
Abstract
Background:
Grieving is a natural process, and many people adjust with support from family and friends. Around 40% of people would benefit from additional input. Online bereavement support interventions may increase access to support. Evidence regarding their acceptability and effectiveness is emerging but needs to be synthesised.
Aim:
To synthesise evidence on the feasibility, acceptability, effectiveness, impacts and implementation of online interventions to improve wellbeing, coping and quality of life after bereavement.
Design:
A rapid review of evidence regarding online bereavement support. We appraised study quality using AMSTAR 2 and the Mixed Methods Appraisal Tool.
Data sources:
English language articles published 1 January 2010 to 4 January 2024, using Ovid MEDLINE, Ovid Embase and APA PsycINFO. Eligible articles examined formal and informal online interventions to improve bereavement outcomes.
Results:
We screened 2050 articles by title and abstract. Four systematic reviews and 35 individual studies were included. Online bereavement support was feasible, acceptable and effective in reducing grief intensity, stress-related outcomes and depression. Where reported, participant retention was typically >70%. Positive impacts included: access to a supportive community at any time, reduced isolation; opportunities to process feelings; normalisation of loss responses; access to coping advice and opportunities for meaning-making and remembrance. Negative impacts included upset due to insensitive comments from others via unmoderated online forums.
Conclusion:
Online interventions can widen access to acceptable, effective bereavement support and improve outcomes for bereaved people. National policies and clinical guidelines relating to bereavement support need to be updated to take account of online formats.
Keywords
Approximately 60% of people who are bereaved adjust with only the support of family and friends, whilst around 40% require additional support with their grief.
Online and digital interventions to support bereaved people are rapidly developing and show promise as a way to meet increased demand.
Online bereavement support is feasible, acceptable and effective in improving grief intensity, reducing stress-related outcomes and depression.
Online bereavement support can enable access to a supportive community, reduce isolation, provide opportunities to express and process emotions, normalise grief responses, give access to information on adaptive coping and provide opportunities for adaptive meaning-making.
Negative aspects of online bereavement support include technical issues accessing support, insensitive comments via unmoderated online forums or distress triggered by reading other people’s experiences of loss.
Online bereavement support interventions including self-directed, volunteer-led, and formal psychological interventions, delivered online by mental health specialists, have much potential in ensuring that differing levels of bereavement support needs experienced by individuals can be met.
Challenges to accessing online support and potential negative impacts should be taken into consideration when developing a new online bereavement support intervention.
Future research should investigate the value of distinct forms of online bereavement support for more diverse populations, assess its cost-effectiveness, and determine optimal levels of facilitation for different levels of need.
Background
Grieving is a natural process, and typically 60% of people who are bereaved adjust with support from family and friends. Approximately 40% need additional support, including 6%–10% who experience symptoms of pathological grief.1,2 Since the COVID-19 pandemic, demand for bereavement support has increased, as has the complexity of need. 3 The increase in the prevalence of grief symptoms and disorders since the COVID-19 pandemic is a global phenomenon, with a meta-analysis of 15 studies involving 9289 participants across several countries estimating a pooled prevalence rate of grief disorder at 46%. 4 A UK-based longitudinal study of 711 bereaved individuals found that the proportion of people meeting the threshold for posttraumatic grief disorder was higher following the COVID-19 pandemic compared with pre-pandemic times, with over one-third of people bereaved showing these symptoms at 13 months following bereavement. 5 Loneliness, social isolation, disruption to typical mourning practices and limited access to support is associated with this increase,3 –6 and has contributed to the growing need for accessible evidence-based bereavement support.
Healthcare organisations and practitioners increasingly recognise the importance of digital health interventions in improving access to quality healthcare services and support. 7 Smartphones, video-conferencing, websites, apps and other virtual and online resources are particularly valuable for people in remote and rural locations, and those who need access to support at any hour.8 –10 In palliative and end-of-life care contexts, such interventions are thought to widen access to support in a cost-effective manner, with evidence indicating positive impacts on education, information sharing, decision-making and communication. 11
Digital interventions used to improve wellbeing and quality of life after bereavement are rapidly being developed and evaluated. Emerging evidence from four systematic reviews indicates acceptability and perceived value of online support for bereaved populations.12 –15 However, these previous reviews were focussed on specific populations such as those bereaved by suicide; 14 specific forms of support such as online forums or support groups13,14 or Cognitive Behavioural Therapy.12,15 So, while they provide valuable detail in relation to specific populations and interventions, they are limited in scope. Critically, all four previous reviews were published before, or at the start of the COVID-19 pandemic, thus only include data collected before the COVID-19 pandemic. Due to radical changes in the design of health and bereavement services during the pandemic, with the rapid introduction of telemedicine, virtual consultations and online support, the way in which people accessed support changed. People became more used to accessing healthcare and bereavement support remotely.16 –18 Given this seismic shift in how health and bereavement care is accessed, a review of the evidence pertaining to the value of online bereavement support interventions that takes account of a wider range of populations, and also includes studies conducted during and since the COVID-19 pandemic, is needed to guide future intervention development.
We aimed to synthesise published evidence on the development, feasibility, effectiveness, impacts and implementation of online interventions for people who have been bereaved. Our aims were broad as we were interested in any evidence that would support the development of online bereavement support, including our own novel online bereavement support intervention (My Grief My Way). 19 To ensure our findings would be of interest to service commissioners, we included evidence on interventions designed to meet the needs of people with bereavement support needs that could not be met by their own family, friends and local networks. We were also keen to examine evidence on implementation, given the recognition of the need to consider factors that influence implementation from the early stages of intervention development. 20 We viewed the earlier four reviews as a starting point, but sought to draw on a wider range of populations, interventions and study designs to meet our aims. Our research questions were:
i. What types and formats of online interventions for bereavement support have been evaluated, and what is the evidence for their effectiveness and impacts?
ii. For which populations have online bereavement support interventions been evaluated and what evidence exists on their effectiveness?
iii. What is the evidence on the feasibility and acceptability of online interventions for bereavement?
iv. What are the barriers and facilitators regarding implementing online bereavement support?
v. What type of outcomes have been assessed in research examining online interventions for bereavement support, and what comparators have been used?
