula and flattening compatible with scar tissue formation.
In light of the excellent clinical outcome despite the lack of radiographic union, the cat was discharged with instructions to gradually return to a normal exercise regime.
To our knowledge, this is the first report of a scapular avulsion in conjunction with a comminuted scapular fracture in a cat; the use of CT to follow the progression of this fracture is novel.
Surgical treatment of scapular avulsion is recommended to avoid continued dorsal dislocation. 2 The goal of surgery is to temporarily stabilise the scapular body until fibrous healing has occurred. 2 When non-absorbable sutures secured through small holes in the scapula are used 2 it is recommended that a wire be placed between the caudal angle of the scapula and an adjacent rib to provide additional support. 2 In this large, active, overweight patient, supplementary support would have been desirable. However, the fracture involved the caudal scapular angle and the entire caudal border through which the circumcostal suture would have been placed, which negated this option. Use of a Velpeau sling and carpal flexion bandage were considered but not used because of the challenges of management in fractious feline patients. Thus, strict cage rest was recommended. In this patient, follow-up at 7 and 14 weeks showed a stable scapula, no crepitus upon manipulation, no lameness and resolution of swelling, indicating that even in a large, active patient, soft tissue repair combined with strict rest can be sufficient for successful stabilisation. Use of circumcostal sutures should therefore be considered carefully as the procedure is not without potential complications. 5
Fractures involving the scapula can either be managed surgically or conservatively. Type 1 fractures involve the scapular body, type 2 the scapular spine and acromion process, and type 3 the scapular neck, supraglenoid tubercle and glenoid cavity. 8 A different classification accounts for the biomechanical principles which govern therapeutic decision-making and classifies fractures as stable extra-articular, unstable extra-articular or intra-articular.7,8 The fracture in this cat would be classified as type 1 or unstable extra-articular. Most fractures of the scapular body can be treated conservatively but open reduction may result in a more rapid and certain recovery in cases with severe displacement. 4 Moderate displacement of the ventral angle and caudal border of the scapula was evident here. A retrospective review of displaced scapular fractures in humans reported that all fractures healed and no differences were found in return to work, pain, or complications between operative and non-operative treatment. It concluded that operating on any scapular neck or body fracture displaced less than 20 mm was not recommended. 9 These results cannot be applied directly to our patient as cats must bear weight on their thoracic limbs and the anatomy of the human scapula is different. To our knowledge, only one veterinary report exists which compares surgical treatment of scapular body fractures with conservative therapy. 10 This concluded that plating was advantageous in that it enhanced early healing and return to function, but long-term results were similar between treatments. In this study, the ‘fractures’ were created necessitating a surgical approach in both groups. This negated one of the major advantages of conservative management 9 and may have biased the study in favour of surgical management. Despite this, no long-term advantage of surgical treatment was found. Surgical management of scapular fractures for this case would have been complex because of the extensive approach required, the small fragment size, and the thin and fragile nature of the scapular body. Therefore, as the scapular neck, glenoid cavity, supraglenoid tubercle, supraspinous fossa and cranial border remained intact we elected for conservative management of the scapular fractures. In contrast, the stabilisation of the scapula was achievable through a small approach with no significant further compromise to the soft tissue envelope.
Arguably, there is a distinction to be drawn between simple scapular injuries and more complex ones; isolated scapular body fractures treated conservatively in humans have a better prognosis than those in patients with multiple injuries. 11 One of the postulated explanations is that associated thoracic injuries may influence functional outcome by affecting the thoracoscapular joint. 11 The cat reported here had a combination of injuries affecting the thoracoscapular joint and thus might have been expected to have a more guarded prognosis.
To our knowledge, radiographic follow-up of conservatively-managed scapular fractures in cats has not been reported, rendering progression of these unknown. In this report at 7 weeks, very little callus formation was evident with the major finding being fragment remodelling. At 14 weeks the appearance was consistent with a non-union or a fibrous union. Similarly, in human patients, imaging follow-up is rarely obtained in patients without symptoms at clinical follow-up. 11 An appreciation of what would normally be expected for these cases is useful such that unusual complications can be recognised and treated appropriately. For example, delayed unions of scapular fractures are an unusual cause of persistent shoulder pain in humans. 12 Whether this can be extrapolated to our feline patients is unknown currently. Further intervention may be necessary should chronic pain associated with scapular non-union become evident.
Conclusions
This case report details the presentation, management and follow-up for a case of scapular avulsion with concomitant comminuted scapular fracture. In this case, soft tissue repair followed by cage rest offered excellent function of the injured limb following an initial debilitating injury. Further studies to document the outcome of similar cases would be beneficial, as would a comparison of outcome following surgical and conservative therapy.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.