
Abstract
Pancreatic trauma and rupture are rare after feline high-rise syndrome; however, should it happen, pancreatic enzymes will leak into the abdominal cavity and may cause pancreatic autodigestion and fatty tissue saponification. If not diagnosed and treated, it can ultimately lead to multiorgan failure and death. In this case series, 700 records of high-rise syndrome cats that presented between April 2001 and May 2006 were analysed, and four cats with pancreatic rupture were identified. Clinical signs, diagnosis using ultrasonography and lipase activity in blood and abdominal effusion, and treatment modalities are reported. Three cats underwent surgical abdominal exploration, one cat was euthanased. Rupture of the left pancreatic limb was confirmed in all cases. Two of the operated cats survived to date. High-rise syndrome can lead to abdominal trauma, including pancreatic rupture. A prompt diagnosis and surgical treatment should be considered.
Introduction
Feline high-rise syndrome is characterised as a fall from the second floor or higher and was defined by Robinson 1 by a triad of injuries, including epistaxis, hard palate fracture and pneumothorax. Injuries most often described following high-rise syndrome in cats are shock (8–70%), facial trauma (10–64.4%), split hard palate (5–60%) and thoracic injuries, followed by orthopaedic conditions.2–7 In a retrospective study on 112 cats, Barth 7 described a haemoabdomen in 17.7% and haematuria in 40% of patients. Lettow et al 4 documented pancreatic rupture in 10 out of 930 cases of high-rise syndrome cats. Traumatic pancreatitis in cats has also been reported in two case reports.8,9 Pancreatic rupture is followed by leakage and activation of pancreatic enzymes in the abdominal cavity. This leads to pancreatic autodigestion and hydrolysation of fatty tissue ester bonds by lipase. The resulting free fatty acids undergo saponification and bond into insoluble calcium salts which results in severe pancreatitis. 4 The condition is likely to result in multiorgan failure and death if the detrimental pathophysiology cannot be stopped early in the course of the disease. The retrospective study reports four cases of pancreatic trauma in high-rise syndrome cats and the diagnosis in three of them using a comparison of lipase activity in abdominal fluid and blood.
Materials and methods
Medical records of cats that had fallen from at least the second floor and were presented to the Clinic for Surgery, Ophthalmology and Dentistry of the University of Veterinary Medicine in Vienna, Austria, between April 2001 and May 2006, were reviewed. The database was searched for evidence of high-rise syndrome combined with ascites, intra-abdominal haemorrhage or haematoma, pancreatitis and pancreatic rupture and peritonitis. Cats were included if the diagnosis of pancreatic rupture was confirmed during exploratory surgery or post-mortem examination. Data retrieved from case records included signalment, height of fall, clinical signs (including time for development of clinical signs caused by pancreatic trauma), blood chemistry and haematology results, abdominal effusion analysis, ultrasound diagnosis, surgical findings and histopathology or post-mortem results (whichever was applicable).
