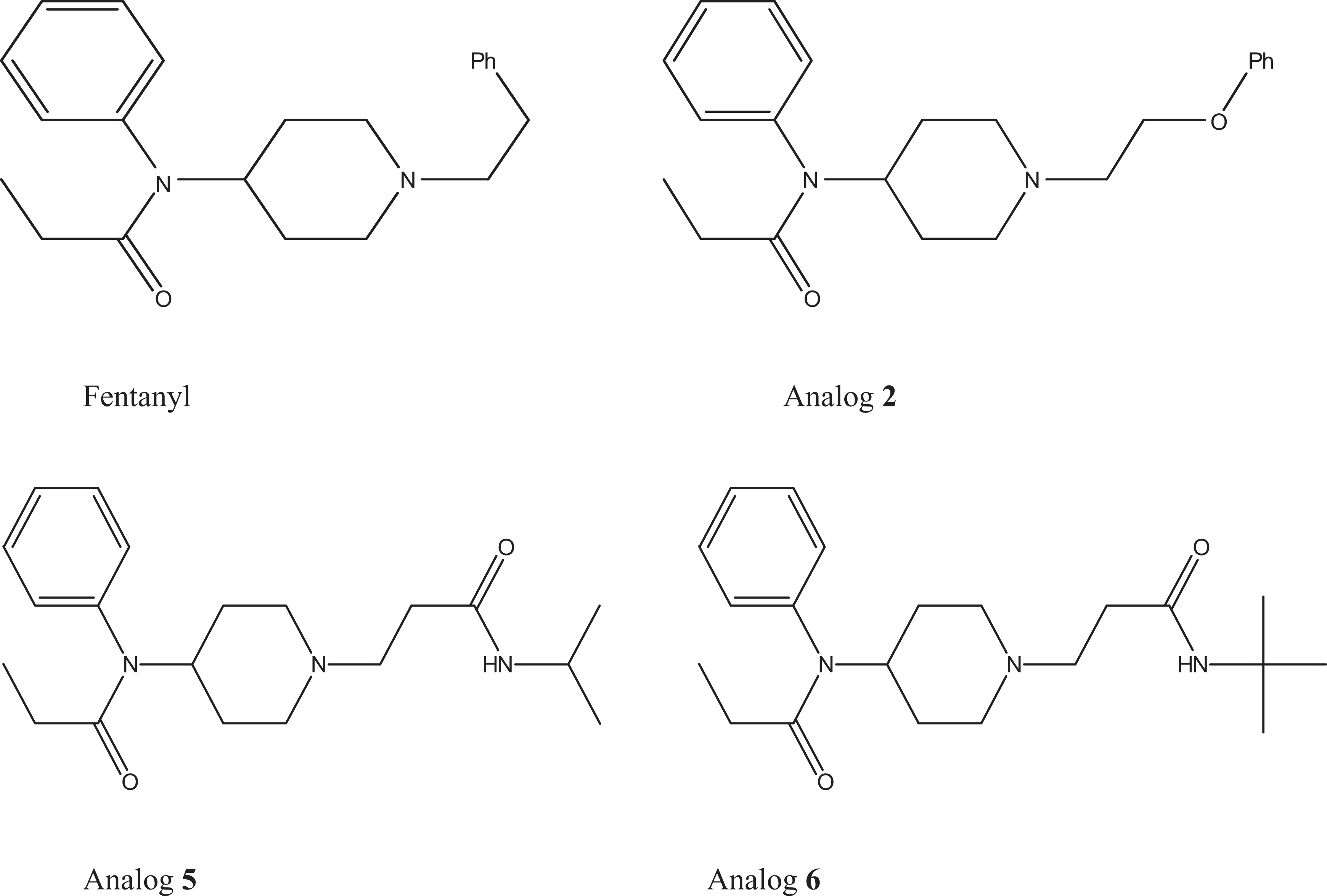
Synthesis and bioefficacy of fentanyl and its 8 new 1-substituted analogs (1-8) were earlier reported by us. Of these 8 compounds, N-(1-(2-phenoxyethyl)-4-piperidinyl)propionanilide (2), N-isopropyl-3-(4-(N-phenylpropionamido)piperidin-1-yl)propanamide (5), and N-t-butyl-3-(4-(N-phenylpropionamido)piperidin-1-yl) propanamide (6) were found to be more effective and less toxic compared to fentanyl. The present study reports the acute effect of fentanyl (0.50 Median Lethal Dose (LD50); intraperitoneal) and its 3 analogs (2, 5, and 6) on various biochemical and oxidative parameters in mice and various physiological parameters in rats. Blood alkaline phosphatase (1 hour and 7 days) and urea levels (1 hour) were significantly elevated by fentanyl, while alanine aminotransferase levels (1 hour) were increased by both fentanyl and analog 2 compared to the corresponding control. Increase in partial pressure of carbon dioxide and decrease in partial pressure of oxygen were also caused by fentanyl and analog 2 (1 hour). Analog 6 alone elevated malondialdehyde levels in the brain, liver, and kidney tissues (7 days). The LD50 of fentanyl and analogs 2, 5, and 6 were found to be 0.879, 87.88, 69.80, and 55.44 mg/kg, respectively, in rats. Significant decrease in heart rate, mean arterial pressure, respiratory rate (RR), and neuromuscular transmission was produced by fentanyl and analog 2, while analog 5 decreased the RR alone. The changes, particularly the respiratory depression, were found to be reversed by naloxone, a μ-receptor antagonist. Thereby, indicating involvement of μ-receptor mediated effects of the compounds. To conclude, all the analogs were found to be less toxic compared to fentanyl, suggesting their possible role in pain management.
The opioid analgesics are the best option for the management of severe and chronic pain. One such analgesic is fentanyl, which is a morphine-like narcotic analgesic agent. Fentanyl is a μ-receptor agonist and is 50- to 300-folds more potent than morphine.1 Compared to morphine, strong potency of fentanyl is mainly attributed to its high lipophilicity, which facilitates its entry into the central nervous system.2 It is a fully synthetic potent opioid analgesic with a rapid onset and short duration of action. Synthesis of fentanyl further resulted in better understanding of the structure–activity relationship of opioid analgesics. This prompted synthesis of many similar compounds with greater potency and higher safety margins.3 Immediately after synthesis of fentanyl, a series of 4-anilidopiperidine derivatives were synthesized, which were structurally analogous to fentanyl and acted as μ-opioid receptor agonists. Among these analogs, alfentanil, sufentanil, and remifentanil found clinical applications in humans.4
Fentanyl is mainly metabolized in the liver through oxidative deamination at the piperidinic nitrogen to form N-dealkylated norfentanyl. Its minor metabolites are despropionylfentanyl, hydroxyfentanyl, and hydroxynorfentanyl. All metabolites have negligible pharmacological activity.5,6 The majority of opioids are excreted as metabolites through kidney. Due to renal transformation of these compounds, effect on kidney is anticipated, which could be clinically presented.7 Less than 10% of fentanyl is excreted unchanged by the kidney.8 Acute and repeated exposure of opioids has been found to deplete reduced glutathione (GSH) levels and increase lipid peroxidation, protein oxidation, and oxidative DNA damage.9–14 Fentanyl is known to affect various physiological parameters such as respiratory rate (RR), heart rate (HR), blood pressure (BP), and so on.15 The majority of opioids are known to cause respiratory depression, which restricts their clinical use. Furthermore, the degree of respiratory depression largely varies with different opioids, and currently, there are no opioids which are free from such undesirable effects.16 Therefore, development of new opioid analgesics with minimal side effects may be more desirable for pain management.
