
Abstract
Purpose:
To investigate the effect of subclinical hypothyroidism on pregnancy outcomes of women early in their pregnancy with different thyroid-stimulating hormone levels and thyroid peroxidase antibody–negative status and to explore reasonable thyroid-stimulating hormone levels for subclinical hypothyroidism in early pregnancy.
Methods:
A total of 2378 women early in their pregnancy were studied retrospectively. The baseline characteristics were collected from medical records. Pregnancy outcomes were compared between the euthyroidism and subclinical hypothyroidism groups that were diagnosed by 2011 or 2017 American Thyroid Association guidelines. In addition, the effect of different maternal thyroid-stimulating hormone levels on adverse pregnancy outcomes was analyzed using binary logistic regression.
Results:
According to the 2011 American Thyroid Association diagnostic criteria of subclinical hypothyroidism, the prevalence of pregnancy outcomes was not significantly higher in the subclinical hypothyroidism group than in the euthyroidism group. However, pregnant women with subclinical hypothyroidism identified by the 2017 American Thyroid Association criteria had a higher risk of premature delivery (odds ratio = 3.93; 95% confidence interval = 1.22–12.64), gestational diabetes mellitus (odds ratio = 2.69; 95% confidence interval = 1.36–5.32), and gestational anemia (odds ratio = 3.28; 95% confidence interval = 1.60–6.75). Moreover, no differences in the prevalence of adverse pregnancy outcomes were observed between the mildly elevated thyroid-stimulating hormone group (2.5 < thyroid-stimulating hormone ⩽4.0 mIU/l) and the normal thyroid-stimulating hormone group (0.27 < thyroid-stimulating hormone ⩽2.5 mIU/l). The significantly elevated thyroid-stimulating hormone group (4.0 < thyroid-stimulating hormone < 10.0 mIU/l) had a higher prevalence of premature delivery, gestational diabetes mellitus, and gestational anemia than the normal thyroid-stimulating hormone group, even after controlling for potential confounding factors.
Conclusion:
A mildly elevated thyroid-stimulating hormone level or maternal subclinical hypothyroidism diagnosed by 2011 American Thyroid Association guidelines during early pregnancy in thyroid peroxidase antibody–negative women was not associated with adverse pregnancy outcomes. However, maternal subclinical hypothyroidism identified by the 2017 American Thyroid Association guidelines increased the risks of several adverse pregnancy outcomes in women untreated with levothyroxine. The 2017 American Thyroid Association guidelines could be more reasonable for the diagnosis of subclinical hypothyroidism in southern China.
Keywords
Introduction
Hypothyroidism in pregnancy has been shown to provoke many negative effects on pregnancy outcomes. Domestic and foreign guidelines indicate that overt hypothyroidism in pregnancy must be detected and treated urgently.1,2 However, when pregnancy copresents in the clinic with subclinical hypothyroidism (SCH), there is often a lack of clinical symptoms, and the risk of adverse pregnancy outcomes may increase. 3
In 2011, the American Thyroid Association (ATA) and the Chinese guidelines for the diagnosis and treatment of thyroid diseases in pregnancy and postpartum suggested that the upper limit of thyroid-stimulating hormone (TSH) in early pregnancy was 2.5 mIU/l. 4 According to these diagnostic standards, epidemiological investigations determined that the prevalence of pregnancy copresenting with SCH in the United States was 15.0%2,5 and 27.8% in China. 6 However, a number of follow-up studies have suggested that the diagnostic standard of SCH at 2.5 mIU/l in early pregnancy might represent an overdiagnosis and subsequent treatment.7,8 Thus, the ATA and Chinese Society of Endocrinology updated the reference upper limits of TSH in early pregnancy to 4.0 mIU/l by analyzing the latest prospective clinical study data.1,6,7,9 However, there is insufficient clinical evidence to confirm whether the standards recommended in the ATA guidelines are suitable for pregnant women in southern China.
