
Abstract
The Cosmetic Ingredient Review (CIR) Expert Panel (Panel) reviewed the safety of barium sulfate, which functions as an opacifying agent in cosmetic products and is being used at concentrations up to 0.99% and 37% in rinse-off and leave-on products, respectively. The Panel noted that the history of safe medical use of barium sulfate indicates no significant toxicity concerns relating to systemic exposure to this ingredient. Furthermore, the extensive clinical experience of the Panel, including the results of numerous patch tests, indicates that barium salts do not have the potential to induce sensitization. The Panel noted that since salts of sulfuric acid can be irritating to the skin, cosmetic products containing barium sulfate should be formulated to be nonirritating. The Panel concluded that barium sulfate is safe in cosmetics in the present practices of use and concentration described in this safety assessment when formulated to be nonirritating.
Keywords
Introduction
The safety of barium sulfate, an inorganic sulfate, as used in cosmetics is reviewed in this safety assessment. Barium sulfate is reported to function as an opacifying agent in cosmetic products.
Chemistry
Definition and Structure
Barium sulfate (BaSO4, CAS No. 7727-43-7) is the barium salt of sulfuric acid. 1
Physical and Chemical Properties
Barium sulfate, available in the form of polymorphous crystals, has a molecular weight of 233.39 Da and is soluble in sulfuric acid but insoluble in water. 2
Method of Manufacture
Barium sulfate may be produced by treating a solution of a more water-soluble barium salt with sodium sulfate (salt cake). 3
Composition/Impurities
Barytes is the naturally occurring rock form of BaSO4. 4 A study was performed to characterize the mineralogical forms of barium and the trace heavy metal impurities in commercial barytes of different origins using electron probe microanalysis (EPMA), X-ray diffraction, and inductively coupled plasma mass spectrometry (ICP-MS). Qualitative EPMA results indicated the presence of different minerals in commercial barytes, including barite (BaSO4), barium feldspar, galena (PbS), pyrite (FeS2), sphalerite (ZnS), quartz (SiO2), and silicates. Quantitative EPMA confirmed that the barite crystals in the barytes contain some strontium and a little calcium, whereas trace heavy metals occur in the associated minerals. Analysis of aqua regia extracts of barytes samples by ICP-MS has indicated the presence of a large number of elements in the associated minerals. Arsenic, copper, and zinc concentrations correlate closely in all 10 samples. The heavy metals content of cosmetic-grade barium sulfate was not stated in this publication.
Chromium has been detected in commercial samples of pharmaceutical-grade barium sulfate at concentrations ranging from 0.45 to 1.06 µg/g. 5
Use
Cosmetic
Barium sulfate functions as an opacifying agent in cosmetic products. 1
According to information supplied to the Food and Drug Administration by industry as part of the Voluntary Cosmetic Registration Program (VCRP), barium sulfate is used mostly in leave-on products. 6 Results from a survey of ingredient use concentrations provided by the Personal Care Products Council (Council) in 2013 indicate that this ingredient is used at concentrations up to 0.99% (in skin cleansing products–rinse-off products) and 37% (in lipsticks–leave-on products). 7 Summarized data on frequency and concentration of use in cosmetics are presented in Table 1.