We have earlier reported the synthesis and bioefficacy of fentanyl and its 8 new 1-substituted analogs (1-8) in mice.17,18 Of these 8 analogs tested, N-(1-(2-phenoxyethyl)-4-piperidinyl)propionanilide (2), N-isopropyl-3-(4-(N-phenylpropionamido) piperidin-1-yl)propanamide (5), and N-t-butyl-3-(4-(N-phenylpropionamido)piperidin-1-yl)propanamide (6) were found to be more effective and less toxic compared to fentanyl. The present study reports the acute effect of fentanyl and its 3 analogs (2, 5, and 6) on various biochemical, oxidative, and physiological parameters in rodents.
Materials and Methods
Animals
Male Swiss albino mice (25-30 g) and male Wistar rats (200-250 g) bred in the animal facility of Defence Research and Development Establishment (DRDE), Gwalior, were used in the study. The animals were housed in polypropylene cages on dust-free rice husk as the bedding materials, with free access to food (Ashirwad Brand, Chandigarh, India) and water ad libitum. They were maintained in controlled environmental conditions of ambient temperature (22°C ± 2°C) and relative humidity of 40% to 60% in a 12:12 light:dark cycle. The care and maintenance of the animals were as per the approved guidelines of the Committee for the Purpose of Control and Supervision of Experiments on Animals, India. Animal experiments were carried out with the approval of Institutional Animal Ethical Committee.
Chemicals
All chemicals used in the present study were of the highest purity. Dimethyl sulfoxide (DMSO; CAS 67-68-5), naloxone hydrochloride (naloxone; CAS 51481-60-8), reduced GSH (CAS 70-18-8), glutathione disulfide (GSSG; CAS 27025-41-8), and thiobarbituric acid (CAS 504-17-6) were purchased from Sigma-Aldrich Inc (St Louis, Missouri). N-ethylmaleimide (CAS 128-53-0) and metaphosphoric acid were purchased from Acros Organics (Morris, NJ, USA). O-phthaldialdehyde was purchased from Fluka Chemika (Buchs, Switzerland). Potassium chloride, sodium dodecyl sulfate, and sodium hydroxide were purchased from Merck Ltd (Mumbai, India). Glacial acetic acid was purchased from Ranbaxy (New Delhi, India). Fentanyl and its 1-substituted analogs (2, 5, and 6) were synthesized and characterized by IR, 1H NMR, 13C NMR, GC-MS, and elemental analysis in the Synthetic Chemistry Division of DRDE, as per the methods discussed elsewhere.17,18 The structures of the compounds are as follows:
Treatment
Thirty mice were divided into 5 groups of 6 animals each as follows: (1) control (DMSO), (2) fentanyl (0.50 LD50), (3) analog 2 (0.50 LD50), (4) analog 5 (0.50 LD50), and (5) analog 6 (0.50 LD50). All compounds were dissolved in DMSO and administered intraperitoneally (IP) in a volume of <10 mL/kg body weight. The LD50 (IP) of fentanyl and its analogs 2, 5, and 6 was determined during our previous studies.17,18 Blood was collected at 1 hour, 24 hours, and 7 days postexposure for various biochemical estimations. Blood was drawn from the retro-orbital plexus of anesthetized animals using heparinized capillary. After 7 days, animals were killed by cervical dislocation and the brain, heart, lung, liver, kidney, and spleen were excised quickly. The organs were rinsed in 0.9% saline, blotted, and weighed to determine organ-to-body weight index (OBI). The OBI was calculated as the ratio of organ weight × 100 and the animal body weight. Oxidative stress markers were measured in the brain, liver, and kidney homogenate.
In a separate study, 24-hour LD50 (IP) of fentanyl and its analogs was determined in male Wistar rats by Dixon’s up-and-down method using 4 to 6 animals for each LD50.19 Thereafter, 36 rats were divided into 9 groups of 4 animals each as follows: (1) control (DMSO), (2) naloxone (5 mg/kg; subcutaneous; 10 minutes), (3) fentanyl (0.50 LD50), (4) analog 2 (0.50 LD50), (5) analog 5 (0.50 LD50), (6) analog 6 (0.50 LD50), (7) naloxone + fentanyl, (8) naloxone + analog 2, and (9) naloxone + analog 5. Various physiological parameters were measured as discussed below (see “Physiological Studies” section).
Clinical Biochemistry
Various biochemical parameters such as alkaline phosphatase (ALP; U/L), aspartate aminotransferase (AST; U/L), alanine aminotransferase (ALT; U/L), lactate dehydrogenase (LDH; U/L), creatinine (mg/dL), urea (mg/dL), and albumin (g/dL) were measured in blood plasma using commercial diagnostic kits (Merck Ltd). All measurements were made on Ultraviolet Visible spectrophotometer (Thermo Electron Corp., Rugby, Warwickshire, UK).
Blood Gas Analysis
Blood gas and electrolyte analyses were performed 1 hour and 7 days postexposure using an automated blood gas analyzer (Roche OPTI CCA, Mannheim, Germany). Various parameters measured were pH, partial pressure of oxygen (Po2; mm Hg), partial pressure of carbon dioxide (Pco2; mm Hg), bicarbonate (HCO3−; mmol/L), sodium (Na+; mmol/L), and potassium (K+, mmol/L).
Hematological Variables
Hematological variables, namely, white blood cells, red blood cells (RBCs), hematocrit (HCT), mean cell volume, mean cell hemoglobin concentration, mean cell hemoglobin, platelets, and hemoglobin, were measured 1 hour, 24 hours, and 7 days postexposure by an automated hematology analyzer (Beckman-Coulter Inc., Porterville, CA, USA ).
Oxidative Stress Markers
Oxidative stress markers such as GSH and GSSG levels and lipid peroxidation were measured in the brain, liver, and kidney homogenate. Reduced GSH and GSSG were estimated by the method of Hissin and Hilf20 and expressed as μmol/g wet tissue. Lipid peroxidation was assessed by measuring malondialdehyde (MDA) levels, and the values were expressed as nmol/g wet tissue.21
Urine Analysis
Pooled urine samples were collected 24 hours and 7 days postexposure from animals housed in metabolic cages and examined for pH, protein, glucose, ketones, urobilinogen, bilirubin, and blood using urinalysis strips (Multistix SG) of Siemens Healthcare Diagnostics Ltd (Baroda, India).
Physiological Studies
All animals were anesthetized with urethane (1.6 g/kg; IP) and various physiological parameters were recorded on Grass Polygraph (model 7-16 P-35) at different time intervals. Briefly, the trachea was cannulated and connected to a pneumotachometer (Fleisch tube) to record the RR through a differential pressure transducer (Hugo Sachs Elektronik, March-Hugstetten, Germany). The carotid artery was cannulated to record BP with a low-level DC preamplifier (model 7 P1) attached to a pressure transducer (P 23 1D; Gould Laboratories, Pitman, NJ, USA). Mean arterial pressure (MAP) was calculated from the recorded BP. Pulse signals were also fed into a tachograph preamplifier (type 7 P4) to record the HR. The neuromuscular transmission (NMT) studies were carried out to record the twitch responses. The gastrocnemius muscle was opened and the sciatic nerve was stimulated with a supramaximal voltage (1-10 V) of 0.2 milliseconds duration at a frequency of 0.2 Hz using a Grass stimulator model S 11 (Grass Instrument, Quincy, MA, USA). The twitch response of muscle was recorded using a force transducer (model FT0-3). Rectal temperature (RT) was measured using a rectal probe. Animals were allowed to stabilize prior to various treatments.