The impacts of pregnancy with SCH on pregnancy and perinatal outcomes have not been clearly concluded to date. 10 Some investigators reported that SCH was not associated with adverse pregnancy outcomes.11,12 In a study of the relationship between SCH and the risk of premature delivery, a prospective cohort study showed that increased levels of TSH were not associated with premature delivery at 37 weeks of age. In contrast, other studies revealed that SCH may have adverse obstetric complications, including preterm delivery, pregnancy loss, and placental abruption.13–15 In support of an adverse impact attributable to premature delivery, data from a large prospective population-based study demonstrated when compared with the control group, the risk of premature delivery in the TSH >4.0 mIU/l group significantly increased before 37 and 34 weeks. When thyroid peroxidase antibody (TPOAb)-positive pregnant women were excluded, the study did not find any relationship between SCH and premature delivery. 16 The inconsistency of these studies might be related to the influence of different TSH cutoff set points and TPOAb levels on SCH, and many of the studies tended to focus on SCH patients with positive TPOAb. Thus, for pregnant women who are negative in the early stages of pregnancy, the relationship between different degrees of increased TSH and adverse pregnancy outcomes requires further study.
The overarching aim of this study was to investigate the effect of SCH on pregnancy outcomes of early pregnant women with different TSH levels who were TPOAb-negative according to 2011 and 2017 ATA guidelines and to explore a reasonable TSH level for SCH during early pregnancy in southern China.
Materials and methods
Participants
We report here on data from a retrospective analysis of pregnant women who underwent the first prenatal examination before 13+6 gestational weeks at the Guangzhou Red Cross Hospital and Zhujiang Hospital of Southern Medical University from January 2017 through December 2018. A total of 2378 TPOAb-negative pregnant women were included for comparison of thyroid parameters with baseline characteristics and pregnancy outcome data. The exclusion criteria for study participants were as follows: (1) evidence of previous thyroid disease, hypertension, diabetes, heart disease, or other major organ diseases; (2) family history of autoimmune disease, personal history of genetic disease; (3) current or previous treatment with levothyroxine or antithyroid drugs; (4) multiple pregnancies; (5) pregnancy via assisted reproductive technology; (6) TSH concentration higher than 10 mIU/l or less than the lower limit of the reference range (0.27 mIU/l); (7) FT4 concentration out of the reference range; and (8) anti-TPOAb levels higher than the upper limit of the reference value. In Figure 1, we illustrated in detail the inclusion/exclusion criteria with a flowchart. According to the diagnostic criteria of the ATA guidelines in 2011 and 2017, all participants were consecutively stratified into two groups: euthyroidism and SCH. According to the 2017 ATA guidelines and our exclusion criteria, all enrolled participants did not receive LT4 treatment. The study was approved by the Ethics Committee of Guangzhou Red Cross Hospital (No. 2021-169-01) and carried out in accordance with the approved guidelines. Written informed consent was obtained from all participants.

Flowchart of the enrolled pregnant women in the study.
Data collection
Fasting venous blood was collected for thyroid functions detection, including TSH, FT4, and TPOAb, at the first prenatal examination before 13+6 gestational weeks. In addition, peripheral venous blood was sampled between 24 and 28 weeks of pregnancy for oral glucose tolerance testing (OGTT) to screen gestational diabetes mellitus (GDM).
Details on maternal age, pregestational body mass index (BMI = weight(kg)/height (m 2 )), number of pregnancies, gestational age at delivery, neonatal birth weight, and obstetric and neonatal outcomes were obtained from medical records.
Diagnostic criteria
According to the 2011 ATA guidelines, the definition of SCH in early pregnancy was described as TSH >2.5 mIU/l with normal FT4 levels. However, the 2017 ATA guidelines recommended that SCH in pregnant women be defined as TSH >4.0 mIU/l with normal FT4 levels. In addition, TPOAb positivity was defined as a TPOAb value that was higher than the upper limit of the normal reference value, which was a TPOAb >34 IU/ml.
The definition of maternal and neonatal outcomes were as follows: premature delivery (a live birth before 37 weeks of pregnancy), GDM (plasma glucose level ⩾5.1 mmol/l at 0 h, ⩾10.0 mmol/l at 1 h or ⩾8.5 mmol/l at 2 h after a 2-h 75 g oral glucose tolerance test), gestational hypertension (systolic blood pressure ⩾140 mmHg and (or) diastolic blood pressure ⩾90 mmHg after 20 weeks of pregnancy), gestational anemia (peripheral blood hemoglobin concentration ⩽110 g/l, or hematocrit ⩽0.33), placental abruption (placenta partly or completely separate from the inner wall of the uterus before delivery), premature rupture of membrane (PROM, membrane rupture before the onset of labor), intrauterine growth restriction (IUGR, a fetal weight ⩽10th percentile for gestational age), low birth weight (a live birth weight ⩽2500 g), and neonatal asphyxia (regular spontaneous breathing cannot be established within a minute after delivery).