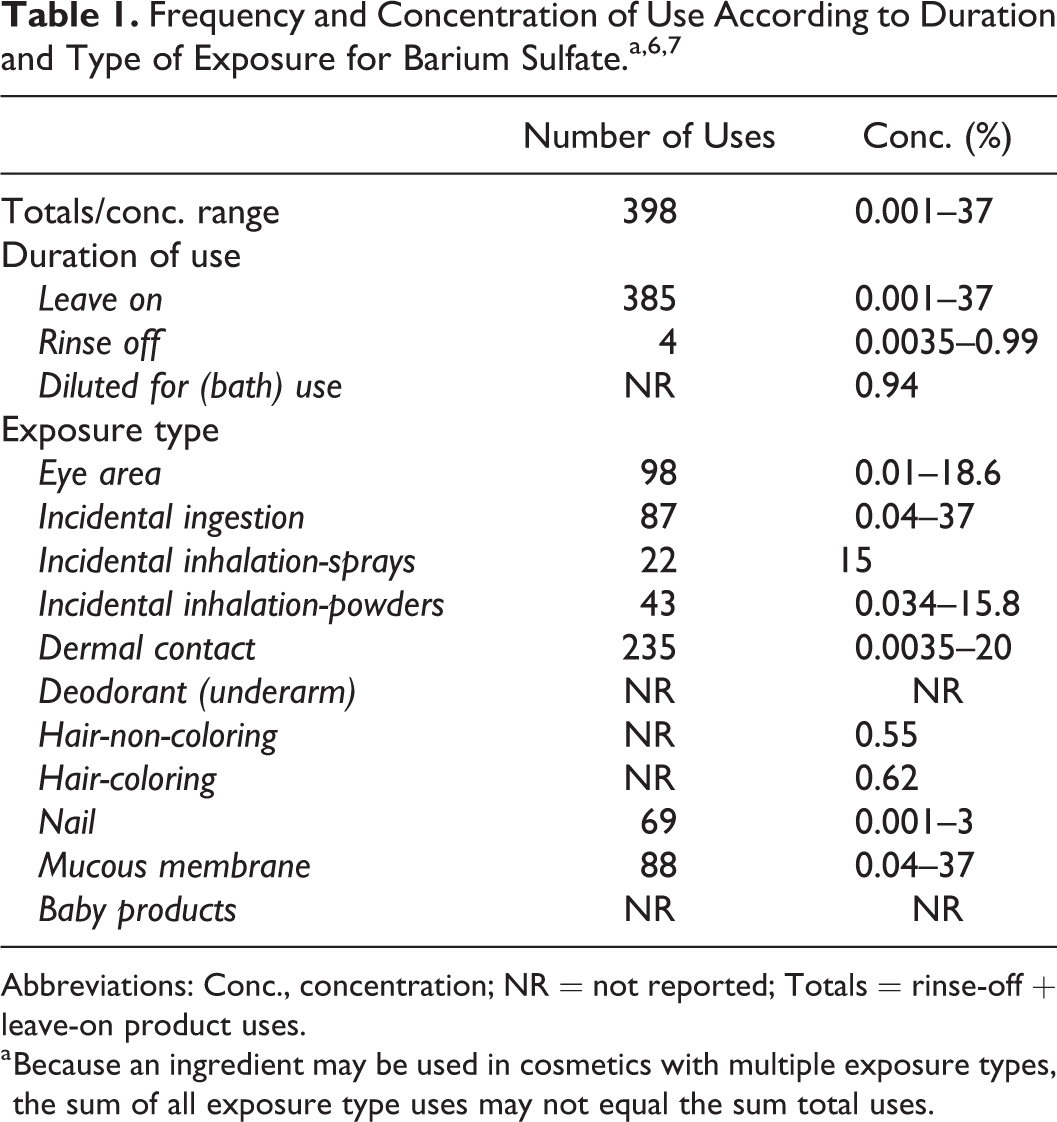
Abbreviations: Conc., concentration; NR = not reported; Totals = rinse-off + leave-on product uses.
a Because an ingredient may be used in cosmetics with multiple exposure types, the sum of all exposure type uses may not equal the sum total uses.
Cosmetic products containing barium sulfate may be applied to the skin and nails or, incidentally, may come in contact with the eyes and mucous membranes. Products containing these ingredients may be applied as frequently as several times per day and may come in contact with the skin or hair for variable periods following application. Daily or occasional use may extend over many years.
