
Abstract
Aims:
To determine who provides bereavement support in the community, what sources are perceived to be the most or least helpful and for what reason, and to identify the empirical elements for optimal support in developing any future compassionate communities approach in palliative care.
Design:
A population-based cross-sectional investigation of bereavement experiences. Sources of support (informal, community and professional) were categorised according to the Public Health Model of Bereavement Support; most helpful reasons were categorised using the Social Provisions Scale, and least helpful were analysed using inductive content analysis.
Setting and participants:
Bereaved people were recruited from databases of funeral providers in Australia via an anonymous postal survey (2013–2014).
Results:
In total, 678 bereaved people responded to the survey. The most frequently used sources of support were in the informal category such as family, friends and funeral providers. While the professional category sources were the least used, they had the highest proportions of perceived unhelpfulness whereas the lowest proportions of unhelpfulness were in the informal category. The functional types of helpful support were Attachment, Reliable Alliance, Social Integration and Guidance. The five themes for least helpful support were: Insensitivity, Absence of Anticipated Support, Poor Advice, Lack of Empathy and Systemic Hindrance.
Conclusion:
A public health approach, as exemplified by compassionate communities policies and practices, should be adopted to support the majority of bereaved people as much of this support is already provided in informal and other community settings by a range of people already involved in the everyday lives of those recently bereaved. This study has provided further support for the need to strengthen the compassionate communities approach, not only for end of life care for dying patients but also along the continuum of bereavement support.
The majority of bereaved people rely on family and friends for bereavement support.
There is little evidence as to how this support is provided and the reasons for its perceived helpfulness.
Consequently, there is little indication about which particular support strategies are optimal for building a community’s capacity to provide the type of support advocated by the compassionate communities approach now widely advocated by palliative care services.
While the professional sources were the least used, they had the highest proportions of perceived unhelpfulness.
The types of informal social support most valued as helpful were the emotional bonds (attachment), the practical assistance (tangible alliance) and the perceived sense of belonging (social integration).
A public health approach to bereavement care is needed to support ‘everyday assets’ in the community who care for the majority of the bereaved, without the overreach from professional services.
The compassionate communities approach, so far focussed on care of the dying, is well and truly operational in the bereavement phase.
This study provides strong empirical indicators and directions that encourage a compassionate community approach to future bereavement support practice and policy.
Findings provide guidance as to operationalising how to offer professionalised services to those who would most benefit, while not providing these services unnecessarily to those who are supported within their natural support networks.
More research is needed in identifying a range of useful practice models that connect health and social care services with local communities and build upon local helping networks.
Introduction
Social support is an important factor influencing bereavement outcomes.1,2 Despite social support being the protective factor that is most amenable to intervention, it has received limited attention in the literature.3,4 Albrecht and Adelman 5 describe social support as ‘verbal and non-verbal communication between recipients and providers that reduces uncertainty about the situation, the self, the other, or the relationship, and functions to enhance a perception of personal control in one’s life experiences’ (p. 19). Research suggests that, following the loss of a relative or friend, social support can act as a buffer against psychological morbidity by reducing grief symptomatology and facilitating psychological adaptation.3,6 Importantly, it is also one of the few factors influencing the grieving process that can be modified and targeted during treatment to reduce the effects of those risk factors less modifiable, such as gender and personality features.2,7 Despite this, there is little empirical evidence supporting the methods employed to build the community’s capacity to provide this type of support. While many studies have identified that the majority of bereaved people rely on family and friends as providers of support, there are limited studies, in number and methodological rigour, examining in detail the ways in which this support is provided and the reasons behind its perceived helpfulness.4,8 –11
Building the community capacity to support death, dying and loss is an important public health issue in palliative care. Central to any public health approach focussed on bereavement care in this particular context is the development of community supports and interventions that address the multiple morbidities (e.g. depression, job loss or social isolation) and mortalities (e.g. suicide or sudden death) associated with bereavement and that may be amenable to prevention, harm reduction and early intervention. ‘Compassionate Communities/Cities’ approaches are community development strategies, now widely discussed in recent palliative care literature, that attempt to build these kinds of supports and interventions to address the social epidemiology of grief and loss.12 –14 These models of community support rely on identifying and developing local caring networks around the dying person and their family. Compassionate communities normalise seeking and accepting help from family, friends, neighbours, schools and workplaces for emotional and social support. In health promotion terms, support for grieving people is not only the task for health and social services but becomes everyone’s responsibility. 15 This is also one of six key recommendations of the recent UK palliative care framework for local action 2015–2020 – ‘Ambition 6: Each community is prepared to help’. 16
Qualitative studies on social support have highlighted its importance in adapting to life in the wake of loss via the death of a significant other. They indicated that connecting with bereaved others and experiencing compassion from support providers are two of the most helpful forms of social support reported by participants.17 –19 The few quantitative studies that have examined different forms of social support and their relationship to bereavement outcomes have shown that people who would most likely benefit from support might be least likely to receive it.20,21
Weis’ model of social provision affords perhaps the most comprehensive assessment of perceived social support by offering a clear conceptualisation of six separate functions of social support. 22 The Social Provisions Scale (SPS) was developed based on Weis’ model and taps into these following six types of social support provisions: ‘Attachment’ refers to having an emotional and affectionate bond with another person, thus providing a sense of security; ‘Social Integration’ refers to the perceived sense of belonging to a group that shares similar interests/concerns; ‘Guidance’ refers to the perceived availability of someone one can turn to for advice or information; ‘Reliable Alliance’ refers to the perceived availability of someone to rely on for tangible assistance; ‘Reassurance of Worth’ refers to the belief that one is valued by others; and ‘Opportunity for Nurturance’ refers to the belief that one is needed by other people. 23
However, no studies have examined the perceived social support in bereavement in a systematic way with the use of the SPS as a framework guiding the classification of functional types of social support. 23 Also no studies have examined the interaction between source and functional type of support in a population-based bereaved sample. Knowledge of bereavement based just on clinical encounters has resulted in many service providers taking an undifferentiated approach to bereavement care, despite research suggesting that this type of early intervention by professionals may not be effective.24,25 Rumbold and Aoun 10 conclude that the research community, clinical practitioners and support services are well informed by the minority who seek support through health professionals; however, little is known about how bereavement is lived out in everyday life by the majority of those who do not seek these services.