Statistical analysis
The data were analyzed by SPSS version 22.0 software. Data are presented as the mean ± standard deviation for normally distributed variables or median with interquartile range for non-normally distributed variables. Frequencies were exhibited for categorical variables. The basic characteristics or pregnancy outcomes of the participants were compared using the Mann–Whitney U test for continuous variables or chi-square tests for categorical variables. Moreover, binary logistic regression analyses were further performed to assess the odds ratios (ORs) and 95% confidence intervals (CIs) for adverse perinatal outcomes. p < 0.05 was considered statistically significant.
Results
Basic characteristics of pregnant women under different TSH levels
The basic characteristics of pregnant women and their newborns during early pregnancy under different TSH levels are shown in Table 1. According to the distribution of serum TSH levels in the women included, the median and 2.5th and 97.5th percentile values were 1.26, 0.33, and 3.73 mIU/l, respectively. Among women with TSH levels >2.5 mIU/l, 79.3% had TSH levels <4.0 mIU/l. Of all the enrolled women, the median age was 30 (27–33) years, the median gestational age at birth was 39 (38–39) weeks, and the median pre-pregnancy BMI was 20.4 (19.3–21.4) kg/m2. There was no significant difference found in the context of these characteristics for all three groups.
Baseline and demographic characteristics in all patients according to the thyroid function status.

BMI, body mass index; IQR, interquartile range; TSH, thyroid-stimulating hormone.
Non-normally distributed variables are expressed as median with interquartile range.
Categorical variables are expressed as percentages.
Maternal SCH diagnosed by the 2011 ATA standards was not related to adverse pregnancy outcomes
We explored the association of adverse pregnancy outcomes and maternal SCH defined by the 2011 ATA criteria. As shown in Table 2, there was no significant difference between the study groups in terms of GDM, gestational hypertension, placental abruption, PROM, IUGR, low birth weight, and neonatal asphyxia, even after adjustment for maternal age, pre-pregnancy BMI, number of pregnancies, and gestational age. A rising trend was observed in the SCH group for prevalence and the risk of premature delivery (p = 0.059) and gestational anemia (p = 0.058) in contrast to the euthyroidism group.
Association of maternal SCH and adverse pregnancy outcomes according to 2011 ATA standard.

Adjusted OR, adjusted for maternal age, prepregnancy BMI, number of pregnancies, and gestational age; ATA, American Thyroid Association; CI, confidence interval; ET, euthyroidism; GDM, gestational diabetes; IUGR, intrauterine growth restriction; OR, odds ratio; PROM, premature rupture of membrane.
Maternal SCH defined by the 2017 ATA standards was associated with several adverse pregnancy outcomes
We determined the association of adverse pregnancy outcomes and SCH according to the 2017 ATA guidelines. The results of binary logistic regression analysis are shown in Table 3. The prevalence of premature delivery (OR = 3.93; 95% CI = 1.22–12.64) was significantly higher than that of euthyroidism. At the same time, compared with the euthyroidism group, we also found that the prevalence and risks of GDM (OR = 2.69; 95% CI = 1.36–5.32) and gestational anemia (OR = 3.28; 95% CI = 1.60–6.75) were prominently higher in the SCH group.
Association of maternal SCH and adverse pregnancy outcomes according to 2017 ATA standard.