Methods
Design
We undertook a rapid integrative review of the evidence for online interventions for bereavement support. Rapid reviews are an efficient approach to evidence synthesis, ensuring that findings can be quickly made available to decision-makers. 21 We chose a rapid review design so that evidence could quickly be generated and synthesised to inform the development of our My Grief My Way online bereavement support intervention (ISRCTN: 18357870). 19 We conducted a rapid integrative review as we were interested in evidence generated from diverse methodologies. 22
To ensure rigour, we followed interim guidance for rapid reviews.21,23 In line with this, we established an experienced team in conducting systematic reviews; we registered our protocol; we searched at least two electronic databases; we involved more than one reviewer in article screening; we ensured all data extracted were cross-checked by a second reviewer; we ensured each article was independently appraised for quality by two reviewers; we used Covidence (software) to streamline the process; and we provided a comprehensive knowledge synthesis describing results, quality of evidence and implications.26 We sought feedback on findings from our My Grief My Way 19 stakeholder group, which included organisations involved in designing and delivering bereavement support, as well as public representatives with experience of grief.
Search strategy
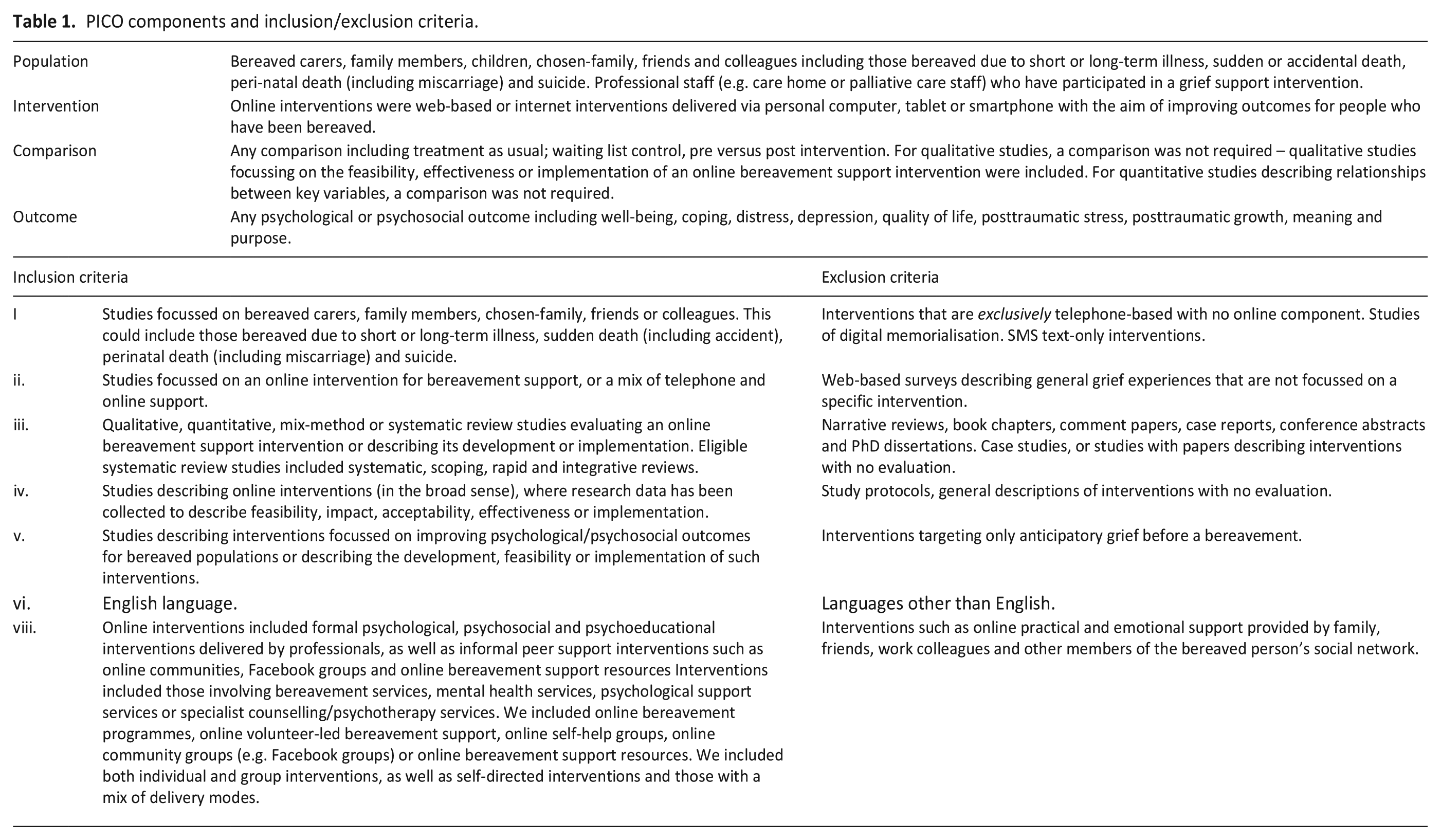
We use the PICO (Population, Intervention, Context, Outcome) mnemonic to refine the search strategy, research questions and the inclusion and exclusion criteria (Table 1). 24 We searched three databases: Ovid MEDLINE, Ovid Embase and APA PsychInfo to identify papers published between 1st January 2010 and 11th January 2023. We decided to include articles published prior to the pandemic, as our research questions were broader than those covered in existing reviews, and this allowed for a more comprehensive synthesis of evidence. We used 2010 as a starting point as smartphones started to become popular from this period onwards, and there was a consensus within the research team that evidence prior to this may have less relevance given the rapid technological changes since. We updated the search in January 2024 to add studies published between 11th January 2023 to 4th January 2024. All searches were undertaken by AF. We included primary research and review papers in the English language only, due to time constraints and a lack of translation resources. Commentaries, protocols and editorials were excluded. We also searched PROSPERO and ISRCTN for information on current studies and reviews in progress. The review protocol was registered with PROSPERO on 3rd March 2023. 25
PICO components and inclusion/exclusion criteria.
