
Abstract
Bereavement is a significant social stressor associated with heightened mortality risk. To date, the role of social health in this relationship remains unclear. This systematic scoping review synthesizes the literature examining the association between social health and mortality risk among bereaved individuals.
A comprehensive literature search was performed in the following databases from inception—July 2024: Ovid MEDLINE, Ovid EMBASE, CINAHL, AgeLine, PsycINFO, Web of Science, and Scopus. The study was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) methodological framework.
A total of 23 studies with significant heterogeneity in measurement methods and contexts met the criteria for inclusion in this review. Overall, the literature suggests the social health of bereaved individuals is associated with both increased and decreased mortality risk; often dependent on social contexts and/or based on certain factors (e.g., sex, time since death). Higher and consistent levels of perceived social support were associated with reduced mortality risk. Declining support trajectories and perceived isolation were linked to increased risk. Remarriage and diverse network connections (e.g., family and nonfamily support) were protective, but this association varied by gender and cause of death. Limited sampling of non-Western populations, inconsistent use of validated tools, and a focus on spousal bereavement represent limitations of research conducted to date.
Results suggest that bereavement-related mortality risk associated with social structural factors (e.g., remarriage) may be promising avenues of future research. Future research should explore mechanisms of these associations and expand to diverse populations and bereavement types to advance understanding of the role of social health in bereavement-related mortality risk.
Introduction
Research has established a link between bereavement and an increased risk of death.1–5 Biopsychosocial health models posit that, in addition to biological factors, psychological, and social factors are critical to understanding health and mortality risk. 6 While bereavement research has examined relationships between physical health,7–11 mental health,10,12 and the risk of death of bereaved survivors, the role of social health remains unclear.
Strong social support systems can buffer against the adverse effects of a stressful life event 13 such as bereavement. 14 Social relationships have demonstrated a comparable influence to well-established mortality risk factors, such as smoking and alcohol use, and have exceeded the influence of other known risk factors, such as physical activity. 15 However, other studies show no indication of this buffering effect.16,17 To date, no systematic reviews examine the relationship between social health and mortality risk following bereavement and the associated mechanisms of action.
Social health—an individual’s overall sense of well-being stemming from feelings of connection with others and ties to a larger interpersonal community 18 —appears to be a casualty of bereavement. 19 As such, it may influence the health and survival of bereaved survivors. The conceptualization of bereavement as a social event—the loss of a significant or close other—is a key element of our microsociological theory of adjustment to loss. 19 The theory suggests that bereavement creates social voids and deprivations that undermine social, mental, and physical health. Deprivations can arise from multiple factors. For example, bereaved people not only lose the relationship with the deceased but may also lose confidence in navigating their remaining social connections and activities. 20 Furthermore, responses of one’s social network to the death may prove unsupportive, unwelcome, absent, or even hurtful, creating a disconnect between the bereaved individual and those they may have otherwise called upon for support. 21 These social health voids and deprivations together may be implicated in the mortality risk posed by bereavement and underscore why a comprehensive understanding of bereavement-related mortality risk must attend to associated social health impacts.
We hypothesize here that social health is adversely affected by bereavement—a fundamentally social event that creates social voids. 19 How these voids are filled likely influences a mourner’s social health. In this framework, social health can be operationalized as feelings of belonging, support, and nurturance, and a clear sense of one’s roles within their social network. However, within the broader literature, significant heterogeneity in social health measurement exists.22,23 Thus, social health indicators are often categorized as structural or functional aspects. Structural aspects capture the existence of relationships, such as the network size,22,23 whereas functional aspects focus on relationship qualities and functions, such as perceived support.22,23
This systematic scoping review aims to synthesize the existing literature examining the relationship between social health and mortality in bereavement. Additionally, we aim to identify which aspects of social health are most relevant and impactful to identify targets for future interventions. The review protocol was registered prospectively with the PROspective REgister of Systematic Protocols and Reviews (PROSPERO; CRD42024559217).
Methods
The review was performed following the Preferred Reporting Items for Systematic reviews and Meta-Analyses for Scoping Reviews (PRISMA-ScR) framework. 24
Search strategy
Searches were run on 07/08/2024 in the following databases: Ovid MEDLINE (ALL-1946 to Present); Ovid EMBASE (1974 to present); CINAHL (EBSCO); AgeLine (EBSCO); PsycINFO (EBSCO); Web of Science–Core Collection (Clarivate); and Scopus (Elsevier). Search strategy included all appropriate controlled vocabulary and keywords for the concepts of “social health,” “mortality,” and “bereavement” (See Supplementary Data S1). Social health search terms were informed by the aforementioned definitions.22,23
Study selection
Covidence systematic review software was used for initial title/abstract and full-text screening. Each screening phase was completed by at least two trained independent reviewers (M.H., H.W., and S.K.) using predefined inclusion/exclusion criteria. Discrepancies were resolved by consensus.
Studies were required to examine mortality risk as an outcome and social factors associated with mortality risk following bereavement. Only full-length, peer-reviewed journal articles were included. Studies were excluded if bereavement was not the focus or clearly measured or analyses did not examine the relationship between social health and mortality.
We completed a reference chasing search following the initial identification of eligible studies to bolster the identification process rigor. With medical librarian support (see Acknowledgments), any study citing eligible studies was retrieved and underwent the full screening process.
Data extraction
Data were extracted from all eligible studies. To minimize error and improve data reliability and quality, extraction was completed in duplicate using Covidence. Two independent reviewers (H.W. and S.K.) charted the data using predefined, standardized templates (See Supplementary Data S1). M.H. resolved discrepancies.
Results
Overall, 2533 records were identified via database (n = 2186) and reference (n = 347) searches. After duplicate removal, 1539 records underwent screening. Seventy-one studies were identified for full-text review. Twenty-three met inclusion criteria. See Figure 1 for process details.
