
Abstract
A 4-month-old domestic shorthair female cat weighing 1.3 kg was presented for evaluation of respiratory distress. The animal showed evident dyspnoea with exercise intolerance and a marked concave deformation of the sternum. After measurements of the fronto-sagittal and vertebral indexes, the pectus was classified as moderate and surgery was elected. Surgical correction was performed using an open approach to the sternum with osteotomy of the last sternebra and costochondral junctions of the eighth and ninth ribs bilaterally. A silicone based, U-shape external splint was manufactured and used to stabilise the sternum. Immediate and 5-week postsurgical radiographs revealed a decreased concavity of the sternum and an increase thoracic height at the level of the last sternebra. Postoperative results suggest that this technique could be an effective and economical option for cats with pectus excavatum with a non-compliant sternum.
Case Report
Pectus excavatum (PE) is a rare congenital deformity of the chest wall. It is characterised by a concave deformity of the caudal sternum associated with costal cartilage deformity and consecutive narrowing of the entire thorax.1,2 This defect has been reported in both dogs and cats, being diagnosed just after birth. 1 The cause of PE is not well understood. There is a genetic predisposition, as more than one littermate is affected, but there are no sex or breed predispositions.2–4 Possible causes include excessive growth of the connective tissue and cartilage of the costo-chondral region, which secondarily causes the inward defect of the sternum.
PE can significantly compromise cardiac and pulmonary function. Pulmonary effects are associated with restrictive lung disease secondary to decreased intrathoracic capacity or lung atelectasis by cardiac compression. Cardiac effects result directly from the decreased cardiac output or the presence of other concomitant congenital cardiac abnormalities. The main clinical signs are respiratory distress, exercise intolerance, tachypnoea and cyanosis related with the severity of the disease. However, other clinical cardiorespiratory signs can be associated with secondary or concomitant congenital diseases. 4
Diagnosis is based on clinical and radiographic examination, with identification of the sternum deformity and decreased caudal thoracic space. 1
The present case report describes a successful correction of a PE in a non-compliant sternum, with the use of an open surgical approach associated with a polypropylene and silicone based external splint.
A 4-month-old domestic shorthair intact female cat weighing 1.3 kg was evaluated at the Faculdade de Medicina Veterinária-Universidade Lusofona de Humanidades e Tecnologias. The animal was referred with a history of respiratory distress, exercise intolerance and occasional emesis. On clinical examination, a delayed growth and obvious signs of dyspnoea and tachypnoea were observed. The caudal sternum was displaced dorsally. Upper respiratory signs of rhinitis and conjunctivitis exacerbated the respiratory signs and exercise intolerance. Thoracic auscultation showed upper respiratory turbulence and increased vesicular murmur. Routine blood work revealed mild leukocytosis, and search for feline immunodeficiency virus (FIV) antibody and feline leukaemia virus (FeLV) antigen were negative.
Radiographic examination showed dorsal elevation from the fifth to the last sternebra, a shortened diaphragm line and dorsal displacement of the cardiac silhouette. Fronto-sagittal index (FSI) and vertebral index (VI) were calculated as previously described. 5 The FSI value was 2.21 [reference interval (RI) 0.7–1.3] and VI value was 6.94 (RI 12.6–18.8). Concomitant cardiac alterations and diaphragm abnormalities were ruled out by echocardiography.
As the respiratory signs of PE could be aggravated by a potential upper respiratory tract infection, amoxicillin-clavulanic acid (Synulox; Pfizer, 12.5 mg/kg, q12h) was prescribed for 2 weeks, as well as meloxicam (Metacam; Boehringer Ingelheim, 0.2 mg/kg, q24h) for 5 days. After 15 days, clinical signs were improving, but respiratory distress was still present. Surgery was scheduled 8 days later, while a concave external splint was manufactured. The material used consisted of a commercial polypropylene mesh which was sectioned in three basic pieces (two laterals and one ventral), connected by silicone used for dental prosthesis (Silicone Denture Soft Liner, Versa-Soft) (Figure 1). A fourth rectangular component of polypropylene mesh was used to support the splint dorsally, tied by four strips. The splint was then sterilised.
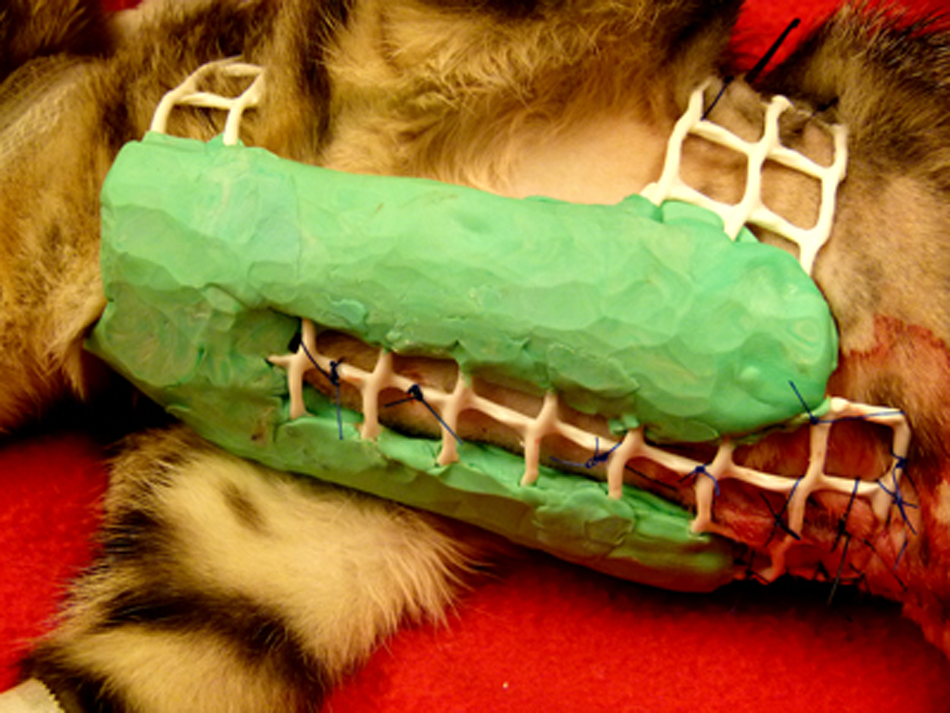
Polypropylene and silicone based thoracic splint
The animal was anaesthetised using a combined protocol of dexmedetomidine (Dexdomitor; Esteve, 0.05 mg/kg) associated with ketamine (Clorketam; Vetoquinol, 5.5 mg/kg) and morphine (Morfina 1%; Braun, 0.5 mg/kg). Maintenance was assured with isoflurane (Isoflo; Esteve) and mechanical ventilation. Perioperative amoxicillin-clavulanic acid (Synulox; Pfizer, 15 mg/kg) and meloxicam (Metacam; Boehringer Ingelheim, 0.02 mg/kg) was also administered.
