
Abstract
Introduction:
This study aimed to evaluate the potential value of placental anatomic features and various types of normal and abnormal cord insertion types in predicting adverse maternal-fetal outcomes in singleton pregnancies. We also tried to assess the association between these outcomes and various types of placental cord insertion.
Method:
This prospective observational study was performed on singleton pregnancies. For each patient placental features including diameter, thickness, type of cord insertion, and the shortest distance between the cord insertion point and placental edge were recorded. The relationship between these factors and the development of multiple adverse pregnancy outcomes including preterm labor, intrauterine fetal death (IUFD), and the rate of neonatal intensive care unit (NICU) admissions were evaluated and reported.
Results:
Overall 308 patients were enrolled in the study. Smoker mothers had significantly smaller placentas (P-value = .008), and those with lower diameter placentas were more likely to suffer from IUFD (P-value = .0001). Shorter placental cord insertion distances led to more episodes of preterm labor (P-value = .057). Eccentric-type placental cord insertion was significantly associated with the development of preeclampsia (P-value = .006).
Discussion:
Abnormalities in placental diameter and cord insertion can lead to significant maternal-fetal complications including preterm labor, IUFD, and preeclampsia.
Introduction
In human pregnancies, the cord connects the fetus to maternal circulation through the placenta. Placental cord insertion sites can be classified as normal and abnormal; central and eccentric types are considered normal while velamentous and marginal site insertion types are classified as abnormal.1-3 In velamentous type umbilical vessels insert directly into amnion/chorion membranes before reaching placental mass (thus lacking the protection of Wharton’s Jelly) 4 in marginal type cord inserts into the edges of the placental mass.1,2 The prevalence of these abnormal types has been reported to be around 0.5–2.4% and 8.5% among all pregnancies in different studies.4 -7 This rate is higher in pregnancies conceived with the help of assisted reproductive methods 8 and those with multi-fetal pregnancies. 9
Previous studies have shown that velamentous type placental cord insertions (VCI) are associated with worse pregnancy outcomes,4 -6,10-12 including but not limited to pregnancy-induced hypertension, placenta previa, vasa previa, reduced birth weight, preterm birth, prenatal intrauterine death, and emergency cesarean deliveries.1,6,13-16 While there is little doubt about the clinical importance of VCI the significance of marginal insertion type (MCI) is less clear and more controversial, with 1 study showing that these pregnancies are not at risk of adverse perinatal outcomes. 17 A recent systematic review 1 of 17 published studies in singleton pregnancies could only find a strong relationship between rates of emergency cesarean deliveries and abnormal cord insertion (mostly velamentous type); lack of standard diagnostic definitions and heterogeneous classification of abnormalities were major obstacles in comparing similar studies. Another study showed that placental cord insertion distance is neither predictive of fetal growth restriction nor related to fetal birth weight, it also had no impact on adverse perinatal outcomes and was only associated with more Neonatal Intensive Care Unit (NICU) admissions. 18
One other area that has seen some important disparities in practice recommendations is the role of ultrasound in diagnosing placental cord abnormalities antenatally. American Institute of Ultrasound in Medicine suggests describing placental cord abnormalities in each trimester while the International Society of Ultrasound in Obstetrics and Gynecology is against reporting any abnormality during the first 2 trimesters.17,19-22
It has been shown that the health of the neonate at term is directly related to the normality in placental growth and anatomy. As the placenta is an organ that undergoes the same intrauterine stress as the fetus its features can help determine the health status of a pregnancy. So measuring parameters such as placental thickness or diameter can help assess many of the intrauterine disease conditions that can affect the fetus. For example, conditions like hydrops fetalis can lead to increased placental diameters and thickness through induction of edema, whereas conditions like preeclampsia or intrauterine growth restrictions can lead to thinning of the placenta. 23
Despite this, only a few studies have evaluated the relationship between placental anatomy and pregnancy outcomes24-26 and the relationship is still not clear with most of the evidence being inconclusive, for example, there are conflicting reports ranging from weak correlation to strong positive relationships between adverse maternal-fetal outcomes and placental thickness measurements.23,27-29 It should also be emphasized that fewer studies have evaluated the role of placental diameter in predicting adverse pregnancy outcomes and evidence in this regard is very limited and mostly low-quality. It should be noted that most studies have only sought the correlation between placental measurements and gestational age and not maternal-fetal outcomes. Given that placental anatomic features can be measured with a high degree of precision in the antenatal period establishing a relationship between these features and adverse outcomes can lead to more timely diagnoses and interventions.