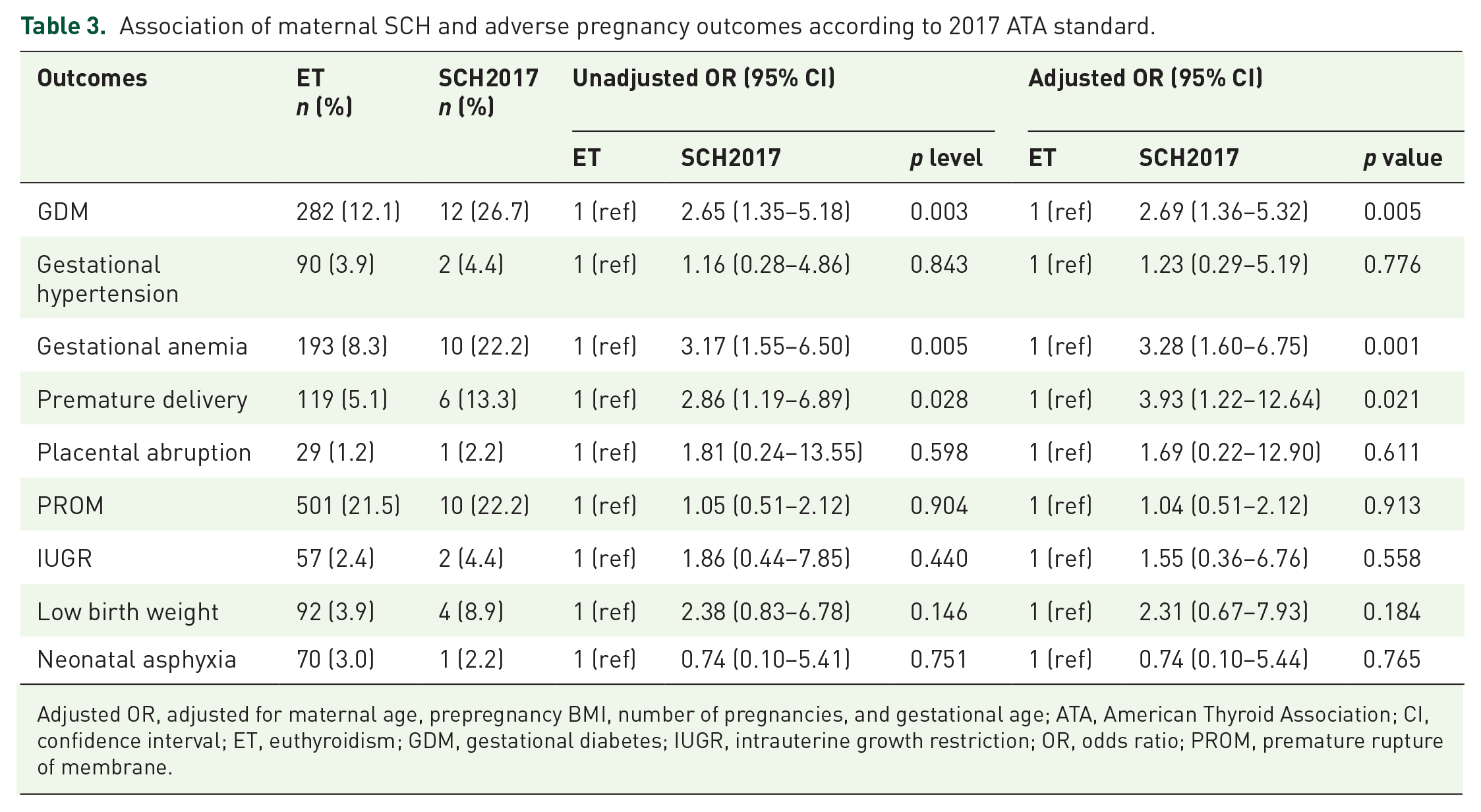
Adjusted OR, adjusted for maternal age, prepregnancy BMI, number of pregnancies, and gestational age; ATA, American Thyroid Association; CI, confidence interval; ET, euthyroidism; GDM, gestational diabetes; IUGR, intrauterine growth restriction; OR, odds ratio; PROM, premature rupture of membrane.
Association of different maternal TSH levels and adverse pregnancy outcomes
We further subdivided all participants into three groups according to TSH value [normal TSH group (0.27 < TSH ⩽ 2.5 mIU/l), mildly elevated group (2.5 < TSH ⩽ 4.0 mIU/l), significantly elevated group (4.0 < TSH < 10.0 mIU/l)], and then estimated the relationship between TSH status and adverse pregnancy outcomes. As depicted in Table 4, there were no significant differences in adverse pregnancy outcomes between the normal TSH group and the mildly elevated TSH group. However, the significantly elevated TSH group had a higher prevalence and risk of GDM (OR = 2.67; 95% CI = 1.35–5.29), gestational anemia (OR = 3.32; 95% CI = 1.61–6.82), and premature delivery (OR = 4.07; 95% CI = 1.26–13.14) than the normal TSH group.