Results
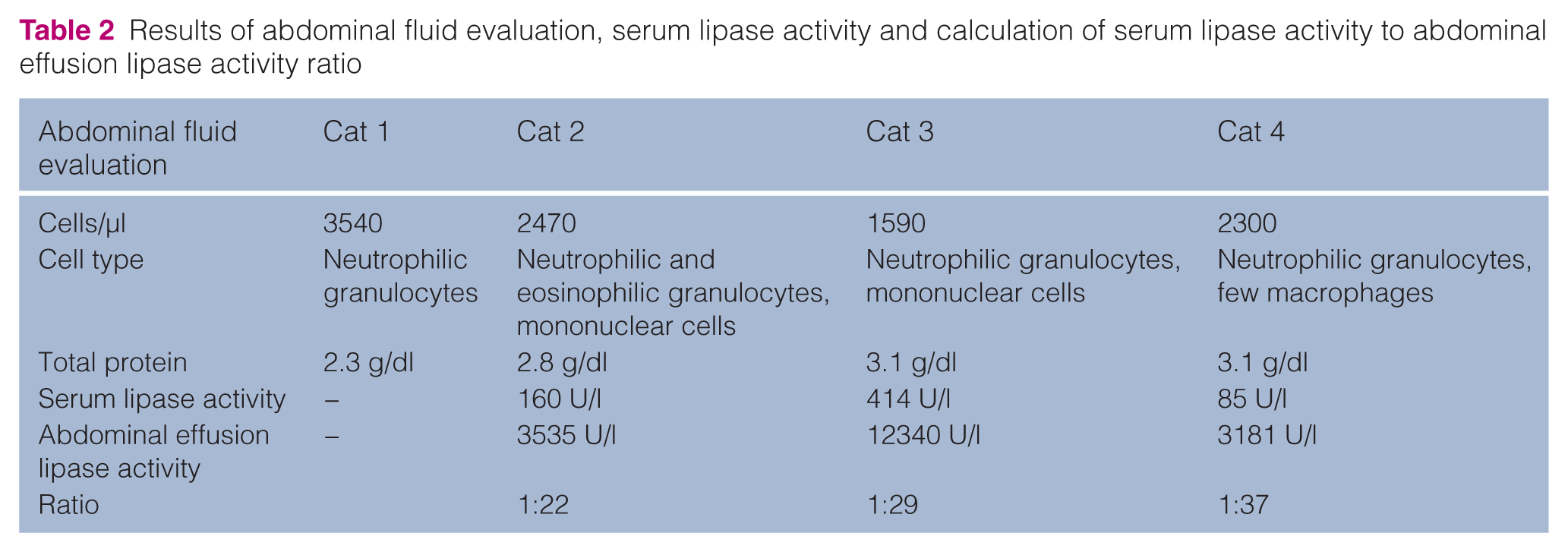
During the study period, 700 cats were presented for high-rise syndrome, four of which with a confirmed pancreatic rupture. Clinical data are presented in Table 1 and the results of the abdominal fluid evaluation are summarised in Table 2.
Clinical, diagnostic imaging and blood biochemistry/haematology data of four cats with pancreatic rupture

ALT = alanine aminotransferase, DSH = domestic shorthair cat, f = female, mn = male neutered.
Results of abdominal fluid evaluation, serum lipase activity and calculation of serum lipase activity to abdominal effusion lipase activity ratio
Cat 1
A 13-year-old, 4 kg male castrated Persian cat was presented after a fall from the seventh floor. Cardiovascular shock was present and was treated accordingly with colloidal and crystalloid fluids. On thoracic and abdominal radiographs, a subcutaneous emphysema overlying the left thoracic wall, fractures of the second and fourth to seventh ribs, lung contusions and reduced peritoneal detail indicative for abdominal effusion were present. A right hind limb lameness and crepitus of the dependent hip was evident, and a coxofemoral luxation was diagnosed. After an initial good response to medical treatment [lactated Ringer’s solution 8 ml/kg/h intravenously (IV), buprenorphine (Buprenovet 0.3 mg/ml; Bayer) 20 µg/kg q12h IV, ampicillin (Standacillin; Sandoz) 20 mg/kg q12h], the cat’s clinical condition deteriorated 2 days after the initial presentation and showed depression, icteric mucous membranes, mild hypothermia (37.7°C), and a distended and painful abdomen. A mass could be palpated in the cranial abdomen. On day 3, the cat became anorexic and vomited yellow and foamy gastric contents. Abdominal ultrasound showed ascites, hypomotility of the gastrointestinal tract and hyperechogenicity of the pancreas and peripancreatic tissue indicative for severe pancreatitis and peripancreatic peritonitis. Blood biochemistry indicated elevated plasma bilirubin of 4.05 mg/dl (range <0.2 mg/dl) and increased activity of alanine aminotransferase (ALT) of 302 U/l (range <50 U/l). Haematology revealed leukopenia of 4430 cells/µl with a left shift (bands 664 cells/µl) and moderate toxic cell changes. The cat was also hypoproteinaemic [5.14 g/dl (range 6–7.5 g/dl)]. Abdominocentesis revealed serosanguineous fluid with a total protein of 2.3 g/dl and 3540 cell/µl consisting mainly of non-degenerated neutrophilic granulocytes. Exploratory laparotomy was declined by the owners and the patient was euthanased for humane reasons. Histopathology showed complete rupture of the left pancreatic limb, severe pancreatitis, omental saponification and patches of necrosis in all intra-abdominal fatty tissues (Figures 1, 2A and B).