Barium sulfate is used at concentrations up to 15% in cosmetic products that are sprayed (perfumes) and at concentrations up to 15.8% in powders (face and dusting powders). Because this ingredient is used in products that are sprayed and in powders, it could be incidentally inhaled. In practice, 95% to 99% of the droplets/particles released from cosmetic sprays have aerodynamic equivalent diameters >10 µm, with propellant sprays yielding a greater fraction of droplets/particles below 10 µm, compared to pump spray. 8,9,10,11 Therefore, most droplets/particles incidentally inhaled from cosmetic sprays would be deposited in the nasopharyngeal and bronchial regions and would not be respirable (ie, they would not enter the lungs) to any appreciable amount. 8,9
With the exceptions of barium sulfide (under the conditions laid down in Annex III, Part I) and barium sulfate, barium salts are included on the list of ingredients that cosmetic products marketed within the European Union must not contain. 12 In particular, it should be noted that barium sulfate (with no limitations or requirements) appears on the list of coloring agents allowed for use in all cosmetic products marketed within the European Union.
Noncosmetic
There are a number of indirect food additive uses for which barium sulfate has been approved. 13 -16
Barium sulfate has been used as a gastrointestinal contrast agent in roentgenographic procedures. 17 Barytes (the naturally occurring rock form of BaSO4) has been referred to as the standard densification agent used in drilling fluids worldwide. 4
Toxicokinetics
In one study, rats inhaled barium sulfate at a concentration of 40 mg/m3, 5 days per week (5 h/day) for up to 2 months. 18 The rats were killed at 2-week intervals after the beginning of the exposure period, and the barium content of the lungs, lymph nodes, jaw, and femur was determined. Lymph transport was negligible. The barium content of bone increased initially and then gradually decreased during treatment. After 2 weeks of exposure, the barium content of the lungs was high but decreased rapidly and then increased considerably over the next 4 weeks of treatment.
In another study, groups of male Wistar rats were exposed (whole-body) 5 days per week (7 h/day) to barium sulfate dust at target aerosol concentrations of 37.5 µg/m3 and 75 µg/m3. 19 At each of 6 time points, 6 rats were drawn for dust burden measurements. Considering that dust deposited higher in the respiratory tract would have time to clear, animals used for lung and dust burden analyses were killed 66 hours after the end of exposure. In terms of milligram dust per gram of dry lung tissue, the burdens at the final exposure points were 24 mg/g and 17 mg/g for the high and low barium sulfate concentrations, respectively.
Following endotracheal administration of a barium sulfate containing mixture (formulated as a radiodiagnostic contrast agent for oral administration) into 220 Sprague-Dawley rats and 3 dogs, radiographic and histologic studies were performed. 20 The barium sulfate containing mixture (0.25 mL), under fluoroscopic control, was injected endotracheally into rats, and a 1.75 mL/kg dose of was administered endotracheally to dogs. The 0.25 mL dose was selected based on the results of a pilot study in which all 30 rats died after intratracheal administration of 0.5 mL of this mixture. After dosing with this mixture, radiographs were obtained immediately and at 15 and 30 minutes, at 1 hour, 2 hour, 3 hours, 4 hours, 5 hours, and 6 hours, and then 3 times daily for 1 week. All of the rats and 2 dogs were radiographed for a total of 9 months. The barium sulfate containing mixture was virtually cleared from the trachea and stem bronchi in 30 minutes. It cleared more slowly from the lungs of 3 dogs when compared to these data on rats. Additional study results are included in sections on Acute Intratracheal Toxicity and Inflammatory Response.