Statistics
The results are expressed as mean ± standard error of the mean (SEM). The data were analyzed by 1-way analysis of variance followed by Dunnett test. Statistical significance was drawn at *P < 0.05 and **P < 0.01 levels using SigmaStat software (SPSS Inc., Chicago, IL, USA).
Results
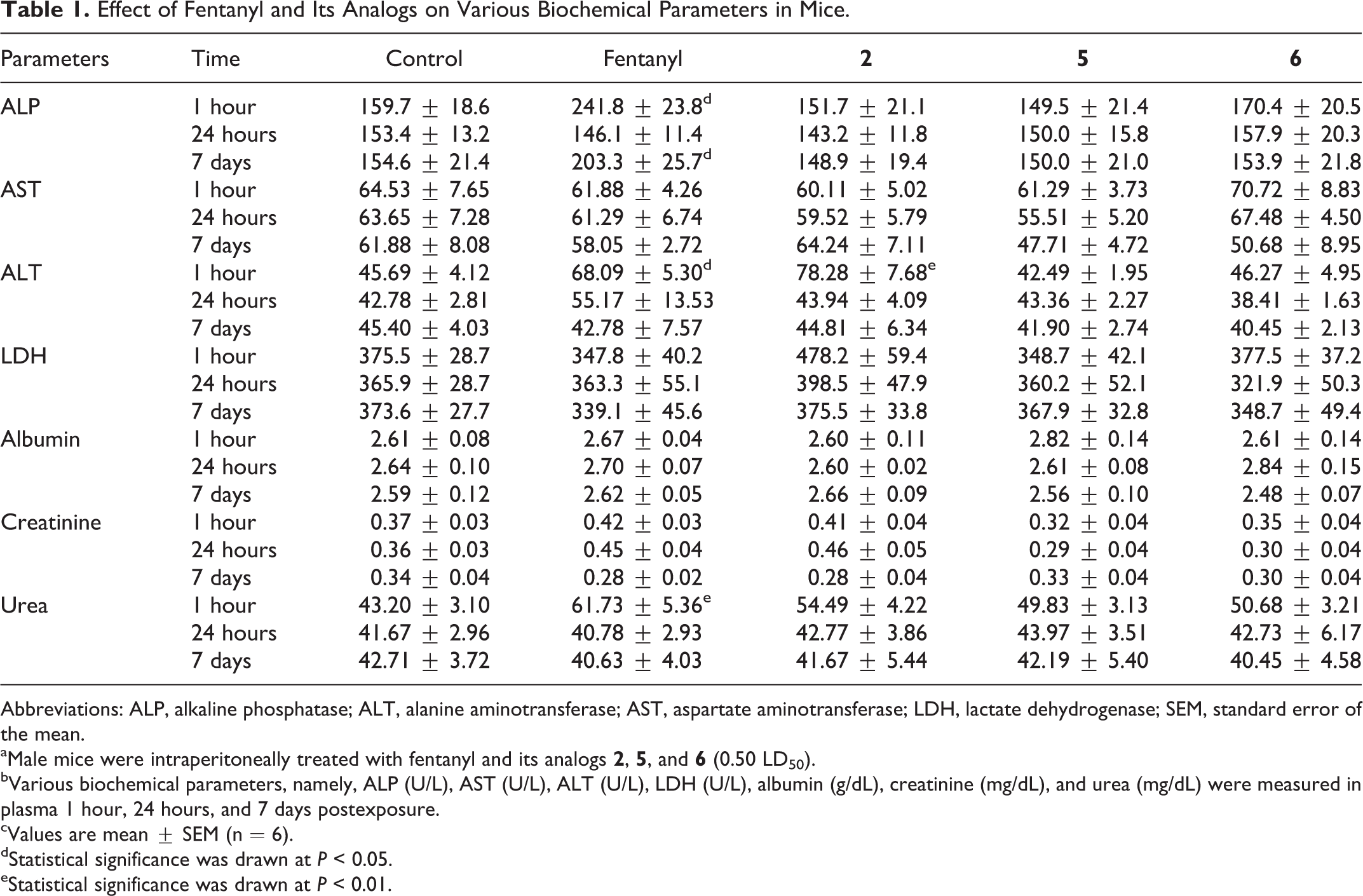
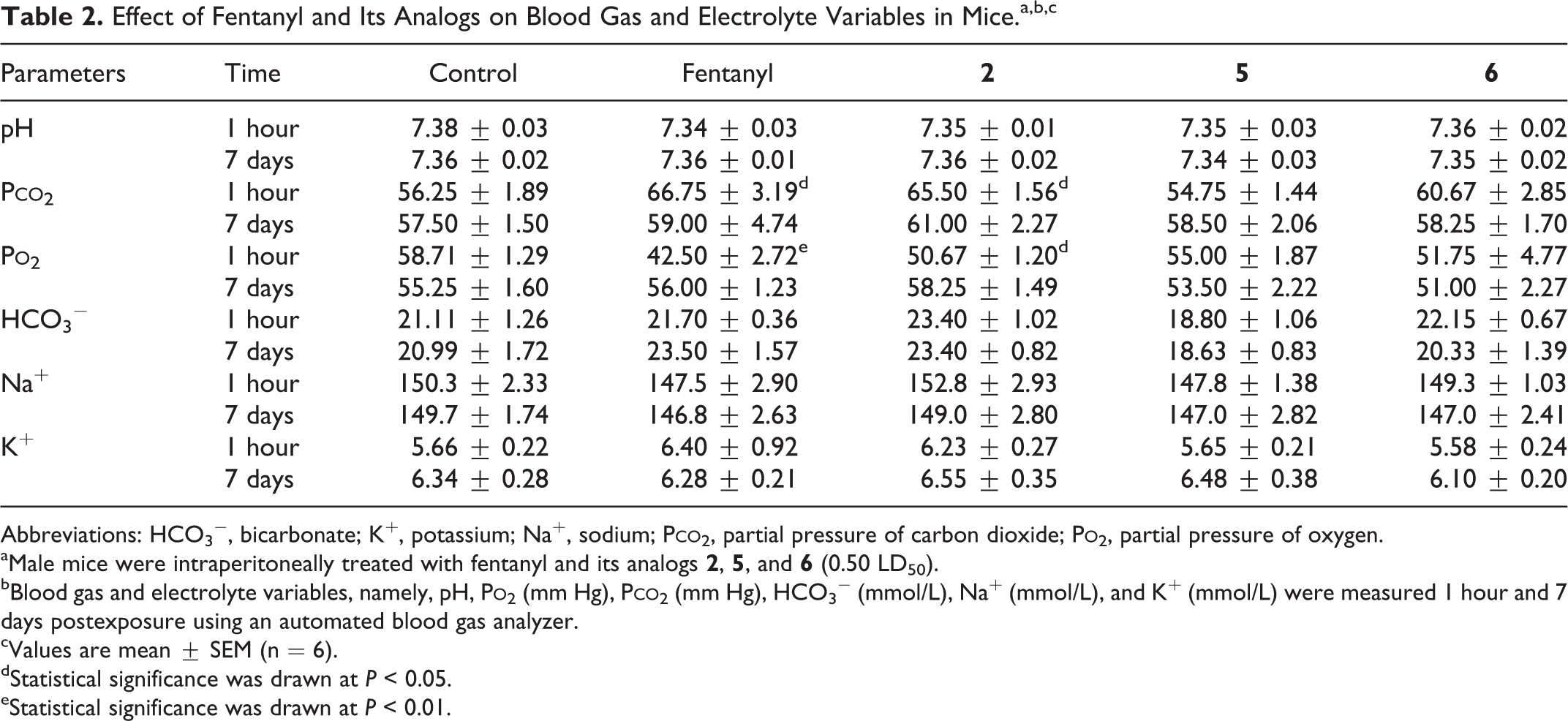
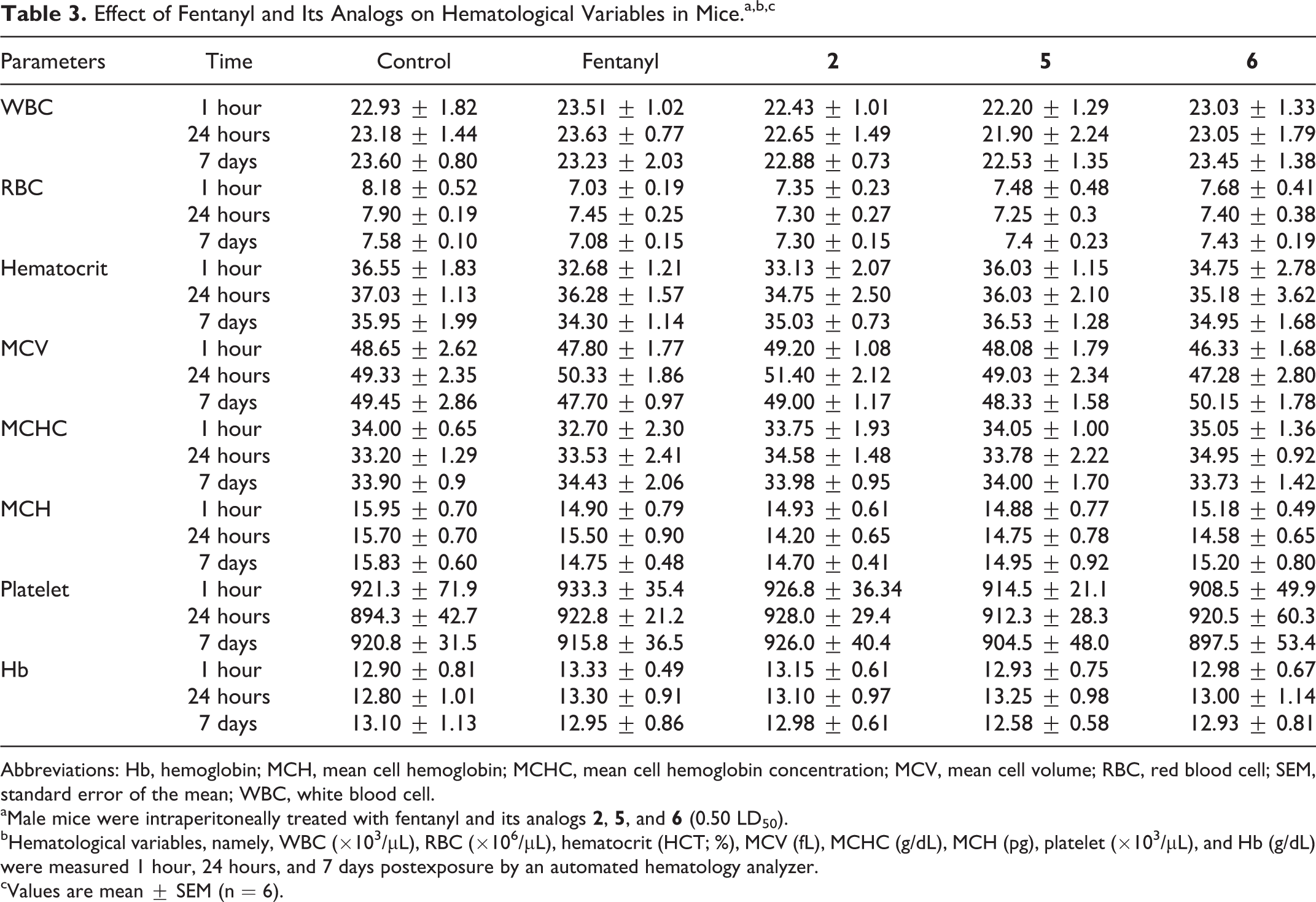
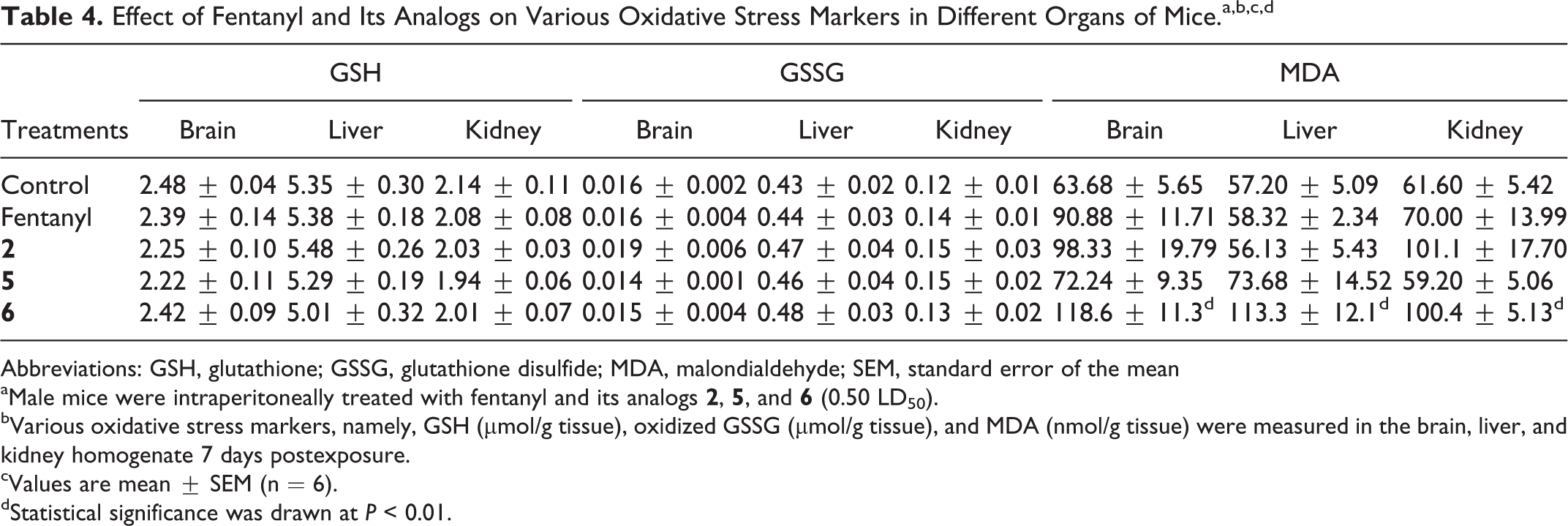
Table 1 shows the effect of fentanyl and its analogs on different biochemical parameters in mice blood. The ALP levels were significantly elevated in the fentanyl-treated group 1 hour and 7 days postexposure, while the ALT levels were increased in the fentanyl and analog 2-treated groups 1 hour postexposure, compared to the corresponding control. The urea levels were significantly increased in the fentanyl-treated group alone 1 hour postexposure. Table 2 shows the effect of fentanyl and its analogs on blood gas and electrolyte variables. Fentanyl and its analog 2 significantly increased Pco2 and decreased Po2 after 1 hour compared to control. Fentanyl and its analogs did not show any significant change in various hematological variables when observed 1 hour, 24 hours, and 7 days postexposure (Table 3). Effects of fentanyl and its analogs on GSH, GSSG, and MDA levels in different organs of mice are shown in Table 4. There was no change in GSH and GSSG levels in brain, liver, and kidney in all the treated groups. However, MDA levels in the brain, liver, and kidney were found to be increased in analog 6-treated group alone after 7 days exposure. Animals treated with fentanyl and its analogs did not show any change in the body weight, OBI, and urine analysis (data not shown).
