
Abstract
Objectives:
This study evaluates awareness of folic acid and neural tube defects, use of folic acid and knowledge of folic acid usage among female university students in Saudi Arabia.
Methods:
An analytical cross-sectional survey was conducted in the Jeddah branch of Saudi Electronic University. A total of 400 female students in the 19–45 years age group were contacted to participate in the study using a convenience sampling method. Eighty-eight students refused to participate, so 312 students were included in the study. Demographic characteristics of participants and their awareness, usage and knowledge of folic acid are presented as frequencies and percentages. Logistic regression analysis was used to compute crude odds ratios to show the association between demographic factors and knowledge of folic acid supplementation. A further adjusted odds ratio was calculated to control for other cofactors. A p-value < 0.05 was considered significant.
Results:
Overall, 81.1% (253/312) of respondents had heard of folic acid, 30.4% knew about neural tube defects, and 47.1% of respondents reported using folic acid supplements. Marriage was found to be associated with awareness of folic acid (adjusted odds ratio (95% confidence interval) = 2.64 (1.01–6.91)). Health sciences specialization and experience of pregnancy were associated with the usage of folic acid (adjusted odds ratio (95% confidence interval) = 3.46 (1.73–6.91) and adjusted odds ratio (95% confidence interval) = 6.70 (3.09–14.53), respectively). A bachelor’s and above education level was found to be associated with knowledge of folic acid deficiency leading to neural tube defects (adjusted odds ratio (95% confidence interval) = 2.03 (1.17–3.52)), and health sciences specialization was found to be associated with knowledge of natural sources of folic acid (adjusted odds ratio (95% confidence interval) = 2.33 (1.25–4.36)). Similarly, marriage was found to be associated with knowledge of the correct dosage of folic acid and timing of folic acid to prevent neural tube defects (adjusted odds ratio (95% confidence interval) = 6.34 (3.50–11.48) and adjusted odds ratio (95% confidence interval) = 3.45 (1.93–6.16), respectively). Experience of pregnancy was found to be an associated with good total knowledge of folic acid (adjusted odds ratio (95% confidence interval) = 3.05 (1.65–5.63); p = 0.0001).
Conclusion:
The study findings highlight the lack of awareness among female university students about the importance of folic acid usage in the prevention of neural tube defects. There is a need for interventional programs in universities to create awareness.
Introduction
Folate is a member of the vitamin B family. It is essential in the generation of new cells and the synthesis of new DNA, so its demand increases during pregnancy. 1 In 1965, Hibbard and Smithells 2 first suggested that deficiency of folates in the maternal diet is related to the occurrence of neural tube defects (NTDs). These are abnormalities that occur during neurulation, the process that forms the neural tube and ultimately the spinal cord, brain, and central nervous system. The two most common forms of NTDs are anencephaly (total or partial absence of brain) and spina bifida (presence of bony vertebral defect), causing serious mortality and disability among infants. 3 The process of neurulation is usually completed by 28 days postconception, that is, before the woman knows she is pregnant. 3 A number of studies have documented that NTDs can be significantly reduced by folate supplementation in the periconceptional period,4–6 suggesting that folate supplementation is the best way to reduce NTDs. The folic acid (FA) action mechanism is still under investigation; however, it is known that FA plays an important role in methionine synthase activity. FA provides methylation that converts homocysteine into methionine, without which homocysteine levels increase preventing the closure of neural tubes. 7
The World Health Organization (WHO) recommends that all women take an FA supplement (400 mcg daily) from the time they start planning to conceive until 12 weeks of gestation. 8 Furthermore, the daily dosage of FA should be increased up to 5 mg if the woman has already given birth to a child with a NTD. 8 Busby et al. 9 reported an overall mean decline in the prevalence of NTDs in the United Kingdom and Ireland by 32% (17%–44% decline) from 1989–1991 to 1999–2001 after the FA supplementation policy was implemented. 9 Furthermore, a mean reduction in the prevalence of NTDs by 17% (44% decline to a 4% rise) was reported in countries (the United Kingdom, Ireland, Netherland, Switzerland, Denmark, Norway, Portugal, Malta, and Finland) that introduced the policy of raising folate levels through supplementation or diet by 1999, compared to a mean reduction in the prevalence of NTDs by 9% (26% decline to a 12% rise) in countries (France, Spain, Austria, Belgium, Croatia, Germany, and Italy), which had no government policy to improve the folate levels of pregnant women. 9 According to a Cochrane review based on five clinical trials, FA supplementation alone or in combination with other micronutrients prevents the occurrence of NTDs (relative risk (RR) = 0.28, 95% CI = 0.15–0.52). 10