Toxicology
Acute Toxicity
Oral
Six groups of 16 to 26 young male CBL-Wistar albino rats (ages not stated) received the following 6 total doses of barium sulfate (150% w/v suspension), respectively, by intragastric cannula: 188, 225, 263, 300, 338, and 375 g/kg. 21 For each total dose, 40% was given initially, followed by 35% of the dose 3 hours later, and 25% 4 hours later. Fifty control rats were dosed with distilled water. Fifty experimental animals died from stomach rupture, and the mean LD50 was 307 ± 29 g/kg. Stomach rupture appeared to have been due, in part, to failure of the animal to pass barium sulfate along the gastrointestinal tract. In 90% of the animals, hemorrhagic areas were found in the gastric mucosa, mainly on the anterior and posterior surfaces. The adrenal glands were enlarged, the liver was small, and the stretched abdominal muscle had a watery consistency. It should be noted that, in pilot tests, barium sulfate doses ranging from 1 to 160 g/kg body weight did not cause death.
Intratracheal
Following endotracheal administration of a barium sulfate containing mixture (formulated as a radiodiagnostic contrast agent for oral administration) into 220 Sprague-Dawley rats and 3 dogs, radiographic and histologic studies were performed. 20 The barium sulfate containing mixture (0.25 mL), under fluoroscopic control, was injected endotracheally into rats, and a 1.75 mL/kg dose was administered endotracheally to dogs. The 0.25 mL dose was selected based on the results of a pilot study in which all 30 rats died after intratracheal administration of 0.5 mL of the mixture. After dosing with this mixture, the protocol dictated that all of the rats and 2 dogs would have been radiographed for a total of 9 months. However, 2 of the 3 dogs dosed with the barium sulfate containing mixture (1.75 mL/kg) died during the first 24 hours; both dogs had diffuse alveolarization of the contrast agent. Diffuse, but patchy, acinar filling resulted in a slow decrease in barium aggregates from the lungs of rats and the dog over a 9-month period. New infiltrates were found in 15% of the rats on serial follow-up.
Inflammatory Response
Inhalation
Groups of male Wistar rats were exposed (whole-body) 5 days per week (7 h/day) to barium sulfate dust (particle size = 4.3 µm) at target aerosol concentrations of 37.5 µg/m3 and 75 µg/m3. 19 At each of 6 time points, 12 rats were drawn, 6 for bronchoalveolar lavage (BAL) and 6 for dust burden measurements (See Toxicokinetics section). Of the 6 time points included in the protocol, only the following 4 were clearly defined: 42 days, 50 days, 70 days, and 90 days. Animals destined for BAL studies were killed 18 hours after completion of the final day of exposure for that time point. Three age-matched, sham-exposed animals were used as controls at each time point for each test condition in the lavage studies.
The results of BAL fluid analyses indicated that the time course of neutrophil recruitment during exposure to barium sulfate resembled that of lymph node burden; barium sulfate dust produced a low degree of inflammation at the last 3 time points of the higher (75 mg/m3) exposure concentration; the mean numbers of alveolar macrophages did not change significantly when compared to the background level in control animals; and animals exposed to barium sulfate dust had significantly higher numbers of lymphocytes in BAL fluid when compared to controls. 19
Histological sections from animals killed at timepoint 6 indicated that inhalation of barium sulfate elicited accumulation of pulmonary macrophages around the dust deposition sites. The highest concentrations of macrophages with phagocytosed dust were at the bifurcations of the terminal airways and bronchioles. In some cases, there was an accumulation of inflammatory cells, including fibroblasts in the interstitium. Some macrophages with their dust burdens had become interstitialized as well, with the lesions becoming microgranulomas. In most cases where centriacinar macrophage aggregations were found, the walls of surrounding alveoli appeared thickened, mainly due to the rounding of epithelial cells, indicative of type II cell hyperplasia. Barium sulfate did not show significant fibrogenic activity in this study. 19 The histopathological changes reported in this study were classified as minor, and there was little difference between results at the low (37.5 µg/m3) and high (75 µg/m3) exposure concentrations.