Given all the uncertainties surrounding this important obstetric topic we sought to assess the relationship between anatomic placental features, various types of normal and abnormal cord insertion types, and the fetal and maternal outcomes; plus evaluating the possible relationships between outcomes and cord insertion distance quantitatively. This prospective analysis enrolled singleton pregnancies in a series of patients at a teaching hospital in Tehran, Iran.
Method
Study Setting
This was a prospective cross observational enrolling consecutive singleton pregnant patients who were 18 years or above and were admitted for delivery in a teaching hospital affiliated with the Iran University of Medical Sciences (IUMS) in Tehran, Iran. This study was performed between June and August of 2022.
Eligibility Criteria
All patients 18 years old and older with singleton pregnancies who were admitted for delivery of their pregnancies were enrolled in the study. Pregnancies with multiple fetuses, chromosomal abnormalities, and known congenital defects were excluded.
Data Gathering
After delivery placenta of each patient was grossly examined and anatomic features including diameter, thickness, type of placental cord insertion, and distance between cord insertion edge and placental edge (placental cord insertion distance) were recorded based on the visual inspection. For each patient’s maternal demographic information including age, parity, any previous medical condition (e.g. Diabetes Mellitus or hypertension), and information regarding past pregnancies was obtained using patients’ medical records. Maternal-fetal outcomes recorded in the study included gestational age at delivery, mode of delivery, birth weight, 5 and 10-minute Apgar Scores, presence or absence of gestational diabetes, hypertension, preeclampsia, post-partum hemorrhage, preterm labor or premature membrane rupture, need for NICU admission and intrauterine fetal death (IUFD).
Ethical Consideration
The Ethics Committee of IUMS and the Institutional Review Board at the hospital approved the study design, all patients enrolled in the study only after signing an Informed Consent Form and their data was unidentifiable throughout the study period.
Statistical Analysis
For each continuous variable, a Shapiro-Wilk test was performed to evaluate the normality of data distribution. Continuous variables were presented as the mean ± the standard deviation (SD) when data was normally distributed and with median and interquartile ranges where data were not normally distributed. Categorical variables were described as percentages. Differences in categorical and continuous variables were assessed using the χ2 test and independent t-test or Mann Whitney U test (when applicable), respectively. A P-value of less than .05 was considered significant. All statistical analyses were conducted with R Programming language (R for Windows, version 4.1.3, Vienna, Austria), R Studio version 1.1.463 (Posit PBC, Boston, MA, United States) utilizing the “tidyverse” statistical package.
Results
Overall we identified 308 eligible patients who entered the final analysis. Demographic features of the cohort are presented in Table 1. 84 (27.4%) patients were nulliparous and 94% (n = 290) of the cohort population had either central or eccentric type cord insertion. The prevalence of marginal and velamentous types were 2% (n = 7) and 4% (n = 11) respectively. Placental observation revealed no notable anomalies in 81.2% (n = 250) of the cases, placental calcifications were present in 10.4% (n = 32).
Demographic and Basic Clinical Features of Patients Enrolled in the Study.