However, the recommendation of periconceptional supplementation of FA in planned pregnancies is not effective, as many women may not receive or respond to health promotion messages to commence supplementation preconceptionally, or may remain unaware of dietary modifications needed to achieve sufficient folate intake. 6 Furthermore, a large proportion of pregnancies in most countries are not planned, so women may not take FA supplements in the preconception period; thus, relying on supplementation alone is not sufficient to prevent NTDs. 9
The folate status of most women of childbearing age can be improved through fortification of staple foods with FA, which would also help to reduce socioeconomic inequalities in the prevalence of NTDs. 11 The implementation of mandatory fortification of cereal grains, resulted in a 27% reduction in NTDs in the United States from 1995–1996 (prefortification) to 1999–2000 (postfortification), 12 and a reduction of 46% in Canada from 1993–1997 (prefortification) to 2000–2002 (postfortification). 13 A meta-analysis of eight population-based observational studies examining FA food fortification (before and after) reported an estimated reduction in NTD incidence of 46% (95% CI = 37–54) and provided an estimate that FA fortification would prevent 13% of neonatal deaths attributed to congenital abnormalities in low-income countries. 14 Moreover, the prevalence of spina bifida is also significantly lower in countries with mandatory FA fortification policies than in those without such policies. 15
Saudi Arabia has programs that seek to reduce NTD incidences, including a national policy of the Ministry of Health and its food regulator for the mandatory fortification of flour with iron, FA, niacin, riboflavin, and thiamine starting from 2001 with the minimum requirement of 1.653% (16.53 g of FA for each kilogram of flour). 16 As all flours in Saudi Arabia are produced in industrial mills, 100% coverage of fortification has been achieved. 17 A decline in the incidence of NTDs was observed in Saudi Arabia from 1.9/1000 live births (1997–2000) to 0.76/1000 live births (2001–2005) 18 and 0.44/1000 live births (2001–2010). 19 However, a recent study by Majeed-Saidan et al. 20 reported an increase in NTDs to 0.90/1000 live births (2010–2013). 20
Studies from Saudi Arabia show inconsistency in the level of knowledge of FA supplementation among women. A few studies report that a high proportion of women are not aware of the importance of FA in preventing NTDs along with its timing,21–24 while other studies have reported a high level of awareness among married participants regarding the use of FA supplementation before conception and its role in preventing NTDs.25–27
The Saudi Arabia Ministry of Health website has educational content on “Planning for Pregnancy” in “Women’s Health” which describes key prepregnancy preparations such as taking 400 mcg of FA supplements daily before pregnancy and until 12 weeks of gestation. 28 Moreover, in Saudi Arabia, FA supplementation is easily available to the population via over-the-counter from pharmacies with or without a prescription.
The recent increase in the prevalence of NTDs in Saudi Arabia even after the fortification of flour suggests that there is a need to raise the awareness of women regarding the use of FA to reduce the occurrence of NTDs. Only one study has been conducted on university students in Saudi Arabia, 21 and a few studies conducted on the general population also include students as participants.23,24,26 Therefore, to fill the gap in the literature, this study was designed with a primary objective to determine the awareness, usage and knowledge levels related to FA among female university students. The secondary objective was to determine the association of demographic factors with the awareness, usage, and knowledge of participants regarding FA and NTDs. These analyses will help to identify the target population to focus on for the promotion of FA supplementation.
Materials and methods
Study area, study design, study population, inclusion criteria and exclusion criteria
An analytical cross-sectional survey was conducted among female students in the Jeddah branch of Saudi Electronic University (SEU) from March to November 2018. The inclusion criteria were female students aged 19–45 years who were willing to participate in the survey.
Sample size calculation
The sample size was calculated using the RaoSoft Sample size calculator, 29 taking the population (female students from all branches of specialization) size as 1500, margin of error as 5%, confidence level as 95% and response distribution as 50%. The sample size determined was 306, which was rounded to 310. Assuming, a 70% participation rate, the additional 90 participants were added to the sample size and 400 students were contacted for participation.