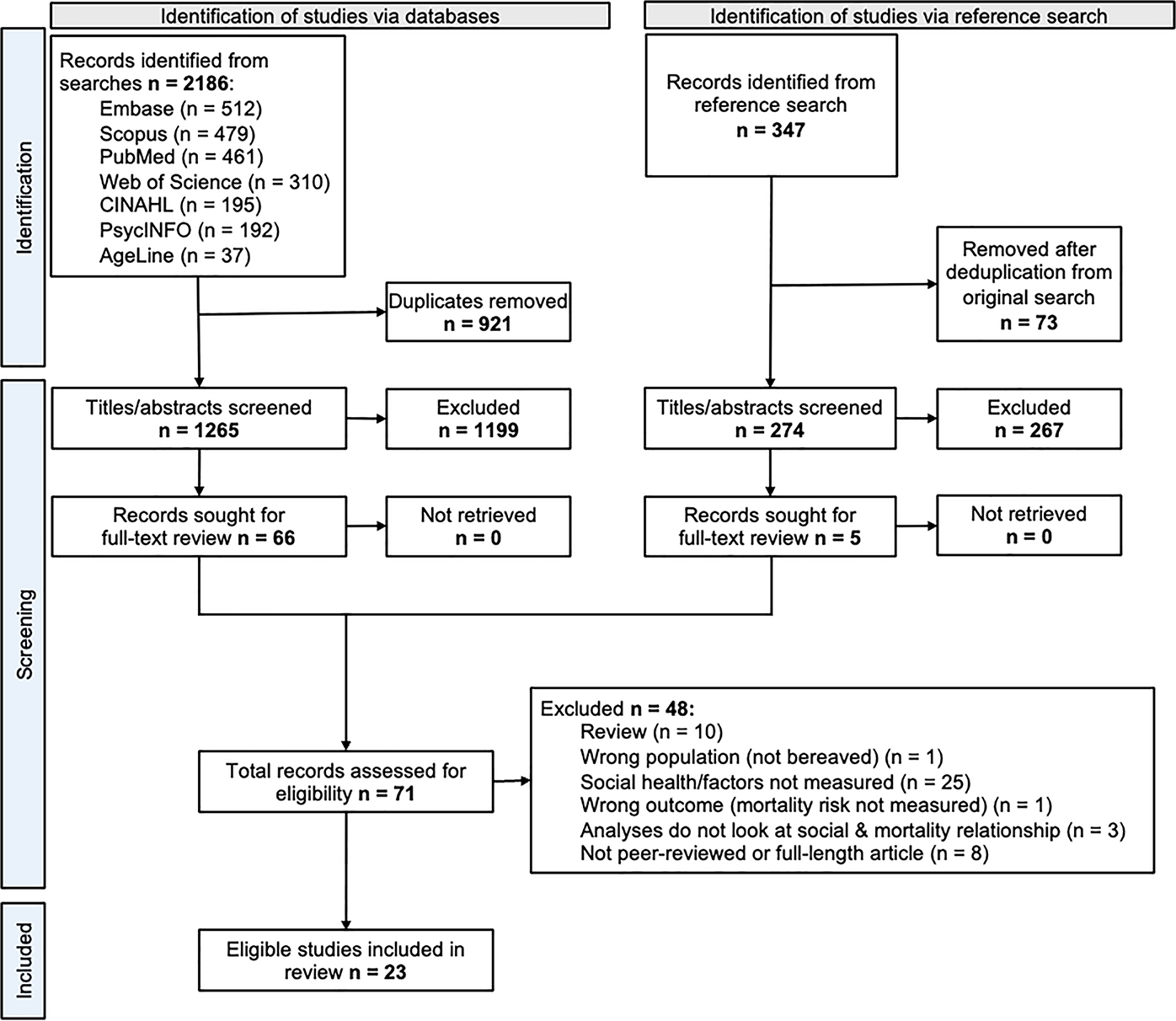
PRISMA flowchart outlining identification and screening of studies that examined associations between social health and mortality in bereaved people.
Characteristics
Table 1 summarizes study characteristics. The 23 included papers reported results from 23 different studies. Two studies25,26 used data from the same database (i.e., Utah Population Database); however, one 26 used a derived cohort (i.e., Caregiving Population Sciences study), and the studies’ focuses differed considerably (i.e., examining bereaved caregivers 26 vs. comparing polygamous and monogamous groups 13 ).
Characteristics of Included Studies
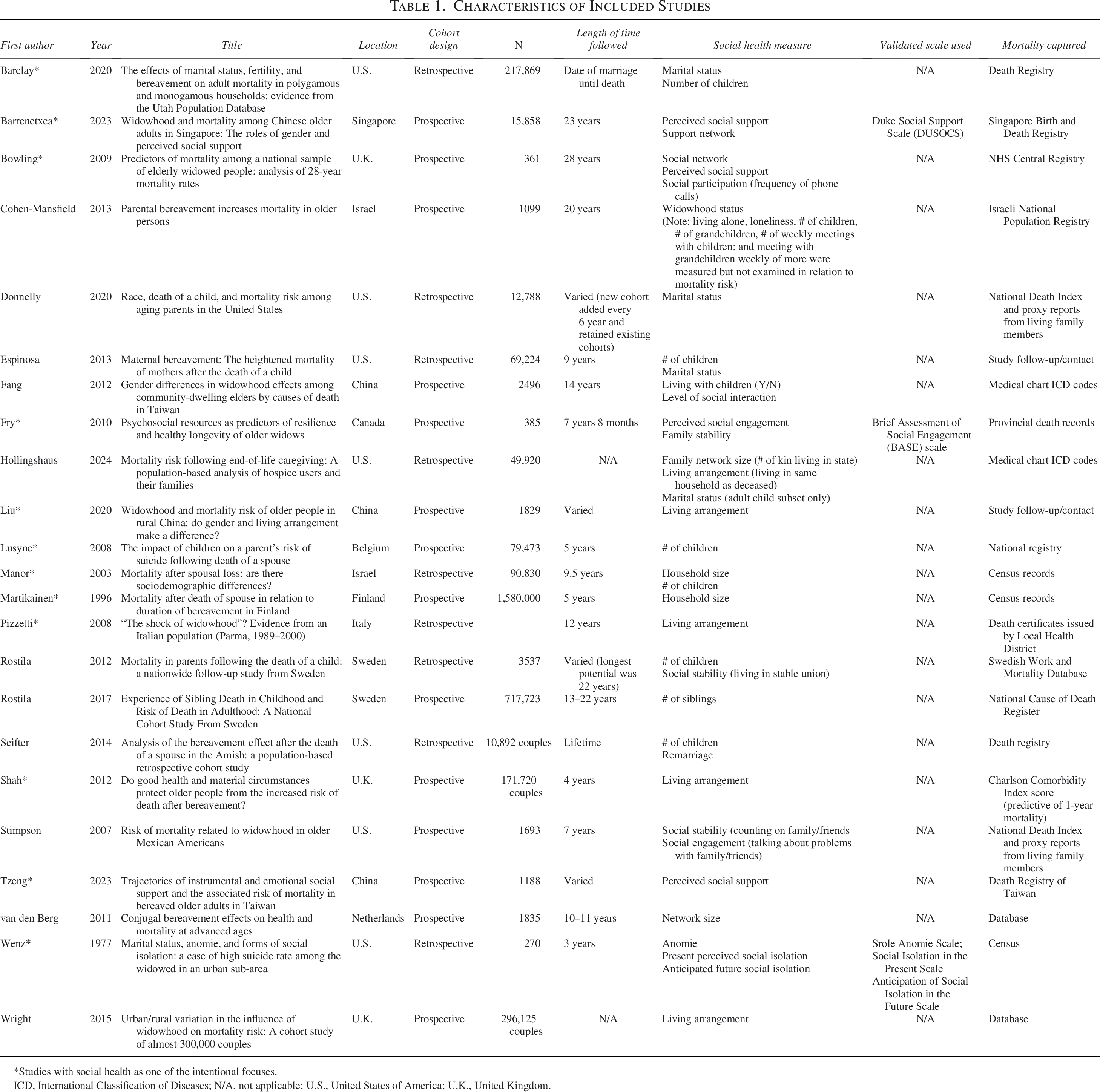
Studies with social health as one of the intentional focuses.