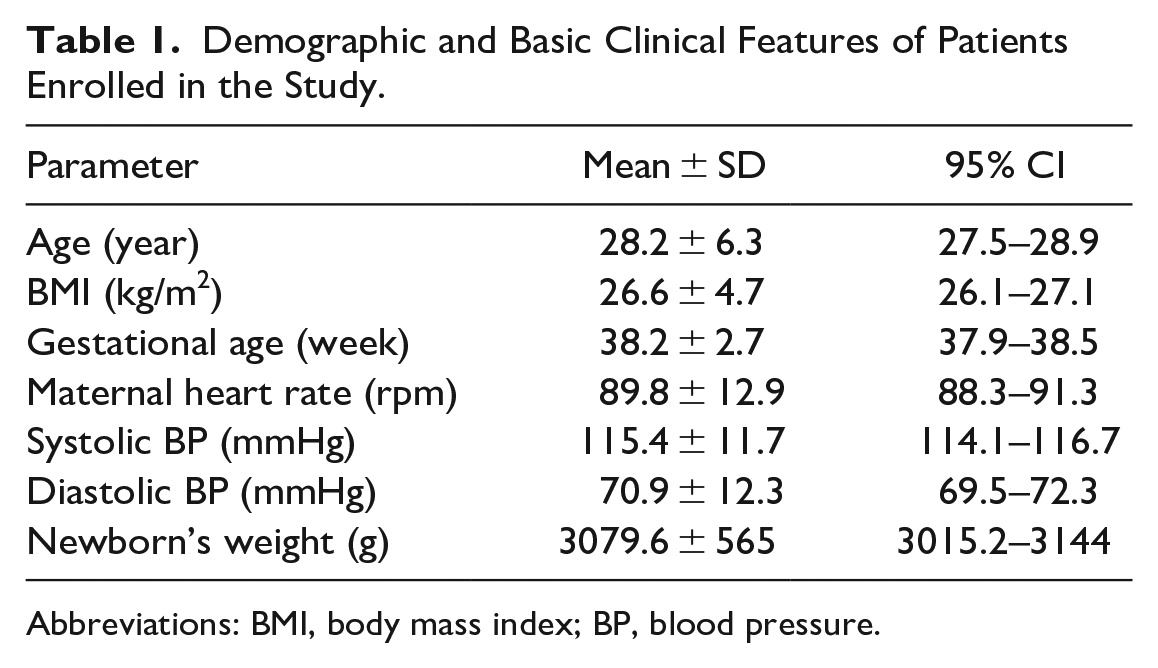
Abbreviations: BMI, body mass index; BP, blood pressure.
0.9% (n = 3) of pregnancies were the result of in-vitro fertilization. Gestational diabetes was the most common complication among the maternal population (14.6%, n = 46), 5.8% (n = 18) had gestational hypertension, 3.6% (n = 11) of which developed preeclampsia. 60.1% (n = 185) of deliveries were vaginal and 93.5% (n = 288) of neonates presented in cephalic position. In 86.7% (n = 267) of neonates 5-minute Apgar score was 9/10, 10 minute Apgar score was 9/10 among 95.1% (n = 293), none of the newborns had a 10-minute Apgar score of lower than 7. 9.4% (n = 29) of newborns were preterm, rate of IUFD was 2.3% (n = 7) in the cohort, eventually 11.7% of newborns required NICU admission (n = 36).
None of the assessed risk factors had any significant relationship with placental thickness. (Table 2, Figure 1) Mothers with a history of smoking had significantly lower placental diameters (P-value = .008, median placental diameter of 16.0 cm in smokers vs median placental diameter of 19.4 cm in non-smokers). IUFD (P-value = .0001, median placental diameter of 19.5 cm vs 15.2 cm) and instances of NICU admission (P-value = .0499, median placental diameter of 18 cm vs 19.5 cm) were both significantly more prevalent in pregnancies with lower placental diameter. Median placental diameter had no significant difference in patients with gestational diabetes, gestational hypertension, preeclampsia, pregnancy being the result of IVF procedure, premature rupture of membranes, post-partum hemorrhage, and pre-term labor vs those without the mentioned complications (Table 2, Figure 2).
Assessing the Statistical Association Between Placental Diameter, Placental Thickness, Shortest Placental Cord Insertion Distance and Type of Placental Cord Insertion and Various Maternal Fetal Adverse Outcomes and Risk Factors.