Effect of Fentanyl and Its Analogs on Various Biochemical Parameters in Mice.
Parameters
Time
Control
Fentanyl
2
5
6
ALP
1 hour
159.7 ± 18.6
241.8 ± 23.8d
151.7 ± 21.1
149.5 ± 21.4
170.4 ± 20.5
24 hours
153.4 ± 13.2
146.1 ± 11.4
143.2 ± 11.8
150.0 ± 15.8
157.9 ± 20.3
7 days
154.6 ± 21.4
203.3 ± 25.7d
148.9 ± 19.4
150.0 ± 21.0
153.9 ± 21.8
AST
1 hour
64.53 ± 7.65
61.88 ± 4.26
60.11 ± 5.02
61.29 ± 3.73
70.72 ± 8.83
24 hours
63.65 ± 7.28
61.29 ± 6.74
59.52 ± 5.79
55.51 ± 5.20
67.48 ± 4.50
7 days
61.88 ± 8.08
58.05 ± 2.72
64.24 ± 7.11
47.71 ± 4.72
50.68 ± 8.95
ALT
1 hour
45.69 ± 4.12
68.09 ± 5.30d
78.28 ± 7.68e
42.49 ± 1.95
46.27 ± 4.95
24 hours
42.78 ± 2.81
55.17 ± 13.53
43.94 ± 4.09
43.36 ± 2.27
38.41 ± 1.63
7 days
45.40 ± 4.03
42.78 ± 7.57
44.81 ± 6.34
41.90 ± 2.74
40.45 ± 2.13
LDH
1 hour
375.5 ± 28.7
347.8 ± 40.2
478.2 ± 59.4
348.7 ± 42.1
377.5 ± 37.2
24 hours
365.9 ± 28.7
363.3 ± 55.1
398.5 ± 47.9
360.2 ± 52.1
321.9 ± 50.3
7 days
373.6 ± 27.7
339.1 ± 45.6
375.5 ± 33.8
367.9 ± 32.8
348.7 ± 49.4
Albumin
1 hour
2.61 ± 0.08
2.67 ± 0.04
2.60 ± 0.11
2.82 ± 0.14
2.61 ± 0.14
24 hours
2.64 ± 0.10
2.70 ± 0.07
2.60 ± 0.02
2.61 ± 0.08
2.84 ± 0.15
7 days
2.59 ± 0.12
2.62 ± 0.05
2.66 ± 0.09
2.56 ± 0.10
2.48 ± 0.07
Creatinine
1 hour
0.37 ± 0.03
0.42 ± 0.03
0.41 ± 0.04
0.32 ± 0.04
0.35 ± 0.04
24 hours
0.36 ± 0.03
0.45 ± 0.04
0.46 ± 0.05
0.29 ± 0.04
0.30 ± 0.04
7 days
0.34 ± 0.04
0.28 ± 0.02
0.28 ± 0.04
0.33 ± 0.04
0.30 ± 0.04
Urea
1 hour
43.20 ± 3.10
61.73 ± 5.36e
54.49 ± 4.22
49.83 ± 3.13
50.68 ± 3.21
24 hours
41.67 ± 2.96
40.78 ± 2.93
42.77 ± 3.86
43.97 ± 3.51
42.73 ± 6.17
7 days
42.71 ± 3.72
40.63 ± 4.03
41.67 ± 5.44
42.19 ± 5.40
40.45 ± 4.58
Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDH, lactate dehydrogenase; SEM, standard error of the mean.
aMale mice were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50).
bVarious biochemical parameters, namely, ALP (U/L), AST (U/L), ALT (U/L), LDH (U/L), albumin (g/dL), creatinine (mg/dL), and urea (mg/dL) were measured in plasma 1 hour, 24 hours, and 7 days postexposure.
cValues are mean ± SEM (n = 6).
dStatistical significance was drawn at P < 0.05.
eStatistical significance was drawn at P < 0.01.
Effect of Fentanyl and Its Analogs on Blood Gas and Electrolyte Variables in Mice.a,b,c
Parameters
Time
Control
Fentanyl
2
5
6
pH
1 hour
7.38 ± 0.03
7.34 ± 0.03
7.35 ± 0.01
7.35 ± 0.03
7.36 ± 0.02
7 days
7.36 ± 0.02
7.36 ± 0.01
7.36 ± 0.02
7.34 ± 0.03
7.35 ± 0.02
Pco2
1 hour
56.25 ± 1.89
66.75 ± 3.19d
65.50 ± 1.56d
54.75 ± 1.44
60.67 ± 2.85
7 days
57.50 ± 1.50
59.00 ± 4.74
61.00 ± 2.27
58.50 ± 2.06
58.25 ± 1.70
Po2
1 hour
58.71 ± 1.29
42.50 ± 2.72e
50.67 ± 1.20d
55.00 ± 1.87
51.75 ± 4.77
7 days
55.25 ± 1.60
56.00 ± 1.23
58.25 ± 1.49
53.50 ± 2.22
51.00 ± 2.27
HCO3−
1 hour
21.11 ± 1.26
21.70 ± 0.36
23.40 ± 1.02
18.80 ± 1.06
22.15 ± 0.67
7 days
20.99 ± 1.72
23.50 ± 1.57
23.40 ± 0.82
18.63 ± 0.83
20.33 ± 1.39
Na+
1 hour
150.3 ± 2.33
147.5 ± 2.90
152.8 ± 2.93
147.8 ± 1.38
149.3 ± 1.03
7 days
149.7 ± 1.74
146.8 ± 2.63
149.0 ± 2.80
147.0 ± 2.82
147.0 ± 2.41
K+
1 hour
5.66 ± 0.22
6.40 ± 0.92
6.23 ± 0.27
5.65 ± 0.21
5.58 ± 0.24
7 days
6.34 ± 0.28
6.28 ± 0.21
6.55 ± 0.35
6.48 ± 0.38
6.10 ± 0.20
Abbreviations: HCO3−, bicarbonate; K+, potassium; Na+, sodium; Pco2, partial pressure of carbon dioxide; Po2, partial pressure of oxygen.
aMale mice were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50).
bBlood gas and electrolyte variables, namely, pH, Po2 (mm Hg), Pco2 (mm Hg), HCO3− (mmol/L), Na+ (mmol/L), and K+ (mmol/L) were measured 1 hour and 7 days postexposure using an automated blood gas analyzer.
cValues are mean ± SEM (n = 6).
dStatistical significance was drawn at P < 0.05.
eStatistical significance was drawn at P < 0.01.