In their public health model of bereavement support which advocates for partnerships between the formal and informal networks, Aoun et al. 8 used a population-based survey to investigate the range of support received overall from professional caregivers and community sources. They classified sources of bereavement support into three: informal support, community support and professional support. Informal support included support offered by family, friends, funeral directors, financial or legal advisors, religious or spiritual advisors and the Internet or literature. Community support included support offered by General Practitioners (GPs), nursing homes, hospitals, pharmacists, community groups, palliative care providers or school-based advisors. Professional support included support offered by trained counsellors, bereavement support groups, social workers, case coordinators, psychologists and psychiatrists.
Objectives
The overall aim of this study is to determine who provides bereavement support in the community, what sources are perceived to be the most or least helpful and for what reason. Therefore, the three specific objectives were
To identify the nature and extent of the sources of bereavement support, as outlined in the public health model of bereavement support, whether perceived helpful or unhelpful;
To identify the nature and extent of the functional types of bereavement support, using the SPS as the guiding theoretical framework;
To explore the empirical evidence for supporting the compassionate communities approach in bereavement support.
Methods
Ethics approval was granted by Curtin University Research Ethics Committee (HR 57/2012). We undertook the quantitative and qualitative analyses of cross-sectional questionnaire data pertaining to helpful and unhelpful sources and types of social support accessed by a population-based sample of bereaved people.
Study design
The study is a population-based cross-sectional investigation of bereavement experiences. A postal survey was used to collect information from clients of four funeral providers in Australia, specifically from metropolitan and regional areas of Western Australia and Victoria (2013–2014), 6–24 months after the death of their family member. Funeral providers were used as it was not possible to recruit through the Death Registry in Australia.
Participants and procedures
A total of 3190 study packages were delivered to the four funeral providers. These packages contained an invitation letter addressed from the funeral provider to the family, information sheet, the questionnaire, a list of support services for the family to use in case the respondent became distressed while completing the questionnaire and a reply-paid envelope. The funeral providers then selected all clients who were bereaved 6–24 months ago from their databases, attached names and address labels on the envelopes and mailed the study packages. Consent was implied by the return of the completed survey. No reminder letter was sent as it was felt to be too intrusive on the bereaved families. Clients were eligible to participate in the study if they had been bereaved by a close family member or friend in the specified time frame, were able to read, understand and write in English and were over 18 years of age.
Measures and analyses
The questionnaire was developed in consultation with a reference group comprising representatives of the funeral industry, bereavement counsellors, palliative care services, primary care and community-based services. It has eight sections with a total of 82, predominantly closed, questions. The questionnaire was designed to gather information on participant demographics, the supports they accessed, those supports they would have liked to have been able to access, their perceived support needs and the extent to which they felt these needs had been met.8,26 The current study focussed predominantly on the survey section pertaining to the perceived helpfulness of bereavement supports the individual accessed. This section asked the bereaved respondent to list in order, three of the most helpful or unhelpful sources of support accessed, and to state why they were the most or least helpful. To ensure quality and rigour of the coding process, two authors independently blind-coded a random 10% of responses. These codes were compared, with differences discussed until consensus was reached and the remaining responses were coded by one author.
The question on helpful support was as follows: ‘Please list up to 3 of the most helpful sources of support that you accessed and reasons why they were the most helpful’. Spaces were provided for free descriptions on the questionnaire. Responses to the first part of the question were categorised according to the three sources of support identified through the Public Health Model of Bereavement Support: informal support, community support and professional support. 8 Descriptive statistics for variables were calculated using IBM SPSS Statistics Version 24. Responses to the second part of the question were categorised using the SPS as an initial framework for the identification of different types of functional support. 23 The SPS has undergone considerable psychometric evaluation with multiple studies demonstrating that the measure has good internal consistency, test–retest reliability and convergent and discriminant validity.23,27
Similarly, the question on unhelpful support was as follows: ‘Please list up to 3 of the least helpful sources of support that you accessed and reasons why they were the least helpful’. As there is no framework for categorising non- or unhelpful support, responses to the second part of the question were categorised using an inductive approach to coding whereby the data were subject to open content analysis and five themes were generated: ‘Insensitivity’ is related to rude or insensitive remarks, unexpected/inappropriate behaviour or behaviour that was incongruent with the situation; ‘Absence of Anticipated Support’ is support that was expected to be provided or available to the bereaved, but it did not materialise; ‘Poor Advice’ included unwanted advice or interference; ‘Systemic Hindrance’ is the system putting up obstacles and ‘Lack of Empathy’ included indifference and lack of interest. 28
Results
Profile of the bereaved and deceased
In total, 678 bereaved people responded to the survey (21.3% response rate). In all, 71% of the bereaved people who responded were female, mean age of 62.4 years (standard deviation (SD) = 12.2); 49.6% were married and 37.0% were widowed; 36.8% were the spouse of the deceased and 45.3% were the son or daughter of the deceased; 69.5% were Australian citizens; 45.2% had finished high school, 30.5% had a diploma or trade qualification and 19.6% had a university degree; 36.9% were currently employed and 38.9% were retired. The mean period of bereavement for respondents was 14.3 months (SD = 6.3; Table 1).
