
Abstract
Dermatophytosis is a contagious superficial fungal infection of the stratum corneum, hair and nails most often caused, in the cat, by Microsporum canis. 1 Feline dermatophytosis has a plethora of clinical presentations ranging from focal or multifocal alopecia with scaling and minimal inflammation to more inflammatory lesions characterised by erythema, scaling, crusting and follicular papules, miliary dermatitis, exfoliative generalised dermatitis, otitis externa, chin acne, tail seborrhoea, pseudomycetoma and onychomycosis. 1 An unusual presentation of dermatophytosis with hyperpigmented lesions has been described in a young Devon Rex cat. 2
Papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa-like dermatitis), a condition reported in 2004 in five Devon Rex cats, is clinically characterised by a maculopapular, often hyperpigmented and/or crusted, cutaneous eruption. 3 Histopathological examination reveals a perivascular to diffuse mastocytic and eosinophilic infiltrate in the dermis. 3 These features are similar, although not identical, to a condition called feline urticaria pigmentosa, which was reported in 1996 in three related Sphynx cats and histopathologically characterised by a perivascular to diffuse dermal and subcutaneous infiltrate of well-differentiated mast cells. 4 The Devon Rex and Sphynx breeds are genetically related and have recently been shown to share a mutation of the KRT71 (Keratin 71) gene.5,6 Both diseases have been compared with human cutaneous indolent mastocytosis, also known as urticaria pigmentosa, which occurs mainly in children. 7 However, the two feline conditions are not identical and it is not clear whether they both represent analogues of human urticaria pigmentosa. In Devon Rex cats, it has been suggested that papular eosinophilic/mastocytic dermatitis could represent a reaction pattern, similar to miliary dermatitis or eosinophilic granuloma, specific to the breed. 3
This report describes three cases of dermatophytosis with clinical and histopathological features suggestive of papular eosinophilic/mastocytic dermatitis in Devon Rex cats.
Clinical reports
Case 1
A 7-month-old female Devon Rex cat was presented with a 2-week history of non-pruritic skin disease. The cutaneous lesions were noticed approximately 3 weeks after discontinuation of a 4-week course of itraconazole (Sporanox; Janssen Cilag) administered by the referring veterinarian for suspected dermatophytosis in a housemate cat. The cat lived indoors with four other cats and three dogs, was fed a commercial dry food and home-cooked fish or turkey, was regularly vaccinated and on ectoparasite prevention with selamectin spot-on once monthly (Stronghold; Pfizer).
On general physical examination, the cat was healthy with abnormalities restricted to the skin. Dermatological examination revealed multiple erythematous papules, some of which had a crusted and hyperpigmented surface, located on the head, neck, chest and abdomen (Figure 1). Differential diagnoses included papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa like-dermatitis), feline atopic dermatitis, adverse food reaction, flea bite hypersensitivity, dermatophytosis and viral plaques.

Erythematous crusted lesions on the ventral chest of case 1
Wood’s lamp examination and microscopic examination of plucked hair were negative and cytological examination of material obtained from the papules showed a neutrophilic inflammatory infiltrate with moderate numbers of macrophages and eosinophils. Due to the clinical presentation being strongly suggestive of papular eosinophilic/mastocytic dermatitis, multiple 6 mm punch biopsies were taken. Specimens were fixed in 10% buffered formalin and stained with haematoxylin and eosin (H&E) and periodic acid-Schiff (PAS). Histopathological examination revealed epidermal and infundibular hyperplasia with epidermal hypermelanosis and interstitial to diffuse dermatitis characterised by a prevalence of mast cells and eosinophils. Microscopic examination showed a few fungal spores in just a single follicular infundibulum (Figure 2). Spores were only detected after performing several microscopic sections.
