
Abstract
Introduction
Spina bifida (SB) is the most common neural tube defect in humans. Here, we analyzed systematically the neuropathological findings of the brain in SB cases.
Methods
79 cases with SB aperta (SBA) and 6 cases with SB occulta (SBO) autopsied at the Charité Neuropathology from 1974 to 2000 were re-evaluated retrospectively. For this, case files and spinal cord as well as brain sections were studied.
Results
While no brain malformations were detected in SBO cases, 95% of SBA cases had brain malformations. Main brain anomalies identified were hydrocephalus (71%), Chiari II malformation (36%), heterotopia (34%), other cerebellar anomalies (36%), gyrification defects (33%), and ependymal denudation (29%). Hydrocephalus was observed as early as gestational week 17 and was highly associated to Chiari II and ependymal denudation. In 55% SBA was accompanied by further anomalies not primarily affecting the CNS.
Conclusion
We confirm using neuropathologic methods brain malformations in most SBA but none in SBO cases. In addition to our previous radiologic study, we now demonstrate the high prevalence of cerebellar malformations and cerebral heterotopias in SBA. The early detection of hydrocephalus and Chiari II malformation in fetuses raises the question whether these arise parallel rather than in strict temporal sequence.
Keywords
Introduction
Spina bifida (SB) is the most common non-fatal neural tube closure defect (NTD) in humans with an incidence of around 0.5 per 1000 pregnancies worldwide.1–4 SB results from an incomplete neurulation between day 18 and 28 of embryogenesis and is classified roughly into an open (SB aperta, SBA) or closed (SB occulta, SBO) subtype, 2 depending on whether there is skin coverage or not. We recently proposed a systematic classification of SB phenotypes that includes the following SBA subtypes 5 : (i) myeloschisis (MYS) characterized by a neural placode lining within the skin surface and being directly exposed without meningeal or dermal coverage; (ii) myelomeningocele (MMC) defined as sac of spinal cord and meninges protruding through the vertebral defect; (iii) meningocele (ME) with protrusion only of the meninges without spinal cord through the defect. Furthermore there is the rare limited dorsal myeloschisis (LDM) defined as a focal closed midline skin defect with a fibroneural stalk that links the skin lesion to the underlying cord. 6
Patients with SBA depict various degrees of motor and sensory function impairment as well as urinary and fecal incontinence,4,7 depending on their anatomical and functional lesion level. The outcome of patients with SBA, however, also depends on associated brain malformations that range from Chiari II malformation and hydrocephalus to heterotopia, gyrification defects and further neocortical anomalies as well as hypoplasia or aplasia of cranial nerve nuclei, agenesis of corpus callosum, fusion of the thalami and reduction in total white matter with increased neocortical thickness in the frontal regions.8–11 Patients with malformations of cortical development such as heterotopias or polymicrogyria may present with symptoms such as developmental delay, epilepsy and focal neurologic deficits.12–14 There is strong evidence that the pathogenesis of SB reflects a long-term disruption of the central nervous system development far beyond an isolated NTD of the spine. We recently reported in a radiological study that cerebral pathology is always present in patients with SBA but rarely in those with SBO. We further reported the relationship between brain malformations and lower cognitive function in SBA patients. 15
The currently favored model for brain malformation and hydrocephalus in SB invokes venting of cerebrospinal fluid (CSF) through the open caudal end of the neural tube to cause Chiari II, subsequent additional abnormal CSF flow and hydrocephalus, resulting in abnormal neural development.16–19 Results of other studies suggest that a loss of ventricular lining may trigger cerebral pathology, and it is now acknowledged that fetal ependyma has a key role in brain development as a secretory structure. 20 In this regard, it has been shown that ependymal pathology, e.g. denudation, occurs prior to the occurrence of Chiari II and/or hydrocephalus21,22 and may therefore not be the result of hydrocephalus as previously suggested. 23 This is further underpinned through results in mouse models showing that hydrocephalus may result from a primary alteration of ependymal lining. 24
Understanding the SB pathomechanism and the sequence of occurrence of brain malformations is important for the general knowledge on the disease occurrence but also in view of therapeutic approaches. The aim of this study was to systematically analyze neuropathological findings of the brain at various developmental time points in SB.
Cases and Methods
Cases
Autopsies including neuropathological examination of all children and fetuses with SB who deceased at Charité – Universitätsmedizin Berlin from 1974 to 2000 was performed at the Institute of Neuropathology. Clinical data were available from the electronic database provided by the Central Biobank Charité (ZebanC). A search within the database for the ICD10 diagnoses Q05 (SB) and Q76 (SBO) yielded 99 cases which were subsequently re-evaluated. Inclusion criteria were SB with or without associated brain malformations. 14 cases had to be excluded due to false allocation of the ICD-10 code (n = 8), missing clinical data (n = 1) or missing histological specimen for re-evaluation of the SB subtype (n = 5). In total, 85 cases could be included (Supplemental Figure 1), and corresponding histological sections and/or clinical data were anonymized and investigated retrospectively. The study cohort included 79 cases with SBA of different subtypes and 6 cases with SBO. For those cases medical information and autopsy findings were obtained from the database. Pathological reports were sometimes incomplete, and some histological specimens were not usable for interpretation due to their autolytic condition as a consequence of induced abortion, which represent limitations in the retrospective analysis of neuropathological findings in brain sections. Brain malformations identified in SB cases are listed in Tables 1 to 4. The ethic committee of the Charité approved the study (EA1/076/19).
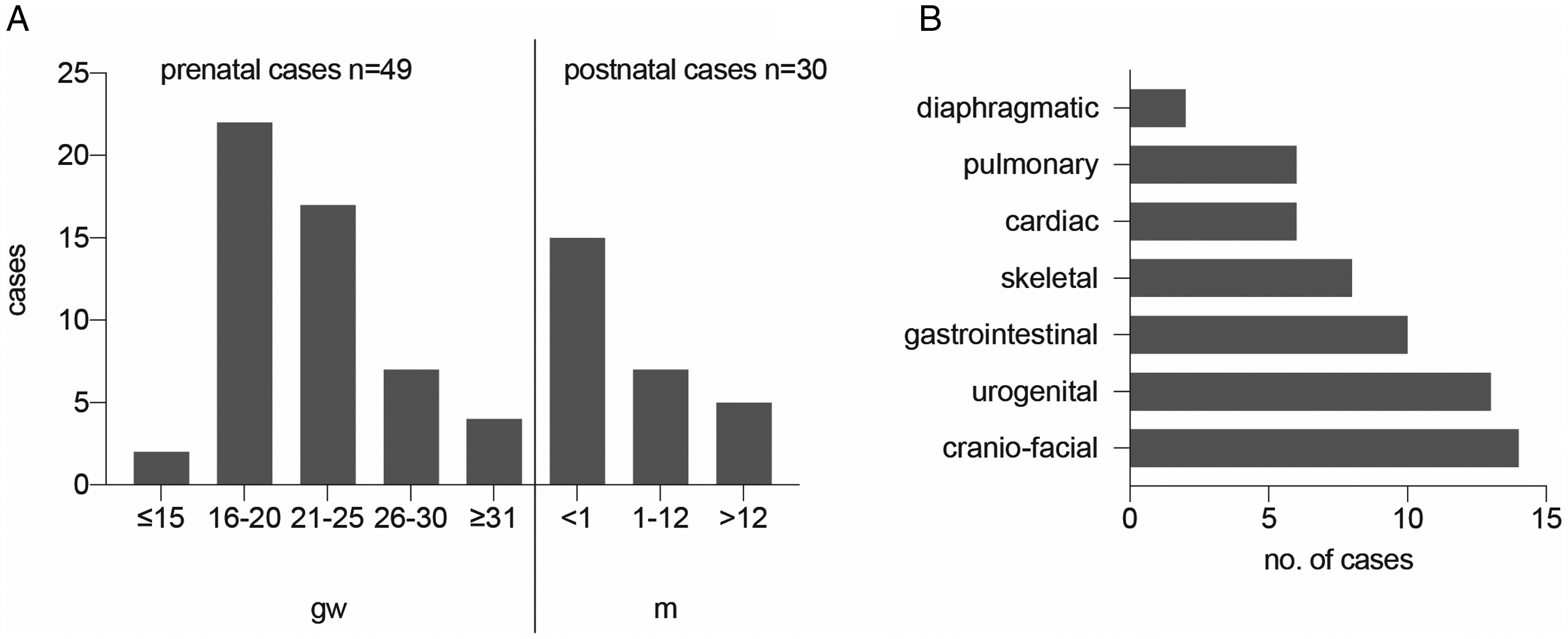
Study cohort. A, Age distribution of cohort with 79 SBA patients. Fetal ages ranged from GW15 to GW40. Surviving children were older than GW25 and are divided into categories depending on survival for ≤1 month, >1 month and >1 year. B, Cranio-facial, urogenital and gastrointestinal malformations dominate associated malformations in individuals with SB. Abbreviations: GW, gestational weeks; m, months; SBA, spina bifida aperta; SBO, spina bifida occulta; NTD, neural tube defect.