Characteristics of the Bereaved.
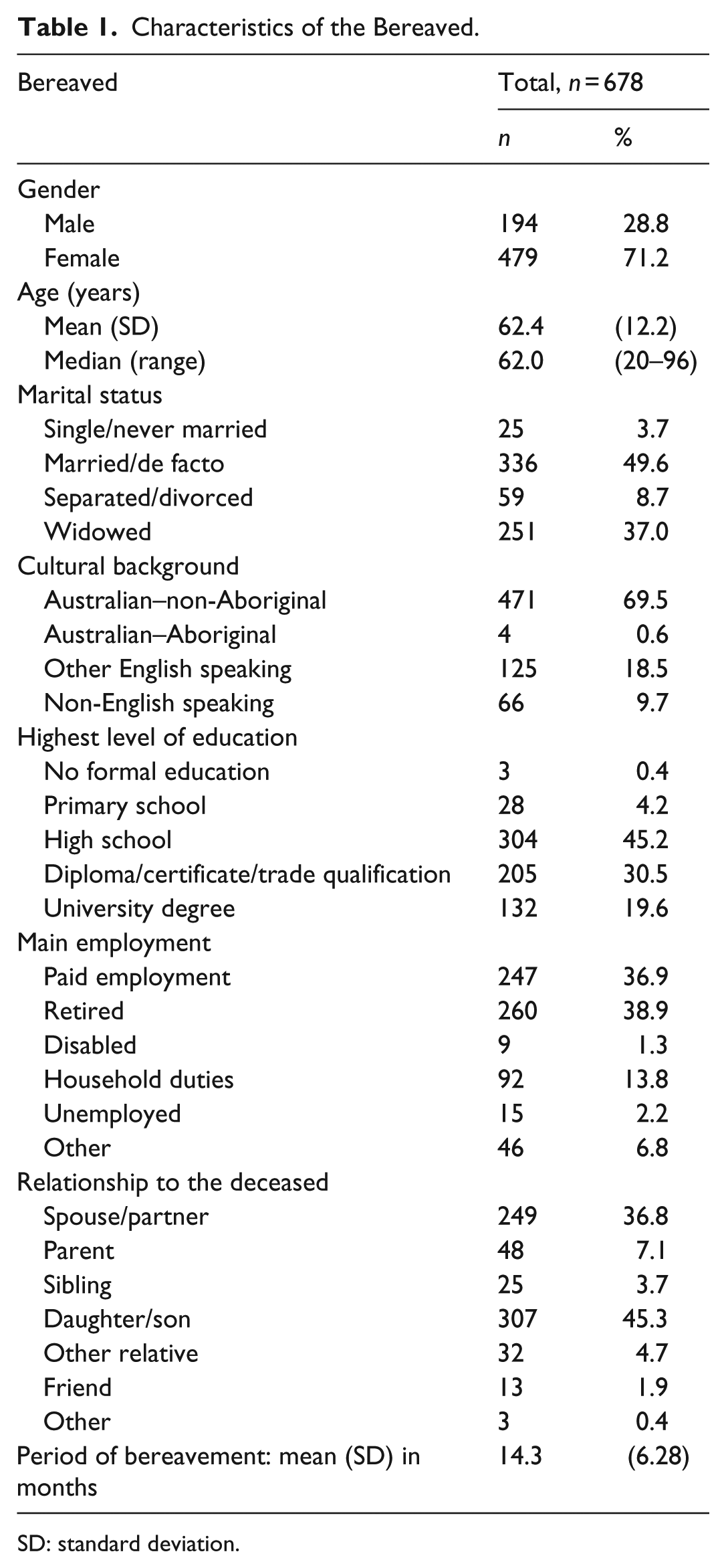
SD: standard deviation.
The mean age of the deceased was 75.4 years (SD = 18.3); about half of the deceased were female; 68% of the deaths were due to life limiting illnesses (mainly cancer 30%, heart disease/organ failure 18% and dementia/old age 15%) and 54% of these care recipients used palliative care services; their death occurred in hospital (39%), nursing home (32%), home (18%) and hospice (9%).
Perceived helpfulness
The most frequently used sources of support were those in the informal category such as family, friends and funeral providers (80%–90%), followed by GPs from the community category (58%) (Figure 1). While the professional category sources were the least used, they had the highest proportions of perceived unhelpfulness (Table 2): nearly half of those who used psychiatrists found them unhelpful (46%), and over a third of respondents who used the following services rated them unhelpful – bereavement support group (41%), case coordinator (39%), social worker (38%) and school-based advisor (36%). Similar high rates of unhelpfulness were reported in the community category and in particular a community group (40%), community pharmacist (39%) and palliative care service (33%). By contrast, the lowest proportions of unhelpfulness were in the informal category where only 8% found family unhelpful, followed by the funeral provider (8.7%) and friends (11.7%) (Table 2).
