
Abstract
A rare case of bilateral fusion of a supernumerary kidney was found during the necropsy of a female, 8-year-old, mixed breed cat that died as a result of azotemia and chronic enteritis. Apart from enteritis, necropsy revealed four kidneys, two in the sublumbar left region and two in the sublumbar right region, with cortical and medullary regions well individualized and independent; however, the pelvis was partially fused, giving rise to a single ureter. The kidneys were small, whitish and firm, with irregular surfaces. Microscopically, all kidneys displayed normal renal glomeruli and tubules among the immature renal glomeruli and tubules with characteristics of hypoplasia. Foci of glomerulosclerosis, nephrocalcinosis and interstitial fibrosis were also observed.
Case Report
A supernumerary kidney is a rare congenital anomaly of the genitourinary tract, particularly when it occurs bilaterally. 1 It is among the rarest anomalies of the genitourinary tract,1–3 with fewer than 100 cases reported in human medicine 1 and only two cases reported in animals, one in a wild pig 4 and the other in a monkey. 5 In fact, to the best of our knowledge, only two cases in animals have been described. This is the first reported case of a supernumerary kidney in a cat.
It is believed that the supernumerary kidney may be formed during embryonic development from two ureteral buds that originate from the caudal end of the Wolffian ducts so that they penetrate the nephrogenic blastema and form two kidneys.
The objective of this report is to describe a rare case of bilateral fusion of the supernumerary kidney that was found during the necropsy of a female cat.
A female, 8-year-old, mixed breed cat died and was forwarded to the Department of Pathology of the Veterinary Hospital of Universidade Federal de Minas Gerais for necropsy. The clinical history provided by the pet owner showed that the animal had weight loss, lack of appetite and diarrhea. The results of hematology and serum biochemistry showed leukocytosis (29,400 leukocytes/mm3; reference interval (RI) 6000–19,000/mm3), elevated urea (390 mg/dl; RI 10–30 mg/dl) and creatinine (6.26 mg/dl; RI 0.7–1.8 mg/dl). The other parameters (blood count and liver enzymes) were normal. Serology for feline immunodeficiency virus, feline leukemia and feline infectious peritonitis was negative.
Necropsy revealed four kidneys, two located in the sublumbar left region and two in the sublumbar right region. The kidneys were small, with the kidneys on the right side measuring 4 × 3 cm and 3 × 3 cm; on the left side kidneys measured 4 × 3 cm each. The kidneys showed cortical and medullary regions that were individualized and independent but partially fused with the pelvis, giving rise to a single ureter. The kidneys had an irregular surface, with pale, firm and whitish striations in the medullary region (Figure 1a, b). The capsules were independent and fused to one pole of each kidney. The ureters exited the renal hilum and traveled the sublumbar region to the bladder trigone (Figure 1c). The lower urinary tract showed no macroscopic changes. In addition, in small intestine, there was enteritis characterized by discrete hyperemia, a thick fibrous wall, diarrhea and mesenteric lymphoadenomegaly.
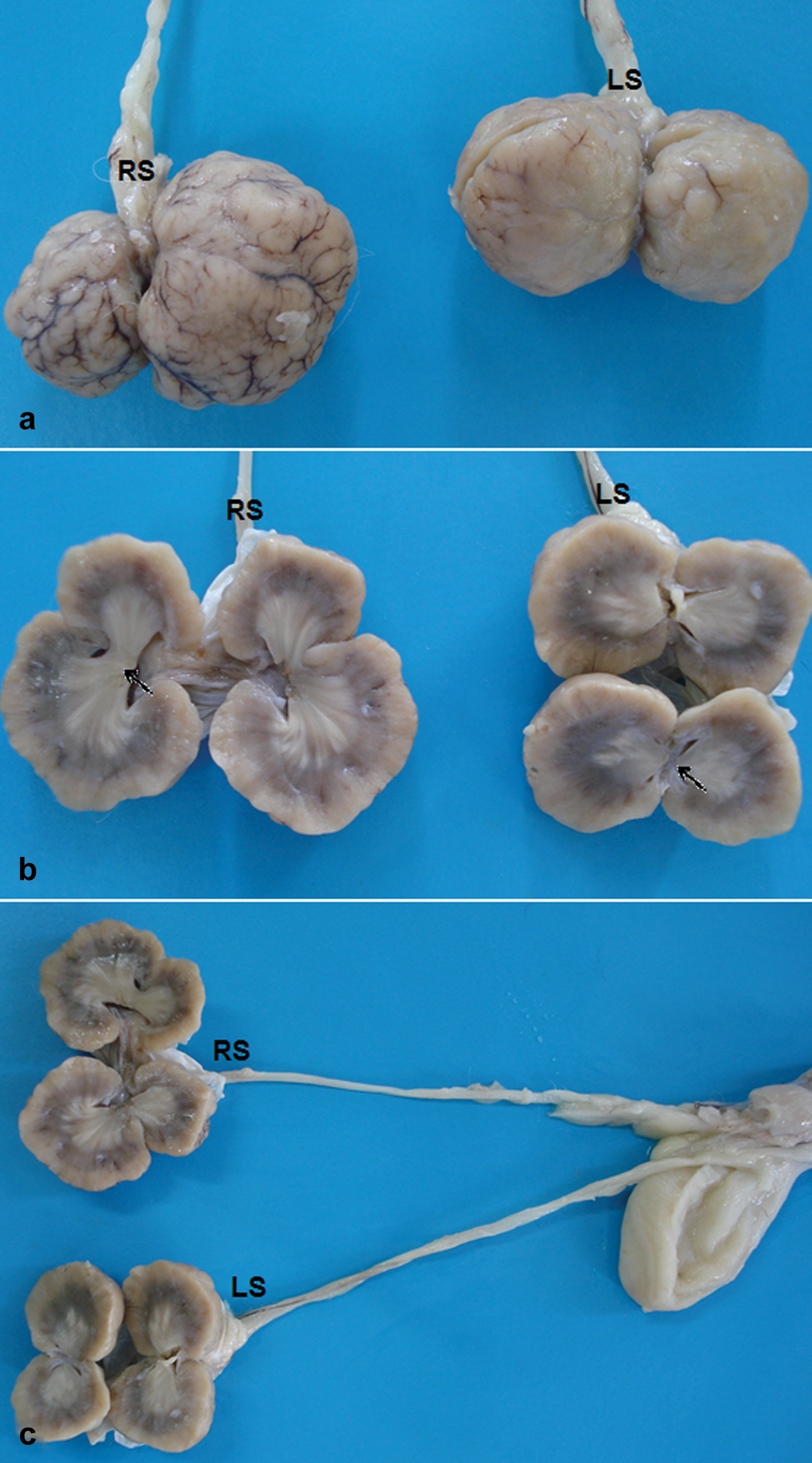
Bilateral fusion of a supernumerary kidney in a cat. (a) Right and left kidneys of small size, with an irregular surface and whitish color. (b) Kidneys with cortical and medullary regions that are well individualized and independent but with the pelvis partially fused (arrow), giving rise to a single ureter. (c) Ureters leave the renal hilum and travel to the bladder trigone, showing no macroscopic changes (RS = right side, LR = left side)
Fragments of four kidneys, large and small intestines and other organs were fixed in 10% neutral phosphate-buffered formalin, embedded in paraffin, cut at 5 µm, and stained with hematoxylin and eosin for morphological analysis. The kidney tissue was also stained with Masson’s trichrome and von Kossa to evaluate renal fibrosis and mineralization, respectively.