Study selection
We included studies evaluating online bereavement support for anyone who had been bereaved, irrespective of their relationship to the person who died, the type of bereavement or when this occurred (Table 1). We included all types of research designs and systematic reviews. While systematic reviews are often excluded from updated reviews, Cochrane rapid review recommendations suggest including systematic reviews as a relevant study design. 21 We also included informal interventions, such as online forums, if these were formally evaluated.
Data extraction
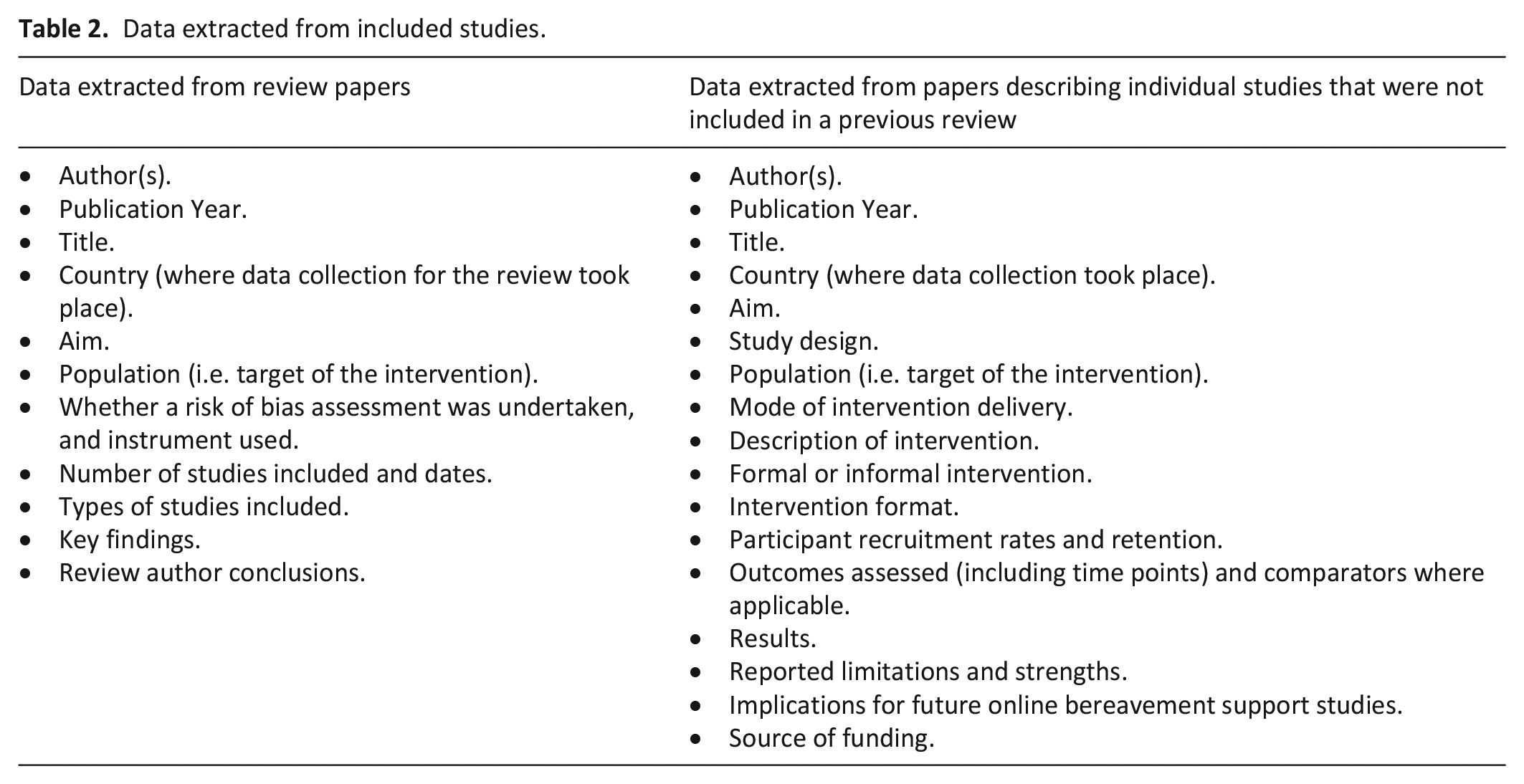
Search results were uploaded to Covidence, an online platform that supports systematic data handling for systematic review studies. 26 Duplicates were automatically removed by the Covidence software. A team of six researchers independently screened article titles and abstracts (AC, AF, APAM, DW, BS and EH) before progressing to independent full text review by two researchers (AC, AF, EH, DW, BS and DG). All abstracts were independently screened at least twice. Where areas of conflict were identified, consensus was reached through consulting a third researcher or the wider team. Data were extracted from individual studies by one member of the review team and cross-checked by another. Data extracted were saved in an MS Excel file, which contained one worksheet for systematic review studies and another for individual studies. Data extraction headings are outlined in Table 2. Data from individual studies previously reported in systematic reviews were not extracted, 21 instead we extracted data from the systematic review in its entirety.
Data extracted from included studies.
Quality appraisal
We used the AMSTAR (A MeaSurement Tool to Assess Systematic Reviews) Version 2 27 to assess the quality of systematic reviews, and the MMAT (Mixed Methods Appraisal Tool) 28 to appraise all other studies. Each article was assessed independently by two members of the research team (AC, AF, APAM, DW, EH or BS). Disagreements were discussed to reach consensus, involving a third reviewer if needed.
Data analysis and synthesis
The first author (AF) conducted a narrative synthesis organised around our research questions. This was descriptive in nature in line with recommendations for rapid reviews.21,23 MS Excel pivot tables were used to tabulate key characteristics of each study, alongside a summary of the quantitative and/or qualitative findings. Systematic review studies were tabulated and described separately from individual studies due to the different design and approach to quality appraisal. All papers were downloaded into NVivo 12 alongside the data extraction tables. Our analysis was informed by a framework approach, 29 whereby we sought to deductively code study findings in relation to pre-existing categories relevant to our research questions: intervention feasibility and acceptability, effectiveness, impacts and factors relating to implementation to guide future online intervention development. NVivo search and explore functions were used to support this process. A meta-analysis was not performed given the heterogeneity of study designs, interventions and outcomes.
