
Abstract
The case described herein presented with craniofacial malformations resembling hemifacial microsomia (HFM), a congenital disorder described in humans. To our knowledge, this is the first reported case of HFM in a domestic cat.
Case Report
A 5-month-old, male, entire, domestic shorthair (DSH) kitten was presented to the Valentine Charlton Cat Centre for further investigation of malocclusion of the jaw, which had been noted by the owner since the kitten was acquired as a stray at approximately 12 weeks of age. On physical examination, the mandible was displaced 5 mm to the right, causing malalignment of the teeth and ulceration of the right upper gingiva by the right mandibular canine tooth. Retained maxillary deciduous canine teeth were present bilaterally. The right pinna was vestigial and there was no opening to an external ear canal (Figure 1). A rice grain-sized cutaneous papule was present over the right mandible.
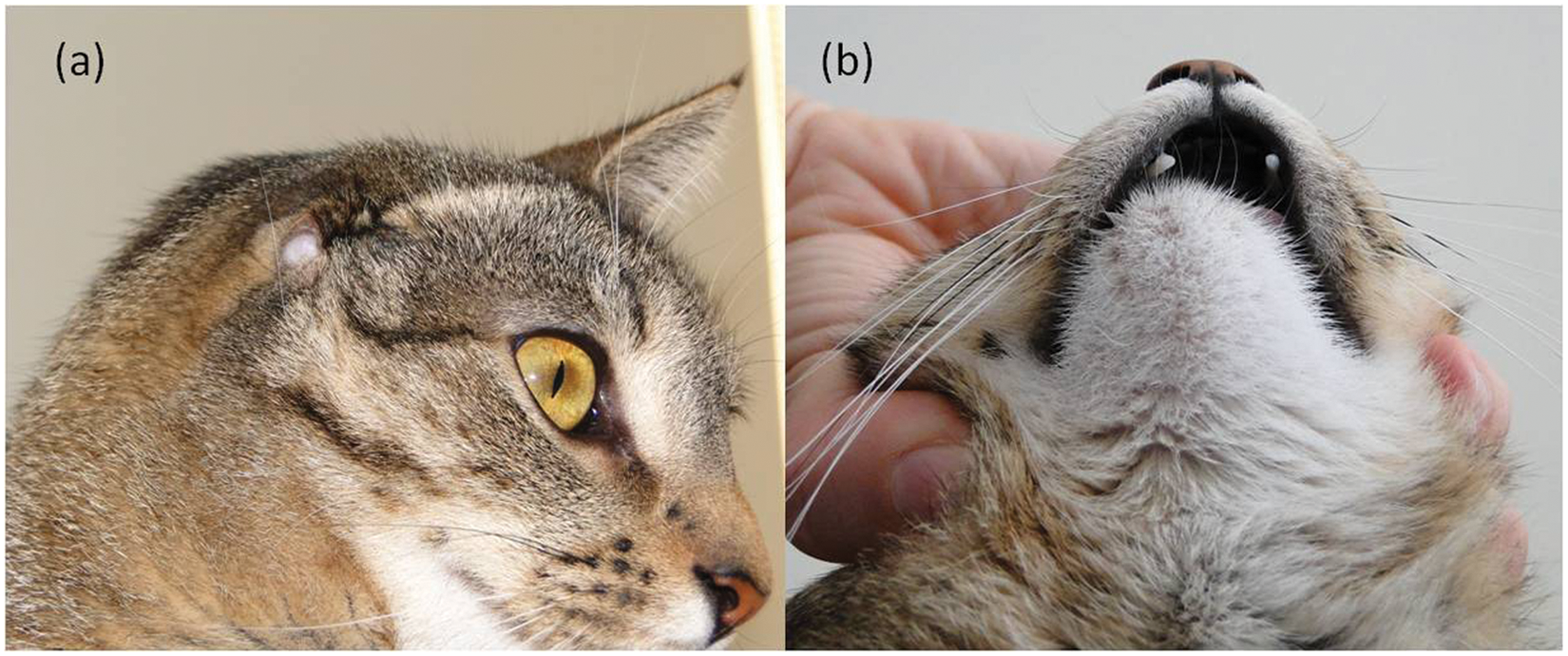
Vestigial right pinna and absent external ear canal (a) and right mandibular drift at 18 months of age (b)
An axial helical computed tomography (CT) scan of the skull was performed under general anaesthesia using a Philips CT 16 Slice and Brilliance 190P computer system. Ultra-high resolution helical slices were obtained both pre- and post-administration of 3.78 g iohexol intravenously (IV) (Omnipaque; GE Healthcare), with the following thin bone imaging parameters: 0.80 mm slice thickness; 0.4 mm slice increment; 0.5 s rotation time; 0.417 pitch; 120 kilovolts (kV) and 251 milliamps per second (mAs). The CT scan revealed agenesis of the lateral compartment of the right tympanic bulla, external acoustic meatus, tympanic membrane and pinna (Figure 2). The squamous portion of the temporal bone was malformed. The base of the zygomatic process, including the mandibular fossa and retroglenoid process of the temporal bone, were not formed. The lateral portion of the zygomatic process was present and received a small, malformed mandibular condyle to form a temporomandibular joint (TMJ) (Figure 2). It was concluded that the kitten had congenital malformation of the right temporal bone and right mandible, and agenesis of the right external ear.