The four kidneys showed similar histological features characterized by congenital and acquired pathological changes. The cortex had multifocal areas of normal renal glomeruli, tubules among immature renal glomeruli and tubules characteristic of discrete hypoplasia (Figure 2a, b). In addition, foci of fibrosis, glomerulosclerosis and nephrocalcinosis were observed and confirmed by Masson’s trichrome and von Kossa techniques, respectively (Figure 2c, d). Histology of the small intestine showed foci of necrosis and discrete lymphocytic infiltrate associated with atrophy and fusion of intestinal villous and multifocal fibrosis. The other organs were histologically normal.

Bilateral fusion of a supernumerary kidney in a cat. (a) Cortical with multifocal areas of normal renal tissue and hypoplasia (asterisk). Hematoxylin and eosin (H&E), bar = 63 µm. (b) Immature renal glomeruli (arrows). H&E, bar = 8.0 μm. (c) Multifocal foci of glomerular fibrosis in blue. Masson’s trichrome, bar = 28 µm. (d) Nephrocalcinosis in brown, von Kossa, bar = 32 µm
Based on the macroscopic and microscopic findings, a diagnosis of bilateral fusion of supernumerary kidneys was confirmed.
The embryogenesis of a supernumerary kidney is poorly known. One hypothesis is that the supernumerary kidney may be formed during embryonic development from two ureteral buds that originate from the caudal end of the Wolffian ducts so that they penetrate the nephrogenic blastema and form two kidneys. Another hypothesis is that there is a bifurcation of the Wolffian ducts that gives rise to two kidneys after penetrating the metanephric blastema, leading to the formation of a double ureter,3,6 which was not observed in this case. Fusion of the bilateral supernumerary kidney in this case may have been the result of the development and approach of two ureteral buds from the Wolffian ducts, with subsequent fusion caused by contact between them and the metanephric blastema. 7
Although a supernumerary kidney is a congenital anomaly, the diagnosis occurs (incidentally or not) during adulthood. 3 In this report, the finding was incidental; the animal’s death was caused by azotemia and intense chronic enteritis, the cause of which could not be identified.
When identified, the supernumerary kidney is usually hypoplastic. 2 It can be encapsulated and completely separated from the ipsilateral kidney or partially fused. In this case, the macro- and microscopic features of all the kidneys were similar, which impeded the identification of supernumerary kidney.
All types of renal malformations are often associated with changes in other organs, particularly in the genitourinary tract. The few cases of supernumerary kidneys diagnosed in humans have also been associated with other urogenital anomalies, including horseshoe kidney, ectopic ureter, urethral duplication, double penis, vaginal atresia and posterior urethral valve.1,3,7 However, in this case, no alteration of the development was observed in the lower urinary tract in any other system.
The methods used to diagnose a supernumerary kidney in humans include intravenous urography, retrograde pyelography, nuclear scintigraphy, ultrasound, computed tomography, magnetic resonance imaging and angiography. 3 Treatment will depend on renal function and whether there are associated symptoms. Supernumerary kidney nephrectomy is performed in cases of urinary incontinence resulting from ectopic ureteral drainage caused by urinary stasis, infection or calculi formation when there are symptoms of pain caused by its physical presence or when neoplastic processes have developed.1,3,8,9
Footnotes
Funding
This work was supported by grants from Pró-reitoria de Pesquisa da Universidade Federal de Minas Gerais (PRPq/UFMG).
Conflict of interest
None of the authors have any conflicts of interest to declare.