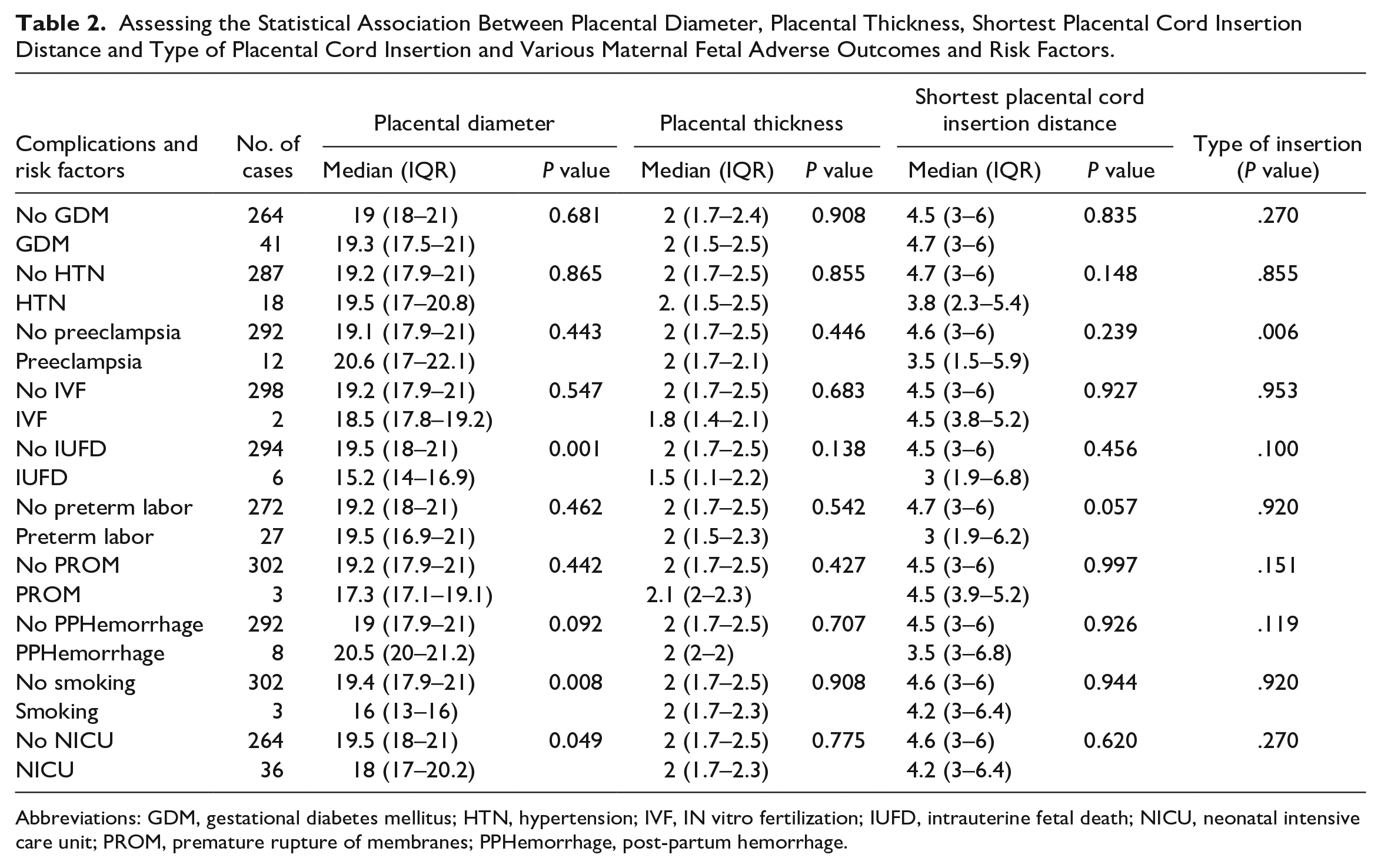
Abbreviations: GDM, gestational diabetes mellitus; HTN, hypertension; IVF, IN vitro fertilization; IUFD, intrauterine fetal death; NICU, neonatal intensive care unit; PROM, premature rupture of membranes; PPHemorrhage, post-partum hemorrhage.