ICD, International Classification of Diseases; N/A, not applicable; U.S., United States of America; U.K., United Kingdom.
Sociodemographic characteristics were inconsistently reported between studies (See Table 2). Over half (n = 12, 52.2%) of the studies did not report participants’ average age. All but three studies reported sex/gender frequencies. However, only 15 studies reported sex/gender statistics for the bereaved participants separately from non-bereaved. Only seven studies reported race/ethnicity.
Characteristics of Bereaved Sample Within Included Studies
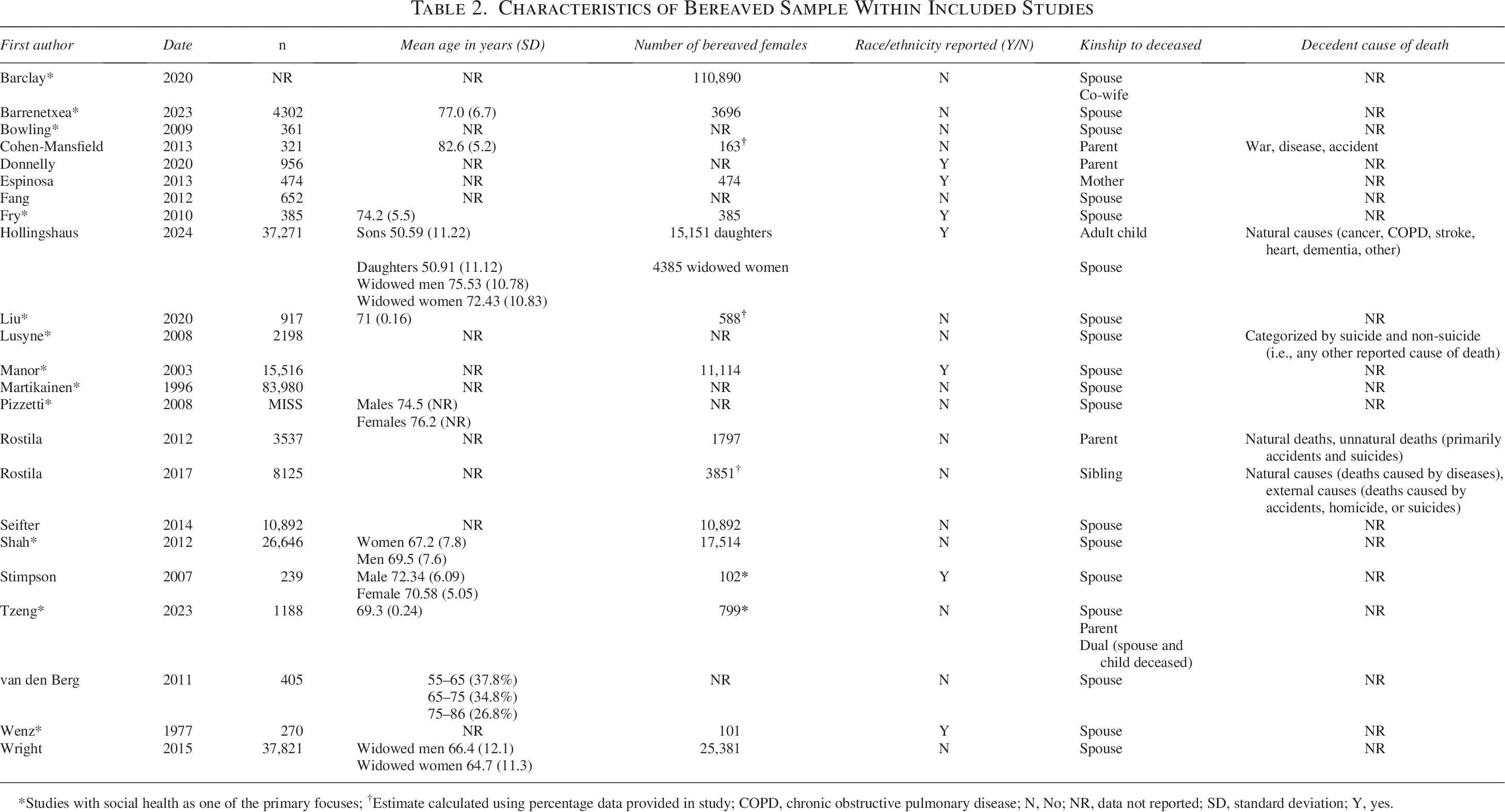
Studies with social health as one of the primary focuses; †Estimate calculated using percentage data provided in study; COPD, chronic obstructive pulmonary disease; N, No; NR, data not reported; SD, standard deviation; Y, yes.
Regarding bereavement and death-related characteristics (see Table 2), most studies focused on spousal bereavement (n = 15, 65.2%)4,27–40 and did not report decedents’ cause of death (n = 18, 82.6%).
The role of social health on mortality following bereavement was a primary focus in 11 studies (asterisked in Table 1). The remaining 12 studies included social health measures within their analyses but did not center their investigations on it.