Subcutaneous
The effect of intrauterine, subcutaneous (s.c.) injection of sterile barium sulfate into rabbit fetuses was evaluated. Healthy pregnant rabbits (number not stated) of gestational periods ranging from 21 to 26 days were used. 22 Two fetuses were selected at random. The dorsum of the fetus was delivered and a sterile aqueous suspension of micro-opaque barium sulfate was injected into the subcutaneous tissue of each dorsolateral surface. The hysterotomy wounds were then closed. The pregnancy was allowed to progress and fetuses were removed at varying postoperative intervals for morphological studies. Similar s.c. injections were performed in newborn rabbits. The rabbits were killed at regular intervals and the morphology of the wounds was studied. Subpannicular injection of sterile barium sulfate in newborn rabbits produced an acute inflammatory response that was observed clearly at 24 hours and well-established by 48 hours. The process of repair had begun by day 4, whereby the appearance of proliferating capillaries and fibroblasts was observed. Both vascular and cellular components of the acute inflammatory response were more prominent in rabbit fetuses and appeared earlier (well-developed within 24 hours) when compared to newborn rabbits. The process of repair also began earlier in fetuses; the proliferation of capillaries and fibroblasts was prominent by 48 hours. By day 4, the lesion was compact, less cellular, and relatively avascular.
Endotracheal
A barium sulfate containing mixture (formulated as a radiodiagnostic contrast agent for oral administration) was administered endotracheally into 220 Sprague-Dawley rats (0.25 mL volume) and 3 dogs (1.75 mL/kg dose). 20 After dosing with this barium sulfate containing mixture, the protocol dictated that all of the rats and 2 dogs would have been radiographed for a total of 9 months. However, 2 of the 3 dogs dosed with the mixture died during the first 24 hours. Barium in the alveoli and a mild acute inflammatory response were observed in rats at microscopic examination. A few hours after instillation, macrophages were observed in the alveoli and subsequently became evident in thickened septa. Focal alveolar wall granulomata were also observed. After 3 months, focal areas of acute and chronic inflammatory cells with focal fibrosis persisted, and areas of atelectasis and emphysema were also observed. At 6 months, aggregates of macrophages containing barium were the main finding. At 9 months, nodules of phagocytic cells in bronchioles and perivascular structures persisted. At 9 months after instillation into the lungs, the same histological findings were observed in the dog.
Genotoxicity
The genotoxicity of barium sulfate was evaluated using murine fibroblasts in the in vitro single-cell gel (comet) assay. The fibroblasts were exposed for 5 hours (at 37°C) to barium sulfate at final concentrations ranging from 10 to 1,000 µg/mL. Vehicle control cultures were exposed to phosphate-buffered solution, and positive control cultures were exposed to 10 µmol/L hydrogen peroxide. A total of 50 randomly captured comets per treatment (25 cells from each slide) were examined using a fluorescence microscope. Barium sulfate did not increase cell mortality and was not genotoxic, that is, did not induce DNA breakage. The positive control caused a significant increase (P = 0.02) in tail moment, when compared to the negative control. 23 Barium sulfate (1 to 1,000 µg/mL) also was not genotoxic in human peripheral blood lymphocytes in the in vitro single-cell (comet) assay. 24
Clinical Data
Barium sulfate has been tested clinically for sensitization activity, and none has been detected. 25 Barium sulfate-induced granulomas have been associated with some diagnostic procedures in medical practice. These case reports and others relating to hypersensitivity reactions associated with diagnostic procedures involving barium sulfate are summarized below.
Exposure to barium sulfate occurs in miners of barium and its salts, workers in the lithopone industry, and in patients undergoing diagnostic roentgenography of the gastrointestinal tract. 26 Barium sulfate dust, when inhaled, leads to a benign form of pneumoconiosis (baritosis), which occurs primarily in miners and workers in the lithopone industry. Escape of barium sulfate from the digestive tract into the peritoneal cavity has been reported in patients with peptic ulcers undergoing X-ray studies. Barium granulomas have been reported in the appendix, sigmoid and peritoneum, and rectum in patients receiving barium enemas.