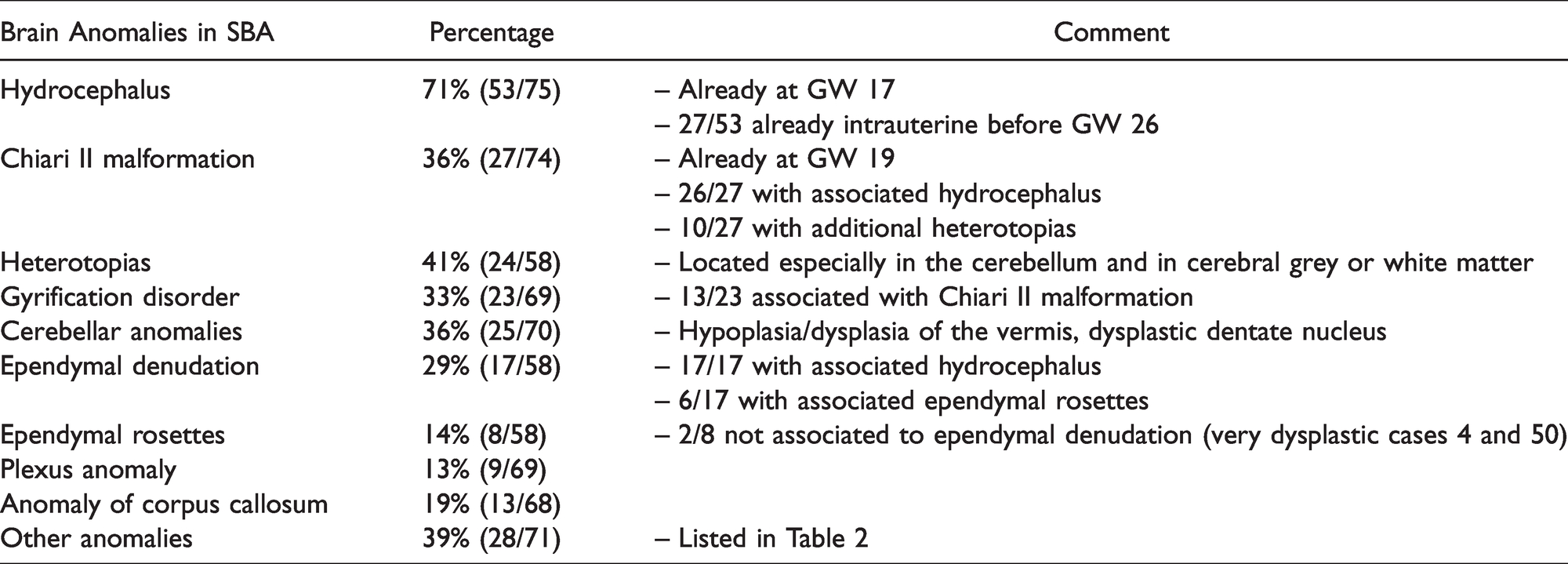
Anomalies of the Brain in SBA.
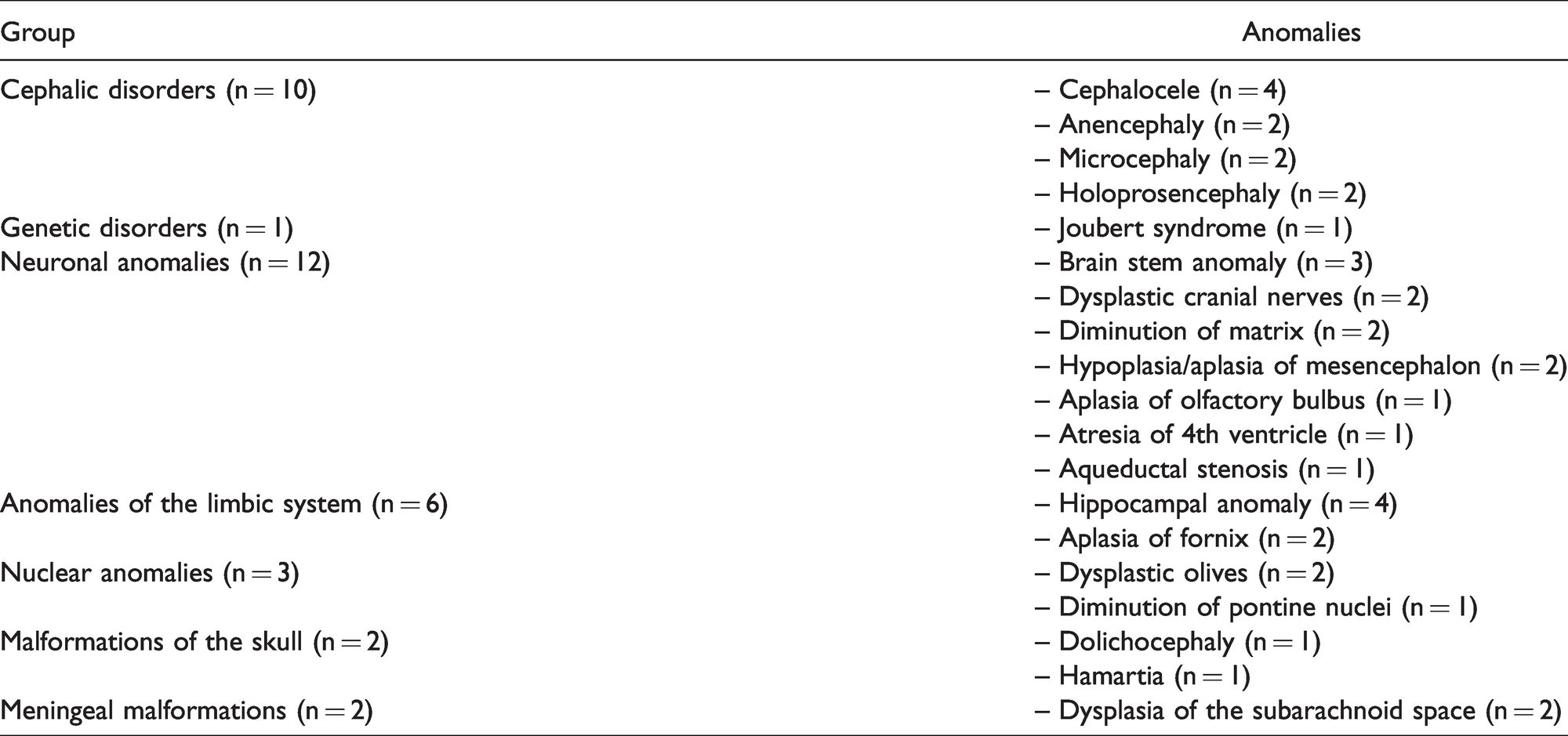
Other Anomalies of the Brain in SBA.
Malformations in SBA.
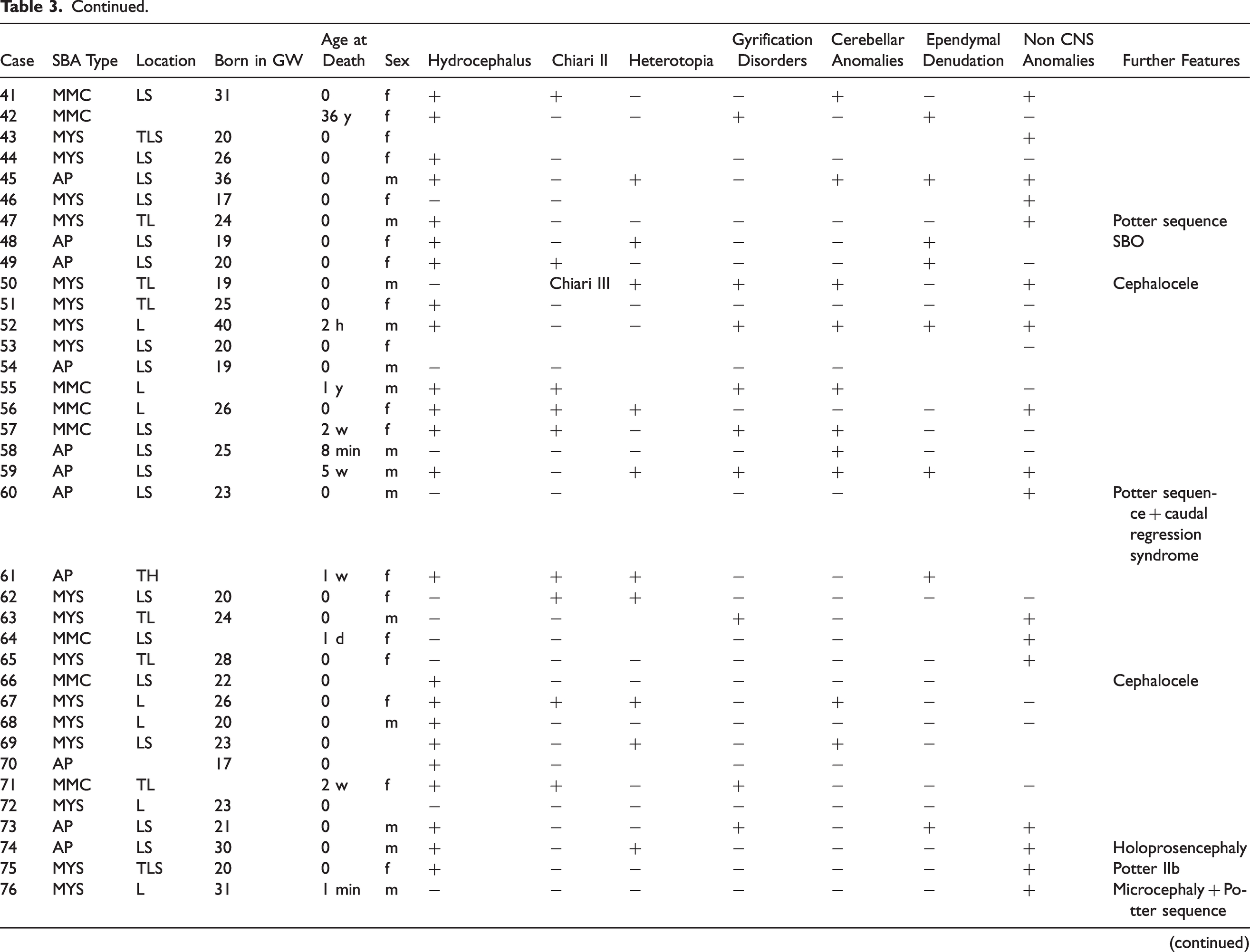
Abbreviations: AP, spina bifida aperta unspecified; C, cranial; CNS, central nervous system; CTLS, cervico-thoracic-lumbo-sacral; d, days; f, female; GW, gestational week; h, hours; L, lumbar; LDM, limited dorsal myeloschisis; LS, lumbo-sacral; m, male; ME, meningocele; min, minutes; MMC, myelomeningocele; MYS, myeloschisis; S, sacral; SBO, spina bifida occulta; T, thoracic; TL, thoracic-lumbar; TLS, thoracico-lumbo-sacral; w, weeks; y, years.