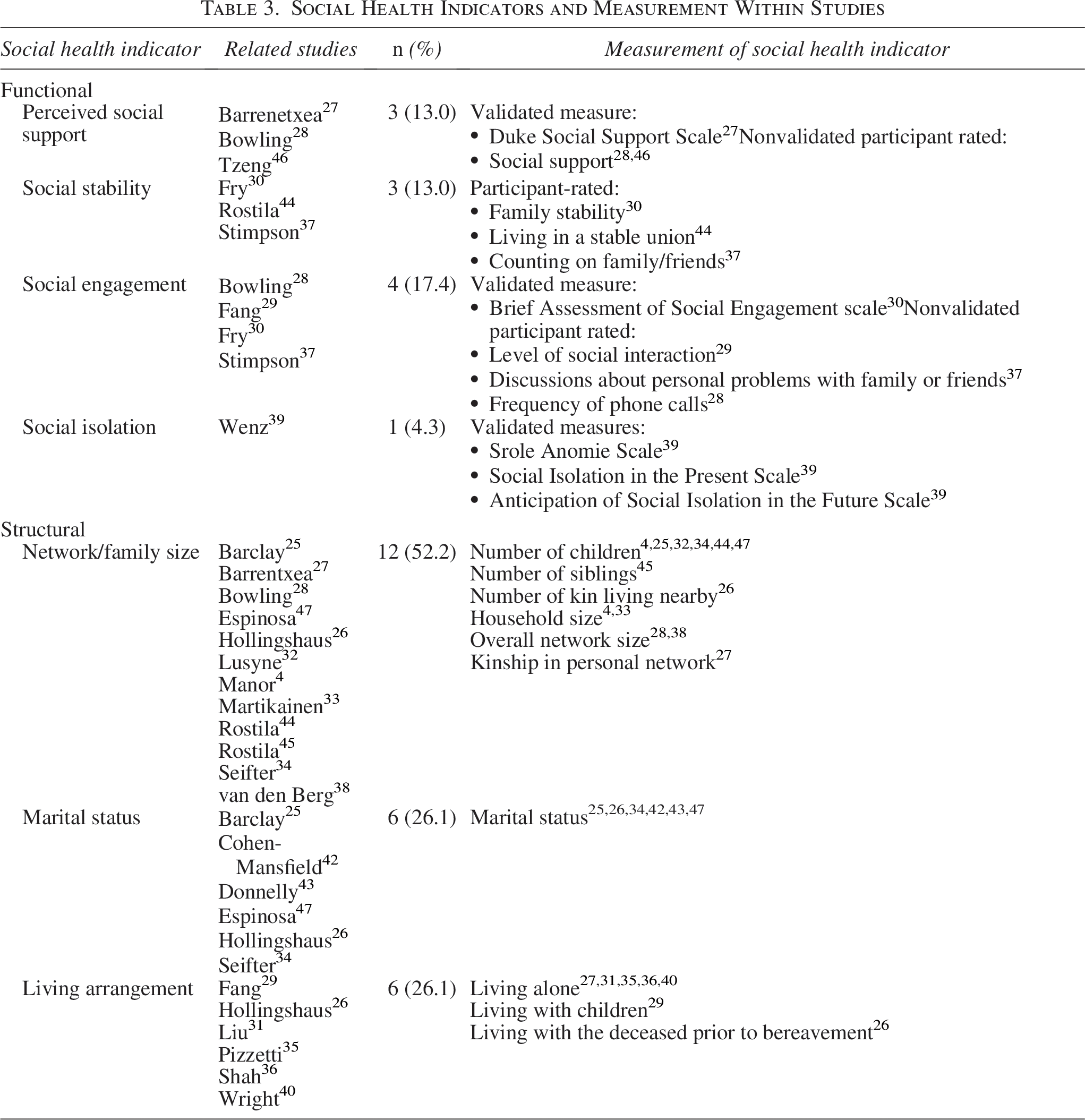
Eleven studies reported a single social health indicator in their mortality risk-related results. Remaining studies had two (n = 9, 39.1%) to three (n = 3,13.0%) indicators. Structural indicators (i.e., network or family size, marital status, living arrangement) were used more frequently than functional indicators (i.e., perceived social support [PSS], social stability, social engagement, perceived social isolation). See Table 3 for indicator descriptives. Network or family size (n = 12, 52.2%) was the most frequently used structural indicator. Social engagement (n = 4, 17.4%) was the most used functional indicator. Only three studies used validated social health measures. Moreover, among the five validated measures employed, no two studies used the same one.27,30,39
Social Health Indicators and Measurement Within Studies
For mortality risk measurement, most studies (n = 16, 69.6%) relied on death registries/records. Other studies used medical chart codes (n = 2, 8.7%), study follow-up/proxy contact (n = 3,13.0%), a combination of national death index and proxy reports (n = 2, 8.7%), and the Charlson Comorbidity Index score as a proxy predictive of 1-year mortality (n = 1, 4.3%).
Quality assessment
The Newcastle-Ottawa Scale was used for quality assessment. 41 Most studies (n = 17; 73.9%) were judged as good quality.4,25,28,29,31–33,35–37,40,42–46 Three (13.0%) were fair26,27,34 and three (13.0%) were poor.30,39,47 See Supplementary Data S1 for additional data.