Effect of Fentanyl and Its Analogs on Hematological Variables in Mice.a,b,c
Parameters
Time
Control
Fentanyl
2
5
6
WBC
1 hour
22.93 ± 1.82
23.51 ± 1.02
22.43 ± 1.01
22.20 ± 1.29
23.03 ± 1.33
24 hours
23.18 ± 1.44
23.63 ± 0.77
22.65 ± 1.49
21.90 ± 2.24
23.05 ± 1.79
7 days
23.60 ± 0.80
23.23 ± 2.03
22.88 ± 0.73
22.53 ± 1.35
23.45 ± 1.38
RBC
1 hour
8.18 ± 0.52
7.03 ± 0.19
7.35 ± 0.23
7.48 ± 0.48
7.68 ± 0.41
24 hours
7.90 ± 0.19
7.45 ± 0.25
7.30 ± 0.27
7.25 ± 0.3
7.40 ± 0.38
7 days
7.58 ± 0.10
7.08 ± 0.15
7.30 ± 0.15
7.4 ± 0.23
7.43 ± 0.19
Hematocrit
1 hour
36.55 ± 1.83
32.68 ± 1.21
33.13 ± 2.07
36.03 ± 1.15
34.75 ± 2.78
24 hours
37.03 ± 1.13
36.28 ± 1.57
34.75 ± 2.50
36.03 ± 2.10
35.18 ± 3.62
7 days
35.95 ± 1.99
34.30 ± 1.14
35.03 ± 0.73
36.53 ± 1.28
34.95 ± 1.68
MCV
1 hour
48.65 ± 2.62
47.80 ± 1.77
49.20 ± 1.08
48.08 ± 1.79
46.33 ± 1.68
24 hours
49.33 ± 2.35
50.33 ± 1.86
51.40 ± 2.12
49.03 ± 2.34
47.28 ± 2.80
7 days
49.45 ± 2.86
47.70 ± 0.97
49.00 ± 1.17
48.33 ± 1.58
50.15 ± 1.78
MCHC
1 hour
34.00 ± 0.65
32.70 ± 2.30
33.75 ± 1.93
34.05 ± 1.00
35.05 ± 1.36
24 hours
33.20 ± 1.29
33.53 ± 2.41
34.58 ± 1.48
33.78 ± 2.22
34.95 ± 0.92
7 days
33.90 ± 0.9
34.43 ± 2.06
33.98 ± 0.95
34.00 ± 1.70
33.73 ± 1.42
MCH
1 hour
15.95 ± 0.70
14.90 ± 0.79
14.93 ± 0.61
14.88 ± 0.77
15.18 ± 0.49
24 hours
15.70 ± 0.70
15.50 ± 0.90
14.20 ± 0.65
14.75 ± 0.78
14.58 ± 0.65
7 days
15.83 ± 0.60
14.75 ± 0.48
14.70 ± 0.41
14.95 ± 0.92
15.20 ± 0.80
Platelet
1 hour
921.3 ± 71.9
933.3 ± 35.4
926.8 ± 36.34
914.5 ± 21.1
908.5 ± 49.9
24 hours
894.3 ± 42.7
922.8 ± 21.2
928.0 ± 29.4
912.3 ± 28.3
920.5 ± 60.3
7 days
920.8 ± 31.5
915.8 ± 36.5
926.0 ± 40.4
904.5 ± 48.0
897.5 ± 53.4
Hb
1 hour
12.90 ± 0.81
13.33 ± 0.49
13.15 ± 0.61
12.93 ± 0.75
12.98 ± 0.67
24 hours
12.80 ± 1.01
13.30 ± 0.91
13.10 ± 0.97
13.25 ± 0.98
13.00 ± 1.14
7 days
13.10 ± 1.13
12.95 ± 0.86
12.98 ± 0.61
12.58 ± 0.58
12.93 ± 0.81
Abbreviations: Hb, hemoglobin; MCH, mean cell hemoglobin; MCHC, mean cell hemoglobin concentration; MCV, mean cell volume; RBC, red blood cell; SEM, standard error of the mean; WBC, white blood cell.
aMale mice were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50).
bHematological variables, namely, WBC (×103/μL), RBC (×106/μL), hematocrit (HCT; %), MCV (fL), MCHC (g/dL), MCH (pg), platelet (×103/μL), and Hb (g/dL) were measured 1 hour, 24 hours, and 7 days postexposure by an automated hematology analyzer.
cValues are mean ± SEM (n = 6).
Effect of Fentanyl and Its Analogs on Various Oxidative Stress Markers in Different Organs of Mice.a,b,c,d
GSH
GSSG
MDA
Treatments
Brain
Liver
Kidney
Brain
Liver
Kidney
Brain
Liver
Kidney
Control
2.48 ± 0.04
5.35 ± 0.30
2.14 ± 0.11
0.016 ± 0.002
0.43 ± 0.02
0.12 ± 0.01
63.68 ± 5.65
57.20 ± 5.09
61.60 ± 5.42
Fentanyl
2.39 ± 0.14
5.38 ± 0.18
2.08 ± 0.08
0.016 ± 0.004
0.44 ± 0.03
0.14 ± 0.01
90.88 ± 11.71
58.32 ± 2.34
70.00 ± 13.99
2
2.25 ± 0.10
5.48 ± 0.26
2.03 ± 0.03
0.019 ± 0.006
0.47 ± 0.04
0.15 ± 0.03
98.33 ± 19.79
56.13 ± 5.43
101.1 ± 17.70
5
2.22 ± 0.11
5.29 ± 0.19
1.94 ± 0.06
0.014 ± 0.001
0.46 ± 0.04
0.15 ± 0.02
72.24 ± 9.35
73.68 ± 14.52
59.20 ± 5.06
6
2.42 ± 0.09
5.01 ± 0.32
2.01 ± 0.07
0.015 ± 0.004
0.48 ± 0.03
0.13 ± 0.02
118.6 ± 11.3d
113.3 ± 12.1d
100.4 ± 5.13d
Abbreviations: GSH, glutathione; GSSG, glutathione disulfide; MDA, malondialdehyde; SEM, standard error of the mean
aMale mice were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50).
bVarious oxidative stress markers, namely, GSH (μmol/g tissue), oxidized GSSG (μmol/g tissue), and MDA (nmol/g tissue) were measured in the brain, liver, and kidney homogenate 7 days postexposure.
cValues are mean ± SEM (n = 6).
dStatistical significance was drawn at P < 0.01.