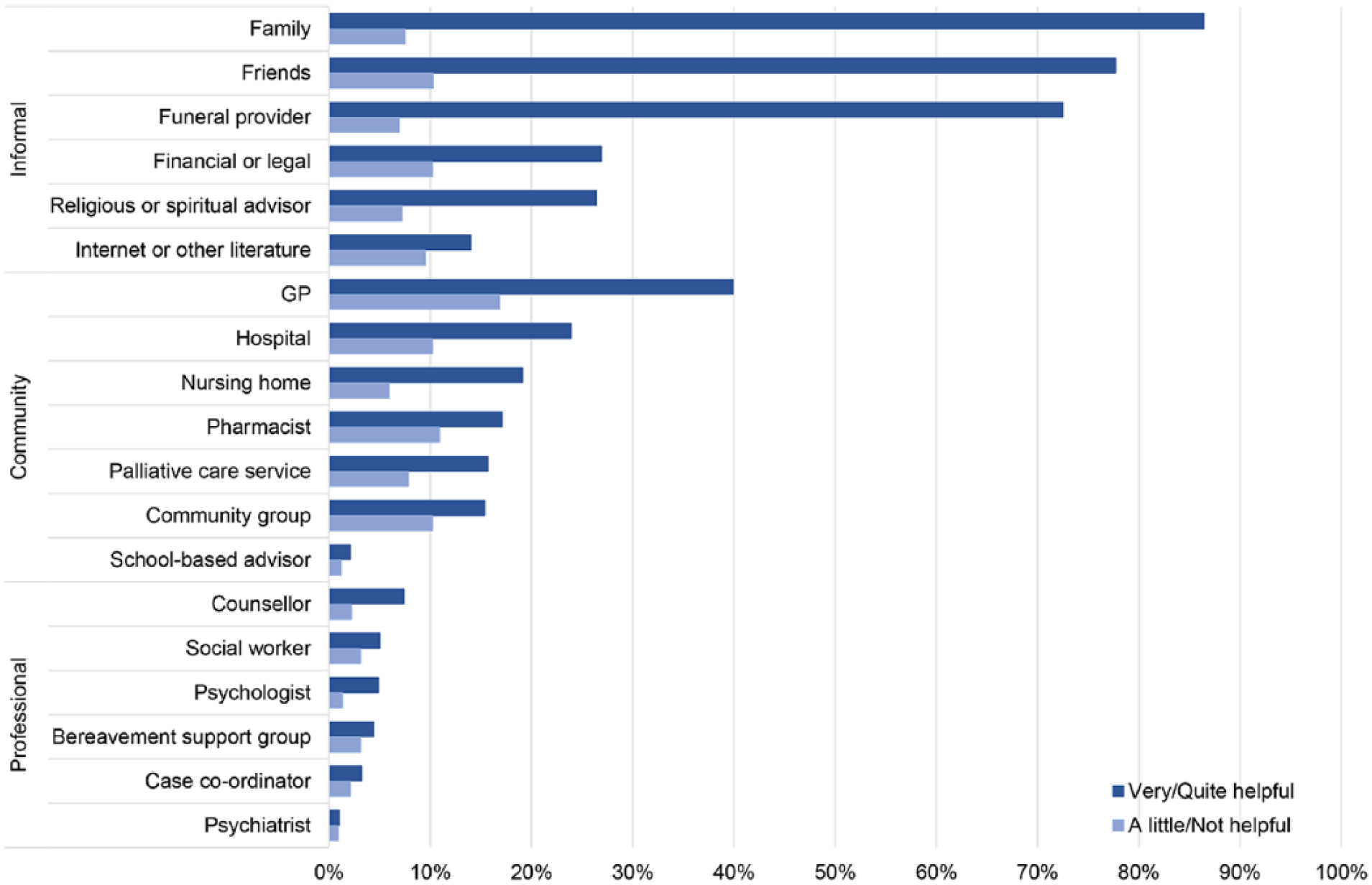
Perceived helpfulness of sources of bereavement support.
Perceived helpfulness of each source of bereavement support (n = 678).