Brain Sections
The brains obtained from all cases were fixed by immersion in 4% buffered formaldehyde. Coronal cuts were obtained for evaluation of ventricular volume, and ventriculomegaly was assessed by neuropathologists. In selected cases, sagittal and horizontal cuts were performed. Whole brain slices and larger blocks were embedded in Celloidin (Figure 3(B), Supplemental Figure 3(C)). Blocks of brain tissue containing representative brain regions were processed for paraffin embedding. Serial sections from paraffin blocks were cut, mounted on SuperFrost Plus™ slides (Thermo Fisher Scientific Inc., Schwerte, Germany, J1800AMNZ) and then stained with hematoxylin-eosin. In case the available stained sections were not sufficient for evaluation, additional sections were cut for immunohistochemistry at 4 µm.
Immunohistochemistry
The following primary antibodies were used: mouse anti-acetylated tubulin (Sigma Aldrich, St. Louis, USA, t6793/t7451, 1:1000 dilution) and rabbit anti-glial fibrillary acidic protein (GFAP, DAKO, Glostrup, Denmark, Z0334, 1:500 dilution). Incubation of the primary antibody at 4°C was in a moist chamber for 24 hours in antibody diluent with background reducing components (DAKO, Carpinteria, CA, USA, S3022) after blocking of the endogenous peroxidase with hydrogen peroxide at a dilution of 1:10 and with unconjugated normal goat serum (Jackson Immuno Research Europe Ltd, West Grove, PA, USA, 005-000-121). Anti-rabbit IgG biotinylated antibody raised in goat (Sigma Aldrich, St. Louis, USA, B8895) and anti-mouse IgG biotinylated antibody raised in goat (Vector Laboratories, Inc., Burlingame, CA, USA, ZB0324) were applied as secondary antibodies at a dilution of 1:200 for 30 minutes at room temperature. Detection was induced by Vectastain ABC-KIT (Vector Laboratories, Inc., Burlingame, USA, PK-6100) in a moist chamber for 50 minutes. 3.3’-diaminobenzidine tetrahydrochloride (DAB+ Substrate Chromogen System, DAKO, Carpinteria, CA, USA K3468) was used for development.
Photographic Documentation
For documentation of microscopic findings M8 PreciPoint digital microscope and scanner (PreciPoint GmbH, Freising, Germany) was used. Images of the scanned histological specimen were created with the software ViewPoint (PreciPoint GmbH, Freising, Germany) and detailed figures were generated using Adobe Illustrator (Illustrator 2020 (Version 24.1.2), Adobe Inc., San José, California) and Gimp (Gimp 2020 (Version 2.10.22), The Gimp-Team).
Statistical Analysis
To evaluate correlations, we used the Chi-square test and considered test results with a p-value <0,05 as statistically significant. Data analysis was performed, and graphs were generated using GraphPad Prism 8 (version 8.4.0, GraphPad Software Inc., San Diego, California).
Results
We analyzed the presence of brain malformations in 79 cases with SBA and 6 cases with SBO at a mean age of GW23, with 49 prenatal (range GW15-40) and 30 postnatal SBA (range GW24-40) cases as well as 5 prenatal cases and 1 postnatal SBO case (Figure 1(A)). Of the 49 SBA cases that deceased prenatally most died because of induced abortion (n = 36), followed by pregnancy or birth complications (n = 7) or unknown reasons (n = 6). Of the 30 liveborn SBA cases more than a third died shortly within the first postnatal 24 hours (11/30). The causes of postnatal death included respiratory (n = 8) or cardiac (n = 3) insufficiency, survived induced abortion (n = 3), status epilepticus, meningoencephalitis or surgical complications (n = 9), renal failure (n = 1), birth complications (n = 1) and unknown reasons (n = 5). In the SBO group cases deceased because of induced abortion (n = 3), intrauterine death (n = 2) and for the one liveborn case due to respiratory insufficiency as a result of pulmonary hypoplasia with bilateral renal agenesis (Potter sequence, n = 1). Data concerning age at death, sex, type and level of SBA and associated brain malformations are presented in Table 3 and detailed information on brain malformations in SBA is listed in Table 1. While the SBA group showed a high prevalence of additional brain anomalies, none were present in the SBO group (Table 4).
Brain Malformations in SBO.
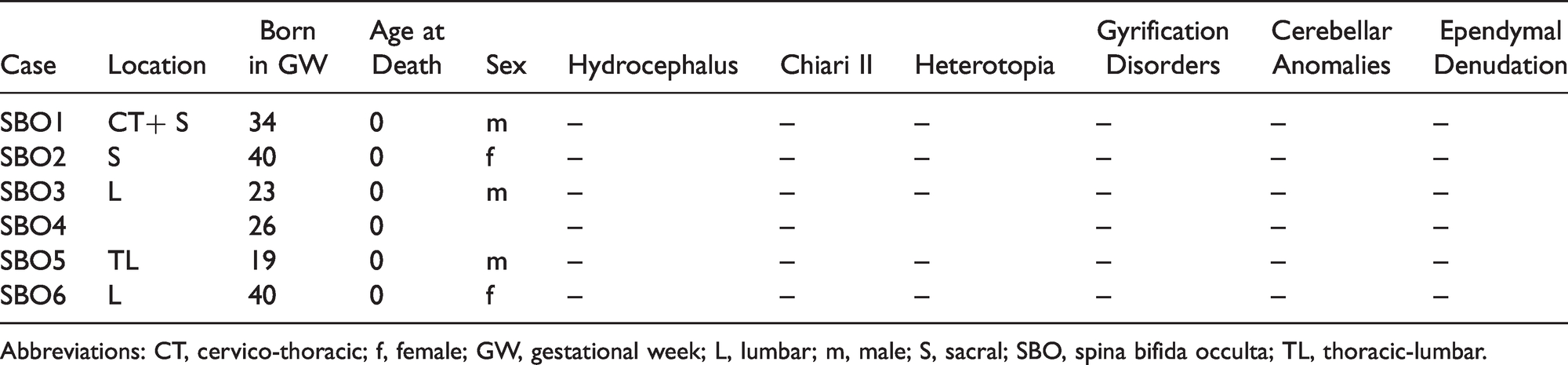
Abbreviations: CT, cervico-thoracic; f, female; GW, gestational week; L, lumbar; m, male; S, sacral; SBO, spina bifida occulta; TL, thoracic-lumbar.