Sampling technique and procedure
A convenience sampling method was used to enroll the participants. The researcher contacted 400 students in the university cafeteria during breaks. Among 400 students, 88 students refused to participate in the study, and the remaining 312 (78%) students were provided the survey link for participation. The study protocol was reviewed and approved by the Institutional Review Board of Saudi Electronic University.
Study instrument and procedure
An online, close-ended, multiple-choice questionnaire was developed based on a previous study with slight modification to assess the awareness and knowledge of FA usage during pregnancy. 27 The first part of the questionnaire includes questions on the demographic characteristics (age, education, specialization, and marital status) and experience of pregnancy, and the second part assessed awareness, usage, and knowledge of FA. The awareness domain questions were “Have you ever heard of FA supplements” and “Have you ever heard of NTDs”; the question on FA use was “Do you take FA supplements or multivitamins containing FA prenatally or during current pregnancy regularly,” and the knowledge domain questions included “Can FA deficiency lead to NTDs,” “What is the timing of FA supplementation to prevent the occurrence of NTDs,” “What is the recommended dosage of FA,” and “What are the natural sources of FA” (Appendix 1). The researcher described the study objectives of the survey to the student. If the student agreed to participate, signed informed consent was obtained and the survey link was sent to the student on mobile devices for self-administration of the questionnaire under the researcher’s supervision.
Data management and analysis
The statistical package for social sciences (IBM SPSS version 24 software, Armonk, NY, USA) was utilized for statistical analysis. The demographic characteristics, awareness, usage of FA, and knowledge of FA are described as frequencies and percentages. Knowledge about FA was assessed using four closed-ended, multiple-choice questions. Polychotomous responses were dichotomized for analysis. Each correct answer was assigned a score of “1,” and incorrect answer as a score of “0.” The total score was calculated and considered “poor” if the score was “⩽2,” “fair” if the score was “3,” and “good” if the score was “4” for the overall knowledge level among the respondents.
The factors affecting FA awareness, FA usage, and knowledge about FA were assessed by computing crude odds ratios (ORs) and adjusted odds ratios (AORs) for other covariates (age, education level, specialization, marital status, and current or previous pregnancies) using logistic regression along with CIs. A p-value < 0.05 was considered statistically significant.
Results
Demographic characteristics of the study population
The response rate of the survey was 78% (312/400). The majority of the respondents (215, 68.9%) were in the 20–30 years age group, and almost half (160, 51.3%) were in the preparatory year of their educational course. Table 1 shows the sociodemographic characteristics of the study population.
Distribution of sociodemographic characteristics of total respondents, n = 312.

One-year course in university to teach students English, basic mathematics, and computer application.
Awareness and usage of FA
The details of awareness and usage of FA are shown in Table 2. Unadjusted and adjusted (for all five demographic variables) ORs with 95% CIs for awareness about FA supplementation and its usage are presented in Table 3. The respondents above 30 years of age were found to have significantly higher awareness and usage of FA than their younger colleagues (<30 years), but when adjusted for covariates, the AOR showed no difference in the level of awareness and usage of FA between the age groups. Marriage was found to be an independent factor associated with FA awareness (AOR (95% CI) = 2.64 (1.01–6.91); p = 0.047). The usage of FA was found to be significantly higher among married respondents, but when adjusted for covariates (age, education, specialization, and current or past pregnancies), AOR showed no difference in the usage of FA for marital status. Age, health sciences specialization, and pregnancy experience were found to be independent factors associated with FA supplement usage (AOR (95% CI) = 2.10 (1.12–3.94), AOR (95% CI) = 3.46 (1.73–6.91), and AOR (95% CI) = 6.70 (3.09–14.53), respectively).
Distribution of awareness and usage of folic acid among total respondents, n = 312.

FA: folic acid.
Association of sociodemographic factors with awareness and usage of folic acid among the total respondents, n = 312.

FA: folic acid; OR: odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
One-year course in university to teach students English, basic mathematics, and computer application.
p-value < 0.05 considered significant.