A ventral midline incision was performed extending from the fifth sternebra to the umbilical scar. Soft tissues were dissected down to the sternebrae and costo- chondral junctions. The abnormal portion of the sternum was separated from the rest of the thoracic cage through partial sternotomy and sterno-costochondroplasty on the last three sternebrae and corresponding costo-chondral junctions. Blood flow from the internal thoracic artery, intercostal and sternal branches was preserved to avoid ischaemic necrosis of the dissected piece of the thoracic cage. Multiple stay and traction sutures [non-absorbable 3-0 suture material (Dafilon; Braun)] were applied in different directions around the sternum and the eighth and ninth ribs, passing through the skin and subcutaneous tissues. The sutures were then secured to the previously sterilised external splint pulling the sternum and ribs outward. A thoracostomy tube was temporary placed to prevent postoperative pneumothorax and was removed 6 h after surgery. The diaphragmatic incision was sutured with a simple continuous pattern of 3-0 glyconate (Monosyn; Braun). The same material was used for routine closure of the soft tissues and skin. A chest radiograph was performed immediately after surgery and 5 weeks postoperatively. The splint was maintained in place for a period of 5 weeks (Figure 2).

(a) Lateral thoracic radiographs at the time of diagnosis and (b) 5 weeks postoperatively
Postoperative follow-up consisted of weekly clinical evaluation. There were no splint associated complications. The splint was adapted on two occasions by lengthening of the strips. The animal showed a progressive increased exercise tolerance and decreased tachypnoea, an increased appetite and a more active attitude. The FSI value was 1.3 and VI value was 13.7 at 150 days after surgery .
Different surgical approaches have been described in the literature to correct PE. The placement of percutaneous circumcostal sutures and an external splint are indicated for very young animals (less than 4 months old), with a non-ossified and compliant sternum.2,6 The goal of this technique is to pull the sternum outward, keeping it in that position until ossification and bone maturation occurs.2,7–9 In the present case report, the sternum was already ossified and non-compliant, whereas the literature discourages the use of percutanous sutures on the sternum.6,10,11 There are only three reported cases of ossified PE in cats.12–14 One case consisted of a sternal deformed segment which was removed along with the associated cartilages; 12 another report described the realignment of the sternum with surgical reconstruction using a combined internal fixation and external splint; 13 and the last one consisted of an internal fixation with plate and screws. 14
PE surgery has three main objectives: (1) soft tissue mobilisation; (2) sternal concavity correction; and (3) stabilisation of the anterior thoracic wall.15,16 In the present clinical case, there are several factors to consider. One of these factors was economical restriction. The use of an external splint was the most economical option; however, it was not indicated for an animal with an ossified sternum because it would not be sufficient to keep the sternum in place unless there was sternum and rib remodelling. Additionally, splint associated complications have been described, for example, skin dermatitis and suture reaction, with prolonged splint maintenance. 17
The use of an internal fixation was less economical and has an increased failure risk owing to inadvertent vessel laceration and ischaemic lesions secondary to the application of an internal fixation system in a very small skeleton.
Taking all of this together lead us to considerer that the best option for this case was open sternal remodelling associated to an external splint. A partial sternotomy associated with a sterno-costochondroplasty allowed sternum remodelling and the insertion of multiple traction sutures in different directions, avoiding the main blood vessels. The fixation of the ribs and sternum was adapted from Fossum, 2 where six transverse sutures around the sternum were applied in a blind manoeuvre. In the present case, different traction sutures in different directions allowed the remodelling of the ossified chest and downward pulling of the costo-chondral junctions and ribs with an better tension distribution. Together with the reticulated structure of the splint, the use of the traction sutures helped to reinforce and stabilise the chest cage and keep the sternum in place for 5 weeks during the healing process.
A hand-made rigid splint was designed with the following objectives: to have sufficient rigidity; to be lightweight; to be slowly reactive; to have a reduced cutaneous contact surface; to be well tolerated; and to be adapted to continuous and rapid growth of the animal. Additionally, it should be of accessible material, inexpensive, easily manufactured and allow for sterilisation.
The successful management of this case suggests that placement of traction sutures allowed better tension distribution of sutures and, at the same time, increased the rigidity of the immobilisation with a minimum of contact surface. Also, the silicone/polypropylene base splint for the management of PE could be a good option for compliant and non-compliant sternum. For the non-compliant sternum, an open surgical approach and sternum remodelling should be considered.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.