Association of elevated maternal TSH levels with adverse pregnancy outcomes.

Adjusted OR, adjusted for maternal age, prepregnancy BMI, number of pregnancies, and gestational age; BMI, body mass index; CI, confidence interval; GDM, gestational diabetes; IUGR, intrauterine growth restriction; OR, odds ratio; PROM, premature rupture of membrane; TSH, thyroid-stimulating hormone.
p<0.05 (4.0 ⩽ TSH < 10.0 mIU/l versus TSH < 2.5 mIU/l).
Discussion
This study found that the upper limit of TSH in TPOAb-negative participants in early pregnancy in Guangzhou was 3.73 mIU/l, a value that was significantly higher than the SCH diagnostic cutoff point that was recommended by the 2011 ATA guidelines and was similar to the latest diagnostic cutoff point of the 2017 ATA guidelines. SCH with a mild increase in TSH levels in early pregnancy had no adverse effect on pregnancy outcomes. However, SCH pregnant women who were diagnosed by the 2017 ATA guidelines or identified with a significant increase in the TSH level exhibited a significantly higher prevalence and risk of premature delivery, GDM, and gestational anemia than euthyroid pregnant women after controlling for possible confounding factors. The 2017 ATA guidelines could be more reasonable for the diagnosis of TPOAb-negative SCH in early pregnancy in southern China.
TSH is the most sensitive index that reflects changes in thyroid function, and TPOAb is closely related to the thyroid autoimmune state. 17 It has been suggested that iodine nutrition status and the age of pregnant women may affect the relative levels of TSH and TPOAb.18,19 Pregnant women in this study came from southern China, where dietary iodine intake is relatively sufficient. There was no difference found in the context of age, gestational weeks, or gravidity of pregnant women. Therefore, this study excluded the possible impacts of these factors on TSH and TPOAb.
The upper limit of normal TSH for TPOAb-negative early pregnancy females in this study group was 3.73 mIU/l, which very closely approximated that of the 2017 ATA standard. Compared with the 2.5 mIU/l diagnostic cutoff point of TSH recommended by the 2011 ATA, the incidence of SCH according to the 2017 ATA standard was only 1.93%, which approximated that of studies in other countries.12,20 An increasing number of studies have suggested that the use of a TSH value of 2.5 mIU/l as the normal upper limit in early pregnancy might overdiagnose SCH in pregnant women.7,21
There is still insufficient evidence regarding SCH diagnosed at different cutoff points in early pregnancy and adverse pregnancy outcomes, especially for changes in thyroid function with TSH levels of 2.5–4.0 mIU/l. Some clinical studies have shown that SCH is closely related to adverse outcomes, such as hyperglycemia, hypertension, and anemia during pregnancy.22–24 A meta-analysis suggested that when compared with pregnant women with normal thyroid function, pregnancy abortion, placental abruption, PROM, and neonatal mortality of pregnant women with SCH were significantly increased. 3 However, these studies did not conduct a subgroup analysis at the time of thyroid screening. The study by Tudela et al. 23 reported that the risk of gestational diabetes in subclinical hypothyroid pregnant women was significantly higher than that found for the normal group when adjusting for confounding factors, such as age and weight. However, unfortunately, none of the above studies considered the impact of TPOAb status on pregnancy outcomes.14,23–26 Our study demonstrated that in TPOAb-negative pregnant women, when the TSH levels in early pregnancy were 2.5–4.0 mIU/l, the incidence of adverse pregnancy outcomes such as gestational hypertension, GDM, gestational anemia, IUGR, and low birth weight were not significantly different when compared with the control group. Similar to our findings, a secondary analysis of data was conducted from a prospective cohort study 18 and found that TSH levels that exceeded 2.5 mIU/l at 20 weeks of gestation did not increase the risks of premature delivery and GDM. Negro et al. 27 documented that the abortion rate of pregnant women with a TSH level between 2.5 and 5.0 mIU/l exceeded that of women with a TSH <2.5 mIU/l, but there was no significant difference in the incidence of premature delivery. A recent meta-analysis including 15 clinical studies also suggested that there was no significant correlation between the slightly increased TSH level in early pregnancy. 28 Therefore, our results further provide evidence that a slight increase in TSH levels in TPOAb-negative pregnant women in early pregnancy does not increase the risk of adverse pregnancy outcomes.