A 43-year-old patient was diagnosed with acute appendicitis, and barium sulfate was used in diagnostic studies, that is, upper gastrointestinal series and barium enema. 26 During these procedures, barium sulfate entered the appendix and escaped into the mesoappendix and adjacent periappendical fat. The resulting foreign-body granuloma was said to have been due to the escape of barium sulfate.
A case of barium sulfate-granulomatosis of the lung was reported for a 67-year-old man due to barium sulfate aspiration during an X-ray investigation of the stomach. 27 In the lung parenchyma, multiple granulomas were observed in groups of alveoli where barium sulfate had been deposited.
Barium enema examination is a frequently performed radiographic procedure, and this procedure was reported to caused barium granuloma of the rectum in 2 patients (males 75 and 78 years old). 28 Rectal intramural extravasation of barium occurs as a result of asymmetric enema balloon inflation and impaction of the enema tip against the rectal mucosa. The lesions appeared as indurated, ulcerated rectal masses that resembled carcinoma on endoscopic examination. Deep mucosal biopsy results demonstrated no malignancy or barium sulfate crystals in tissue macrophages. Radiographs showed persistent soft-tissue barium in the rectum.
A severe anaphylactic reaction was observed in a 51-year-old female patient with cancer at approximately 5 to 10 minutes after starting a barium enema. 29 The barium enema mixture contained barium sulfate, sodium benzoate, potassium sorbate, citric acid, sodium saccharin, ethyl maltol, vegetable gum, sorbitol, simethicone, and natural and artificial flavors. It was stated that the anaphylactic reaction could have been an IgE-mediated hypersensitivity reaction to one of the barium sulfate suspension constituents. The patient had a history of prior sensitizing exposure to barium radiographic contrast material. No skin prick test reaction, that is, no cutaneous hypersensitivity, to diluted sodium benzoate, potassium sorbate, or whole liquid barium sulfate suspension was detected. The patient declined further provocation testing. The authors noted that the patient’s severe reaction to barium may have been partly attributable to the following 3 factors: (1) her history of atopy and prior medication allergy, (2) a prior sensitizing exposure to barium sulfate, and (3) possible increased absorption of allergens into the bloodstream through the recurrently bleeding ulcerated carcinoma of the sigmoid colon.
Two children developed hypersensitivity reactions of varying severity following upper GI series. 30 The first case involved an 11-year-old boy with documented anaphylaxis, following exposure to fish and peanuts, and multiple food intolerances. The patient experienced oral swelling and a red swollen tongue after drinking 150 mL of 45% weight/weight barium sulfate. The absence of sequelae after prior upper GI series that involved drinking barium sulfate was noted. Endoscopic biopsies from the upper and lower GI tracts established the diagnosis of eosinophilic gastroenteropathy. The second case involved a 7-year-old girl with a history of mild allergy to penicillin (hives) but no other known allergies. After drinking 150 mL of 45% barium sulfate, she developed urticaria on her face, trunk, and lower extremities.
Cases of patients with a “magenta colon” from radiologic barium have been reported every 3 to 4 years. 31 This condition can occur with either upper or lower barium contrast studies, resolves over 4 to 7 days and can be present without visible residual barium. It was noted that most reactions are mild, but, occasionally, are severe enough to hamper determining whether there is true colitis. The severe reaction is characterized by edema, loss of all vascular markings, and redness to almost a magenta color but without ulcerations, friability, necrosis, or exudate. Biopsies show inflammatory changes.
Summary
Barium sulfate is reported to function as an opacifying agent in cosmetic products. According to the VCRP, barium sulfate is used mostly in leave-on products. Results from a survey of ingredient use concentrations provided by the Council indicate that this ingredient is used at concentrations up to 0.99% in rinse-off products (skin cleansing products) and up to 37% in leave-on products (lipsticks).
Barium sulfate may be produced by treating a solution of barium salt with sodium sulfate (salt cake). Chromium has been detected in commercial samples of pharmaceutical grade barium sulfate at concentrations ranging from 0.45 to 1.06 µg/g.