Omental saponification on post-mortem examination of cat 1. Note the severe affection of all fatty components of the omentum

Microscopic section of the pancreas of cat 1. (a) Normal pancreatic tissue can be seen (black arrows), as well as interstitial oedema and fibroblasts (star). The open arrow depicts a fine necrotic area on the periphery of the pancreatic lobule, covered by fibrinous effusion. (b) Necrotic peripancreatic adipose tissue with visible calcified areas (blue spots, arrow), the area is demarcated by karyorrhectic leukocytes
Cat 2
Cat 2 was a 4-month-old, female domestic shorthair cat weighing 1.8 kg, that was presented after a fall from the 10th floor. It was dyspnoeic on admission and had bilateral radius and ulna fractures. It showed bilateral bloody nasal discharge and anisocoria. Thoracic radiographs demonstrated increased lung density suggestive of bilateral lung contusions, as well as a mild haemothorax. The cat recovered well on medical treatment [methadone (Heptadon 10 mg; EBEWE Pharma) 0.1 mg/kg IV q6h, cefamandol (Mandokef 500 mg Trockenstechampulle; Eli Lilly) 20 mg/kg q12h, lactated Ringer’s solution during the next day]. On day 2 after admission, a painful cranial abdominal mass and free abdominal fluid were found. Medical treatment was continued for 2 days. Clinical deterioration, including tachycardia (140 bpm) and hypothermia (36.7°C), was present on day 4 when blood chemistry changes inlcuded an elevation of ALT activity (312 U/l) and of serum lipase (160 U/l range <125 U/l). We found severe leukopenia (1400 cells/µl) with no toxic cellular changes, hypoproteinaemia (4.1 g/dl) and anaemia (haematocrit 19%). Abdominal echosonography showed ascites, hypomotility of the gastrointestinal tract and hyperechogenicity of the pancreas and peripancreatic tissue. Free abdominal fluid characteristics were serosanguineous with a total protein of 2.8 g/dl. Total cell count was 2470/µl, and neutrophilic and eosinophilic granulocytes, as well as mononuclear cells were present. In this cat, the level of lipase activity in the free abdominal fluid was determined by colorimetric assay (Lipase, Roche, Hitachi kit 182 17 33, Mannheim, Germany) in a Hitachi 911 and was 3535 U/l. The intra-abdominal lipase activity exceeded the serum lipase activity by a factor of 22, and a preliminary diagnosis of pancreatic rupture was established (Table 2) and aggressive fluid therapy reinstituted. During laparotomy, 20 ml of abdominal fluid was found, as well as separation of the left pancreatic limb. The intra-abdominal fatty tissues were discoloured and hardened, the omentum was clumped. Surgical treatment consisted of partial pancreatectomy of the left pancreatic limb and thorough abdominal lavage with warm sterile electrolyte solution (Table 1). Abdominal drainage was facilitated with a Penrose drain. Recovery from anaesthesia was prolonged and despite further efforts to stabilise the cat, it died within the postoperative period. Histopathology showed acute to subacute reactive pancreatitis, and necrosis and calcification of intra-abdominal fatty tissues.
Cat 3
A 4.3-year-old male castrated cat weighing 4.3 kg was admitted after a fall from the third floor. Cardiovascular shock was treated accordingly. Thoracic radiographs showed a mild pneumothorax and lung contusions. Additional orthopaedic conditions were diagnosed as follows: a left-sided coxofemoral luxation and fracture of the left fourth metatarsal bone. One day after presentation, the cat developed subicteric mucous membranes, a painful and distended abdomen and started to vomit yellow foamy gastric contents. White blood cell count was within normal limits at that stage (9640 cells/µl), ALT activity was 692 U/l, serum lipase activity was 414 U/l (range <125 U/l) and serum bilirubin was 0.27 mg/dl. Abdominal echosonography showed ascites, hypomotility of the entire gastrointestinal tract and hyperechogenicity of the pancreas and peripancreatic tissue. Abdominal fluid analysis showed serosanguineous fluid with a total protein of 3.1 g/dl and 1590 cells/µl. Fluid lipase activity was 12340 U/l, so the calculated ratio of serum to abdominal fluid lipase activity was 1:29. Exploratory laparotomy findings resembled those of cat 1 and 2, and are listed in Table 1. A partial pancreatectomy of the left pancreatic lobe and abdominal lavage were performed, histopathological changes of excised tissue are listed in Table 1. The cat made an uneventful recovery from anaesthesia and surgery. Postoperative regimen included opioid analgesia for 7 days (methadone 0.1 mg/kg IV q8h) and cefamandol 20 mg/kg IV q12h. Starting from the first postoperative day, it was force fed via syringe with a bland diet.
Gastric motility was supported with metoclopramide (Paspertin; Solvay Pharma) 0.2 mg/kg subcutaneously (SC) q8h. The cat started eating normal amounts only after its discharge 2 weeks after surgery. It recovered well and underwent uneventful surgery for femoral head and neck excision 5 weeks after the initial accident.