Results
Overview
A total of 2050 article titles and abstracts were screened (Figure 1). From these, 1904 papers were excluded, leaving 146 papers for full text review. Following a full text review of all papers, a further 107 papers were excluded as they did not meet study criteria (n = 94) or had been previously reported in the included systematic reviews (n = 13). Four systematic reviews (Table 3) and 35 primary studies (Table 4) were included in the synthesis.
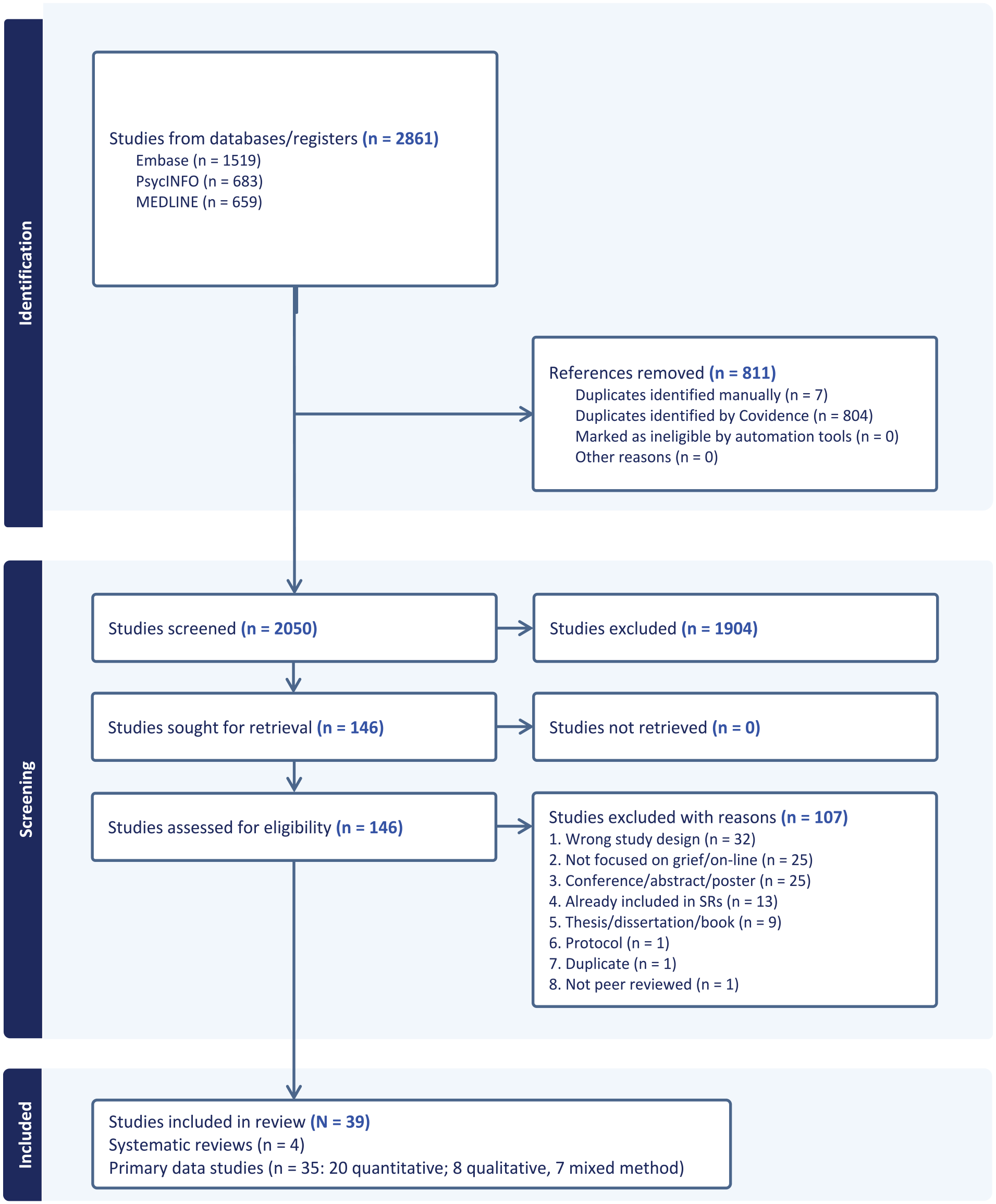
PRISMA flow chart. 30
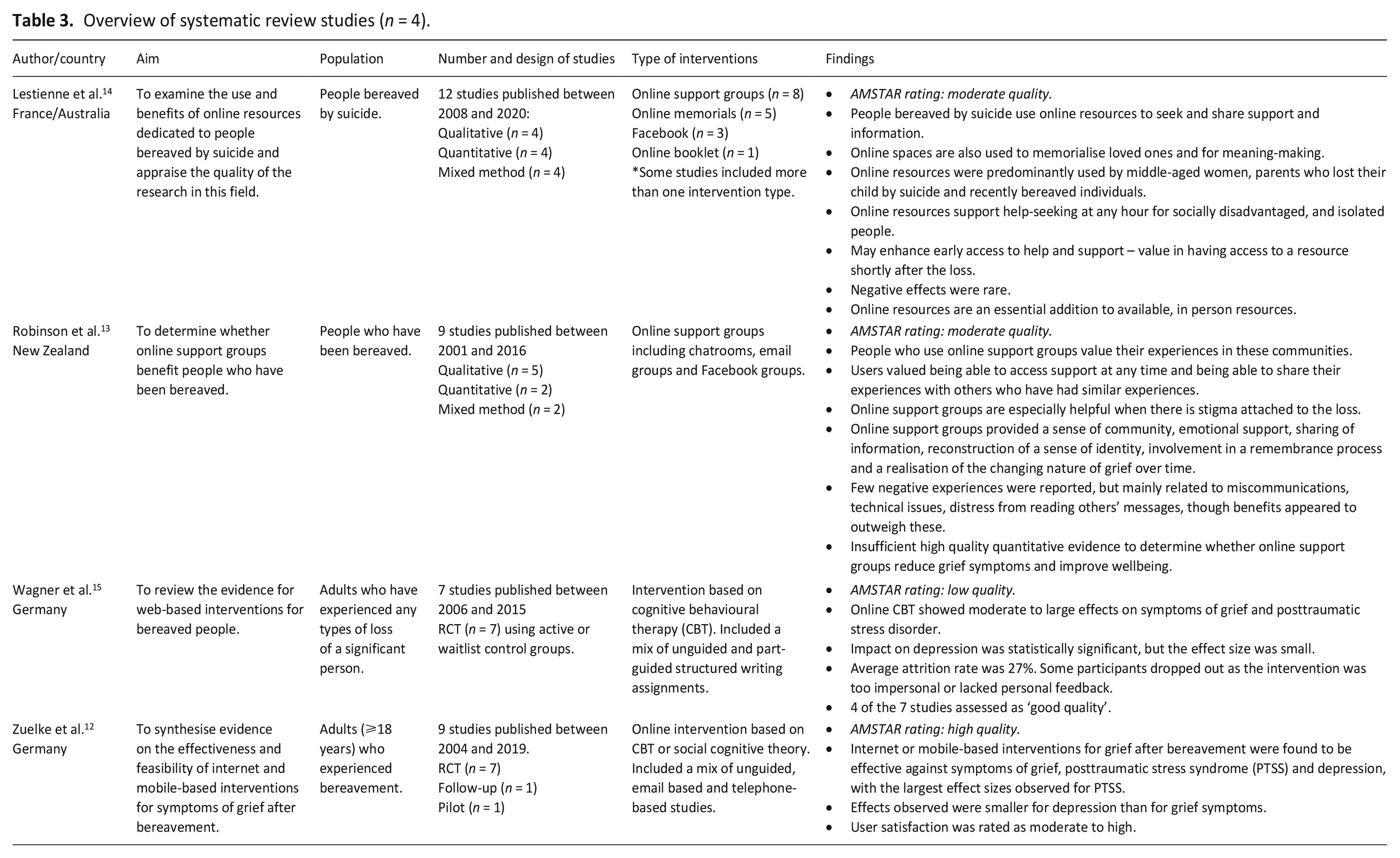
Overview of systematic review studies (n = 4).
Overview of original studies (n = 35).
Evidence quality
Of four systematic reviews, one was high quality, 12 two were moderate quality13,14 and one was low quality. 15 Most primary research studies were judged as high (n = 20) or moderate quality (n = 10), with few low-quality studies (n = 5; Supplemental Material File 1). We did not exclude studies based on their quality; instead we included all studies to allow for a comprehensive understanding of the evidence. We refer to quality when reporting findings from the systematic review papers in the relevant sections below; and report the quality score allocated to each individual study in our Supplementary material file.
Findings from systematic reviews
Four systematic reviews examining online bereavement support were included (Table 3).12 –15 These were published between 2019 and 2021, with all included studies conducted before the COVID-19 pandemic. One review focussed on bereavement following suicide 14 and three were focussed on support for adults irrespective of the type of bereavement.12,13,15 Two reviews included quantitative, qualitative and mixed-methods study designs,13,14 one evaluated randomised controlled trials (RCTs) and feasibility studies, 12 while one included RCTs only. 15
Interventions based on cognitive behavioural therapy (CBT) were the focus of two reviews.12,15 One review, evaluated as low-quality, included seven RCTs focussed on web-based CBT; 15 their meta-analysis revealed moderate to large effects relating to improvements in symptoms of grief and posttraumatic stress disorder for those receiving online CBT compared to those in a control group. A statistically significant improvement in depression was noted, though the effect was small. A higher number of treatment sessions was linked with greater impact. The other, a high-quality review, included nine studies, 12 seven of which were the same as those evaluated by first review described. 15 All but one were CBT-based interventions. The non-CBT intervention was a psychoeducational online resource based on social cognitive theory. Both reviews found that online bereavement support resulted in statistically significant improvements in symptoms of grief, depression and posttraumatic stress compared to a control group. User satisfaction was reported in over half of the online CBT-informed interventions analysed in the high-quality review, 12 and was typically rated as moderate to high.