Key findings
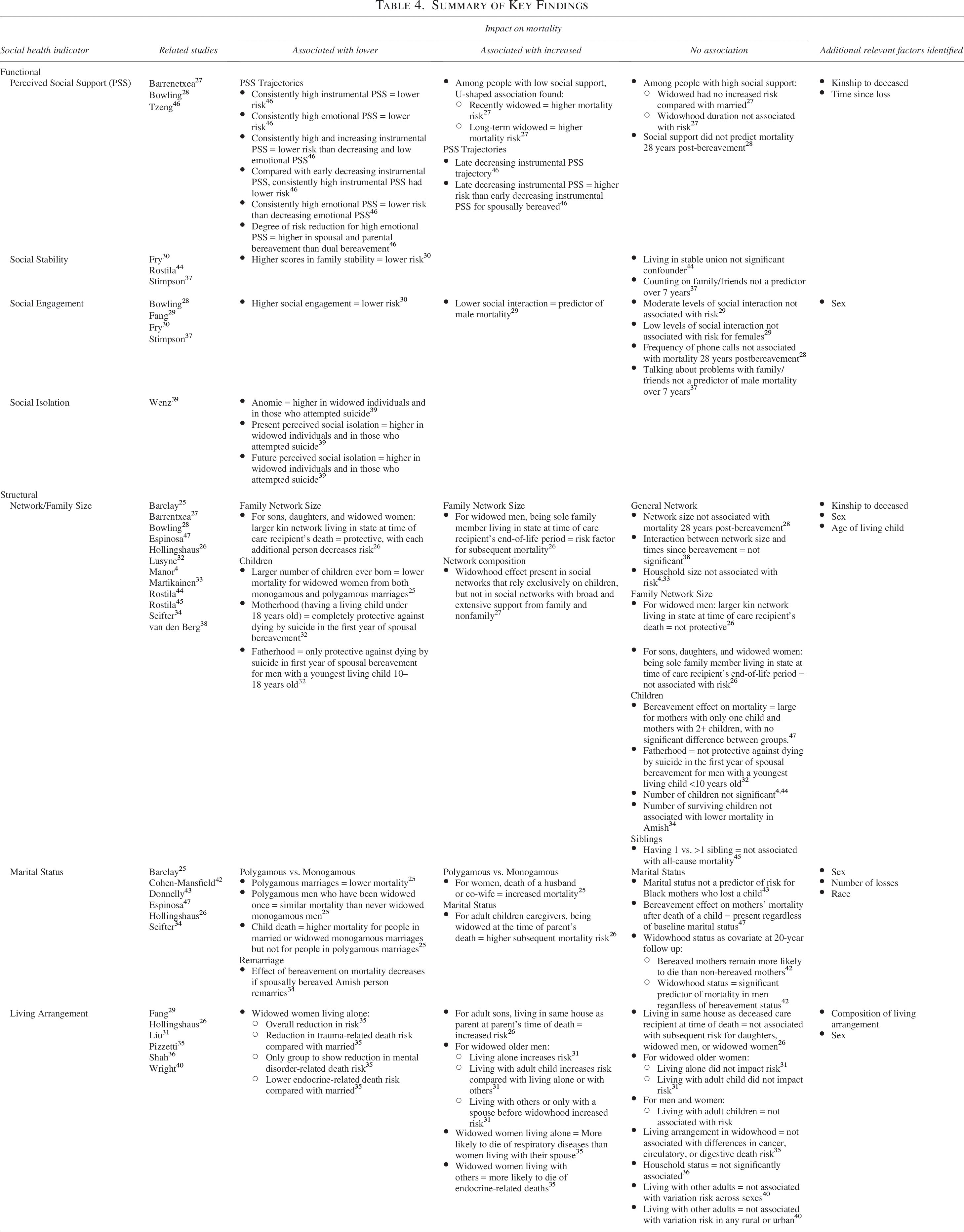
Key mortality-related findings associated with social health indicators are summarized in Table 4 and described below by functional and structural indicator groups.
Summary of Key Findings
Functional
Perceived social support
Three studies examined the relationship between PSS and mortality.
One Taiwanese study investigated 7-year trajectories of PSS and mortality risk in bereaved older adults. Findings showed that individuals with consistently high instrumental PSS (i.e., perceived quality of support received from close persons when sick) and consistently high emotional PSS (i.e., perceived willingness of close people to listen to personal problems and feelings) had a lower mortality risk. 46 Further trajectory comparisons revealed that individuals with consistently high instrumental PSS or instrumental PSS that increased over time had a lower mortality risk than those with an early decreasing instrumental PSS trajectory (i.e., initially high baseline scores followed by declines at 3 and 7 years). 46 Similarly, those with consistently high emotional PSS had a lower mortality risk than those with decreasing or consistently low emotional PSS trajectories. 46 Adjusting for covariates, the study found that, compared with those with an early decreasing instrumental PSS trajectory (i.e., initially high baseline scores followed by declines at 3 and 7 years), those with consistently high instrumental PSS had a 54% lower mortality risk for spousal bereavement, a 71% lower risk for parental bereavement, and a 59% lower risk for dual bereavement (i.e., individuals who experienced both spousal and parental bereavement). 46 Similarly, individuals with consistently high emotional PSS had a lower mortality risk compared with those with decreasing emotional PSS trajectories. Degree of risk reduction was higher in the parental bereavement group (74%) and the spousal bereavement group (72%) than in the dual bereavement group (58%). This study demonstrated clear associations between PSS and lower mortality risk, as well as specific associated trajectories.
Two studies reported significant associations between PSS and increased mortality risk. The aforementioned Taiwanese study found that late decreasing instrumental PSS trajectory (i.e., high baseline and 3-year scores followed by low 7-year scores) was significantly linked to increased mortality risk in the full sample. 46 However, when examined by bereavement type, increased mortality risk with late decreasing instrumental PSS was only significant for the spousal bereavement group. Additionally, among the spousally bereaved participants, those with a late decreasing instrumental PSS trajectory had higher mortality risk than those with an early decreasing instrumental PSS trajectory. 46
The second study, which examined widowhood and mortality in older adults in Singapore, found that widowhood was associated with increased mortality risk among individuals with low social support, but not among those with high social support. 27 When considering the duration of widowhood, a U-shaped pattern emerged among individuals with low social support, where both recently widowed adults (<5 years) and long-term widowed adults (>10 years) had heightened mortality risk, but individuals widowed between 5 and 10 years ago did not demonstrate heightened risk. 27
In contrast, one study found no significant associations between PSS and mortality risk. This study, which focused on elderly widowed individuals in England, reported that PSS did not predict differences in mortality rates at 28 years postbereavement. 28
Social stability
Three studies examined the relationship between social stability, such as counting on others and living in a stable union, and mortality.
One study found a significant association between social stability and mortality. A 6.5-year longitudinal, Canadian study on mortality risk among older widowed women found the relative risk of death associated with perceived family stability was 0.84 (95% CI 0.82, 0.87). 30 Widowed women with higher family stability had a 60% lower risk of mortality than those with low scores. 30
In contrast, a study on older Mexican Americans found that widowhood was a risk factor for mortality in men, 37 but their nonvalidated social stability measure (i.e., ability to count on family or friends) was not a significant predictor of mortality. 37 Similarly, a Swedish study found social stability (i.e., living in stable unions) did not significantly influence the association between child death and parental mortality. 44
Social engagement
Four studies investigated the relationship between social engagement, such as social activity participation and frequency, and mortality.