Most cases with SBA had lumbar and/or sacral lesions (72%, n = 57), followed by thoracolumbar (13%, n = 10) and cranial and/or thoracic lesions (3%, n = 2). One case had a lesion reaching from the cervical to the sacral spine, and two cases had a lesion reaching from the thoracic to the sacral spine. The lesion level could not be unambiguously determined in 6 cases. We diagnosed myeloschisis (MYS) in 32% (n = 27), myelomeningocele (MMC) in 31% (n = 26), meningocele (ME) in 2% (n = 2), limited dorsal myeloschisis (LDM) in 1% (n = 1) and SBO in 7% (n = 6) of all cases. The SBA subtype could not be unambiguously identified in 23 autopsied cases (27%) due to missing or incomplete histological specimen or because of wrong cutting position for re-evaluation of SB type (AP). Occurrence of brain malformations was not associated with the lesion level and/or the sex in our cohort, in comparison to higher rates of malformations in thoracic/cranial NTDs and/or female cases described previously by others. 25
SB was frequently accompanied by further anomalies. In SBA cases this was the case in 55% (34/62) of the cases with associated anomalies not primarily affecting the CNS. Such anomalies ranged from cranio-facial (n = 14), urogenital (n = 13) and gastrointestinal (n = 10) malformations via skeletal (n = 8), cardiac or pulmonary deficiencies (n = 6 each) or diaphragm abnormalities (n = 2) (Figure 1(B)) to syndromes like Potter sequence (n = 3). Other syndromes we detected affecting the CNS were Joubert syndrome (n = 1) and a caudal regression syndrome which occurred together with Potter sequence (n = 1). Of all SBA cases, 10 cases (13%) had the following additional cephalic disorders: microcephaly (n = 2), holoprosencephaly (n = 2) and the additional NTDs: cephalocele (n = 4), anencephaly (n = 2) (Table 2), while none were present in SBO. Four of the cases with SBA had characteristic malformations leading to the diagnosis of following defined syndromes: Potter sequence (n = 2), Potter sequence and caudal regression syndrome (n = 1), Polycystic kidney disease (Potter IIb, n = 1) and Joubert syndrome (n = 1). Accessibility of genetic testing was limited at the time of analysis with only seven chromosome analysis results available that were all normal. Modern genetic approaches applied to patients with SB have, however, revealed several genetic causes,26–28 and it would be desirable to perform future neuropathological studies in genetically well characterized cases. Detailed information about the associated malformations is given in Supplemental Figure 2.
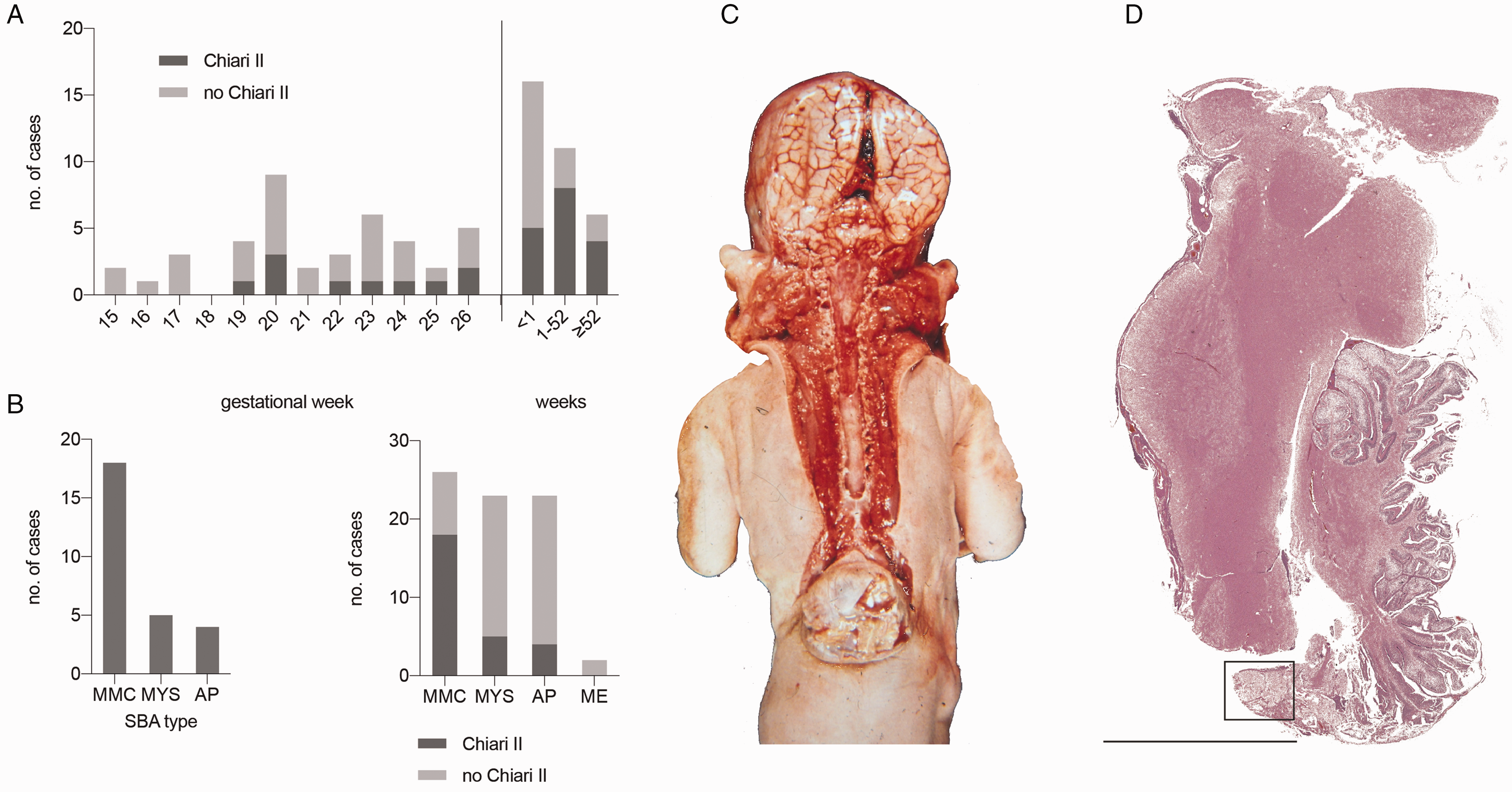
Chiari II malformation in SBA. A, Presence or absence of Chiari II in 74 SBA cases. Chiari II was identified as early as GW19 but presents increasingly postnatally in individuals born after GW25 (n = 74 SBA cases). B, Chiari II was present predominantly in myelomeningocele but was also present in the other SBA subtypes myeloschisis and in cases with SBA where subtype could not be closer specified (AP). In comparison distribution of SBA cases without Chiari II are displayed. C, Chiari II in a 2 weeks old female newborn with lumbosacral myelomeningocele and hydrocephalus (case #88). Note the displacement of the cerebellar vermis and low-lying brain stem characteristic for Chiari II. Effacement of sulci are evidence of hydrocephalus. D, Cerebellar herniation and its position in relation to the brain stem are part of a Chiari II malformation. Additionally, the dysplastic cerebellum is outlined and magnified for better analysis in Figure 4(D) of a 10-day-old newborn with SBA, Chiari II and hydrocephalus (case #16, H&E, sagittal section, bar 1 cm). Abbreviations: GW, gestational weeks; SBA, spina bifida aperta; H&E, hematoxylin-eosin; MMC, myelomeningocele; MYS, myeloschisis; AP, SBA not closer specified; ME, meningocele.
Brain malformations were found in 95% of SBA cases while no malformation was found in SBO cases. Additional malformations would be expected in SBO significantly less frequently than in SBA (p = 7,5 × 10−11). All neuropathological findings in the brain are summarized in Tables 1 and 2.
Chiari II malformation, defined as cerebellar vermis herniation through the foramen magnum and brain stem elongation (Figure 2(C) and (D)),17,19 was present in 36% of the cases (27/74) and was detected as early as GW19 (Figure 2(A)). 74 cases were included in analysis while 4 cases of the total 79 cases with SBA were excluded due to insufficient preservation of histological specimen and 1 was excluded because of Chiari III malformation. Chiari II malformation is highly associated to MMC (Figure 2(B)). In our cohort 26 of the cases had associated hydrocephalus, while only one case (#62) presented Chiari II malformation without hydrocephalus. The latter case was aborted in GW 20 and is one of the youngest cases developing Chiari II malformation in our cohort. SBA, especially MMC, is known to be nearly always associated to Chiari II hindbrain malformation and the onset of hydrocephalus. 29 Whereas the Chiari II rate of all evaluated cases was 36% (27/74 cases), cases with MMC showed higher Chiari II rates (18/26 cases; 69%, p = 0,0389) than cases with MYS (5/24 cases; 21%, p = 0,1549).
Hydrocephalus was identified in 71% of the cases (53/75). 75 cases were included in analysis while the same 4 cases mentioned above had to be excluded because brain examination was not possible due to insufficient preservation of histological tissue. Hydrocephalus was detected as early as GW17 and was present in over half of the prenatal cases (n = 27) (Figure 3(A)). Diagnosis can be made through macroscopic analysis of ventriculomegaly or via ultrasound while microscopic presentation shows thinning of the cortex and ventricular dilatation (Figure 3(B) and (C)). Today MRI and ultrasound enable more accurate analysis of ventricular enlargement15,30 and SB 31 and will be the leading methods for future studies addressing the question whether the severity of hydrocephalus correlates with the degree or extend of associated malformations.