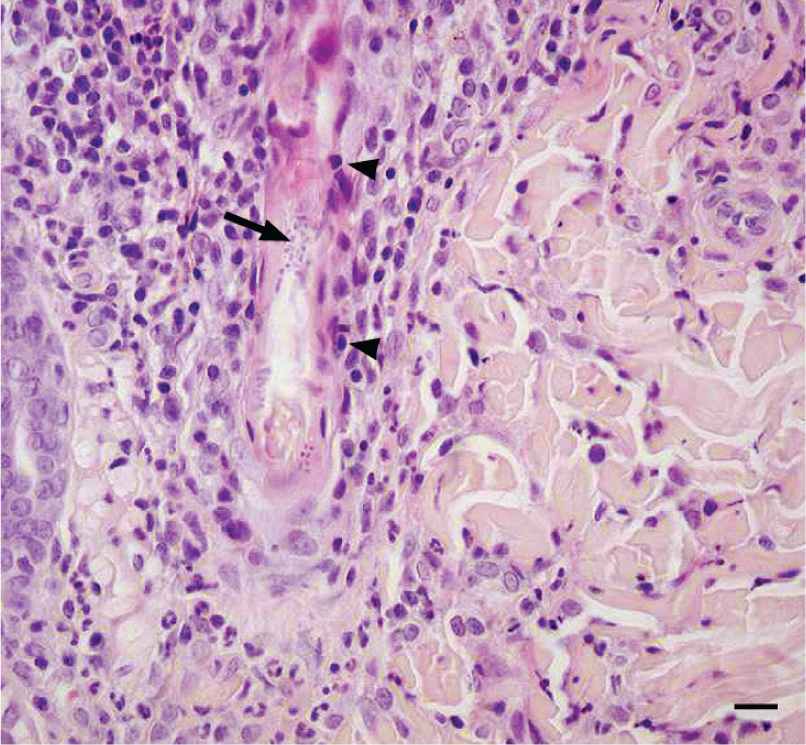
Fungal arthrospores within a follicular infundibulum (arrow) in case 1. Surrounding the infundibulum, with a perivascular to interstitial distribution, a mixed population of inflammatory cells is evident. Non-degenerate neutrophils and small mature lymphocytes are prevalent, with fewer numbers of macrophages and occasional plasma cells. The follicular infundibulum is characterised by minimal mural infiltration by small mature lymphocytes (arrowheads). Haematoxylin and eosin (H&E), bar = 27 µm
Other features seen in case 1 included follicular keratosis, neutrophilic exocytosis, lymphocytic mural folliculitis and deep perivascular lymphoplasmacytic dermatitis. The final diagnosis was dermatophytosis.
The cat showed a complete clinical response to itraconazole given at 5 mg/kg orally q24h for 4 weeks, and was negative on fungal culture at the end of the treatment. All the in-contact animals received the same systemic treatment. Topical therapy and environmental decontamination, as well as a second fungal culture to be performed a few weeks after stopping the treatment, although strongly advised, were all declined by the owner.
Case 2
A 10-month-old male Devon Rex cat was presented with a 2-week history of non-pruritic skin disease. The cat had been treated by the referring veterinarian for suspected superficial pyoderma with amoxicillin and clavulanic acid (Synulox; Pfizer) for 11 days, but this produced no improvement. The cat lived indoors with seven other cats, was fed commercial dry and canned food, was regularly vaccinated and on ectoparasite prevention with selamectin spot-on once monthly.
General physical examination was unrewarding, with abnormalities restricted to the skin. Dermatological examination revealed multiple erythematous papules, some of which had a crusted and hyperpigmented surface, located on the chest and in the groin. The papules on the chest had a linear distribution (Figure 3) and erythema involving the medial aspect of both front legs was also observed. Differential diagnoses included papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa-like dermatitis), feline atopic dermatitis, adverse food reaction, flea bite hypersensitivity, dermatophytosis and viral plaques.

Multiple erythematous papules with a linear distribution on the lateral chest of case 2
Wood’s lamp examination and microscopic examination of plucked hair were negative, while fungal culture performed by toothbrush technique was positive for M canis. Due to the clinical presentation, which was strongly suggestive of papular eosinophilic/mastocytic dermatitis, the significance of a positive fungal culture was considered questionable, and a possible consequence of environmental contamination. Multiple 6 mm punch biopsies were taken and specimens were fixed in 10% buffered formalin and stained with H&E and PAS. Histopathological examination revealed epidermal and infundibular hyperplasia with epidermal hypermelanosis and interstitial to diffuse dermatitis characterised by an abundance of mast cells and eosinophils. Microscopic examination also showed a few fungal spores in only one follicular infundibulum. The final diagnosis was dermatophytosis.