Two studies reported significant associations between social engagement and mortality risk. A 6.5-year longitudinal, Canadian study of older widowed women found the relative risk of death associated with social engagement (i.e., Brief Assessment of Social Engagement scale) was 0.80 (95% CI 0.71, 0.89). 30 Widowed women with higher social engagement scores had a 52% lower risk of mortality than those with lower scores. 30 Another Taiwan-based widowhood-focused study found that, among elderly men, lower reported social interaction levels (i.e., no endorsed social activity engagement) significantly predicted higher mortality risk. 29 However, moderate social interaction levels (i.e., endorsing 1–4 types of social activity engagement) did not predict mortality risk in men. 29 Among elderly women, neither moderate nor low social interaction levels were predictors of mortality risk. 29
Two studies found no significant association between social engagement and mortality risk. A 28-year follow-up study of elderly widowed individuals in England found that telephone call frequency was not associated with mortality differentials. 28 Similarly, in a study of older Mexican American men, widowhood was identified as a mortality risk factor, but their social engagement measure (i.e., frequency of discussing personal problems with family/friends) was not a predictor. 37
Social isolation
One U.S.-based study examined the relationship between three measures of social isolation and suicide-related mortality risk in widowed individuals, finding that all three social isolation measures were associated with an increased risk of mortality. 39 Anomie (i.e., pervasive sense of social disconnection or alienation from others) was higher in widowed individuals than other marital statuses and in widowed individuals who attempted suicide compared with individuals with other marital statuses. It was more pronounced in widowed individuals who had attempted suicide than those who had not. 39 Similarly, present social isolation (i.e., actual felt social isolation from meaningful relationships) was also higher in widowed individuals than in other marital statuses and in widowed individuals who attempted suicide compared with those who did not. Following this pattern, anticipated future social isolation was higher in widowed individuals and in widowed individuals who attempted suicide compared with those who did not. 39
Structural
Network/family size
Eleven studies examined the relationship between network/family size and mortality
Regarding general network size, two studies found no significant associations with mortality. An English study found network size—including children, siblings, other relatives, friends, neighbors, professional key people with whom the individual is in contact with—was not linked to mortality among elderly widowed individuals 28-years postbereavement. 28 Similarly, a Dutch study, which also focused on spousal bereavement, found the interaction between network size (i.e., number of children, other family members, friends, and neighbors whom had regular contact) and time since bereavement—which aimed to assess whether reduced social contacts over time influenced mortality—was not significant in their model. 38
One study examined both the size and composition of bereaved survivors’ social networks. This study, which explored the roles of gender and social support in the relationship between widowhood and mortality among older Chinese adults, conducted a sensitivity analysis assessing social support based on its sources and intensity. 27 Findings indicated that the widowhood effect (i.e., increased risk of mortality following spousal bereavement) was observed among individuals with social networks that relied exclusively on adult children. However, this effect was not present in individuals with broader and more extensive support networks that included both family and nonfamily members. 27
Examining family network size alone, a U.S.-based study of bereaved family caregivers in Utah found that having a larger kin network living in the same state at the time of the care recipient’s death was protective for sons, daughters, and widowed women, with each additional family member reducing mortality risk. 26 However, this protective effect did not apply to widowed men. 26 Furthermore, widowed men who were the sole family member living nearby at the time of the care recipient’s end-of-life period faced a higher risk of mortality, whereas this was not the case for sons, daughters, or widowed women. 26
Two studies—one Finland-based and one Israel-based—examined the impact of household size on mortality following spousal bereavement, but neither found significant associations.4,33 Additionally, a Swedish study examining number of siblings found that having one sibling versus multiple siblings was not associated with all-cause mortality among sibling-bereaved individuals. 45
Regarding number of children, one study reported significant findings. A U.S.-based study comparing individuals in monogamous and polygamous marriages found that having more children was associated with lower mortality for widowed women from both marriage types. 25
Conversely, four studies found no significant association between number of children and mortality risk. One U.S.-based study found that the bereavement effect on mortality was large for mothers with one child and mothers with two or more children, and, although the effect appeared more pronounced for mothers with only one child, the difference was not significant. 47 An Israel-based study on spousal bereavement found no interaction between bereavement and number of children for widowed spouses. 4 Another U.S.-based study found that the number of surviving children was not linked to mortality in widowed Amish spouses. 34 Additionally, a Swedish, nationwide follow-up study reported that number of children was not a significant factor in the association between child death and parental mortality. 44
In addition to child presence, one Belgian study explored the impact of child age on suicide-related mortality risk in the first year of spousal bereavement. For women, having a living child under 18 years old was protective against dying by suicide. 32 For men, fatherhood only reduced suicide risk if their youngest child was between 10 and 18 years old. 32 For men whose youngest child was under 10, fatherhood did not provide this protective effect. 32
Marital status
Six studies examined the relationship between marital status and mortality
Three studies showed significant associations. A U.S.-based study of bereaved family caregivers found that when an adult child is the caregiver of their parent, the adult child being widowed (compared with married) at the time of their parent’s death was associated with a higher mortality risk for the caregiver. 26 In a U.S.-based Amish sample, spousal bereavement’s impact on mortality was reduced when individuals remarried. 34 Similarly, a U.S.-based study comparing widowhood-related mortality outcomes in polygamous and monogamous marriages found that people in polygamous marriages had lower mortality rates. 25 Among men in polygamous marriages, those widowed once had a similar mortality risk to never-widowed men in monogamous marriages. 25 However, for women, the death of a husband or co-wife was associated with increased mortality risk. 25 Additionally, child death was linked to higher mortality in married or widowed monogamous individuals but was not associated with increased mortality in polygamous marriages, regardless of whether the death of a husband or co-wife was also experienced. 25
Three studies found no associations between marital status and mortality. A U.S.-based study that examined child death by midlife and subsequent mortality risk in Black mothers found marital status was not a predictor of mortality. 43 Another U.S.-based study found that the bereavement effect on mothers’ mortality after their child’s death was present regardless of baseline marital status. 47
An Israel-based study that followed bereaved parents over 20 years included widowhood status as a covariate, since bereaved parents were more likely to be widowed than non-bereaved. 42 They found that bereaved mothers were significantly more likely to die than nonbereaved mothers, but this effect was not significant for bereaved fathers. 42 Notably, they found widowhood status was a significant model predictor of mortality for men (regardless of parental bereavement status) but not women. 42 However, in this case, widowhood was considered an indicator of spousal bereavement rather than a measure of social health. Nonetheless, findings suggest this relationship warrants additional exploration.
Living arrangement
Six studies examined the relationship between living arrangements and mortality
One study found living arrangement was significantly associated with mortality risk. An Italian study assessing the impact of socio-demographic factors on mortality risk in older adults found that widowed women living alone had a 5% reduction in all-cause mortality risk than married women. 35 When examining specific causes of death, widowed women living alone had a 24% lower risk of trauma-related mortality and a 28% lower risk of endocrine-related death than married women. 35 They were also the only group to show a significant reduction (29%) in mortality from mental disorders. 35 However, there were no differences in living arrangements for mortality due to cancer, circulatory, or digestive diseases. Conversely, widowed women living alone were 30% more likely to die of respiratory diseases than women living with spouses. 35 There were no differences in mortality risk between widowed and married men.