The two reviews examining online support groups and forums included a variety of study designs – quantitative, qualitative and mixed method.13,14 Both reviews were evaluated as moderate quality. The integrative review, 14 concluded that online resources offer around-the-clock support for people who have been bereaved by suicide and are helpful to those who are seeking and sharing support and/or information, memorialising their loved ones and meaning-making. Negative effects were rare. The other, a systematic review, 13 examined online support for bereaved adults, irrespective of the type of loss. It identified positive impacts of online peer support including being part of an understanding community of people who share similar experiences, access to emotional support, information sharing, remembrance, reconstruction of identity and acknowledgement of the how grief changes over time.
Taken together, evidence from four systematic reviews indicate the value of online bereavement support interventions. These include positive impacts on bereavement outcomes, 24-hour access to bereavement support and improved access to support for people in remote areas and those that may not otherwise receive support. However, the reviews also conclude that evidence, in particular quantitative evidence was not high quality, and that further rigorous research is needed to strengthen the evidence base.
Findings from primary studies
Thirty-five papers, not previously identified for inclusion in the four systematic reviews, were synthesised. These were published between 2011 and 2023, with a noticeable increase in the number published from 2021 onwards. Studies were conducted by academic teams based in the USA (n = 11), Europe (n = 16), Australia (n = 3) and one each in China, India and South Korea. A further two papers involved teams from more than one country. Of the 16 European papers, five were from Germany, three from the Netherlands and one each from Denmark, Italy, Norway, Portugal, Spain, Sweden, Switzerland and the UK (Table 4).
Study designs were quantitative (n = 20), qualitative (n = 8) and mixed method (n = 7). Most focussed on evaluation (n = 22), while a sub-set were specifically development studies (n = 5), or feasibility/pilot studies (n = 8). In terms of study populations, nearly half did not specify any type or cause of bereavement (n = 16). Four studies were focussed on support for people bereaved following suicide; six involved people bereaved due to cancer or a long-term condition; three studies examined support following bereavement during the COVID-19 pandemic, three examined peri-natal loss and three focussed on bereavement support following sudden or unexpected death (e.g. road traffic accident or sudden cardiac arrest in a young person). See Table 4.