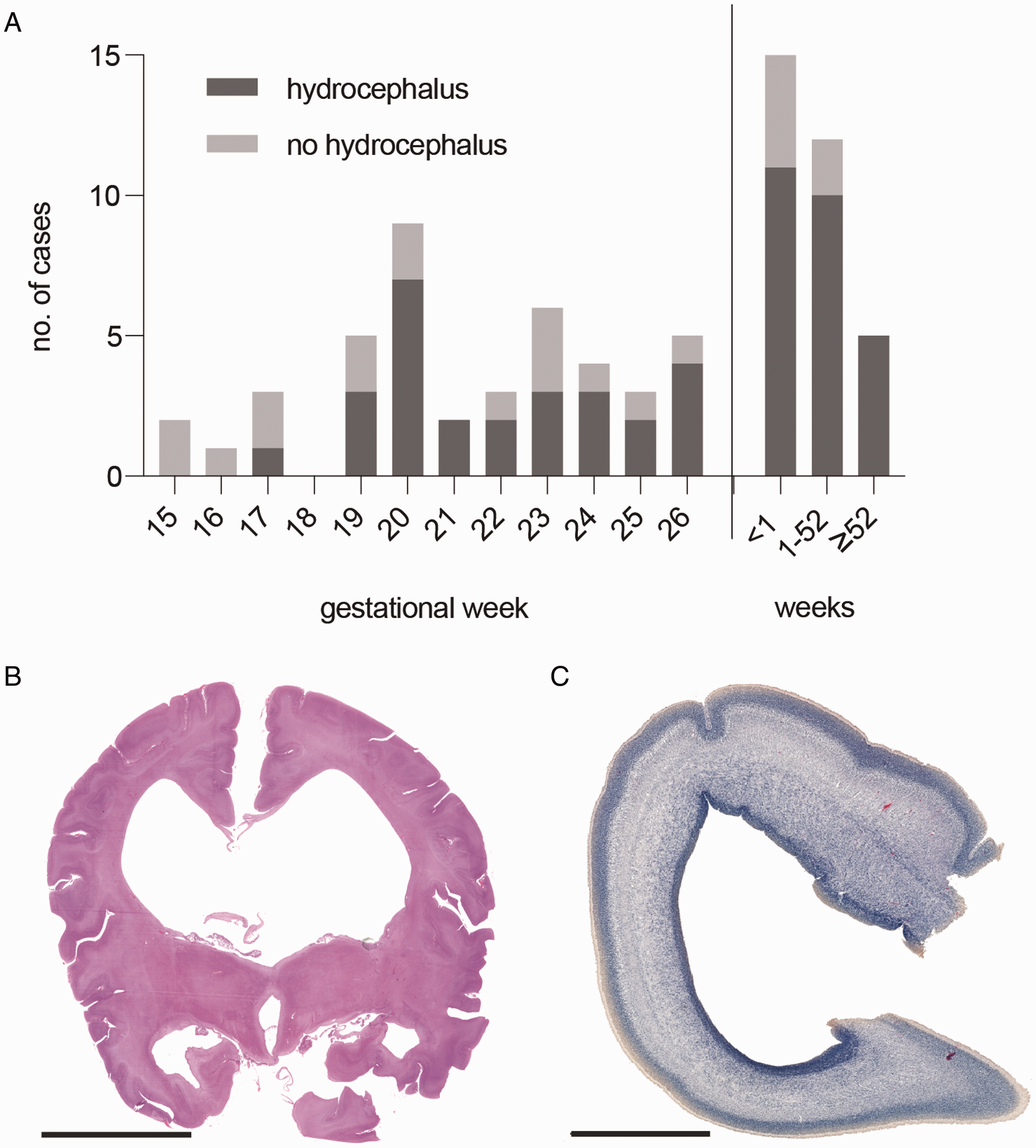
Hydrocephalus in SBA. A, Hydrocephalus is present in 71% of 75 SBA cases. It can be detected as early as GW17, with an increase of incidence after birth. B, Ventriculomegaly signals the hydrocephalus. H&E staining of a coronal celloidin embedded section of a 5 weeks old newborn with myelomeningocele, hydrocephalus and Chiari II malformation (case #34, bar 2 cm). C, Hydrocephalus was identified as early as GW17 and is indicated by thinning of the cortex. H&E staining with faded eosin staining of a coronal brain section of a fetus with SBA at GW17 (case #70, bar 2 mm). Abbreviations: GW, gestational weeks; SBA, spina bifida aperta; H&E, hematoxylin-eosin.
Heterotopia defined as nodules of grey matter in an abnormal location 32 were found in 34% of the cases (20/58) and were only present in SBA (Figure 4(A)). 21 cases were excluded from this analysis due to missing histological specimen for evaluation. Heterotopic neurons were located especially in the cerebellum (n = 9) (Figure 4(B) to (E)) and/or in the white matter (n = 9) of the cerebrum. Other locations included tectum of 4th ventricle (n = 4), meninges of the subarachnoid space (n = 1) and the hippocampal (n = 1) or subependymal zone (n = 1) (Figures 4(B)). Seven of the cases showed heterotopia in multiple locations. All of the cases with heterotopias showed additional brain malformations, whereas 17 were associated to hydrocephalus (17/20; 85%), 7 were associated to Chiari II malformation (7/20; 35%) and 5 of the cases showed additional gyration disorders. The same applies for the cases with cerebellar heterotopias that were also all associated to further brain malformations (90% with hydrocephalus, 33% with Chiari II, 33% with gyration disorders) and did not occur isolated. In addition to the heterotopic nodules, focal cortical dysplasia was seen in 8 cases.
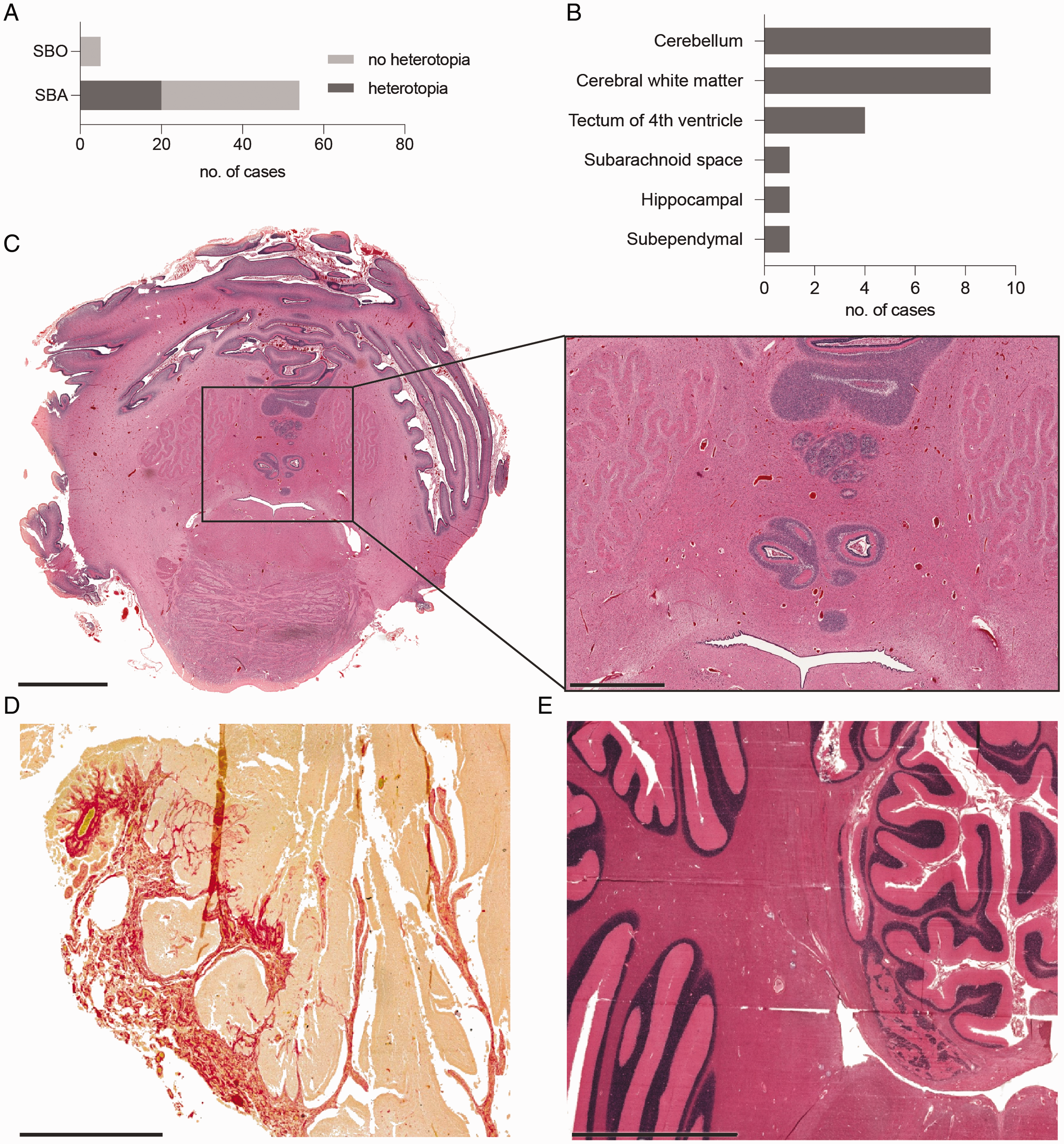
Heterotopia in SBA. A, Heterotopias are present only in SBA (20/58) and not in SBO (0/6). B, Heterotopias are predominantly located in the cerebellum (n = 9) and/or white matter (n = 9). C, Heterotopias in proximity of the 4th ventricle in the cerebellum of a hydrocephalic one-day-old newborn with myeloschisis and SBO (case #17, H&E, transverse section, bar 5 mm). Magnification shows multiple heterotopias forming a nodule (bar 2 mm). D, Cerebellar heterotopias in the subarachnoid space as part of a dysplastic cerebellum in a hydrocephalic 10-days-old newborn with SBA and Chiari II (case #16, H&E, Sirius-Red, sagittal section, bar 2 mm, displayed in Figure 2D at larger size). Red staining shows amplification of connective tissues forming a big cerebellar heterotopia. E, Cerebellar heterotopia in a hydrocephalic 4-year-old child with myelomeningocele and Chiari II (case #24, H&E, transverse section, bar 5 mm). Abbreviations: GW, gestational weeks; SBA, spina bifida aperta; SBO, spina bifida occulta; H&E, hematoxylin-eosin.
