
Abstract
The involvement of the greater omentum in reconstructive, abdominal and thoracic surgery is based on its manifold qualities, which include immunological support, lymphatic drainage, angiogenesis, adhesion, haemostasis and fat storage. The purpose of this study was to determine whether the greater omentum could be extended to the head. In addition, we evaluated the surgical procedures necessary for this extension. Our study reveals that specific surgical lengthening techniques of the greater omentum, such as dorsal extension and inverted L-shape elongation, are necessary to successfully transpose the omentum to the head in cats. As the survival of the omentum after transposition procedures is still unknown, its application in chronic non-healing wounds of the head in cats warrants further investigation.
Short Communication
Chronic non-healing head wounds in cats are difficult to manage because of poor local skin elasticity and the proximity of the eyes. Hence, the creation of local flaps can be challenging. Furthermore, a lack, or absence, of subcutaneous tissue in the head may contribute to delayed wound healing. Bohling et al demonstrated that, especially in feline patients, a lack or absence of subcutaneous tissue restricts the formation of granulation tissue, which is mandatory for secondary wound healing.1–3 Skin advancement flaps that are combined with omentalisation have been used to assist in the closure of chronically non-healing wounds in cats in a variety of locations.4–13 However, there are no reports of these techniques being used on the head. Therefore, the aim of this study was to determine whether the greater omentum could be extended to the head and, if so, what surgical procedures were necessary in cadaver cats.
Thirteen thawed cat cadavers were used in this study and were divided into two groups (six more than and six less than 5 kg). Their suitability for surgery was evaluated by assessing their level of decay. Only one cat had to be excluded from the study and replaced by a more suitable cadaver. An artificial rectangular skin wound was created above the frontal sinus using a 2 cm × 3 cm surgical drape as a template.
After a ventral midline coeliotomy was performed, the greater omentum was identified and its firmness was assessed. A firm omentum, as opposed to a soft omentum, was predicted to have a better chance of enduring the following steps of the procedure. The length of the greater omentum was measured from the centre of the greater gastric curvature to the caudal omental border. The width was measured parallel to the gastroepiploic arcade. The omentum was placed over the body towards the head to determine the need for a dorsal extension. If necessary, the dorsal extension was performed in accordance with the technique described by Hosgood in 1990 and Ross et al in 1993.8,12 The length and width of the omentum was again measured after the dorsal extension had been completed. The length of the newly extended omentum was re-evaluated by placing the omentum over the body towards the head. When the dorsal extension was insufficient to allow the omentum to reach the head wound, an inverted L-shaped elongation, as described by Hosgood and Ross et al, was performed.8,12 Measurements were taken after the dorsal extension and also when the inverted L-shaped extension was necessary. The next step of the study was to exteriorise the omentum. A 2-cm incision, large enough to avoid