(a) Transverse CT skull, thin bone window. Compared with the left side there is agenesis of the lateral compartment of the right tympanic bulla, external acoustic meatus and pinna. (b, c) CT three-dimensional skull reconstruction. Note the small, malformed squamous portion of the temporal bone and absent base of the zygomatic process, including the mandibular fossa and retroglenoid process on the right side (b) compared with the normal structures on the left (c). In addition, on the right, the lateral portion of the zygomatic process receives a small, malformed mandibular condyle to form a temporomandibular joint
Surgical mandibular realignment techniques to improve dental occlusion and/or tooth extraction were considered. Tooth extraction was chosen initially as the least invasive method. The right and left mandibular adult canine teeth were extracted to prevent further oral mucosa ulceration. Lignocaine (Xylocaine; AstraZeneca) 0.4 mg was administered to block the mental nerve. A gingival flap was raised to close the deficit using absorbable sutures. The ulcer created from the right lower canine was left to heal as an open wound. The deciduous upper canines were also removed. Post-surgery, the patient was given buprenorphine (Temgesic; Reckitt Benckiser) 0.029 mg IV for pain relief. The kitten was eating and drinking well within 3 h, and was discharged the following day on amoxycillin/clavulanic acid (Clavulox; Pfizer) 50 mg twice daily orally for seven days and a soft food diet. As there was no requirement for cerumen drainage, surgery was not performed on the right ear.
The kitten was monitored for further mandibular drift that could cause mucosal ulceration or palate perforation. Eight months post-surgery, the kitten represented for left-side, hard palate ulceration caused by the left mandibular third pre-molar and first molar teeth. To prevent perforation, all mandibular pre-molar and molar teeth were removed. At the time of writing, 12 months after initial presentation, there has been no further mandibular drift (Figure 1b). The patient has grown normally, and is maintained on a wet and dry food diet with no evidence of difficulty prehending food.
Additional investigations were performed to rule out concurrent congenital defects. Thoracic radiographs, haematology and biochemistry profiles, and urinalysis showed no abnormalities. Echocardiography revealed hypertrophy of the anterior papillary muscle of the left ventricle (8.6 mm long × 3.6 mm wide), with associated abnormal chordae tendinae tethered from the papillary muscle to the ventricular septum, without restrictive ventricular filling or mitral valve insufficiency. Currently, the patient has no clinical signs of heart disease.
The embryological development of feline craniofacial structures depends on the migration, proliferation and differentiation of neural crest, somitomere and cranial somite cells, and the formation of arches, grooves and branches. 1 The first and second branchial arches, first branchial groove, pharyngeal pouch and otic placode give rise to craniofacial features, including the ear, temporal bone, mandible, maxilla and zygomatic arch. 1 Congenital malformations can result from disruptions to cell migration and differentiation. 1
Congenital craniofacial malformations have been recorded in chickens and mice, and are well documented in humans. Aetiologies include inherited disorders, placental blood flow disruption, physical trauma, interference with chondrogenesis, hypervitaminosis A, excessive exposure to retinoic acid, and defects in embryonic cell signalling proteins and growth factors. Reports of feline congenital craniofacial abnormalities are limited almost entirely to descriptions in stillborns or those suffering periparturient death.2–5
The unilateral craniofacial abnormalities described in this kitten resemble the human congenital disorder hemifacial microsomia (HFM). Seventy percent of human HFM cases are unilateral, with hypoplasia and malformation of the facial skeleton, especially the mandible, maxilla, ear and zygomatic bone.6,7 In humans and chickens, HFM is more common in males, with right-side dominance more prevalent.6,8 Interestingly, the kitten described here was male with right-side defects. HFM in humans is classified into types I–V, depending on the extent of involvement of the TMJ, zygomatic arch and orbit. 9 The findings in this kitten correspond to type III HFM, as defined by the absence of a functional TMJ and a hypoplastic zygomatic arch. Concurrent defects in extracraniofacial structures, known as oculoauriculovertebral spectrum (OAVS), are seen in approximately 50% of human HFM cases.10,11 OAVS includes heart, kidney, lung, skeletal and ocular defects. 11 There was no evidence of extracraniofacial defects on thoracic radiographs, haematology, biochemistry or urinalysis in the case described here. The papillary muscle hypertrophy noted in this case has been recorded in humans and cats to be associated with hypertrophic cardiomyopathy (HCM) and left ventricular outflow obstruction.12–15 It is thought to be either a new subtype or early form of HCM, 12 and is rare in humans.16,17 In contrast, the most commonly seen heart defects in humans with OAVS are tetralogy of Fallot and ventricular septal defect; however, no single cardiac lesion is characteristic.18,19
This case was successfully managed with dental extractions, as reported previously in an 11-year-old DSH cat with class 1 malocclusion of the mandibular canine teeth and maxillary right and left third incisor teeth. 20 Surgical treatment of HFM in humans depends on the severity and classification, but generally involves mandibular and/or maxillary osteotomies with and without bone grafting, and acute correction or distraction osteogenesis.9,21 Surgery to realign and lengthen the mandibular body by osteotomy of the mandibular body and acute distraction or distraction osteogenesis was considered in this case; however, cosmetic appearance is not so important in cats and invasive techniques may not be warranted if tooth extraction produces good clinical results. Another, potentially less invasive, method to restore dental occlusion in the presence of maxillary—mandibular malalignment is to osteotomise the mandibular symphysis and realign the mandibular bodies to match the maxilla. This technique was successfully applied in eight cats with malocclusion secondary to maxillary impaction fractures. 22 However, tooth extractions may still be necessary after surgical realignment. 22
Footnotes
Acknowledgements
The authors would like to thank staff at the University Veterinary Teaching Hospital for their contributions to case management, including Helen Laurendet, Senior Radiographer; Dr Richard Lam, Resident in Diagnostic Imaging; Katherine Briscoe, Senior Registrar in Feline Medicine; and Niek Beijerink, Specialist in Veterinary Cardiology.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Accepted: 23 April 2012