Cat 4
This cat was a 3-year-old, 3.2 kg neutered, male domestic shorthair cat and was presented with cardiovascular shock, dyspnoea and haemostaxis after it had fallen from the sixth floor. In addition to lung contusions and haemothorax, it had a maxillary symphyseal fracture. Shock was treated accordingly and an oesophagostomy tube was placed under anaesthesia on day 2 to provide ongoing nutrition. The cat developed a painful and distended abdomen and hyperthermia of 40°C on day 5 after admission; at the same time, severe thoracic effusion became evident. Echocardiography confirmed mild enlargement of the right ventricle, with normal myocardial function. The cat showed a non-regenerative neutropenia (2860 cells/µl) with toxic cellular changes, anaemia (haematocrit 21%) and hypoproteinaemia of 4.7 g/dl. Serum bilirubin was 0.98 mg/dl and serum lipase was 85 U/l. Tests for feline leukaemia virus (FeLV) and feline immunodeficiency virus (FIV) were negative; a titre of 1:100 was present for feline coronavirus (FeCoV). Abdominal fluid was turbid and yellow, with a total protein of 3.1 g/dl. There were 2300 cells/µl, predominantly consisting of neutrophils and macrophages, both with mild signs of toxicity. Fluid lipase activity was 3181 U/l, resulting in a ratio of 1:37 with serum lipase activity. Based on those findings and serum testing, clinical manifestation of feline infectious peritonitis could not be ruled out at this stage. Abdominal ultrasound revealed the signs of severe peritonitis and pancreatitis (Figure 3). Although the prognosis was guarded, the cat underwent exploratory laparotomy after evacuation of serosanguineous fluid from the thorax by needle thoracocentesis. Surgical findings were consistent with a complete rupture of the left pancreatic limb. The mesentery and omentum were severely necrotic and clumped (Table 1, Figure 4). Splenectomy was performed in addition to partial pancreatectomy in order to excise most of the necrotic fatty tissue. The abdomen was lavaged with warm saline solution and routinely closed. Postoperative medication consisted of cephalexin (Cefazolin Sandoz 1 g; Sandoz), 20 mg/kg IV q8h, metronidazole (Metronidazolm 500 mg; Sandoz) 10 mg/kg IV q12h and buprenorphine 20 µg/kg IV q8h for 9 days. It recovered well from anaesthesia, as well as from surgery, and did not redevelop thoracic effusion. The cat was fed via oesophagostomy tube until discharge. A re-check echocardiogram showed moderate and mild enlargement of the right and left atrium, respectively, and mild enlargement of the right ventricle. The cat was discharged from the hospital 8 days after surgery and is clinically normal to date.

Abdominal ultrasound of cat 4. Pancreatic (P) and peripancreatic hyperechogenicity (arrows) are visible

Intra-operative view of cat 4 after midline coeliotomy: severe fatty tissue necrosis and saponification can be seen in the greater omentum adjacent to the spleen
Discussion
Abdominal injuries secondary to blunt trauma owing to high-rise syndrome are reported at a rate of 0.3–17.7% and are most often characterised by intra-abdominal haemorrhage.2–4,6,7 Lettow et al 4 compared various affected organs and found pancreatic ruptures at a rate as high as 1% of all high-rise syndrome cats (10/930 cats). This study found pancreatic rupture in 0.6% of cats with high-rise syndrome. The early clinical signs of pancreatic injury are reported to be highly unspecific, thus difficulty in diagnosing the condition may have led to a failure to identify it more frequently. Height seems to be an important factor for the presence of pancreatic rupture. The cats in our study fell from the third, sixth, seventh and 10th floors. Similarly, prevalence of pancreatitis was higher after falls from greater heights and the mean height was 4.9 stories (range 3–8) in reported cases.4,8,9 Initial clinical changes of the cats in this study were vague and consisted of anorexia, abdominal pain and vomiting. Abdominal effusion, a painful cranial abdominal mass and icterus was noted in all cats within 1–7 days after fall. One study 10 reports anorexia in 100%, lethargy in 97% and dehydration in 92% of cats with acute necrotising pancreatitis from various causes. Vomiting and abdominal pain developed less reliably in cats compared to dogs. While only two out of four cats described here were vomiting, all developed abdominal pain. The higher incidence may be related to the blunt abdominal trauma they sustained in contrast to the cats in the previously mentioned study. 10
Icterus is most likely caused by pancreatic oedema obstructing the common bile duct at the shared opening of the latter with the pancreatic duct of Wirsung into the duodenum at the major duodenal papilla. 11 Intra-operative findings were dominated by pancreatic and peripancreatic necrosis and calcification, and involved all fatty intra-abdominal tissues. Treatment, therefore, focused on excision of the diseased areas. In the three cats, gall bladder emptying was normal. Surgical treatment using a stent 12 or temporary or permanent biliary diversion13,14 could be indicated in more severe cases.