Furthermore, we explored the incidence of adverse pregnancy outcomes at TSH between 4.0 and 10.0 mIU/l in early pregnancy. We found that when TSH levels were between 4.0 and 10.0 mIU/l, the incidence of GDM, gestational anemia, and premature delivery in pregnancy was significantly higher than that found in the control group. The prevalence of GDM in the TSH significantly elevated group was 26.7%, which was significantly higher than that found in the TSH normal group (12.2%). This result indicated that SCH in early pregnancy could significantly increase the incidence of abnormal glucose metabolism in pregnant women, an observation that was similar to prior studies.22,29,30 During pregnancy, the thyroid hormone has dual effects on islet cells. Not only does it regulate the sensitivity of the body to insulin, but it can also affect its degradation. 31 When pregnancy is combined with SCH, the curve of blood glucose and glucose tolerance is low, and the insulin resistance of peripheral tissues is increased, which eventually leads to the occurrence of GDM. Premature delivery is one of the main causes of neonatal complications and death. Arbib et al. 32 explored 4204 early pregnant women through a retrospective cohort study and found that when TSH >4.0 mIU/l, the risk of premature delivery in the SCH group was 2.3-fold higher than that found in the control group. Cleary-Goldman et al. 12 conducted a prospective study on 10,990 pregnant women. After adjusting for influencing factors, they found that SCH in early pregnancy was not correlated with the risk of premature delivery. A recent meta-analysis of 16 clinical research data studies showed that the risk of premature delivery of pregnant women with SCH was 1.36-fold higher than that of the control group. 33 Our study also showed that the risk of premature delivery in pregnant women with SCH was significantly higher than that in normal pregnant women.
In addition, our study did not find that SCH increased the incidence of pregnancy-induced hypertension, while Wilson et al. 24 and Lai et al. 34 showed that the incidence of pregnancy-induced hypertension in SCH was significantly increased. Consistent with our findings, Casey et al. 35 found that there was no significant difference in the prevalence of either the incidence of high blood pressure during pregnancy or severe preeclampsia in the first trimester between SCH women and euthyroid women. A possible explanation for the inconsistent conclusion may be related to the difference in the definition of SCH or study population selection.
Nevertheless, our study has several limitations. First, it is a retrospective clinical study, and the integrity and reliability of data aggregated from the enrolled population was insufficient, which might affect the analysis of the results. Second, this study selected data from two obstetric hospitals in our city and might not be representative of the general population. Finally, observational indices of adverse outcomes of pregnant women and perinatal children were not comprehensive, which included early abortion rates and the influence on the offspring’s intelligence or psychomotor activities. Further studies in a larger cohort are necessary to validate our findings.
Conclusion
In summary, we have shown that a mildly elevated TSH level or maternal SCH diagnosed by 2011 ATA guidelines in TPOAb-negative women was not associated with adverse pregnancy outcomes. However, the maternal SCH identified by the 2017 ATA guidelines increased the prevalence and risks of several adverse pregnancy outcomes. The 2017 ATA guidelines could be more reasonable for the diagnosis of TPOAb-negative SCH in southern China.
Footnotes
Acknowledgements
The authors would like to thank all the participants in our study. We also thank Dr Yiwen Wang for expert technical assistance and Dr Bo Zhu for valuable discussion.
Author contributions
PZ contributed to conceptualization, data curation, formal analysis, and writing—original draft. RC contributed to conceptualization, formal analysis, methodology, and writing—review and editing. SP contributed to formal analysis, investigation, methodology, and writing—review and editing. XL contributed to formal analysis, investigation, methodology, and writing—review and editing. JR contributed to formal analysis, investigation, and writing—original draft. XL contributed to formal analysis, data curation, investigation, and writing—review and editing.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are available from the corresponding author on reasonable request.