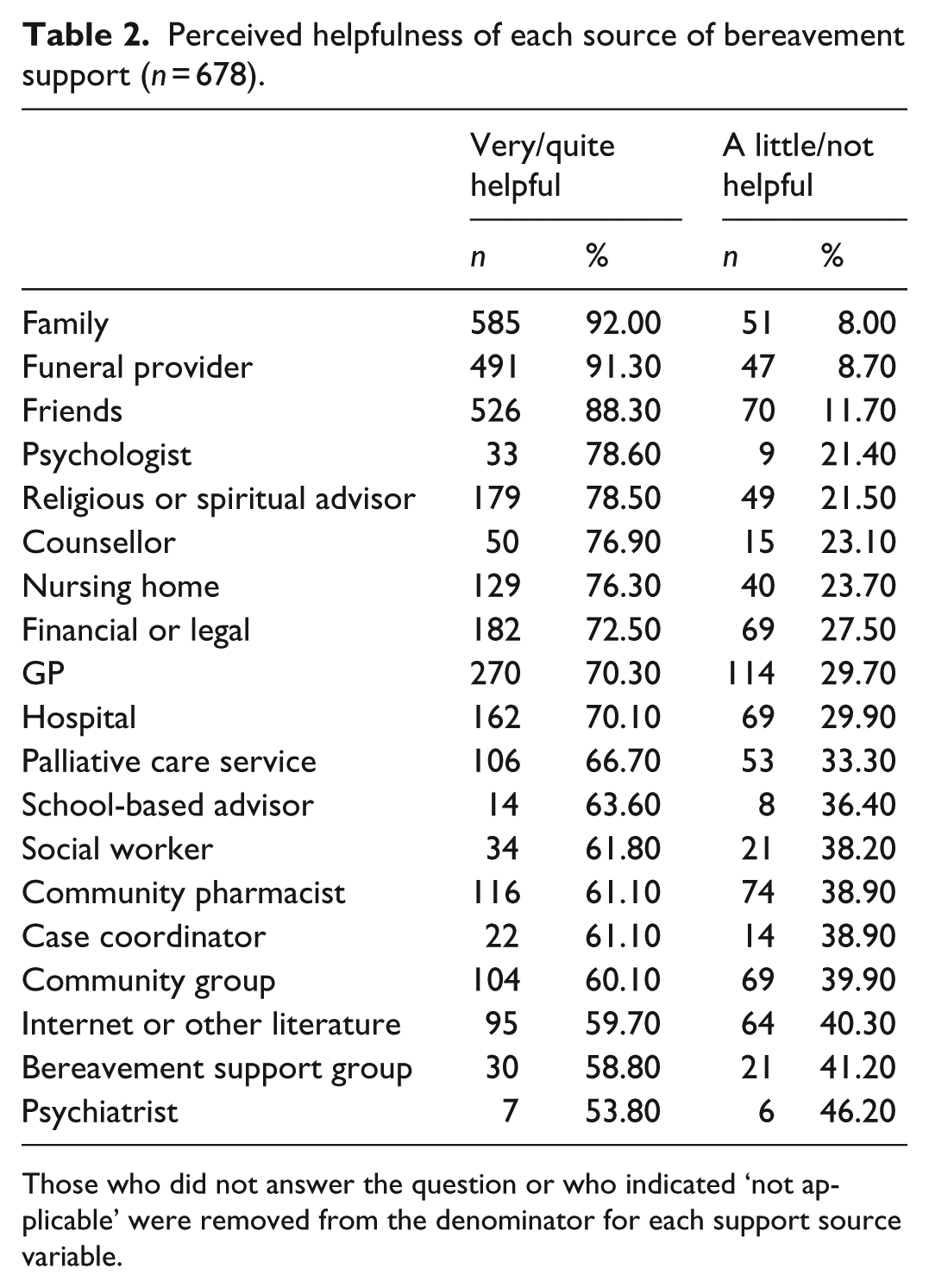
Those who did not answer the question or who indicated ‘not applicable’ were removed from the denominator for each support source variable.
Types of helpful bereavement support
About 80% of respondents provided at least one reason for experiencing helpful support. Using the SPS framework, the concepts ‘reassurance of worth’ and ‘opportunity for nurturance’ were not included as none of the responses aligned with these concepts in this particular sample. A summary table, providing examples of the codes generated and the frequency with which each functional type of support was endorsed by the sample, is shown (Table 3).
Source and corresponding type of functional support endorsed as helpful.
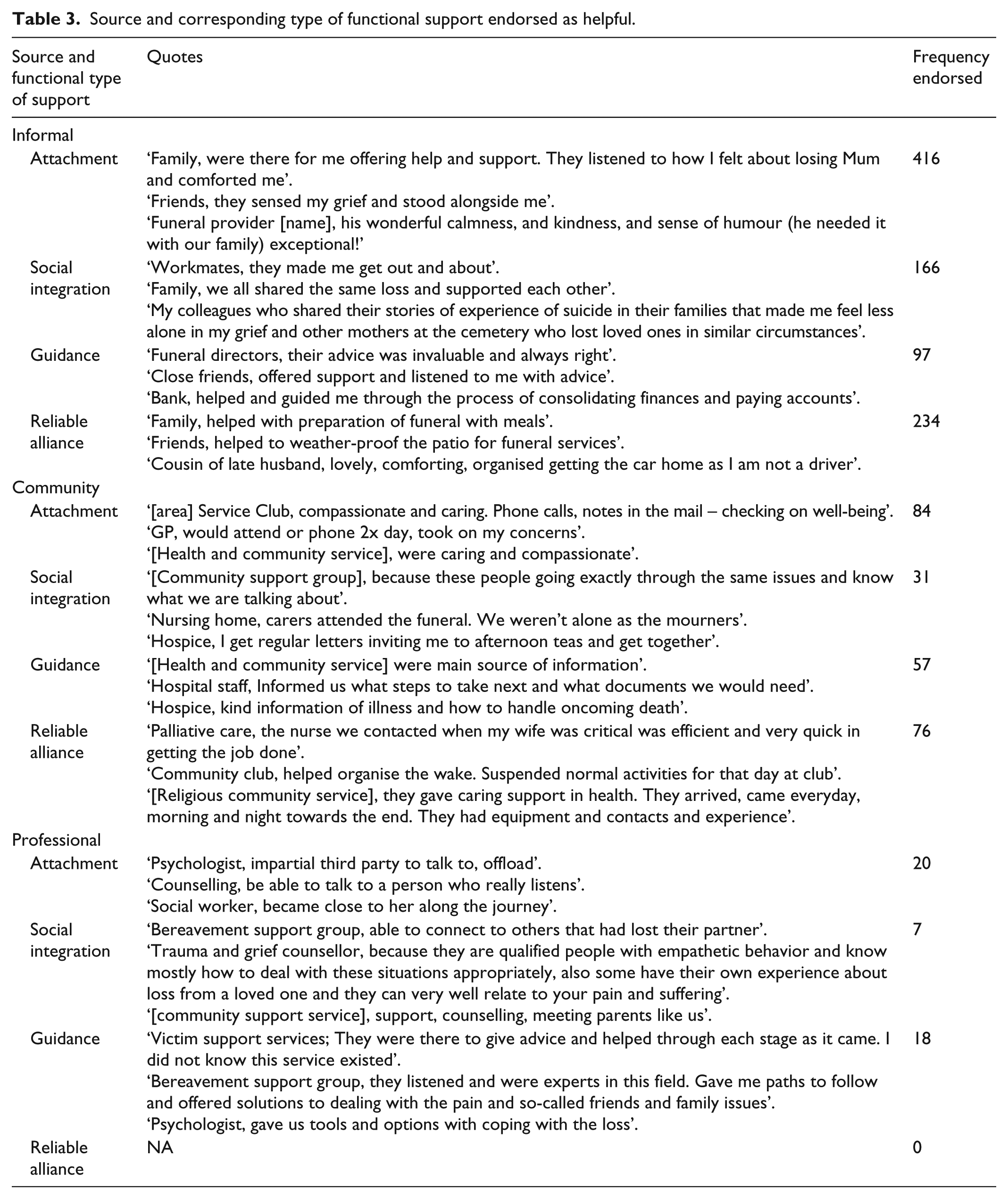
In the informal sources of support, attachment was the form of social support most frequently endorsed as helpful by respondents, followed by reliable alliance and social integration. Guidance came last in the informal