Two studies found that certain living arrangements were linked to increased mortality risk. A U.S.-based study on the mortality risk of family caregivers found that sons who lived in the same household as the care recipient at the time of death had an increased subsequent mortality risk, whereas this association was not found for daughters, widowed women, or widowed men. 26 Another China-based study, examining gender and living arrangement in widowhood-related mortality risk found significant main and moderating effects of living arrangement among men. 31 Specifically, they found that widowed men living alone had an increased the chance of death for than those living with others. However, living alone was associated with a lower chance of death than living with adult children. 31 Compared with living alone or with other adults, living with at least one adult child significantly increased mortality risk for older men. For older women, the main and moderating effects of living arrangement were not significant. 31
Three studies found no significant associations between living arrangements and mortality risk. A Taiwan-based study of bereaved older adults found that living with children was not associated with widowhood effects. 29 Similarly, a U.K.-based study of older adults found that household status did not modify the risk of death after bereavement. 36 Finally, another U.K.-based study found that living with other adults was not associated with mortality risk changes following widowhood in urban or rural areas. 40
Discussion
To the best of our knowledge, this is the first systematic scoping review examining the relationship between social health and mortality following bereavement. Twenty-three studies met criteria. Notably, the overall high level of heterogeneity demonstrated across the focus, design, and methods of the 23 studies warrants cautious interpretation of our findings.
Results suggest mixed evidence regarding the role of social health on mortality risk following bereavement. Overall, bereaved individuals’ social health appears associated with both increased and decreased mortality risk; often dependent on social contexts and/or based on certain factors, such as gender and time since loss.
Functional
The interpretation of our functional indicator-related findings is notably limited by the small number of studies and significant lack of standardized measurement across studies. Some evidence suggested that consistently high levels of PSS were associated with lower mortality risk following bereavement. More consistent evidence suggested that low and decreasing trajectories of PSS were linked to increased mortality risk following bereavement. Importantly, time since loss surfaced as a factor worthy of additional research to further understand the relationship between PSS and mortality.
Higher social engagement and perceived social stability were associated with reduced mortality risk in one study; however, the study quality was poor. Multiple good-quality studies found no significant effects on bereavement-related mortality associated with perceived stability or engagement. However, one good-quality study did identify lower social engagement as a predictor of mortality in men, suggesting sex should be considered within future related research.
One study found that perceived isolation was strongly linked to suicide-related mortality among widowed individuals; however, it was conducted almost 50 years ago and had poor quality. Given that isolation is a major public health concern, 48 these potential suicide-related implications point to a need for more high-quality research.
Structural
Regarding structural indicators of social health, network, and family size-related findings varied based on context. General network size may be a more important factor to attend to for bereaved caregivers; however, general network size or household size may not be an impactful target for reducing bereavement-related mortality risk. While larger family networks or more children can be protective, results are inconsistent. The quality and composition of one’s social network, including availability of both family and nonfamily sources of support, often matter more than sheer size. The presence and age of children also have differential impacts on widowed fathers versus mothers, especially for suicide risk. Although not a modifiable indicator, the number and age of children a bereaved person has may aid with determining suicide-related mortality risk following bereavement. Furthermore, how bereft individuals navigate their relationships with their child(ren) may be a potentially modifiable target. Most network size-related studies were rated fair to good. One poor-quality study found the number of children was insignificant; however, a good-quality study found it was protective. Additional research is needed to determine the appropriate mechanism(s) to target within the bereaved parent–child relationship.
Marital status-related findings suggest that remarriage and polygamous marriage dynamics were associated with lower mortality risk following bereavement. These studies were rated fair and good quality, respectively. Notably, throughout our review, men and women often exhibited different vulnerability patterns. Marital status-related findings showing no significant results tended to be in female populations, where bereavement effects on mortality risk remained present regardless of marital status. Nonetheless, additional research examining marital status’ impact on mortality in men is needed, particularly given findings that suggest marriage and remarriage may serve a protective function. Marital status is an accessible indicator that could be gathered within hospital settings and is useful for identifying bereaved male patients who may benefit from interventions.
Regarding living arrangements, widowed women living alone were the only circumstance associated with decreased mortality risk. Multiple living arrangements were associated with increased mortality risk, particularly for men, including men living alone and living with adult children. Yet several studies found living arrangement was ultimately not significantly associated with mortality risk. Most living arrangement-related studies were rated as good quality. Assessing bereaved individuals’ living arrangements may be important to identifying individuals with heightened mortality risk across several disease populations.
Although additional research is needed, our overall structural indicator-related findings suggest that relying on support from adult children alone may not be sufficient to mitigate the potential negative effects of widowhood on mortality. Interventions aiming to bolster non-familial social networks could be important for older adults, particularly men.
Research gaps
Our review illuminated several limitations in the literature. Notably, we found a significant lack of standardization across studies, particularly regarding measurement and model building. We found limited use of validated tools, with significant variability in constructs and measures selected, which likely explains finding inconsistencies. Additionally, structural indicators predominated. Although structural indicators are often easier to assess, the broader bereavement literature suggests that relationship quality is more important than relationship quantity in protecting against negative outcomes. Methodologically rigorous research examining functional social health indicators and mortality following bereavement is needed.
Limited representation from non-Western populations was another notable limitation. Even within well-represented geographic areas, cross-cultural representation remains suboptimal. Inconsistent reporting of sociodemographic variables, such as age, race, and gender, further limits our understanding of potential subgroup differences. Although gender differences were explored in multiple studies, we found limited exploration regarding how other demographic and cultural factors moderate the relationship between social health and bereavement-related mortality. Given differences among racial groups regarding preferences in the type of social support received following bereavement,49,50 future research should examine the impact of these social health indicators on mortality risk.
Regarding bereavement-related characteristics, multiple gaps were identified. The literature heavily emphasizes spousal bereavement, which is not surprising given the established literature demonstrating widowhood effects on mortality.2,51,52 However, the role of social health on mortality risk following other forms of bereavement remains underexplored. With the growing older adult population, more adult children serve as caregivers for their parents. 53 Caregiving circumstances may negatively impact social health both before and after a parent’s death. Examining mechanisms of action is necessary to determine whether attending to the social health needs of caregivers could be a preventative approach for addressing bereavement-related mortality risk.
Our review highlights a clear gap in understanding potential mechanisms of action that explain the significant relationships found between social health and bereavement-related mortality. One potential explanation for this relationship may be the presence of a stress buffering effect. It is possible that consistent social support aids in mitigating stress, grief, and depressive symptoms following bereavement, which in turn influences mortality risk. Conversely, losing support may have detrimental effects, particularly over longer durations of bereavement. 33 If social support is absent, bereaved individuals may face secondary stressors alone, which further compounds stress and, consequently, increases mortality risk. For example, younger bereaved spouses demonstrate excess all-cause mortality compared with older bereaved spouses. 54 In addition to early spousal death being likely more and unexpected, younger bereaved spouses may have fewer spousally-bereaved peers, which could impact the support provided or available. Additional factors related to death circumstances, such as stigmatization, could also impact social support quality and availability.