FA usage among respondents was assessed across different pregnancy statuses, that is, ongoing pregnancy, planning pregnancy, and non-pregnant. Of the participants who were pregnant or planning to be pregnant, only 61.1% with ongoing pregnancy and 44.4% who were planning pregnancy reported actively taking FA supplements (Figure 1).
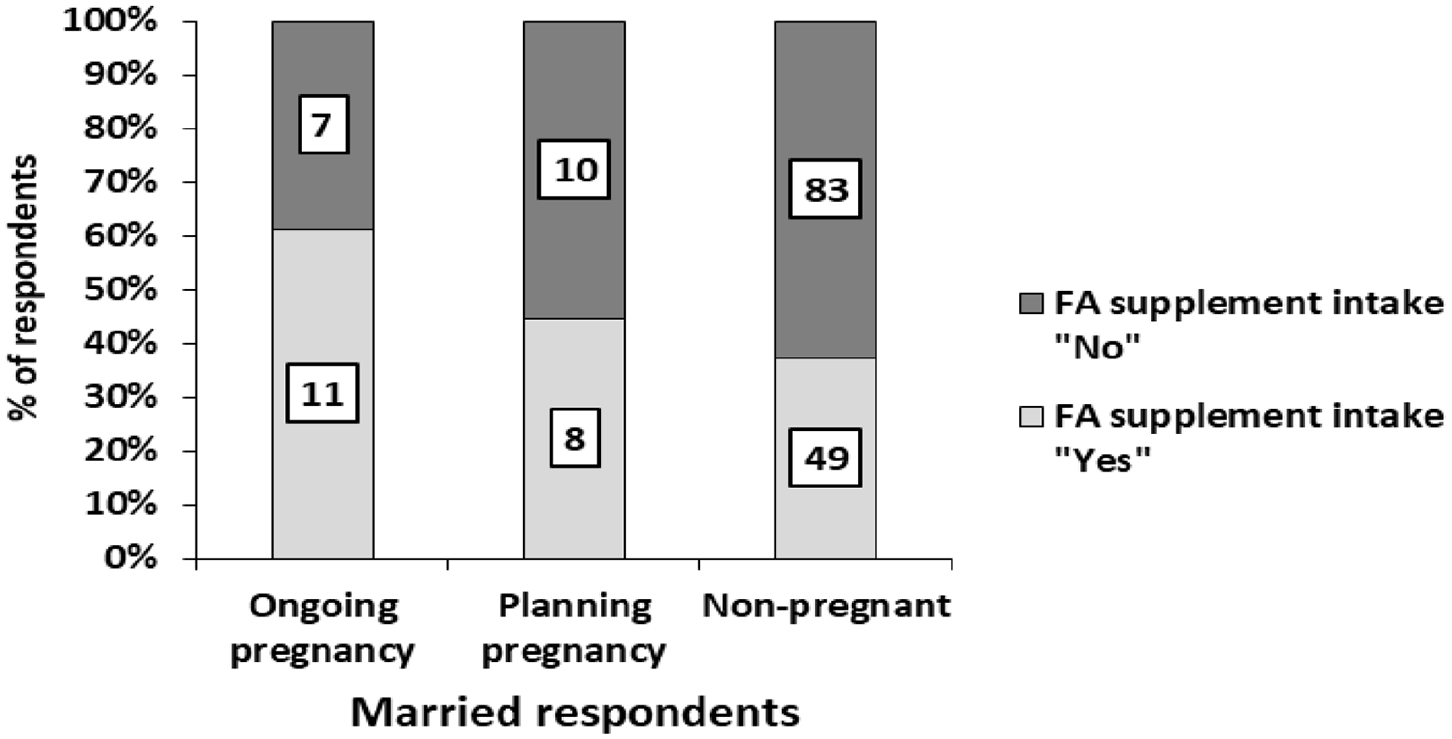
Distribution of FA supplement intake practiced among respondent with respect to their pregnancy status.
Knowledge about the usage of FA
The respondents who were aware of FA supplementation were assessed for their knowledge of FA usage and natural sources. No significant difference was observed between the demographic characteristics of the total study population (312 respondents) and the 253 respondents specifically assessed for their knowledge of FA usage except for their marital status.
Table 4 presents the respondents’ knowledge about the usage of FA. The highest correct responses were received regarding knowledge about natural sources of FA (151, 59.7%). Furthermore, 97 (38.3%) participants had a “poor” level of knowledge. The most common source of information about the usage of FA reported by respondents was health professionals and organizations (79, 31.2%).