sources but became more important in the other two sources. Within the community sources of support, attachment and reliable alliance were still prominent followed by guidance, while in the professional sources, guidance was as frequent as attachment (Table 3).
Types of unhelpful bereavement support
Fewer respondents provided comments on unhelpful sources compared to helpful sources (23.6% vs 78.6%). Table 4 provides examples of the frequency with which each of the five themes (Absence, Insensitivity, Poor Advice, Lack of Empathy and Systemic Hindrance) was endorsed by the sample.
Source and corresponding type of support endorsed as unhelpful.
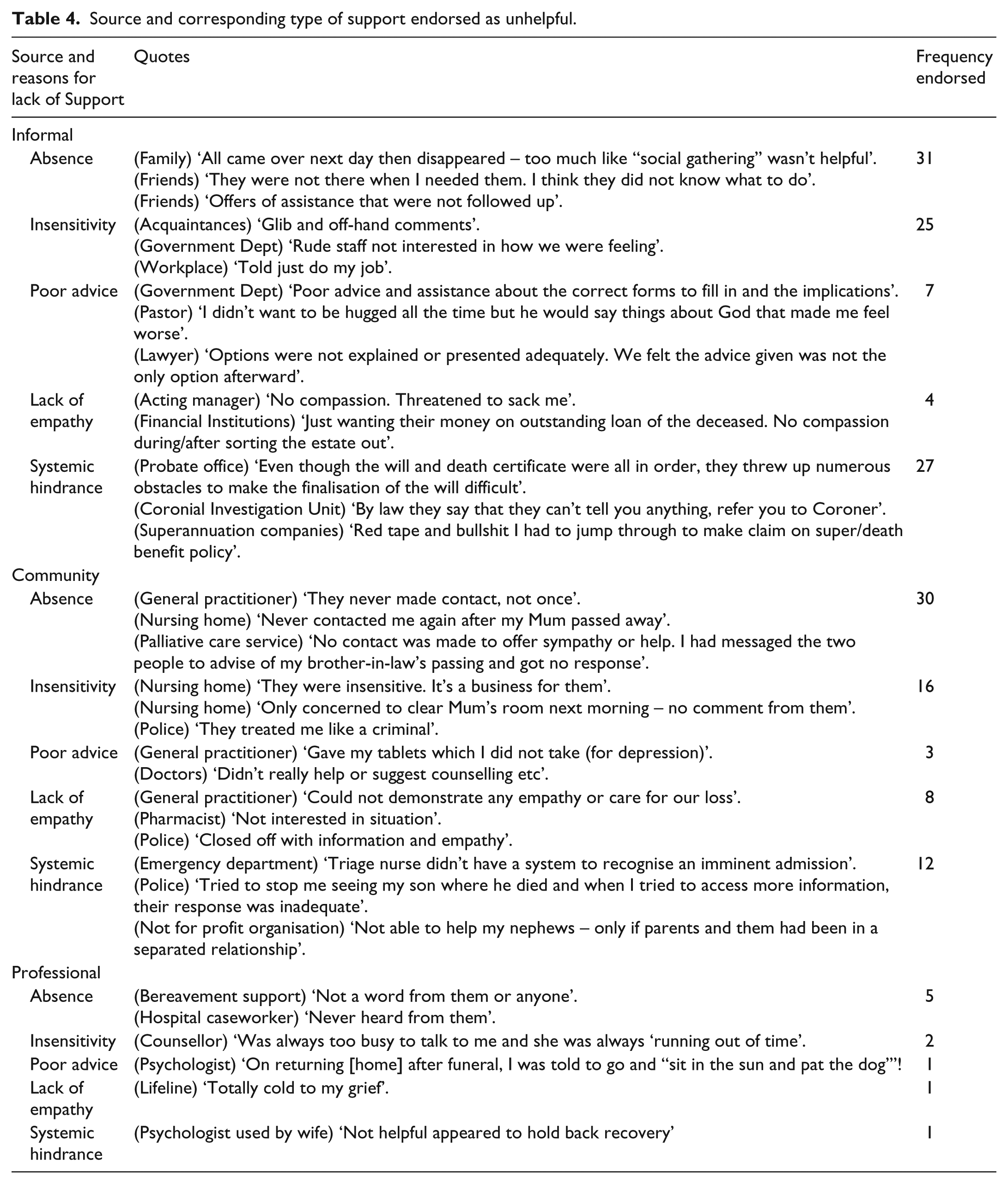
Absence (mainly by family/friends), insensitivity and systemic hindrance (mainly by financial and legal entities) were the most prominent themes in the informal sources. Similarly in the community sources, absence and insensitivity from doctors, health services and nursing homes were highlighted (Table 4).