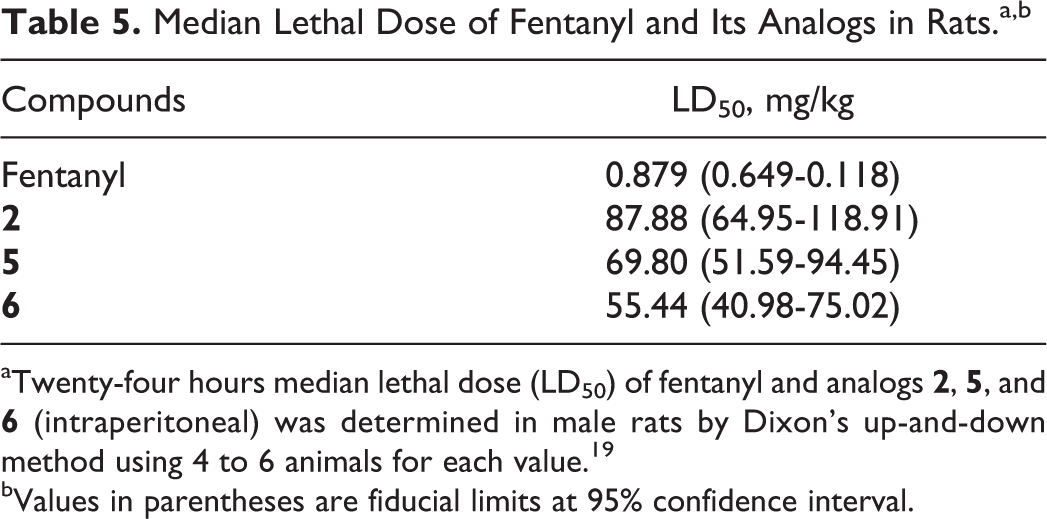
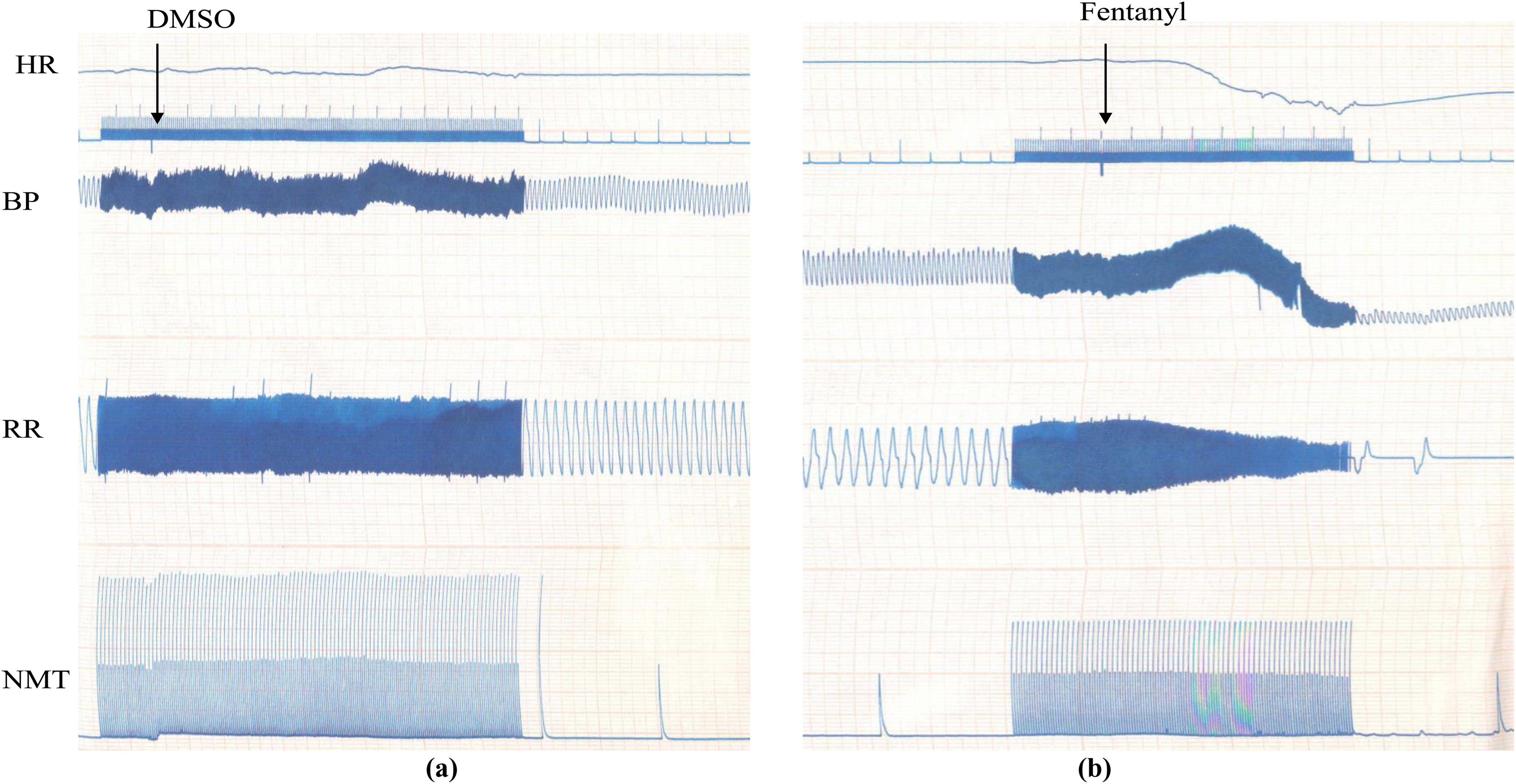
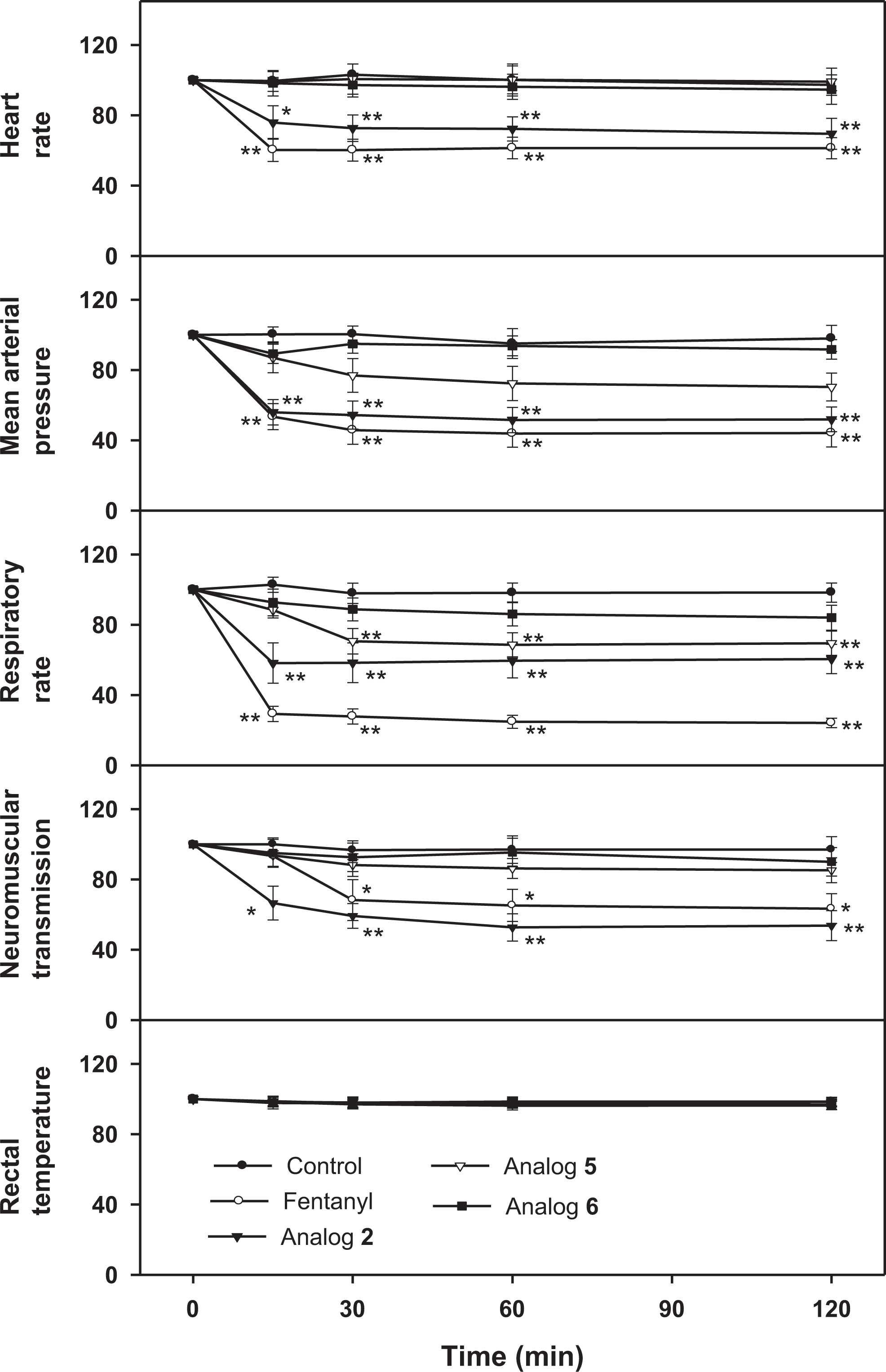
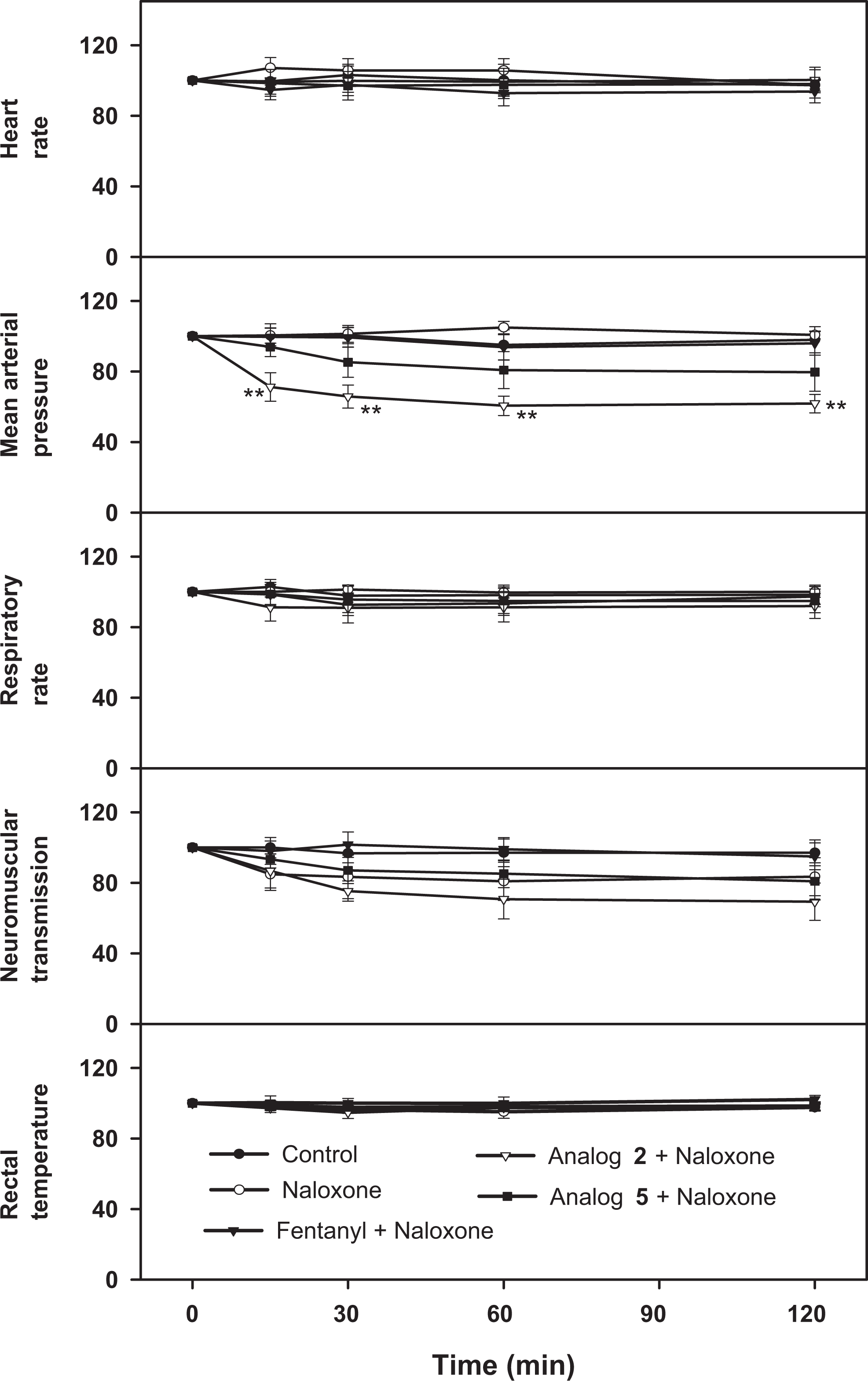
The LD50 values of fentanyl and analogs 2, 5, and 6 in rats are depicted in Table 5. Fentanyl was found to be most toxic (LD50 = 0.879 mg/kg) followed by 6 (LD50 = 55.44 mg/kg), 5 (LD50 = 69.80 mg/kg), and 2 (LD50 = 87.88 mg/kg). Fentanyl and its analogs showed significant changes in physiological variables. Typical polygraphic tracings of vehicle control (DMSO) and fentanyl-treated animal are shown in Figure 1A and B, respectively. Typical fentanyl-induced respiratory depression was observed, along with changes in HR, MAP, and NMT. Figure 2 shows the effect of DMSO, fentanyl, and its analogs on physiological variables, namely, HR, MAP, RR, NMT, and RT. Dimethyl sulfoxide did not produce any change in the physiological variables. In fentanyl-treated group, there was a significant decrease in HR, MAP, and RR between 15 minutes and 2 hours, while NMT was decreased between 30 minutes and 2 hours. In analog 2-treated group, a significant decrease in HR, MAP, RR, and NMT was observed, which persisted from 15 minutes to 2 hours. In analog 5-treated group, only RR was significantly decreased from 30 minutes to 2 hours, and the decrease in MAP and NMT was not statistically significant compared to the corresponding control. Analog 6 did not produce significant change in any physiological variables. Only a minimal decrease in RR was observed between 30 minutes and 2 hours. Fentanyl and its analogs did not produce any change in RT. All the analogs produced change in RR, which was more or less similar to fentanyl. Figure 