Over 40% of studies (n = 15) did not specify the relationship between the deceased and bereaved person, however others examined specific relationships such as parent of the deceased (n = 8, including one study on bereaved fathers and one on bereaved mothers), spouse or partner (n = 4), any family member (n = 4, including one study focussed on children who had lost a close family member), grandparent of the deceased (n = 1), child or young adult who had been bereaved of a parent (n = 1), close friend (n = 1) or sibling (n = 1).
Intervention type and format
Interventions were broadly categorised as psychological, psychoeducational, psychosocial or unspecified/in development, though there were many overlaps. CBT was the most common psychological approach used as a basis for online interventions (n = 13).31,35,37,41,42,44,46,51,55,57,58,60,61 Theories of grief such as task-based approaches to mourning, and the Dual Process Model formed the basis for a small number of interventions.31,63,65 Psychoeducational interventions aimed to share information on grief and coping skills, and normalising grief experiences.32,62,63 Psychosocial interventions included online forums and interventions that aimed to promote peer support and connection with others.33,40,50,52,53,56,65 Many interventions included both psychosocial and psychoeducational components.32,34,36,38,39,43,54,64 A small number of development studies did not specify an intervention type from the outset.
The format of interventions could be broadly classified as self-directed (n = 14), individual (n = 11) or group-based (n = 10; Table 4). Self-directed interventions included engagement with online forums and self-guided access to online CBT with little or no feedback. Individual interventions included live-chat conversations, CBT with individualised feedback and one-to-one support delivered online. Group interventions were typically bereavement support group sessions delivered online and facilitated by a trained volunteer or professional.
Effectiveness of online bereavement support
Across all studies using quantitative measures, there was good evidence that online bereavement interventions result in statistically significant improvements in a range of outcomes (Table 4). These include grief symptoms or severity,31,35,37,43,44,49,51,54,58,60,61 depression,35,37,41,43,46,49,51,58,60,61 anxiety35,41,55 stress or posttraumatic stress,35,41,43,46,51,60 insomnia,37,43,55 coping31,48 and mental health or quality of life.37,41,48 Of these, five studies reported improvements in grief outcomes versus a control condition,35,41,46,57,61 providing strong evidence of effect compared with those studies comparing outcomes based on pre-post designs or within-group changes over time. Other studies reported improvements in outcomes that were not statistically significant, often due to small sample sizes. For example, four studies reported improvements in grief outcomes that were not statistically significant.39,49,55,65 No studies reported worsening of outcomes following online bereavement support. Several studies alluded to cost-savings, low-costs or cost-effectiveness of online interventions, but did not specify the types of costs and cost-savings.
Acceptability of online bereavement support
Acceptability relates to the individual’s perceived satisfaction with an intervention in relation to addressing a problem. Overall, online interventions for bereavement support were judged to be acceptable. Several studies described overall benefits and positive impacts of online interventions indicating appropriateness and acceptability.31 –34,36,38 –41,43 –46,48 –55,59 Such benefits included: access to a supportive community and reduced isolation32,33,36,38,39,40,43,44,47,50,52 –54,62; opportunities to express and process one’s feelings around grief;36,38,40,44,50,52,56,62 normalising of feelings and experiences in response to loss;40,44,56 information on coping strategies;36,40,44,45,48,59,62 meaning-making;33,44,45 and opportunities to remember the person who died.45,50,53
People who had been bereaved described online forums as a safe space in which they could disclose personal information.33,36,49,52 Some experienced online support as less overwhelming than attending an in-person face-to-face support group. 38 People bereaved due to suicide found online ‘live chat’ a safe space to disclose non-socially desirable details relating to their loss and to make sense of suicide through the reconstruction of events and the motivations of the person who died. 33
Effectiveness and acceptability by intervention format
For all types of online support formats, assessed via quantitative, qualitative and mixed method designs, positive impacts were identified. Group-based interventions were perceived as beneficial,32,43,44,62 helped people cope and feel less alone,38,43 supported communication 62 and provided opportunities for longer standing group members to advise and support new members. 44 Individual interventions helped reduce grief symptoms 61 and prolonged grief disorder;41,57,65 promoted adapted coping, 48 and supported emotional processing and meaning-making.33,45 Self-guided interventions, which included self-guided formal interventions such as CBT, as well as unguided access to intervention forums and chat groups were also linked with positive impacts and general benefits. These included reduced grief symptoms,35,46,51,56 improved coping,31,52 access to a supportive community,47,52 opportunities to remember the person who died50,53 and general perceptions of benefit. 40
Impact on access to bereavement support
Online bereavement support was found to facilitate access to support, especially for people who lived in remote or rural areas, or areas where local support was unavailable.32,34,54 Many online interventions are available 24/7, enabling support at any time.36,39 Online forums and communities were found to provide early access to bereavement support before people have managed to arrange access to more formal or structured support.34,50 Online interventions were also viewed as convenient and flexible, with individuals accessing the support they needed, when they needed it.32,36,61 For some bereaved individuals, online interventions were valued as they enabled anonymous engagement.33,36,38,43,57 There was evidence that online support could be beneficial to people of all ages including older individuals.31,37,43,48 One study successfully recruited older adults for a feasibility study examining online CBT versus a control condition for insomnia, mood and quality of life. 37 Mean age of participants was 65 years (range = 55–84 years), though most were white educated women, based in the US with access to a computer and already using social media. 37 Another found evidence for the feasibility and effectiveness of an online virtual reality support group for widow and widowers who had a mean age of 67 years, though the sample consisted of mostly white female participants, based in the US. 43 One study examining the impact of an internet-based meditation programme on coping and quality of life amongst late-life immigrant older widows concluded that an internet-based meditation programme was effective. 48 However, eligibility criteria included self-reported comfort using digital technology and smartphones at the time at the time of recruitment (in 2017).