Discussion
Compared to existing literature, this study presents a more nuanced account of the role of both sources and functional types of social support for bereavement, in terms of the reasons why the supports accessed by a population-based sample of bereaved people were perceived as helpful or unhelpful. While about 90% of respondents listed family and friends as providers of support, we had previously lacked detail about what made this source of support helpful. This is almost inevitable in surveys where it is easier to be specific in listing professional care providers than the myriad of small contributions that come from friends, family and neighbours. 10 Certainly, researchers who studied informal networks of care for people dying in the community found they had to persist to identify the contribution made by informal caregivers. 29
As expected, the most frequently used sources of support were those in the informal category, such as family and friends, and were deemed mostly helpful.8,11 What is unexpected is that funeral providers came next as most helpful and this is worthy of further investigation because of the valuable role they can play as part of the existing networks. While the professional sources were the least used, they had the highest proportions of perceived unhelpfulness (33%–46%). In particular, a third did not find palliative care services helpful and this is highlighted in the latest findings from this survey showing that just half of the bereaved had a follow-up contact from the palliative care services at 3–6 weeks, and only a quarter had a follow-up at 6 months, and that the blanket approach to bereavement support adopted by the services was deemed unhelpful. 30
Most health professionals have little exposure to evidence-based grief information and some draw upon outdated and ineffective models when working with bereaved clients.31 –34 The higher levels of professionals reported as unhelpful could also reflect higher expectations of the care they should offer. But evidence suggesting that inappropriate referrals for intervention may lead to worse outcomes in bereavement should also be remembered.25,35 Early, particularly unrequested, referrals to a counsellor have the potential to problematise grief and compromise the support that could be offered by existing networks – grief is seen as a problem demanding professional intervention.
Using the SPS framework, the concepts exhibited by this study sample were as follows: attachment and social integration which fall in the non-assistance related functions of social ties, while reliable alliance and guidance fall in the assistance-related functions. 27 In the informal sources of support, the findings revealed that attachment (emotional or affectionate bond, often provided by spouse/partner or close family) was the form of social support most frequently endorsed as helpful by participants, suggesting that the majority of bereaved individuals value this relational bond and emotional support from those closest to them. This was followed in terms of frequency by reliable alliance (tangible assistance such as providing meals and transport often offered by family members) and social integration (perceived sense of belonging often provided by friends). These findings are supported by previous research, which found that satisfaction with practical support in the months following loss predicted favourable bereavement outcomes, and that receiving practical support helps buffer the detrimental effects of stress as it reduces the situational demands of the individual.3,36 In addition, receiving tangible aid conveys to the individual that they are valued by their significant others which then bolsters their self-esteem and their sense of worth.
Guidance (advice and information) came last in the informal sources possibly because the bereaved prefer to obtain this from health professionals, who are equipped with the skills and knowledge though the advice and information were not necessarily about bereavement. 37 They also might like to receive this guidance from others who have experienced a similar loss rather than the general friends and family. 38 This was supported by guidance becoming more important in the community and professional sources: within the community sources of support, attachment and reliable alliance were still prominent followed by guidance, while in the professional sources, guidance became equal to attachment, but as expected there was no presence of reliable alliance.
In examining the unhelpful support, it seems that feeling unsupported was more than just the absence of support. While people did mention the absence of support, they also mentioned receiving insensitive comments and unwanted advice. However, fewer bereaved people had experienced unhelpful support (compared to helpful support) and that was mainly from government, financial and legal institutions.
Although the SPS framework is about social support rather than professional support, we took more of a social and public health approach to these care networks, both formal and informal, and considered all service providers as already existing members of communities, rather than placing them outside of these communities. This is supported by Horsfall et al. who explained that ‘In reality of course, especially in regional and rural areas, members of formal networks are also members of the community. They live, work, and play alongside people who are not necessarily providing a “service”’ (pp. 335–336). 39 It is worth noting that three out of four funeral service providers whose clients responded to this survey were in regional areas. This is the narrative that would operationalise the concepts of the public health approach and community capacity building through the compassionate communities approach. Horsfall et al. 39 called for better partnerships between such informal and formal caring networks, within the public health approach to end of life care. These partnership approaches to community support strengthen the capacity of the whole community to respond to dying, death and loss providing synergies that enhance both formal and informal efforts for not only addressing the comorbidities of grief but also enhancing health and well-being.