obstruction of vascular flow in a live patient, was made paramedially through the abdominal wall. The omentum was fed through the incision and kept moist using 0.9% saline-soaked swabs to prevent desiccation. The abdominal wall was closed in a routine manner. Subsequently, the cadaver was repositioned in lateral recumbency, with the head wound facing up. The third step of the study was the creation of the subcutaneous tunnel, through which the omentum would be pulled to reach the head wound. The tunnel was created using a 32 French metal trocar, which was slid subcutaneously, starting at the abdominal exit hole and along the thoracic wall, lateral to the shoulder. The trocar was then passed laterally to the neck until it reached the head wound. A 2 cm external diameter silicon tube was brought through the tunnel from the head wound and was positioned adjacent to the incision in the abdominal wall through which the omentum was passed. The distal-most aspect of the extended omentum was sutured with a single stitch of 2–0 monofilament Glycomer 631 (Biosyn; Syneture, provided by Covidien Vienna, Austria GmbH), and the suture was passed through a U-shaped steel wire. The open ends of the steel wire were pulled through the silicon tube and the omental pedicle was cautiously extracted at the level of the head. Subsequently, the tube was carefully withdrawn, tenting the pedicle at the recipient site. To mimic an actual surgical case, the omental pedicle was also sutured to the wound edges using simple interrupted sutures and 5–0 monofilament Glycomer 631 (Biosyn; Syneture, provided by Covidien Austria GmbH). Any damage or rupture of the pedicle during the procedure was noted. The results are recorded in the Table 1. The mean omental length prior to dorsal extension was 13.75 cm. This length was not sufficient to reach the head wound in any of the models. After dorsal extension, the mean length was 23.41 cm. In 41.7% (5 out of 12 — cats 1, 2, 7, 9, 11), this length was acceptable for reaching the wound. In 50% (cats 3–6, 10, 12) of the cases, the additional L-shaped extension was necessary, and the mean length achieved was 25.75 cm. Altogether, wound coverage was obtained in 66.7% (8 out of 12 — cats 1, 2, 5, 7, 9–12) of the cases using available omental tissue at the head. In only 50% (6 out of 12 — cats 1, 2, 5, 9, 11, 12 ) of the cases, coverage was attained without any damage or rupture of the omentum. In five cases (cats 3, 6–8, 10), damage or rupture occurred, or the available omental tissue appeared to be too thin for adequate coverage. Despite performing the inverted L-shaped extension in cat 4, the omental pedicle never reached the wound. In nine cases (cats 3, 4–7, 9–12) the width after dorsal elongation increased because the omental tissue could be more easily spread. Our results indicate that without any elongation technique, the omentalisation of a wound located at the head is not possible in the cat. Notably, cats over 5 kg had an omentum that was significantly more fat-infiltrated than smaller cats. This fact contributed to increased firmness in the larger cats, but made it more difficult to pull the omentum through the silicon tube. Therefore, in cats larger than 5 kg, a larger tube may be necessary. In cats smaller than 5 kg, transposition of the omentum was easily performed. However, given the omentum’s thin nature, the effectiveness of the transposed omentum at the wound site may have been jeopardised.