Negative impacts and unintended consequences
Few risks or negative impacts were identified. Those that were reported were mainly unintended consequences linked with unmoderated online forums. Such impacts included possible increases in grief intensity on reading posts about other people’s experiences of loss online 39 or upset due to inappropriate or insensitive online comments. 50 A lack of personal contact associated with unmoderated forums such as Facebook was also perceived as negative in comparison with other forms of support. 50 Recognising these issues, one study examining web forums for young people who had been parentally bereaved recommended guiding young people to information regarding online safely when using bereavement support web forums. 52
Intervention feasibility and retention rates
We examined retention rates as an indicator of intervention feasibility. Retention rates and/or dropout rates were available for about half of all studies (n = 16). Overall, retention rates were high – most studies (11 of 16) reported retention rates greater than 70% and all but one 35 reported retention rates over 50%. For instance, an RCT examining the impact of a therapy-assisted web-based writing intervention for prolonged grief disorder reported overall drop-out rates of only 7% (6 of 87 participants). 41 The intervention consisted of 10 structured writing tasks that participants worked on independently in two self-scheduled 45-min sessions per week. Within 24 h of each session, participants received feedback from a trained psychologist. In a secondary data analysis linked with this study, 42 the authors reported that therapeutic alliance (favourable relationship between therapist and client) predicted improvement in symptoms of prolonged grief disorder and suggested this is also likely to have had a positive impact on retention.
Only one study highlighted unusually high levels of drop-out. 35 This was an efficacy RCT of an unguided web-based grief intervention for adults who had been bereaved during the COVID-19 pandemic. Of 882 allocated to the intervention, only 45 completed it, and of those, more than half were lost to follow-up. The authors suggested this may have been due to the online self-guided nature of the intervention, a preference for face-to-face interventions or due to the length of the intervention (12 modules delivered over 36 days, in video or text format). There was also a delay between participant consent and access to the online support, during which many participants withdrew.
Facilitation varied across interventions from no facilitation, to asynchronous feedback;41,42,46,57 real time volunteer or co-facilitator facilitation;33,36 or real-time online support from a therapist or mental health specialist.32,43,44 Retention was lowest for unguided interventions 35 and highest for interventions involving greater levels of facilitation.41,42
Barriers and facilitators of online bereavement support
Factors linked with the implementation of online bereavement support included technical issues and mode of facilitation or support. Technical barriers included challenges typing information or feedback, difficulties controlling sound and hearing audio-visual material, or difficulties logging into a website.37,38 Irrelevant or repetitive material was also a barrier to engagement. 37 Sending feedback or reminders to individuals to keep going with the intervention could promote engagement.34,41 For unguided interventions, instructions need to be simple and clear, and need to take account of different cultural norms. 48 Information also needs to be focussed on topics relevant to the individual and easy to access. 37 For interventions that involved therapist feedback or input, the quality of therapist engagement or ‘therapeutic alliance’ was considered important, and needs to be fostered to support intervention acceptability and effectiveness. 42 While IT literacy and language were occasionally mentioned as a possible barrier, 34 no studies explored this in any detail.
Discussion
Our review of evidence from 4 reviews and 35 individual studies indicates that online bereavement support is an acceptable form of bereavement support for many, and can lead to improvements in grief intensity, depression and stress-related outcomes. Retention rates for formal interventions were typically over 70%, with most bereaved participants completing the intervention once they started. Few risks of online bereavement support were identified. Where reported, such risks tended to relate to informal or non-moderated forms of support such as chat groups where risks included increased grief intensity on exposure to the loss of others; insensitive online comments; or spending too much time online reflecting on loss. However, in general negative impacts were outweighed by positive impacts such as access to a supportive community, space to reflect and share experiences safely, access to information on coping and opportunities to remember the person who had died.
Positive impacts were identified for all formats, from self-guided to individual-facilitated and group interventions, with many of the impacts described also closely resembling those identified in a recent review of predominantly in-person bereavement interventions. 66 This suggests that there is potential value in diverse forms of online bereavement support with different formats appealing to different individuals depending on their preferences and needs. For those seeking a supportive community, online group-based interventions or online forums may serve their needs.13,14 For those struggling with specific grief symptoms or prolonged grief disorder, online interventions offering individualised therapist-facilitated support may be most suitable. For instance, online CBT based interventions delivered by a therapist, can be of particular benefit to those experiencing prolonged grief disorder and related problematic symptoms.12,15 National bereavement support guidance needs to reflect the potential value of online interventions to increase access to bereavement support for people with varying levels of needed, who might not otherwise be able to benefit.
While the findings from this review are generalisable only to those that have accessed online bereavement support, our results suggest that once accessed, online interventions are generally perceived as acceptable across a range of populations. This includes young people, 52 older adults,31,37,47,48,59 bereaved parents,34,36,38,39,45,50,55,62 people bereaved due to chronic conditions,36,41,54,55,63 as well as those bereaved due to suicide and traumatic circumstances.33,44,57,61,64 Overall retention was typically above 70%, and in line with retention rates for online interventions targeting mental health problems. 67 While most studies described good levels of acceptability overall, there was some evidence that particular sub-groups found it less easy to engage in some online formats. For instance, a study of online art therapy reported that bereaved older adults were less likely to express themselves and were more likely to withdraw. 49 Barriers to uptake of online interventions for older adults have been well documented, but can be addressed through active engagement of this group in intervention design, leading to increased self-efficacy in use of technology and knowledge in relation to security concerns. 68
Our findings align with results from reviews of online interventions for mental health and wellbeing for other populations. A meta-review of 304 studies found that digital health interventions offer promise in treating a range of problems including substance use-, anxiety-, mood- and trauma-related disorders. 69 Specifically, they offer greater comfort and flexibility than in-person visits, while retaining usefulness. 69 Similarly, systematic review evidence from 43 studies examining online interventions for anxiety and depression reported that online interventions are generally effective in reducing symptoms, with impacts being enhanced where there is therapist input. 70 There is also evidence that unguided interventions can be effective, with a review of 32 studies focussed on self-guided online interventions aimed at preventing anxiety and depression, revealing that self-guided interventions have a small but meaningful impact on anxiety and depression. 71 The same review found that unguided interventions may lead to a reduced risk of receiving a diagnosis of depression for certain populations, though evidence regarding preventing anxiety was inconclusive. Despite a need for more rigorous evidence, there is a growing consensus from this review and the wider literature that online interventions aiming to improve mental health and wellbeing outcomes, are acceptable and effective.