Three cats developed significant leukopenia and hypoproteinaemia. This often reflects a severe inflammatory response in cats and is a negative prognostic indicator, as ongoing losses exceed the body’s demand, 15 that cannot be adequately met by regeneration. The finding should alert the attending clinician to a thorough search for the underlying cause thus shortening the time to diagnosis and treatment.
Cat 2 showed signs of systemic inflammatory response syndrome (SIRS), 16 clinically reflected by a tachycardia of 140 bpm, hypothermia and leukopenia, even before surgery. Severe peritonitis secondary to pancreatic rupture seemingly aggravated the condition during the 2 days between first clinical signs attributable to pancreatic rupture (abdominal mass) and surgery, and ultimately lead to multiple organ dysfunction syndrome (MODS) and death despite aggressive supportive and surgical treatment. SIRS developed in the euthanased patient (cat 1), even before a preliminary diagnosis of pancreatic rupture was established. A tool for early diagnosis of the underlying pathology would, therefore, be extremely important to prevent further deterioration and death of affected patients.
As pancreatic rupture results in severe pancreatitis and peripancreatitis, it seems logical that the condition should be picked up by tests for pancreatitis. Unfortunately, feline pancreatitis poses a diagnostic challenge to the clinician. Forman et al 17 compared different methods for the diagnosis of pancreatitis in cats and found ultrasonography combined with a serum test for feline pancreatic lipase immunoreactivity (fPLI) to have the highest sensitivity and specificity. However, fPLI is not routinely available as an in-house test. The process of shipping and analysis can prove too long in a critically ill patient. While the sensitivity of ultrasound for the diagnosis of severe or moderate pancreatitis in one study 17 was 80%, it only ranged between 20% and 35% in previous studies.18,19 A report evaluating endosonography with transabdominal ultrasound, 20 found better visualisation of the normal pancreas and better resolution with this method in all sick patients. However, the findings did not alter the diagnosis of transabdominal ultrasound in the six diseased cats of the study. Ultrasonography alone, therefore, should not be relied on for the decision for treatment, rather a combination of findings should be taken into account. Feline TLI and computed tomography (CT) did not prove useful. 17 This was confirmed in a study by Gerhardt et al. 19
Guija de Arespacochaga et al 21 compared ascitic fluid of dogs with acute pancreatitis, abdominal trauma without clinical or ultrasonograhic signs of pancreatitis and abdominal neoplasia and other reasons, and found significantly higher abdominal fluid lipase activity in dogs with acute pancreatitis. Testing for abdominal fluid lipase activity in three cats in our study showed a 22-, 29- and 37-fold elevation compared with serum values. Preliminary results of a comparison of ascitic fluid lipase activity show that cats with pancreatic trauma and rupture had significantly elevated lipase activity compared to ascites from other reasons. 22 These findings indicate that measurement of lipase activity in peritoneal fluid may be useful in the diagnosis of pancreatic rupture in cats with abdominal trauma — further evaluation is warranted.
Lettow et al 4 described radiographic signs of calcification in the pancreatic region in cats with pancreatic saponification and calcification caused by pancreatic rupture. This could not be confirmed in our cases, although calcification of intra-abdominal fat was detected on histopathology of the affected omentum (Figure 1).
In two cats, postoperative drainage of intra-abdominal fluid was provided by the use of Penrose drains. Penrose drains are subject to occlusion with fibrin and omentum; however, in the one cat still alive at the time of drain removal, it was draining fluid out of the abdomen for a period of 5 days when fluid production diminished. Omentectomy performed as a part of surgical treatment as a measure of treatment of the disease may have contributed to the functionality of the drainage system.
Conclusion
In conclusion, a high degree of suspicion was necessary to diagnose the condition early. The combination of clinical signs, diagnostic imaging and a high ratio of serum to intra-abdominal lipase activity led to the tentative diagnosis of pancreatic rupture. However, more cases may have been missed and a prospective study is warranted to truly evaluate the incidence of pancreatic trauma after feline high-rise syndrome. Of the three cats that underwent surgical treatment, two survived and recovered completely. The condition should be considered as a differential diagnosis after severe abdominal trauma that needs to be treated as soon as possible, especially after a fall from a great height.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.