Dimensions of the omentum before and after dorsal and inverted L-shape elongation extensions
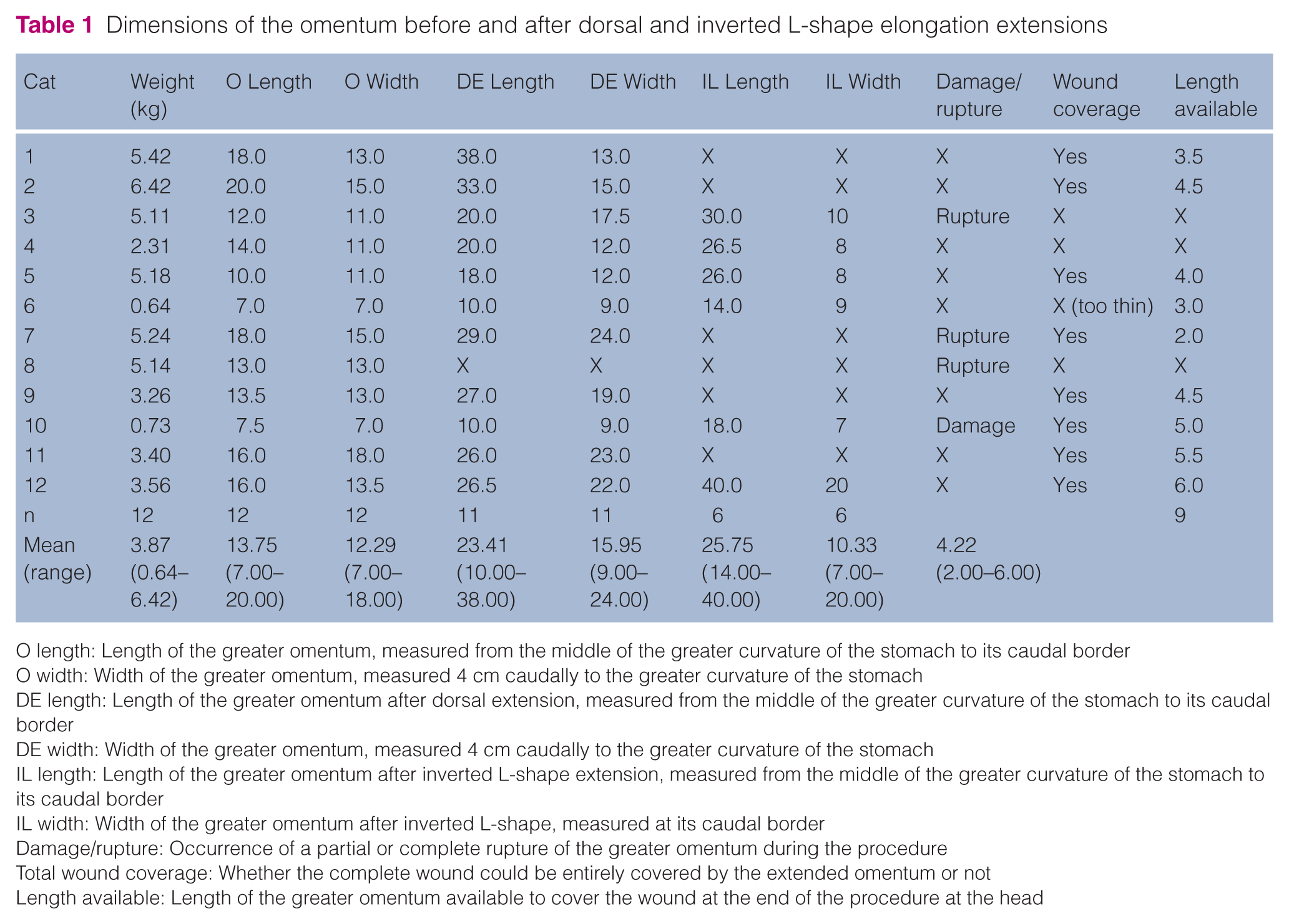
O length: Length of the greater omentum, measured from the middle of the greater curvature of the stomach to its caudal border
O width: Width of the greater omentum, measured 4 cm caudally to the greater curvature of the stomach
DE length: Length of the greater omentum after dorsal extension, measured from the middle of the greater curvature of the stomach to its caudal border
DE width: Width of the greater omentum, measured 4 cm caudally to the greater curvature of the stomach
IL length: Length of the greater omentum after inverted L-shape extension, measured from the middle of the greater curvature of the stomach to its caudal border
IL width: Width of the greater omentum after inverted L-shape, measured at its caudal border
Damage/rupture: Occurrence of a partial or complete rupture of the greater omentum during the procedure
Total wound coverage: Whether the complete wound could be entirely covered by the extended omentum or not
Length available: Length of the greater omentum available to cover the wound at the end of the procedure at the head
To the best of our knowledge, this is the first study describing omental transposition through a subcutaneous tunnel to the head in cats. Ross and Pardo stated that the omentum can be extended to any part of the body, but their study used a canine model. 12 Valat et al indicated that there are no contraindications for the use of the omentum. 13 Our results show that a dorsal extension was fundamental in all cases, except for cat 8, as the omentum had already ruptured while performing a dorsal extension. An inverted L-shaped elongation effectively lengthened the omental flap in six cases, but adequate wound coverage only occurred in three cases. One problem encountered throughout the entire study was the placement of the silicon tube. Tube placement was fairly invasive because the silicon tube used was soft and required significant effort to be placed. A stiffer tube might have eased the process. Based on the data obtained in this study, it is also uncertain whether the 2–6 cm long omental tissue at the recipient site is sufficient for wound healing 14 . This study has a few limitations. As it is based on cadavers, it provides no information regarding vascular survival of the omentum initiating from the exit hole, through the subcutaneous tunnel and exiting at the head. The effect of this manipulation in relation to drainage quality, blood supply, omental twisting, tissue viability and healing progress could not be investigated15,16. It is also likely that the elasticity of frozen-thawed cadaver tissue does not exactly mimic the elasticity of live tissue.
In conclusion, regardless of the number of successful omental transpositions in live patients, our study outlines that the omentum cannot reach a wound located at the head surface without dorsal elongation and, in many cases, without the use of an inverted L-shaped extension. Unfortunately, these procedures may jeopardise the effectiveness and integrity of the omentalisation. Our results suggest that without further experimental studies, omentalisation cannot be safely applied to the head in cats.
Footnotes
Acknowledgements
It is a pleasure to thank Dr Tamara Grubb from Washington State University for her technical assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.