The cat showed a complete clinical response to itraconazole, which was given at 5 mg/kg orally q24h for 4 weeks, and was negative on fungal culture at the end of the treatment. A second fungal culture, to be performed a few weeks after stopping the treatment, was declined by the owner. Topical therapy and environmental decontamination, although strongly advised, were also declined by the owner. The cat relapsed after participating in a cat show and showed a favourable clinical response when treated again with the same therapeutic protocol.
Case 3
A 1-year-old male neutered Devon Rex cat was presented with a 5-month history of moderately pruritic skin disease. The cat had been previously treated with a topical product containing thiabendazole, neomycin and dexamethasone (Tresaderm; Merial) with no improvement. The cat was housed indoors with no other pets, regularly vaccinated, fed a commercial dry food and on ectoparasite prevention with selamectin spot-on once monthly.
On physical examination, the cat was healthy with abnormalities restricted to the skin. Dermatological examination revealed multiple coalescing, hyperpigmented areas of alopecia involving the whole dorsum and the tail (Figure 4), and multiple erythematous papules with a linear distribution on the ventral chest (Figure 5). Differential diagnoses included dermatophytosis, demodicosis, papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa-like dermatitis), feline atopic dermatitis, adverse food reaction and flea bite hypersensitivity.

Multiple coalescing, hyperpigmented areas of alopecia involving the dorsum of case 3

Multiple erythematous papules with a linear distribution on the ventral chest of case 3
Multiple deep skin scrapings were negative for Demodex mites, and cytological tape strip examination revealed only a few corneocytes. Wood’s lamp examination and microscopic examination of plucked hair were also negative, and hair samples for fungal culture were collected by toothbrush technique from the whole body. Multiple 6 mm punch biopsies were taken from the papular lesions on the ventral chest and from one alopecic area on the dorsum, fixed in 10% buffered formalin and stained with H&E and PAS.
Histopathological examination revealed moderate epidermal hyperplasia and hyperkeratosis with focal parakeratosis and diffuse interstitial eosinophilic and mastocytic dermatitis (Figure 6). These features were consistent with a diagnosis of papular eosinophilic/mastocytic dermatitis. Fungal culture was positive for M canis and, following this result, the pathologist was asked to re-examine the slides and cut additional sections in order to demonstrate or exclude the presence of dermatophytes. Multiple PAS-stained sections were examined, but no fungal elements could be observed. The final diagnosis in case 3 was dermatophytosis and papular eosinophilic/mastocytic dermatitis.

Moderate epidermal hyperplasia and hyperkeratosis with focal parakeratosis and interstitial moderate eosinophilic and mastocytic dermatitis (case 3). H&E, bar = 50 µm
The cat was treated for dermatophytosis with itraconazole at 5 mg/kg orally q24h and enilconazole (Imaverol; Janssen Cilag) rinses every fourth day. For papular eosinophilic/mastocytic dermatitis cetirizine (Zirtec; UCB Pharma) 1 mg/kg orally q24h and fatty acid supplementation (Ribes Pet 80; NBF Lanes) orally q24h were administered. Three weeks later, the papular eruption on the ventral chest had disappeared and treatment for papular eosinophilic/mastocytic dermatitis was discontinued by the owner. The lesions recurred within 1 week and therapy with cetirizine and fatty acids was resumed. Treatment for dermatophytosis was continued until two consecutive negative fungal cultures, performed 4 weeks apart, had been obtained (total duration 10 weeks).
After the second negative fungal culture, the lesions consistent with papular eosinophilic/mastocytic dermatitis were in remission and therapy for this disease could be discontinued without further relapses. At the time of writing, 2.5 years later, no recurrence of papular eosinophilic/mastocytic dermatitis had been observed.
Discussion
The three cases described here presented with clinical and histopathological features suggestive of papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa-like dermatitis), but were eventually found to be affected by dermatophytosis.