Distribution of knowledge of folic acid usage among the respondents who were aware of folic acid, n = 253.

Correct responses: folic acid deficiency during pregnancy leads to—neural tube defects or spinal cord defects; timing of folic acid supplementation during pregnancy to prevent NTDs—3 months before conception and during the first 3 months of pregnancy; recommended dosage of folic acid supplement during pregnancy—400 mcg once a day; natural sources of folic acid—fruits and leafy vegetables.
Unadjusted and adjusted (for all five demographic variables) ORs with 95% CIs for knowledge about usage of FA supplements are presented in Table 5. A bachelor’s and above education level was found to be an independent factor associated with the correct knowledge of FA deficiency leading to NTDs (AOR (95% CI) = 2.03 (1.17–3.52); p = 0.012), and health sciences specialization was found to be an independent factor associated with the correct knowledge of natural sources of FA (AOR (95% CI) = 2.33 (1.25–4.36); p = 0.008). Similarly, marriage was found to be an independent factor associated with correct knowledge of dosage of FA along with the timing of FA supplementation to prevent NTDs (AOR (95% CI) = 6.34 (3.50–11.48); p = 0.0001 and AOR (95% CI) = 3.45 (1.93–6.16); p = 0.0001, respectively). The experience of pregnancy was found to be an independent factor associated with good total knowledge about FA (AOR (95% CI) = 3.05 (1.65–5.63); p = 0.0001).
Association of sociodemographic factors with knowledge of folic acid usage among the respondents who were aware of folic acid, n = 253.

FA: folic acid; OR: odds ratio; CI: confidence interval; AOR: adjusted odd ratio.
Correct responses: folic acid deficiency during pregnancy leads to—neural tube defects or spinal cord defects; timing of folic acid supplementation during pregnancy to prevent NTDs—3 months before conception and during the first 3 months of pregnancy; recommended dosage of folic acid supplement during pregnancy—400 mcg once a day; natural sources of folic acid—fruits and leafy vegetables.
One-year course in university to teach students English, basic mathematics, and computer application.
p-value < 0.05 considered significant.
The level of knowledge of FA usage was assessed across marital and pregnancy status, that is, unmarried and never pregnant, married and never pregnant, and married with pregnancy experience. The unmarried and never pregnant respondents (17, 18.5%) showed a low level of total knowledge score, while married and never pregnant respondents showed higher levels of knowledge of FA deficiency leading to NTDs (47.1%) and knowledge of correct timing of FA supplementation (58.8%) compared to their counterparts. The married respondents with pregnancy experience showed a higher level of knowledge regarding the correct dosage of FA supplementation (78.5%), natural sources of FA (61.1%), and total knowledge score (42.4%) than their counterparts (Figure 2).
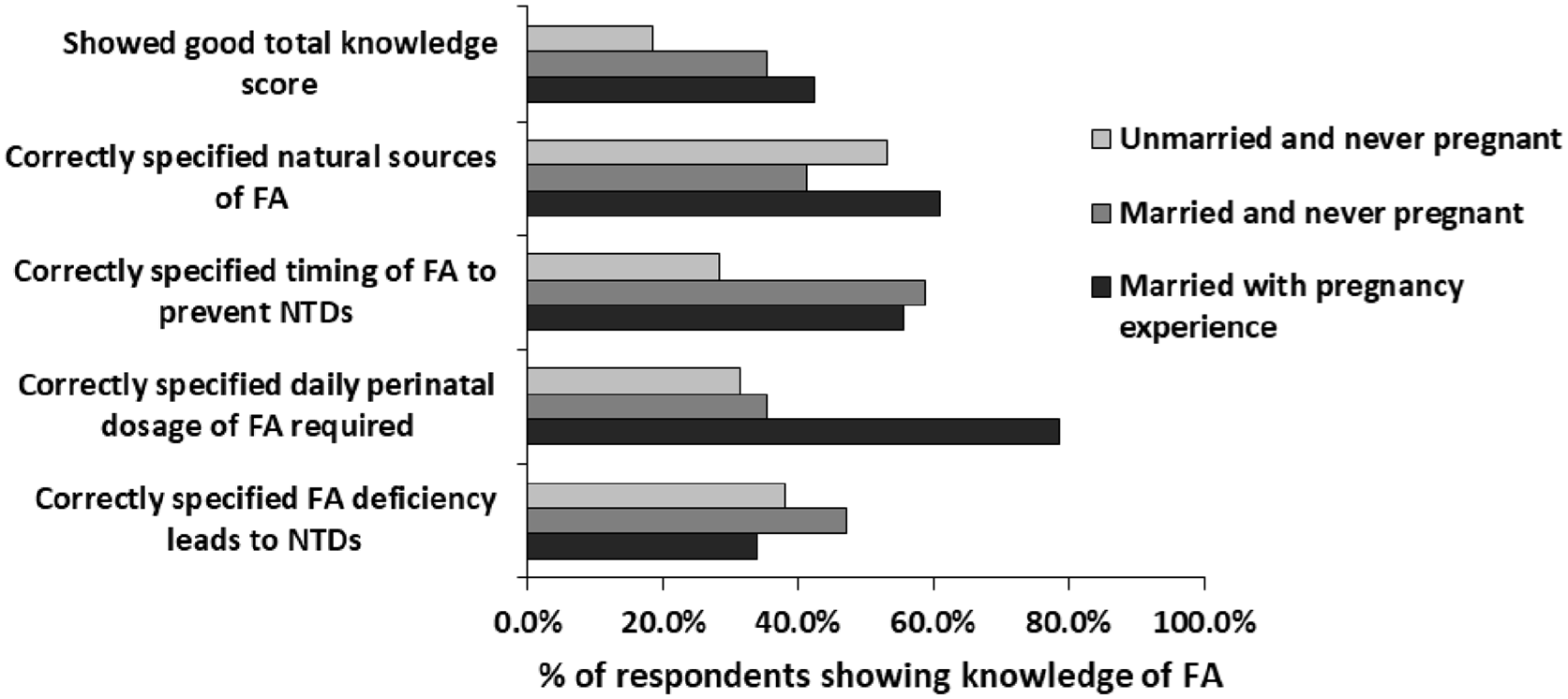
Distribution of respondents showing correct knowledge of FA with respect to their marriage and pregnancy experience.
Discussion
In this study, awareness of FA supplementation was high (81.1%), the usage of FA was comparatively low (47.1%), and the total knowledge score of FA was poor (38.3%) among female SEU students in Jeddah. Further FA supplement intake was reported by 61.1% of pregnant respondents and 44.4% of respondents who were planning for pregnancy. This study found that 47.4% of respondents had knowledge of the correct timing of FA supplementation to prevent NTDs, 57.3% of respondents had knowledge of correct FA dosages, and 61.3% of respondents correctly identified the natural sources of FA. The main source through which respondents received information about FA was healthcare professionals (31.2%).