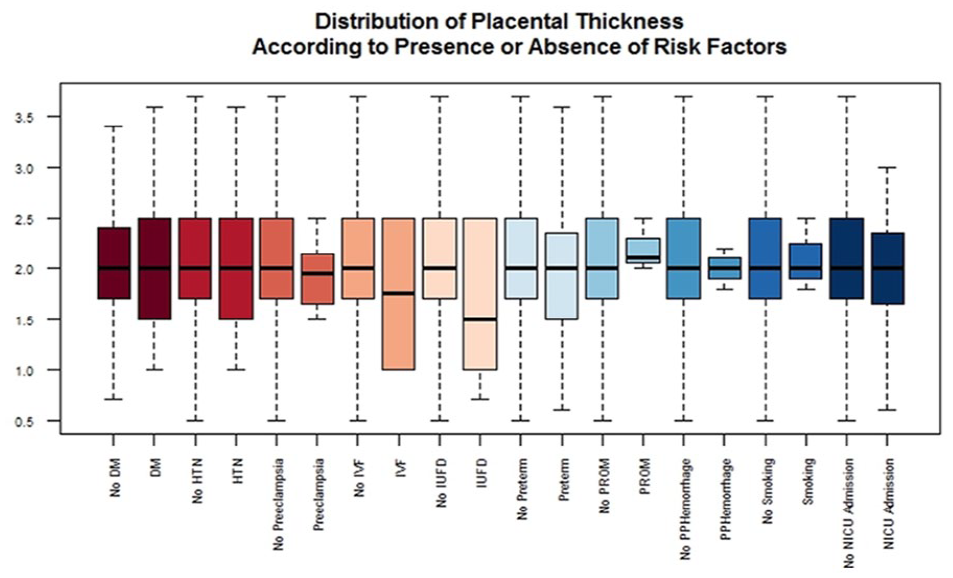
Boxplot of placental thickness measurements based on presence or absence of various complications and risk factors.
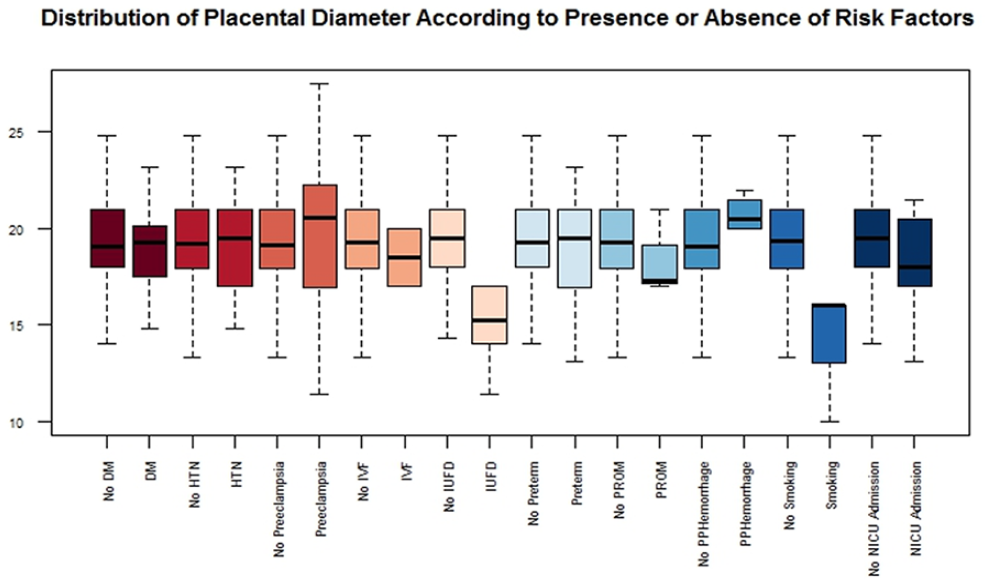
Boxplot of placental diameter measurements based on presence or absence of various complications and risk factors.