The characteristic cutaneous eruption of papular eosinophilic/mastocytic dermatitis, with hyperpigmented papules and macules, sometimes with a linear distribution and mainly located on the trunk, is very similar in Devon Rex and Sphynx cats and has a juvenile onset in both breeds.3,4 Clinical findings in the three cats reported closely resembled the previously described cases of papular eosinophilic/mastocytic dermatitis, with lesions developing at 7 months to 1 year of age. Dermatophytosis is also very common in young cats, with lesions typically characterised by multifocal alopecia and scaling, 1 and this characteristic presentation along with hyperpigmentation was observed only in case 3. Atypical hyperpigmented circular areas on the trunk have been described also in a young Devon Rex cat with dermatophytosis. 2 Pruritus was reported in all Sphynx cats with urticaria pigmentosa but seemed to be variably present in the Devon Rex cats,3,4 as it was for the cats described in this report. The severity of pruritus also varies in cats with dermatophytosis. 1
Fungal culture was positive for two of the three cats (cases 2 and 3) and was not performed in case 1, because the clinical presentation was not particularly suggestive of dermatophytosis. In case 1, the diagnosis was obtained by histopathological examination. A few fungal spores in a single follicular infundibulum could be observed on histopathology in cases 1 and 2, underlining the low sensitivity of histopathology as a diagnostic test for dermatophytosis. In case 3, despite a careful search with the aid of PAS stain, the presence of dermatophytes was not confirmed, while the fungal culture performed by toothbrush technique on the whole body was positive. As biopsies in this cat were also taken from both the ventral chest and the dorsum, it is not possible to ascertain whether dermatophytosis could have been causing a clinical and histopathological reaction compatible with papular eosinophilic/mastocytic dermatitis or whether dermatophytosis could have been just a concurrent infection in a cat with papular eosinophilic/mastocytic dermatitis.
The other histopathological features were suggestive of papular eosinophilic/mastocytic dermatitis in all cases. Histopathologically, the conditions described in Devon Rex and Sphynx cats are both characterised by a moderate to severe, perivascular to diffuse infiltrate of well-differentiated mast cells, with variable numbers of eosinophils, which seem to be more numerous in Devon Rex cats with this disease; fungal cultures were negative in those cases.3,4,8 In feline dermatophytosis, eosinophils may be present within a mixed inflammatory infiltrate around hair follicles, within follicular pustules and in furuncles surrounding free hair shafts, although they are usually observed in small numbers. 8
All cases were treated with antifungals (systemic itraconazole and, in case 3, topical enilconazole), 9 and showed a complete response. Enilconazole is not licensed for cats, as fatal idiosyncratic reactions have been reported; however, studies have since shown that it can be used safely in cats.10,11 In case 2, dermatophytosis recurred following participation in a cat show, but this was considered to be a reinfection and not a relapse. In case 3, cetirizine and essential fatty acids were also prescribed, as recommended by Noli et al, 3 because the cat was diagnosed as having papular eosinophilic/mastocytic dermatitis and concurrent dermatophytosis. Cetirizine and essential fatty acids could be permanently discontinued only after complete resolution of dermatophytosis, confirmed by negative fungal culture. No relapses of papular eosinophilic/mastocytic dermatitis were observed over the following 2.5 years.
Conclusions
Cases 1 and 2 represented atypical dermatophytosis mimicking papular eosinophilic/mastocytic dermatitis (urticaria pigmentosa-like dermatitis), as confirmed by positive fungal culture in case 2, by observing fungal spores in follicular infundibula in both cases and by response to antifungal treatment in both cats. Case 3 was different, as histopathological examination did not allow us to observe fungal spores despite a positive fungal culture and the cat seemed to respond to both antifungal and antihistamine and fatty acids treatments. This suggests either that dermatophytosis in Devon Rex cats could present with clinical and histopathological features identical to papular eosinophilic/mastocytic dermatitis or that this latter condition represents a breed-specific reaction pattern triggered by different diseases such as allergies or dermatophytosis, as proposed by Noli et al. 3
Therefore, at least in the Devon Rex breed, dermatophytosis should always be carefully ruled out in cats presenting with clinical and histopathological features suggestive of papular eosinophilic/mastocytic dermatitis. Wood’s lamp examination, microscopic examination of hair shafts and fungal culture, 12 as well as a careful search for dermatophytes on biopsies, which are suggestive of this disease, are strongly recommended, as the clinical presentation is atypical for feline dermatophytosis and fungal spores may be extremely difficult to find. The differential diagnosis is crucial and has a strong clinical relevance because most cases of papular eosinophilic/mastocytic dermatitis may be treated with glucocorticoids, which are contraindicated in cases of dermatophytosis.
Footnotes
Acknowledgements
The authors wish to thank Dr Giuseppina Azzolina and Clinica Veterinaria San Martino (Novara) for referring cases 2 and 3, respectively, and Dr Antonella Vercelli for histopatological examination of case 3.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case series.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Date accepted: 7 February 2012