The level of awareness of FA was lower in this study than in a study from Taipei 30 and studies from Saudi Arabia, in which awareness ranged between 89.3% and 93.1%.23,24,26 This discrepancy in the level of awareness of FA might be due to differences in the study population characteristics. In this study, nearly 50% of the study population was married, compared to 70%–100% in other studies. In this study, the respondents had a high level of awareness of FA as a supplement but had poor knowledge of FA deficiency leading to NTDs. These findings are consistent with those from other studies from Saudi Arabia24,31 and other countries,32,33 while a study done by AlAhmadi (2014) showed that a higher percentage of knowledge (71.2%) that NTDs can be reduced by FA supplementation. 25 In this study, although awareness of FA was high among the respondents, the usage of FA supplementation reported by respondents was low. Similar findings were reported by studies conducted in Saudi Arabia20,21,34 and other countries.35–38
The present findings suggest that respondents with specialization in health sciences gained knowledge through education, which helped to improve the intake of FA supplements. In this study, it was found that only pregnancy experience and not marital status are associated with the usage of FA supplements. A study on pregnancy-related health behavior among Saudi women reported that nearly 85% of pregnant Saudi women start prenatal care during the first trimester 39 and physicians prescribe FA supplementation, which results in higher usage of FA among pregnant women. Thus, FA supplementation in Saudi women at the time of conception is dependent mostly on fortified flour, but there lies uncertainty regarding the amount of FA consumed through it as fortification with FA is done only for flour and not for other staple foods such as rice and grains. The lack of an appropriate level of FA consumption during preconception may underlie the recent increase in NTDs in Saudi Arabia. 20
However, this study reports a comparatively higher intake of FA supplementation during pregnancy or pregnancy planning than previous studies from Saudi Arabia20,21,34 and other countries that reported low percentages of FA supplementation intake in their study population, especially during the periconceptional period.35–38 Knowledge pertaining to the proper timing of FA supplements is absolutely essential to ensure the normal development of the nervous system in infants, and to minimize the risk of NTDs. The present findings about knowledge of correct timing and dosage of FA supplementation to prevent NTD, and natural sources of FA are supported by another study from Saudi Arabia. 24 However, there is low precision in the estimates of the level of knowledge regarding FA dosage and timing to prevent NTDs from Saudi Arabia, as a few studies have reported lower level26,27,40 and a few studies have reported higher levels of knowledge than this study.25,41
According to WHO recommendations, FA supplementation should begin at the time women start planning to conceive and last until 12 weeks of gestation. 8 Moreover, a research study also reported that the process of neurulation is usually completed by 28 days postconception before a woman realizes she is pregnant. 3 Therefore, it is necessary to create awareness about FA supplement usage and its importance in reducing NTDs to married females, as in most countries, pregnancy is usually unplanned. 9