The median shortest distance between the placenta and cord, median placental diameter, and median placental thickness were 4.5 (3–6) cm, 19.2 (17.9–21) cm, and 2.7 (1.8–2.5) cm respectively. There was no significant statistical relationship between cord insertion distance and history of gestational diabetes, gestational hypertension, preeclampsia, pregnancy being the result of IVF procedure, the occurrence of IUFD, premature rupture of membranes, NICU admission, post-partum hemorrhage, and history of smoking. We identified a weak relationship between cord insertion distance and preterm labor (P-value = .057, median cord insertion distance of 3.0 cm in prematurely born babies vs 4.7 cm in term babies) (Table 2, Figure 3).
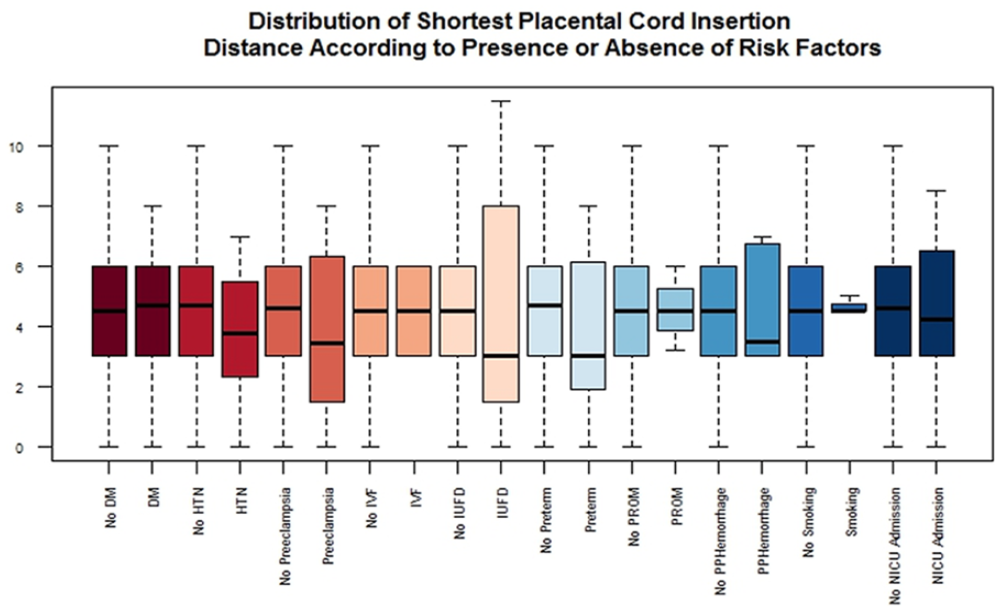
Boxplot of shortest placental cord insertion distance measurements based on presence or absence of various complications and risk factors.
Of the assessed risk factors only the occurrence of preeclampsia was associated with the type of placental cord insertion with mothers who had eccentric type insertion suffering from more bouts of the disease. Also, mothers with velamentous type insertion went into labor significantly earlier than those with other types of insertion. (Mean gestational age at the time of delivery of 39, 38.8, 37.3, and 39.8 weeks for central, eccentric, velamentous, and marginal types respectively, P-value = 0.031). Neonatal weight was not associated with the type of placental cord insertion (Table 2).
Discussion
In the current cohort of patients, we reported 2 sets of findings related to placental anatomy; general anatomic features of the placenta (including diameter, thickness, and any anomalies) and features related to placental cord insertion (including shortest placental cord insertion distances and type of cord insertion). In the anatomic features, we could not find any relationship between placental thickness and any of the adverse maternal/fetal outcomes; smoking was also not associated with placental thickness measurements. An important finding of the current study was that smoking was directly related to lower placental diameters, pregnancies in mothers with lower diameters were significantly more likely to lead to an IUFD episode or more NICU admissions. When assessing cord insertion, we found an association between shorter placental cord insertion distances and instances of pre-term labor. Among various types of cord insertion pregnancies with eccentric type insertions had a significantly more probability of being complicated with episodes of preeclampsia. While VCI was not associated with instances of preterm labor mothers with this type of insertion went into labor significantly earlier.