Rats inhaled barium sulfate (40 mg/m3) for up to 2 months, and barium was detected in the bone and lungs. Lymph transport was said to have been negligible.
Following endotracheal administration of a barium sulfate containing mixture (formulated as a radiodiagnostic contrast agent for oral administration) into rats (0.25 mL volume) and dogs (1.75 mL/kg dose), the ingredient was virtually cleared from the trachea and stem bronchi in 30 minutes. Barium was detected in the alveoli at microscopic examination. Two of the three dogs died during the first 24 hours, but all rats survived. Diffuse alveolarization of the test material was observed in both dogs. Furthermore, a mild acute inflammatory response and a chronic inflammatory response involving the alveoli and bronchioles were also observed in rats and dogs.
Groups of young male CBL-Wistar albino rats received a 150% w/v barium sulfate suspension orally at doses up to 375 g/kg. A mean LD50 of 307 ± 29 g/kg was reported.
Subpannicular injection of sterile barium sulfate in newborn rabbits produced an acute inflammatory response that was observed clearly at 24 hours and well established by 48 hours. In another study, groups of Wistar rats were exposed repeatedly to barium sulfate dust for up to 90 days. Barium sulfate dust produced a low degree of inflammation at an exposure concentration of 75 mg/m3.
Barium sulfate was not genotoxic to murine fibroblasts. It was also not genotoxic in human peripheral blood lymphocytes in the in vitro comet assay.
Barium sulfate dust, when inhaled, leads to a benign form of pneumoconiosis (baritosis), which occurs primarily in miners and workers in the lithopone industry. Barium sulfate-granulomatosis of the lung, appendix, and other tissues has occurred during radiographic procedures. Additionally, though rare, hypersensitivity reactions have been reported after radiographic procedures that involve dosing with barium sulfate.
Discussion
The Panel noted that the long history of safe medical barium sulfate use mitigated concerns about systemic toxicity resulting from cosmetic product exposure. Furthermore, the extensive clinical experience of the Panel, including the results of numerous patch tests, indicates that barium salts do not have the potential to induce sensitization. The Panel noted that salts of sulfuric acid can be irritating to the skin. Therefore, in the absence of skin irritation data on barium sulfate, it was determined that cosmetic products containing barium sulfate should be formulated to be nonirritating. Barium sulfate is being used in leave-on products (lipsticks) at concentrations up to 37%.
Barium sulfate is being used at concentrations up to 15% in cosmetic products that are sprayed (perfumes) and at concentrations up to 15.8% in powders (face and dusting powders). The Panel discussed the issue of incidental inhalation exposure from propellant and pump sprays and powders, and considered pertinent data indicating that incidental inhalation exposures to this ingredient in such cosmetic products would not cause adverse health effects. The data considered include a characterization of the potential for this ingredient to cause acute toxicity (inhalation and oral), inflammation, and genotoxicity. The Panel noted that 95% to 99% of droplets/particles produced in cosmetic aerosols would not be respirable to any appreciable amount. Coupled with the small actual exposure in the breathing zone and the concentrations at which the ingredients are used, the available information indicates that incidental inhalation would not be a significant route of exposure that might lead to local respiratory or systemic effects. A detailed discussion and summary of the Panel’s approach to evaluating incidental inhalation exposures to ingredients in cosmetic products is available at http://www.cir-safety.org/cir-findings.
Conclusion
The CIR Panel concluded that barium sulfate is safe in cosmetics in the present practices of use and concentration described in this safety assessment when formulated to be nonirritating.
Footnotes
Authors’ Note
Unpublished sources cited in this report are available from the Executive Director, Cosmetic Ingredient Review, 1620 L Street, NW, Suite 1200, Washington, DC 20036, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The articles in this supplement were sponsored by the Cosmetic Ingredient Review.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Cosmetic Ingredient Review is financially supported by the Personal Care Products Council.