Gyrification disorders were present in 33% of the evaluable cases (23/69), whereas 13 of those cases showed concomitant Chiari II malformation (Figure 5(A) to (D)). Definition of gyrification anomalies is inconsistent and literature suggests the terms polymicrogyria, microgyria, polygyria, polysulceria, pachygyria and stenogyria being associated to NTDs and/or Chiari II10,15,29,33–35 whereas polymicrogyria (Figure 5(C)) can only be diagnosed histologically and is seen as a real neuronal migration disorder 19 being often associated with SB and/or Chiari II. In this cohort polymicrogyria was only present in 2 of the cases with anomalous gyration whereas abnormal number and form of gyri and sulci was more common. Polymicrogyria, often used synonymously to microgyria, describes a cerebral or cerebellar cortical disorder in which the gyri are reduced in size, increased in number and accompanied by a characteristic four layered lamination19,34 (Figure 5(C)). Stenogyria, which is not a true neuronal migration disorder, stands for the presence of multiple small compacted gyri separated by shallow sulci15,36 and is also mentioned as polygyria33,35 (Figure 5(B)). The gyrification pattern can also show an abnormal number and distribution of principal sulci with increased average length of the sulci and should be referred to as polysulceria. 35 Such pattern with deep branched sulci was also present in our cohort (Figure 5(D)).
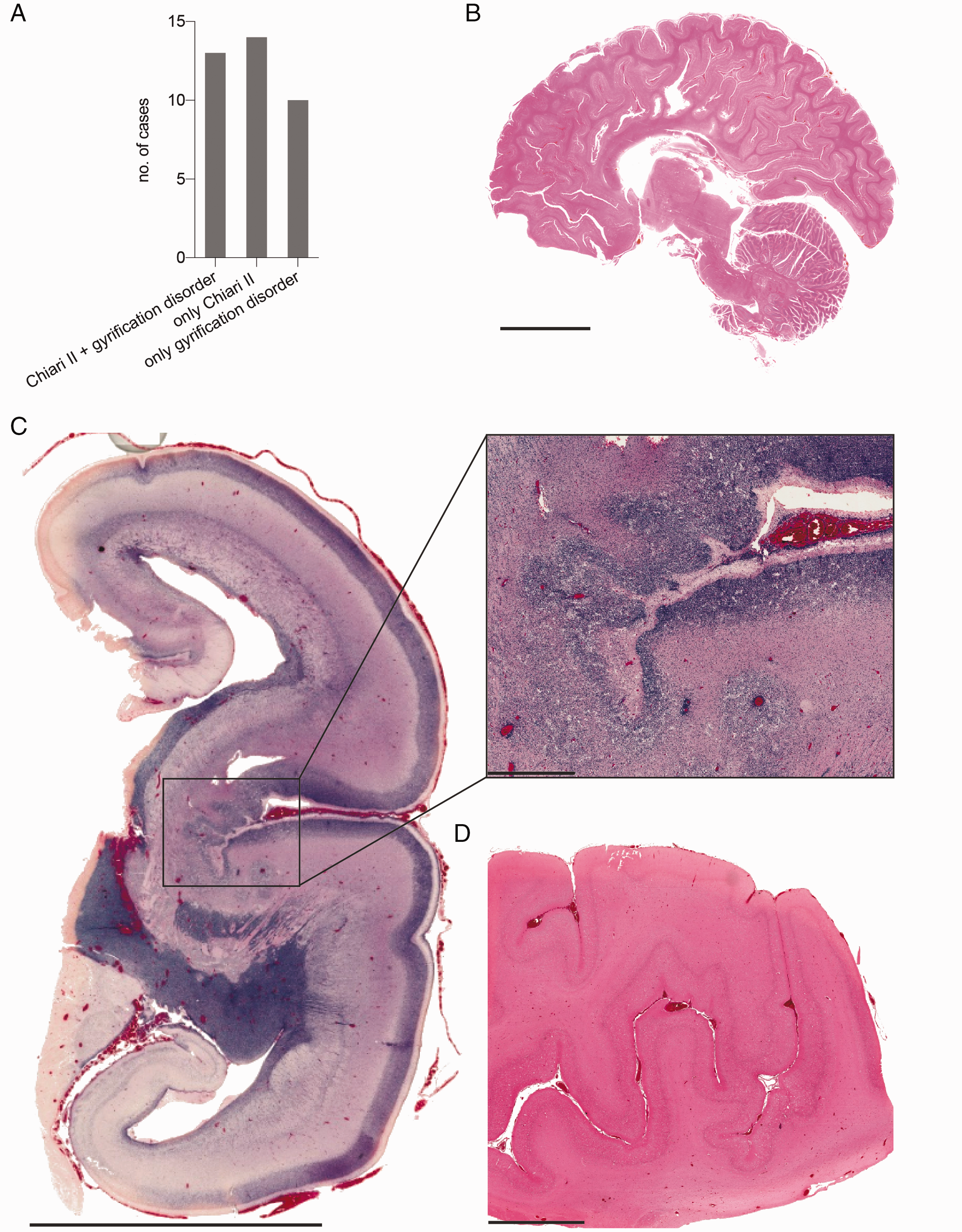
Disorders of gyration in SBA. A, Gyration disorders were present in 33% of 69 SBA cases where analysis of the gyri was possible. 13 of the 23 cases with gyrification disorders showed concomitant Chiari II malformation. B, Stenogyria in a hydrocephalic brain from a one-year-old newborn with myelomeningocele and Chiari II (case #55, sagittal section, H&E, bar 3 cm). C, Polymicrogyria in the right hemisphere of a fetus from GW19 with myeloschisis and Chiari III with a cephalocele (case #50, H&E, coronal section, bar 10 mm). The magnified lateral sulcus shows polymicrogyria with disorganization of the cortical layering (bar 1 mm). D, Polysulceria of the cortex in a 5-week-old newborn with SBA and hydrocephalus (case #59, H&E, bar 5 mm). Abbreviations: GW, gestational weeks; SBA, spina bifida aperta; H&E, hematoxylin-eosin.
Ependymal denudation occurred in 29% of the cases (17/58) and ependymal rosettes only in 14% (8/58). The latter were strongly associated to ependymal denudation and only 2 cases showed ependymal rosettes in absence of denudation. These 2 cases however were the most malformed brains of the cohort (case 4, case 50). All of the cases with loss of ependymal lining had concomitant hydrocephalus (Figure 6(A) and (B)) and rosettes were found in 35% (6/17) (Figure 6(D)). Consequently, from all the hydrocephalus cases 17 showed defects of ventricular lining (32%; 17/53). We discovered that the occurrence of ependymal abnormalities has a prenatal peak in GW19-22 which could embrace the cases where ependymal loss precedes the onset of hydrocephalus and a postnatal peak which could embrace the cases where the ependyma is injured due to higher pressure of cerebral spinal fluid and subsequent ventricular dilatation. Figure 6(B) shows the relationship of hydrocephalus and ependymal defects. Loss of ependymal lining is followed by creation of subventricular gliotic nodules that form within the gaps between ependymal islands bulging into the ventricular lumen (Figure 6(C)). These are accompanied by reactive subventricular gliosis and formation of rosettes in zones of ependymal damage (Figure 6(D) to (F)). All samples from the cerebral aqueduct and lateral ventricles from nonhydrocephalic fetuses examined were lined by a continuous ependymal lining (n = 8 in SBA, n = 6 in SBO).