Presently, Saudi Arabia is undergoing transformation due to improvement in education, which has led to a smaller family size among the new generation. Periconceptional intake of FA is now feasible, as the new generation is opting for family planning. Moreover, in Saudi Arabia, it is mandatory for all couples to attend premarital counseling clinics to obtain general counseling, hepatitis B and HIV screening and testing for genetic disorders. 20 The government can utilize these premarital counseling clinics as a center to educate couples about the importance of FA supplementation during the preconception period. Furthermore, they can give counseling to women about the dosage and timing of FA intake to reduce NTDs along with imparting information about natural sources of FA and encouraging them to consume sufficient amounts of FA either through natural sources or through supplements. This approach will help to reduce the incidence of NTDs in Saudi Arabia in the future. Moreover, the study findings support the outcomes of a number of extant studies that also reported that doctors are typically the main source of information about FA.24,26,41
In the United States, FA education materials are promoted to the public through an annual event called Folic Awareness Week (National Birth Defects Prevention Network 2019). A similar annual event should be considered in Saudi Arabia, in which relevant stakeholders from across the country, including medical associations, healthcare workers, media organizations, and other volunteers can participate. They should conduct education programs such as public seminars focused on the importance of FA supplementation during the periconceptional period, and the timing of FA supplementation to prevent NTDs. Further advertisements through television or pamphlets describing the beneficial effects of FA supplementation and its natural source around the year can also help to expand the responsiveness of vulnerable, young, and unmarried women to the program. Public health programs and campaigns on the use of FA during the periconceptional period to prevent NTDs should be conducted regularly in high schools and universities.
Limitations
The study sample is non-representative of the population, as students were enrolled from a single branch of the university using a convenience sampling method. Therefore, the findings can only be generalized to Jeddah female university students. Second, the data collected by the participants are based on self-reporting which can lead to misclassification of outcomes; however, it is expected to be non-differential with respect to exposure. Third, demographic characteristics of the students who refused to participate were not collected for comparison with the participants who participated in the study. Finally, a pilot study was not carried out to test the validity of the questionnaire.
Conclusion
The study findings highlight the lack of awareness among female university students about the importance of FA usage in the prevention of NTDs. There is a need for annual awareness programs related to FA in universities.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211059682 – Supplemental material for Folic acid awareness and usage among females at Saudi Electronic University in Jeddah, Saudi Arabia
Supplemental material, sj-docx-1-smo-10.1177_20503121211059682 for Folic acid awareness and usage among females at Saudi Electronic University in Jeddah, Saudi Arabia by Mohammed AL-Mohaithef, Hadeel Alaslani, Nargis Begum Javed and Sriram Chandramohan in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express their sincere gratitude to the Deanship of Scientific Research, Saudi Electronic University, Riyadh, Kingdom of Saudi Arabia for their continuous support throughout this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board of Saudi Electronic University (ethical approval no. 4239).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.