In addition to improving emotional well-being and reducing isolation, research in the United Kingdom has shown that a compassionate communities approach can reduce health service usage and ultimately result in significant savings for health services.40,41 Therefore, communities need greater support to adopt a systematic approach to developing and mapping their own asset networks. There are numerous fruitful ways they might achieve this: through implementing suggested strategies such as the Compassionate City Charter or using Healthy End of Life Program (HELP) resources; building public policies that support dying, death, loss and grief; creating supporting environments and in particular social supports from workplaces and schools; strengthening existing community action; and developing personal skills in these areas while reorienting the existing health system towards a stronger and more enabling community and health services partnership.42,43
Implications for research and practice
The implications for further research suggested by these findings indicate that we might usefully trial which elements of community development and support are universally important and which other elements are conditional upon regional and other social factors. This is not merely a call for greater evaluation of these approaches – evaluation of community development models similar to compassionate communities are commonplace in health promotion literature in general. 44 Rather it will be crucial to identify the essential professional or service elements for a programme of support that are best able to build upon local helping networks. In other words, more research is needed in identifying a range of useful practice models that connect health and social care services with local neighbourhoods and cultural life such as workplaces or schools. Evaluation studies will be only one element in a range of other essential and broader social research tasks (ethnographic studies, observational work, community policy audits, etc.) required for this programme style of development.
Furthermore in practice, we expect that members of the networks that support a dying relative or friend will continue to support each other during bereavement, unlike formal services where there is often a disjunction between the palliative care and bereavement teams. 30 This continuity of relationship matters and it is important to talk about the person who has died with others that have known the deceased. Compassionate communities provide this opportunity in the face of the fragmentation that characterises late modern society. 45
Further implications for practice relate to operationalising how to offer professionalised services to those who would most benefit, while not providing these services unnecessarily to those who are supported within their natural support networks. This is a key challenge of the assets-based approach and requires further research, policy and practice investment. Implicit in this is an important question about how this balance will be achieved. Should professional services be making decisions about the assets to be involved? Or is this more properly a decision to be negotiated by the bereaved person and all involved in the support network?
In terms of what levels of bereavement care should be provided and to whom, we have attempted to offer some directions in our previous article, 8 but more research is warranted. Our survey was constructed to provide information on the population-based experiences of bereavement, including the extent of the alignment of bereavement risk and support needs. Using the validated PG-13 (Prolonged Grief Disorder Scale) meant that we were able to determine a population rate of prolonged grief disorder of 6.4% in this sample. In addition, the low- and moderate-risk groups could be distinguished on the basis of PG-13 scores as well as the sources of support (mental health professional sources for high risk, community support for moderate risk and family and friends for low risk). In addition, the profiles of the bereaved provided a context for the scores: low scores typically arose from losses that were expected and less disruptive to daily routines (e.g. the death of an aged parent), moderate scores typically arose from deaths that were both expected and everyday-disruptive (e.g. the death of an ageing and ill partner) and high grief scores typically arose from deaths that were both unexpected or resisted and disruptive (such as a child or a younger spouse).
Limitations
The limitations of drawing on data from this anonymous survey have been highlighted in previous published findings from the survey, namely, that the study sample is not a random sample of the general bereaved population, but it nevertheless compares well with the UK mortality follow-back survey in terms of its demographic composition.8,30,46 The low response rate in this study is in line with others who relied on postal surveys with no reminder follow-up, acknowledging that those who did not respond may have had different experiences to those reported in this study. 47 The selection of respondents from funeral providers’ database may have influenced the significant number reporting support from these providers. Although we were able to use the SPS framework to code the functions of social support, there is no comprehensive model of types of unhelpful supports, which is why we used inductive content analysis.
Other methods of qualitative data collection (e.g. interviews, focus groups) usually allow the opportunity for clarification of meaning or for probing of answers to gain depth in the participant response; this was not possible here as participants provided comments on a self-completed questionnaire. However, the use of open response questions in surveys is increasingly being advocated as a means of enabling respondents to voice their opinion on the topic and is particularly suitable for a large sample size as in our study (n = 678). 48
Conclusion
This is the first study to quantify the amount of support received by the bereaved from their own social networks, how this support works and why it may work. We argue, on the basis of our findings, for the importance of adopting a primary public health approach to support the majority of bereaved people, as this care is already provided in community settings.
Although this conclusion may seem rather obvious in most health policy and practice fields, it is important to note that, for the field of bereavement policy and practice, a public health approach is in its infancy. Furthermore, most research and practice development have to date been focussed on acute care models of therapeutic intervention and not, we emphasise, with a population approach to grief. Our study has revealed that most care comes from people already involved in the everyday lives of those recently bereaved. These people are assets already in place, contributing to each other’s resilience. Some of them are healthcare practitioners contributing through their everyday activities, not bereavement programmes per se. In providing bereavement care, it is therefore prudent to support these ‘everyday assets’, ensuring that their care is recognised, appreciated and not disrupted by overreach from professional services. 10 These assets will complement quality bereavement care that identifies and offers counselling and therapy to those who need it.
Much of the compassionate communities approach has been focussed on end of life care for ageing and dying, and it needs to be extended to bereavement. This study has provided further empirical evidence of the need for more community development approaches such as those exemplified by the compassionate communities movement in palliative care – developing these not solely for the direct end of life care context but also for the journey of grief and bereavement during and after those circumstances.
Footnotes
Acknowledgements
The authors acknowledge the financial support of the WA Cancer and Palliative Care Network, Health Department of Western Australia; the cooperation of funeral providers who assisted with the recruitment of participants, and the bereaved families who agreed to complete the survey and contributed to our understanding in this field. Special thanks to Denise Howting who assisted with the quantitative analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Department of Western Australia.