Strengths and limitations
This rapid integrative review provides a comprehensive and timely synthesis of the evidence relating to online bereavement support. A large team of co-authors facilitated rapid data extraction and quality appraisal of eligible papers. Our inclusion criteria were intentionally broad to allow exploration of a range of online interventions, including formal and informal bereavement support. However, the heterogeneity of study populations, intervention types and outcomes across studies meant that a sub-analysis of impact according to different intervention formats was not possible.
Implications for intervention development and practice
Our findings suggest that online interventions could play a role in improving access to bereavement support for different levels of need.72 –74 This could be through self-guided information and support; online interventions facilitated by volunteers, healthcare professionals and community groups; as well as online interventions delivered by clinical psychologists or mental health specialists to support people experiencing problematic grief or prolonged grief disorder.
Online delivery of bereavement support enables the provision of bereavement support to those who might not otherwise have access, or choose to access, such support. This includes those in remote and rural areas,32,54 those who prefer anonymity when seeking support,14,33,36,39,43,57 and those who need convenient and flexible access, or support outside of usual working hours.36,56 By signposting to, and offering online bereavement support, organisations which provide bereavement support can increase their reach and impact.
The degree of moderation or facilitation needs careful consideration when developing online bereavement support. In general, retention is lowest for unguided interventions 35 and highest for those that involve some level of facilitation.41,42 Personalised feedback, information regarding intervention content or effectiveness, reminders, rewards and feedback about progress was linked to participant retention in the studies evaluated here, and are known to promote engagement with web-based mental health programs in general. 75 To minimise any potential negative impacts from engagement with online forums, use of a forum moderator needs to be considered. Moderators can help create a cohesive culture of empathy, sensitivity and care in a safe community, 76 but also need individual and organisational-level support to operate effectively and maintain their own wellbeing. 77
Directions for future research
Very few studies reported the recruitment or response rate, that is the number of eligible participants versus the number who consented to take part. This is often impossible to determine for studies conducted in applied settings as researchers often do not know the total number of people who had sight of a study invitation or advert. However, this can result in non-response bias, whereby those who were recruited are systematically different from those not recruited, and therefore not representative of the general population. 78 Inequalities in access to bereavement support are well-documented with minoritised ethnic groups, LGBTQ+ communities and people with lower socio-economic status more likely to experience barriers to support.79 –81 Given the lack of data on response rates, it is not possible to gauge the extent to which diverse groups of individuals may have experienced barriers to participation. Across most studies, white females were overrepresented, reflecting the characteristics of participants in previous bereavement interventions 82 and UK national bereavement surveys.79,83 Future studies need to engage more diverse communities so that findings are applicable to a wider range of individuals. No studies focussed on socio-economically deprived or LGBTQ+ communities were identified.
Our review reveals that the evidence for online bereavement support is rapidly emerging, but several gaps can be identified. First, there is a need for more studies examining the effectiveness of online bereavement support compared to a control group. Pre- and post-studies provide weaker evidence as they can’t control for the possibility that improvements may occur with the passing of time, as opposed to engagement with the intervention. Second, most research participants tend to be white females – there is a need to develop and evaluate online interventions with diverse populations, in particular those groups that are typically underserved.84,85 Research that engages minoritised ethnic groups, LGBTQ+ people and individuals from different cultural and faith backgrounds is urgently needed, and individuals that are to be served by the intervention, need to be involved in its design from the outset. Third, research is needed to explore the role of moderators and facilitators of online bereavement support interventions, and their relationship with key outcomes such as coping and quality of life for people seeking support. 86 Fourth, research that involves children and young people in the development of engaging online support needs to be conducted. Fifth, despite the assumption that online interventions are more cost-effective than in-person interventions, we did not identify any health-economic data to support this. Research examining the costs and cost-savings associated with different forms of online bereavement support is urgently needed and needs to take account of indirect costs such as impact on physical health, ability to work and addiction. Finally, future research might usefully adopt implementation science approaches to examine potential barriers and facilitators relating to accessing online bereavement support, and consider steps that can be taken to maximise inclusivity. 87
Conclusion
Online interventions can widen access to acceptable, effective bereavement support and improve outcomes for people who have been bereaved. Negative or unintended consequences of online bereavement support were mainly linked with unmoderated forums, but these were infrequently reported. Future research examining the role of online intervention facilitation and moderation is recommended, as are studies involving more diverse populations and assessing cost-effectiveness. National policies and clinical guidelines relating to bereavement support need to be updated to take account of the wide variety of online bereavement support formats that are now available.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163241285101 – Supplemental material for A rapid review of the evidence for online interventions for bereavement support
Supplemental material, sj-docx-1-pmj-10.1177_02692163241285101 for A rapid review of the evidence for online interventions for bereavement support by Anne Finucane, Anne Canny, Ally Pax Arcari Mair, Emily Harrop, Lucy E Selman, Brooke Swash, Donna Wakefield and David Gillanders in Palliative Medicine
Footnotes
Acknowledgements
We thank the My Grief My Way Advisory Group for comments and feedback on this review. We also thank Libby Sampey for assistance in the early planning stages of this work.
Author note
Donna Wakefield is also affiliated to Wolfson Palliative Care Research Centre, Hull York Medical School, University of Hull, Hull, UK.
Author contributions
AF, DG, LS and EH conceived the study. All authors made a significant contribution to the concept, design, acquisition, analysis or interpretation of data. AF drafted the manuscript. All authors revised it critically for important intellectual content. All authors approved the final version of the article for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Research ethics and patient consent
Ethical approval was not required as this was a rapid review study.
Research ethics
Ethical approval or participant consent was not required for this study as it involved no individual participant contact.
Data management and sharing
All relevant data are included in the article or available in Supplemental Files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.