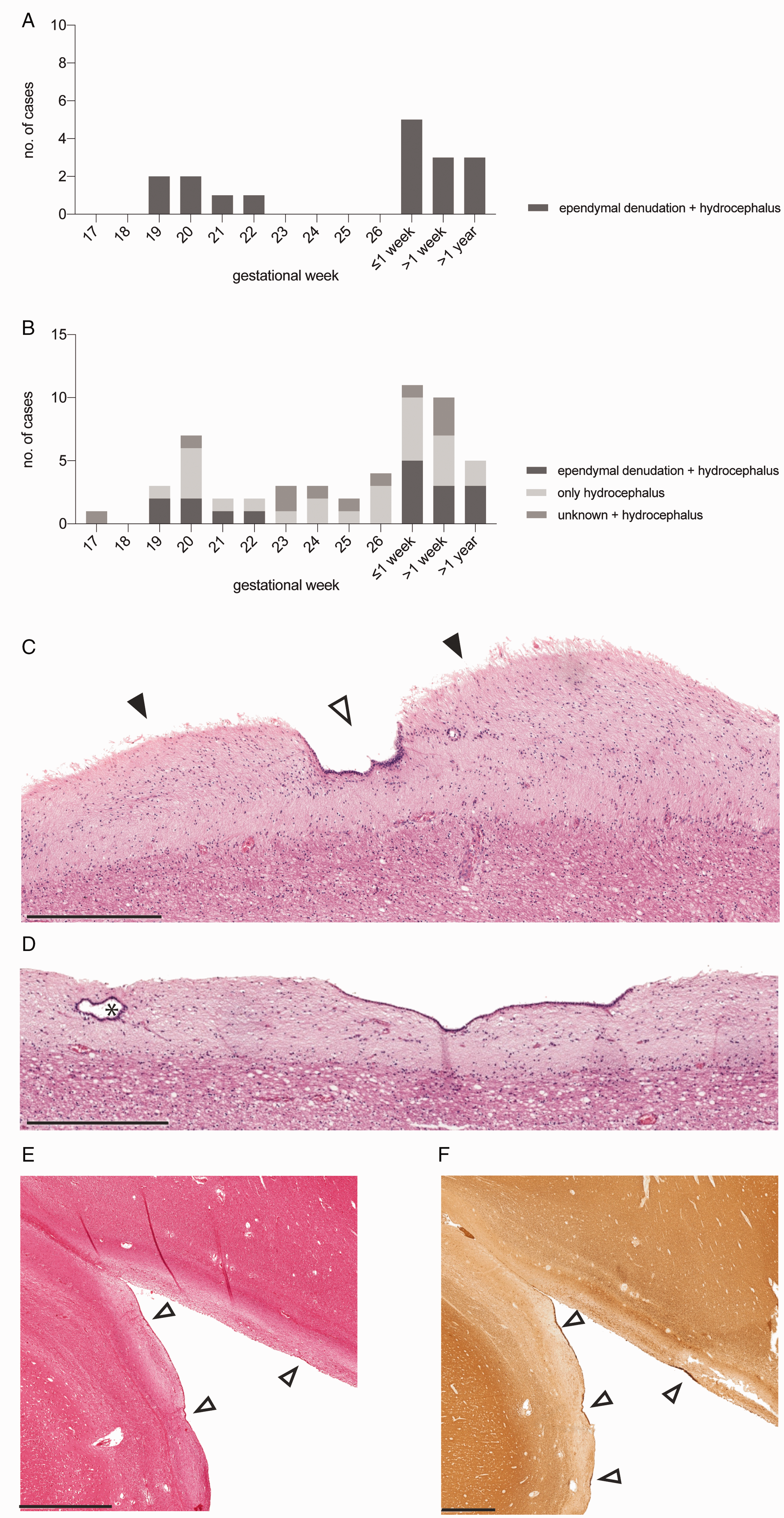
Ependymal denudation in SBA. A, Ependymal denudation in 29% of SBA cases and only in those with hydrocephalus. The two age peaks when ependymal denudation is present could explain the two theories of when ependymal denudation occurs. One peak from GW19-22 builds the group where a defect ependyma causes hydrocephalus while the second peak could be the group formed by ependymal injury as a result of hydrocephalus. B, Additional to A cases with only hydrocephalus and with unknown ependymal status are listed. C, Gliotic nodules bulging into the ventricular lumen (solid arrows) adjacent to the intact ependyma (open arrow) show the denuded areas. Wall of a lateral ventricle of a hydrocephalic 14-year-old child with myelomeningocele, Chiari II and ependymal denudation (case #79, H&E, bar 500 µm). D, Ependymal rosettes form in the subventricular zones devote of ependymal lining (black star). Hematoxylin-eosin-stained section through the ventricular wall of a hydrocephalic 14-year-old child with myelomeningocele and Chiari II (case #79, H&E, bar 500 µm). E and F, Immunostaining of ependymal lining and denudation in SBA: Sections through the wall of the lateral ventricle of a hydrocephalic 4-year-old child with myelomeningocele and Chiari II malformation (case #24) immunostained for acetylated tubulin. E, H&E stain showing nondenuded areas (open arrows) and denuded areas (bar 1 mm). F, The ependyma is reactive for acetylated tubulin showing nondenuded areas (open arrows, bar 1 mm). Abbreviations: GW, gestational weeks; H&E, hematoxylin-eosin.
Our results show additional brain anomalies like heterotopias, gyrification anomalies, anomalies of corpus callosum or the cerebellum in 14 of the cases with ependymal denudation. Only 3 cases with hydrocephalus and ependymal denudation showed no further alterations of brain morphology (case 1, 14 and 49) but had Chiari II malformation suggesting hydrocephalus being a result of hindbrain herniation in those cases. In total, hydrocephalus coincided with Chiari II malformation in 26 cases. In 8 cases hydrocephalus was present without Chiari II malformation but accompanied by discontinuities of ependymal lining. In this group hydrocephalus could be the result of an alternated neuroepithelial lining. For 3 cases with hydrocephalus a hypertrophic plexus epithelium was found but in only 2 of those cases it occurred isolated without Chiari II malformation and could be the cause due to abnormalities of secretion. For 14 cases (14/75; 19%) the pathogenesis of hydrocephalus remains unclear as it is not associated with loss of ependymal lining and/or Chiari II malformation.
Malformations of the cerebellum other than Chiari II were present in 36% (25/70). They included hypoplasia of the cerebellum or isolated dysplasia or aplasia of the vermis, dysplasia of the dentate nucleus and/or gyrification disorders.
More rare malformations were plexus anomalies (13%; 9/69) and anomalies of the corpus callosum in 19% (13/68). From the 9 cases with plexus anomalies, 7 had associated hydrocephalus suggesting that hydrocephalus can be caused also by abnormalities of secretion through abnormal plexus epithelium. Of the two cases without hydrocephalus, one had ectopic plexus epithelium between the two occipital lobes and no choroid plexus in the ventricles and could as a consequence not develop a hydrocephalus even if born with atresia of the 4th ventricle (#50), and the other case was born with microcephaly (#79). Other malformations (Table 2) of the central nervous system (CNS) were detected in 39% of the cases (28/71) and include additional cephalic disorders (n = 10), neuronal anomalies (n = 12), anomalies of the limbic system (n = 6), nuclear anomalies (n = 3), malformations of the skull (n = 2) and the meninges (n = 2). Some of them are displayed in Supplemental Figure 3(A) to (D).
Two cases showed diffuse heterotopias in both hemispheres with prominent neuronal migration disorder (cases 4 and 50). Case 4 is a fetus from GW16 with unknown lumbo-sacral SBA and associated parieto-occipital cephalocele and amelia of the upper right extremity. The brain of this case showed a huge cephalocele in an extremely malformed brain, with hamartia and perivascular ossifications, diffuse heterotopias of the cerebellum and white matter, polymicrogyria of the gray matter and multiple ependymal rosettes (Supplemental Figure 3(A)). Case 50 is a fetus from GW19 with thoracic-lumbar myeloschisis and associated occipital-cervical cephalocele. Brain findings showed asymmetric hemispheres with a completely malformed left hemisphere, polymicrogyria, atresia of the 4th ventricle, ectopic choroid plexus, hippocampal anomaly, Chiari III malformation and multiple heterotopias and ependymal rosettes in the white matter. This is the case mentioned above where the ectopic plexus epithelium explains the missing hydrocephalic ventriculomegaly.
Discussion
In this study we systematically characterized neuropathological findings in the brains of 85 cases with SB (79 SBA, 6 SBO). Our main finding using neuropathologic methods is that brain malformations were present in most (95%) SBA cases, whereas none could be identified in SBO cases. Main brain anomalies identified were hydrocephalus (71%), Chiari II malformation (36%), heterotopia (34%), cerebellar anomalies other than Chiari II (36%), gyrification defects (33%), and ependymal denudation (29%). In addition to our previous radiologic study, 15 we now demonstrate the high prevalence of cerebellar and cerebral heterotopia in SBA. Also, we detected hydrocephalus without a Chiari II malformation in fetuses early in development, a finding that raises the question whether these develop parallel rather than in temporal sequence. The difficult detection of mild forms of hydrocephalus and Chiari II however challenge our statement and call for further, e.g., ultrasound-based studies. We also detected a high prevalence of associated anomalies not primarily affecting the CNS, but rather the lower limbs or the urogenital tract in 55% of the SBA cases. Limitations of this study coincide with the retrospective nature of the study and include incomplete histological specimen as well as limited genetic and imaging results at the time of collection of the cohort. Given the nature of the study on deceased subjects this could lead to a higher incidence of associated anomalies.