We showed that a lower placental diameter was significantly associated with the occurrence of IUFD and it was also marginally associated with more NICU admissions. Lower diameters were associated with smoking, although it must be noted that in both instances our sample size was relatively small, so caution is advised when interpreting these findings, however given the reports of previous studies on morphologic features of the placenta we expect to see similar results in bigger populations. 29 More studies concerning placental thickness have been performed previously23-28 and while we could not find any relationship between outcomes and placental thickness measurements this is probably because we only had 6 patients with thicknesses higher than the 95th percentile for gestational age. Thompson et al 30 could not find an association between placental thickness and pregnancy outcomes but in some other studies,31-35 this relationship specifically between decreasing thickness and IUFD, small for gestational age (SGA), and hypertensive disorders has been shown. For example, in a 2021 study, Shinde et al 36 demonstrated a significant positive correlation between birth weight and placental thickness in second and third trimesters. Increasing thinness can also be a sign of maternal/fetal disease as is shown in a study conducted by Ehleres et al. 37 In this study, it was demonstrated that GDM affects the development of the placenta through hyperglycemia and other metabolic or endocrine mechanisms, such as insulin resistance. Placental overgrowth is a typical occurrence, but it is also accompanied by structural irregularities like villous immaturity and vascular dysfunction that may counteract the advantages of a larger placenta in promoting fetal growth.
The association of placental cord insertion distance and pregnancy outcomes was recently evaluated in a study 18 which reported that insertion distances are only mildly related to episodes of NICU admission and are not related to or predictive of any other type of adverse outcomes. Our findings are mostly in line with these results as we also found a mild (not significant) association with preterm labor. IUFD and maternal complications were not associated with insertion distances and also insertion measurements were not predictive of NICU admission episodes.
Previous studies assessing the relationship between cord insertion types and adverse pregnancy outcomes have mostly used non-standard classification approaches, using heterogeneous definitions and making comparisons between non-uniform groups. (e.g., comparing velamentous with a mix of velamentous and marginal patients). In this study, we sought to eliminate this problem by making direct comparisons between each of the 4 insertion categories. Results from previous studies have been conflicting in this area with contradicting reports about cord insertion abnormalities and risk of SGA babies, preterm labor, and IUFD.5,38 Also, a study specifically assessing the marginal type insertion could not find an association with adverse pregnancy outcomes. 17
While systematic reviews1,16 have shown an association between abnormal cord insertion and complications such as emergency cesarean deliveries and IUFD we could not find any relationship between VCI and these complications which is mostly because our study was underpowered in assessing these features. We acknowledge that our sample size of 7 patients with VCI is small and any result from this cohort cannot be the basis of decision-making in bigger populations.
Overall, what we demonstrated was that anatomic features of the placenta like diameter and cord insertion distances can have some important effects on adverse outcome developments. Our study’s main strength was that we had a clear and well-classified group of patients whose risk factors, complications, and outcomes were well documented, our missing data was scarce and we utilized exact manual measurements after delivery to report anatomic features of each patient’s placenta. The biggest limitation of our study was our relatively small sample size and given the small set of patients with VCI or MCI our study was not powerful enough to demonstrate impactful results. One important area that needs further evaluation is the correlation between ultrasonography measurements of placenta antenatally and maternal fetal outcomes and whether it is possible to use placental measurements instead of weight when weight data is unavailable. We recommend that in future studies an attempt be made to evaluate this.
Conclusion
Placental cord abnormalities and placental anatomic features have a significant impact on the development of adverse maternal-fetal outcomes. Lower diameter placentas are associated with more IUFD and NICU admissions, shorter placental cord insertion distances are weakly predictive of preterm labor and eccentric-type placental insertions are related to the development of preeclampsia.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.