Social conflict may be another contributing factor. In addition to familial conflict at end-of-life being common, 55 it is associated with worse psychological outcomes for bereaved individuals. 56 Further, dysfunctional familial dynamics following bereavement is associated with more psychological symptoms, poorer functioning, and greater difficulty accessing resources. 57 Given that stressful social relations have been associated with increased mortality risk in nonbereavement-specific samples, 58 future research should examine the role of conflict in the relationship between social health and bereavement-related mortality risk.
Health behaviors and monitoring may be another mechanism explaining the relationship between social health and mortality following bereavement. Previous widowhood research suggests factors such as sharing common lifestyles and socioeconomic environment with the deceased account for a small portion of postbereavement mortality risk. 33 Thus, it is likely that socially influenced mechanisms postbereavement would further contribute to risk. Previous research shows a robust relationship between social support and physical health, 59 and social support from within and outside family systems has been longitudinally associated with lower risk of physical frailty. 60 Within the bereavement literature, less social activity is associated with longer deterioration in physical health. 61 Thus, the relationship between social health and mortality risk may be explained via physical health; however, additional research is needed. Examining if the presence of or support from others serves to encourage better health habits, health monitoring, or facilitation of health care access following bereavement may be warranted.
Finally, cultural expectations may be another mechanism for future research. Studies within this review across diverse cultural contexts (e.g., Taiwanese, Amish, polygamous vs. monogamous marriages) suggest that the impact of widowhood and social support on mortality is influenced by cultural norms regarding family structure, remarriage, and social roles. Indeed, factors such as living arrangements or remarriage may carry different psychological or social implications for men versus women or across different societies.
Limitations
Despite our methodological rigor and use of quality appraisal to protect against bias, several limitations are noteworthy. As the only shared language between screeners, this review only included studies published in English. Additionally, although conducting a meta-analysis to examine estimated effects would be ideal, we were unable to complete such analyses due to the heterogeneity of social health measures and the range of variables used as controls within statistical models. Further, given inconsistencies in sociodemographic reporting, the strength of conclusions that can be drawn is limited.
Implications
Our synthesis of the research examining the relationship between social health indicators and bereavement-related indicators clearly demonstrates a need for additional research that (1) implements standardized methodology and (2) aims to better understand the mechanisms at play. Identifying the key mechanisms that explain the relationship will allow for the development of better tools that provide valid results and can be more reliably used to inform the development of impactful interventions for bereaved individuals.
Although the heterogeneity of our findings makes confidently proposing clinical implications difficult, there are several avenues to consider. For example, trajectory patterns of bereaved individuals’ functional social health may better inform subsequent mortality risk compared with solely implementing screeners during the acute bereavement period. Early interventions may be particularly beneficial if support wanes. Thus, monitoring social support for changes (specifically, diminishment) following bereavement should be longitudinal. Additionally, social support interventions that bolster a bereaved individual’s social engagement may be warranted, particularly for bereaved men. Such tailored interventions may be incorporated into existing preventative models of bereavement care within palliative care services. 62 Given the association found between feelings of disconnection or perceived isolation and suicide-related mortality among widowed individuals, additional research examining the association between perceived isolation and suicide-related mortality within other bereaved individuals may be warranted. Our findings suggest that interventions facilitating relationships outside of immediate family members, such as social networking for bereaved older adults, may also be particularly beneficial. Importantly, additional research exploring moderators and mechanisms of action that explain the relationships between social health and mortality are needed to more confidently determine (1) which intervention approaches would be the most appropriate and (2) for whom such interventions may be the most impactful.
Conclusion
This systematic scoping review describes the role of social health in the relationship between bereavement and mortality. Although the current evidence is insufficient for generating firm conclusions, it identifies clear directions for future research that will aid in better understanding and even preventing bereavement-related mortality risk.
Authors’ Contributions
M.H.: Conceptualization, methodology, investigation, formal analysis, writing—original draft preparation, and project administration. K.S.: Conceptualization, writing—original draft preparation, and review and editing. H.W.: Conceptualization, investigation, and writing—review and editing. M.R.: Conceptualization, writing—review and editing. S.K.: Investigation, writing—review and editing. P.M.: Conceptualization and writing—review and editing. H.P.: Conceptualization, methodology, writing—review and editing, and supervision.
Footnotes
Acknowledgments
Thank you to Michelle Demetres at the Weill Cornell Medicine Samuel J. Wood Library for her support in reviewing the search strategy and coordinating retrieval of full-text documents for review, and to Sophia Kakarala, Lexa Harpel, and Francesco Osso for their feedback on an earlier version of this article.
Author Disclosure Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Dr. Prigerson reports payment or honoraria for lectures, presentations, or educational events from relationships with: MD Anderson Cancer Center, University of Connecticut, Rutgers NJ Health Study Scientific Advisory Council, Cleveland Clinic. Dr. Prigerson reports support for attending meetings and/or travel from relationships with: University of Paris, Portuguese Instituto for Psychological Studies, Mid-West Palliative Care. Dr. Prigerson reports receiving royalties through relationships with: American Psychiatric Association Publishing (co-editing Grief and Prolonged Grief book), Routledge (co-editing Bereavement book). Dr. Maciejewski reports receiving royalties through a relationship with: American Psychiatric Association Publishing (co-editing Grief and Prolonged Grief book). Madeleine Rogers reports relationships via employment with: Memorial Sloan Kettering Cancer Center (non-paid), University of Miami (paid). Authors declare that they have no additional known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding Information
Dr. Hardt’s research activities are supported by the National Institute of Aging (T32AG049666). Dr. Prigerson’s research activities are supported in part by the National Cancer Institute (R35CA197730), National Institute of Minority Health Disparities (R21MD017652), the National Institute on Aging (R21AG077144), and the National Institute of Nursing Research (R01NR019831, R01NR021159). Dr. Maciejewski’s research activities are supported in part by grants from the National Institute on Minority Health and Health Disparities (R21MD017652) and the National Institute of Nursing Research (R01NR021159). Hardt, Rogers, Winoker, and Kolla are supported in part by Prigerson and Maciejewski’s research grants (R01NR019831, R35CA197730, R01NR021159). Dr. Smith is supported by the Medical Research Council (MR/V001841/1) and the National Institute for Health and Care Research (NIHR) Oxford Health Biomedical Research Center (NIHR203316). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.