Our results support the strong association of Chiari II malformation and hydrocephalus.16–18 One of the youngest four cases presenting with a Chiari II malformation did not have a hydrocephalus at GW20, but may have developed it later on. This would sustain the idea that hydrocephalus develops as a result of Chiari II malformation. 17 Following that theory of Chiari emergence, the presence of an open neural tube allows constant CSF loss resulting in failure of proper ventricular growth leading to inadequate and disorganized neural development and secondarily to mesenchymal defects like a small posterior fossa and a low-lying tentorium. Hydrocephalus is seen as a result of Chiari II due to maldevelopment of the CSF spaces and consequently abnormal CSF flow.16–18 However, half of the 53 cases with hydrocephalus (n = 27) in our cohort did not have an associated Chiari II malformation, and we detected hydrocephalus already as early as GW17 in one of these. This does not go along with the common belief of a Chiari-II-linked hydrocephalus-onset,17,37 i.e., they must have followed a different pathophysiology.
Newer, extended theories on the pathophysiology of hydrocephalus in SB argue that hydrocephalus results from a primary alteration of the ependymal cell lineage21,22,38 rather than being only a consequence of it.23,39 A loss of ependymal lining preceding hydrocephalus has already been shown in a mouse model for long-lasting hydrocephalus (Hyh mutant mice). 24 In this line, Dominguez-Pinos et al. showed that ependymal detachment is associated with hydrocephalus and abnormal neurogenesis. 22 Our finding of early ependymal denudation is supported by that of de Wit et al. who reported neuroepithelial denudation in fetuses with SBA already at GW16 even in absence of hydrocephalus and/or Chiari II malformation. 21 Together, these results suggest that ependymal denudation may be associated with the onset of hydrocephalus. In addition, further pathomechanisms such as an obstruction to CSF flow or excess CSF production39,40 and defect ciliary function41–44 have been suggested and may also contribute to hydrocephalus. This may explain the 14 cases in our cohort associated neither with a loss of ependymal lining nor with a Chiari II malformation. Reversibility of hindbrain herniation following prenatal surgery suggest that part of the abnormalities associated to SB and Chiari II malformation is secondary to mechanical effects. 45 Prospective studies concentrating on the development of hydrocephalus at an early gestational age are a key to resolve the knowledge gap in causes leading to hydrocephalus.
Not only hydrocephalus and/or Chiari II were present in the cohort, but also further brain malformations arise in most (80%; 57/71) SBA cases. Totally and diffuse malformed brains were only present in 2 of our cases (cases 4 and 50) whereas the incidence of specific structural abnormalities was higher. We suggest there is an underlying malformative aspect in brain development explaining the associated anomalies in SBA.
Only four studies on postmortem neuropathological findings in SB focus on CNS malformations in SB.8,10,25,46 Concentrating only on hydrocephalus (71%) and Chiari II (36%) we now showed a higher incidence for these entities than Bell et al. who detected hydrocephalus in 52% and Chiari II in 57% of cases. 25 In comparison to these studies we showed a higher incidence of neuronal migration disorders such as heterotopias (34%) and gyrification disorders (33%) in our study in comparison to the 7% (4/56) frequency of dysplasia and polymicrogyria reported by others. 10 Gilbert et al. also analyzed specific brain stem anomalies describing hypoplasia or aplasia of cranial nerve nuclei in 20% and other CNS malformations as disordered migration of cortical neurons (92%), cerebellar dysplasia (72%), fusion of the thalami (16%) and complete or partial agenesis of the olfactory tract and bulb (8%). 8 Regarding the higher incidence of heterotopias and gyrification disorders for the latter study it has to be taken into account that criteria for included cases was MMC with Chiari II malformation and hydrocephalus. The occurrence of holoprosencephaly in two fetuses with SBA in GW 17 and 30 is compelling since it implies cooccurring defects in neurulation and in diverticulation at different time points of embryogenesis. This was previously described by Osaka et al. in 18/92 (20%) myeloschistic embryos, 46 but to our knowledge never in fetuses with SBA. Another novel finding was the association of Joubert syndrome with lumbar MMC. Ciliopathies such as Joubert syndrome and Meckel Gruber syndrome have been associated to NTDs, but particularly to cephaloceles 47 and not to lumbar NTDs. Many genes48–50 have been related to the development of Joubert syndrome and this new association underpins the question of a ciliopathic pathogenesis also for SB among the NTDs. Other neuropathological reports did not concentrate on SB explicitly but on NTDs in general bringing malformations other than those of the CNS, like urogenital, gastrointestinal or skeletal malformations, more into account.9,26,51 Associated anomalies not primarily affecting the CNS were previously described in 36% (n = 15/42) 26 and 34% (n = 10/29) 51 while one study coincided with our data (55%, 21/38). 9 Our results underline the importance of a separate analysis of SBA and SBO phenotypes, particularly given the differing prognosis of an affected child in light of associated malformations. The latter would be expected in SBO significantly less frequently than in SBA.15,25,52
We here detected a high rate of cerebellar heterotopias (16%; 9/58). It has to be considered that of all heterotopias (n = 20) most of them were located in the cerebellum (45%; 9/20). Histologic changes of the cerebellum being associated to SBA in our study consisted of hypoplasia of the cerebellum or isolated dysplasia or aplasia of the vermis, dysplasia of the dentate nucleus and/or gyrification disorders as well as heterotopias, heterotaxias and immature germinal cell collections already described by others 8 while general Purkinje and granular cell depletion 53 was not further analyzed. Our findings are in line with those of Gilbert et al. describing frequent cerebellar heterotopias in patients with SBA. 8 While the relevance of cerebellar heterotopias – that are usually not apparent in MRIs – is unclear, 14 they could be an explanation for ataxia often visible in SBA patients. 54 It has to be considered that cerebellar heterotopias are observed in various developmental abnormalities of the CNS but are also not uncommon in normal developing brains. 19
Understanding SB pathomechanism including the sequence of occurrence of brain malformations in affected individuals is important, also in view of the promising approach to repair neural tube defects in utero.45,55 Current data that are based on limited observation periods and only small cohorts suggest that prenatal SBA surgery reduces but not eliminates the need for shunting and improves motor outcomes as well as it results in reversal of hindbrain herniation (the Chiari II malformation)45,55 which could be interesting regarding the intelligence quotients in SBA. To our knowledge there is no data on the brain pathology apart from Chiari II and hydrocephalus in such operated patients. Since hydrocephalus and shunting complications are associated with and potentially cause low IQ values56,57 further data on brain morphology and the cognitive profile of individuals with SBA following in utero closure are urgently needed. Moreover, it needs to be considered that a hydrocephalus can occur early, and that ependymal denudation can indicate hydrocephalus onset and generate cerebral pathology before an intrauterine repair in the GW19-26.
Conclusion
In conclusion we show that a wide range of cerebral malformations can be present in SBA patients in addition to the NTD. Not all of these are detected by MRI. We further show that hydrocephalus and Chiari II malformation can occur together or independent from each other. This finding challenges the usual hypothesis of sequential occurrence, but further analysis is limited due to difficult detection of mild forms of hydrocephalus and Chiari II. In prenatal NTD surgery it has to be considered that hydrocephalus can develop very early, even before GW19 when in utero surgery is usually performed. Prospective studies on the occurrence of brain malformations and hydrocephalus in individuals with SBA from early gestational age following prenatal surgery and in unoperated controls with NTDs are essential to resolve the knowledge gap in causes leading to hydrocephalus and the effect of abnormal CSF flow. The pathophysiology of SB is multifactorial. Correct phenotype nomenclature, further data on the sequence of prenatal malformation occurrence coupled with genotyping using modern genetic techniques will surely lead to a better knowledge on SB subtypes and pathophysiology. This will guide our future therapies.
Supplemental Material
sj-tif-1-pdp-10.1177_10935266211040500 - Supplemental material for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study
Supplemental material, sj-tif-1-pdp-10.1177_10935266211040500 for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study by Fabienne Paschereit, Kim Hannah Schindelmann, Michael Hummel, Joanna Schneider, Gisela Stoltenburg-Didinger and , Akira Nakagawara Kaindl in Pediatric and Developmental Pathology
Supplemental Material
sj-tif-2-pdp-10.1177_10935266211040500 - Supplemental material for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study
Supplemental material, sj-tif-2-pdp-10.1177_10935266211040500 for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study by Fabienne Paschereit, Kim Hannah Schindelmann, Michael Hummel, Joanna Schneider, Gisela Stoltenburg-Didinger and , Akira Nakagawara Kaindl in Pediatric and Developmental Pathology
Supplemental Material
sj-tif-3-pdp-10.1177_10935266211040500 - Supplemental material for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study
Supplemental material, sj-tif-3-pdp-10.1177_10935266211040500 for Cerebral Abnormalities in Spina Bifida: A Neuropathological Study by Fabienne Paschereit, Kim Hannah Schindelmann, Michael Hummel, Joanna Schneider, Gisela Stoltenburg-Didinger and , Akira Nakagawara Kaindl in Pediatric and Developmental Pathology
Footnotes
Acknowledgments
We thank the staff of the Institute of Neuropathology and Pathology who in the years 1974-2000 closely analyzed and documented the findings of fetuses with SB. We also thank Dr. Meske for his help and introduction in using a very new high-resolution scanner for histological specimen and the team of the Institute of Cell and Neurobiology for continuous support.
Author Contributions
AMK and GSD were responsible for the project conception. FP and AMK wrote the manuscript. FP, KHS and GSD collected patient data and incorporated them into a database. FP and KHS analyzed the data. GSD, JS and MH critically reviewed the data. All authors read, revised, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.