3 shows the effect of fentanyl and its analogs on physiological variables in the presence of naloxone. Although physiological changes caused by fentanyl were found to be restored by naloxone, the same induced by analog 2 was not completely abolished. Also, a significant decrease in MAP caused by analog 2 was not restored by naloxone, while a persistent decrease in NMT was not of any statistical significance. Naloxone was also found to prevent the changes in RR produced by analog 5. At the same time, analog 6 did not produce any significant alterations in any of the physiological parameters. Therefore, its effects were not tested further in the presence of naloxone.
Median Lethal Dose of Fentanyl and Its Analogs in Rats.a,b
Compounds
LD50, mg/kg
Fentanyl
0.879 (0.649-0.118)
2
87.88 (64.95-118.91)
5
69.80 (51.59-94.45)
6
55.44 (40.98-75.02)
aTwenty-four hours median lethal dose (LD50) of fentanyl and analogs 2, 5, and 6 (intraperitoneal) was determined in male rats by Dixon’s up-and-down method using 4 to 6 animals for each value.19
bValues in parentheses are fiducial limits at 95% confidence interval.
A typical tracing on the effect of DMSO and fentanyl (0.50 LD50; intraperitoneal) on various physiological parameters in anesthetized rats. DMSO denotes dimethyl sulfoxide.
Effect of fentanyl and its analogs on various physiological parameters in anesthetized rats. Male rats were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50). Heart rate, mean arterial pressure, respiratory rate, neuromuscular transmission, and rectal temperature were measured at various time intervals using a polygraph. Values are expressed as percentage of the corresponding control and are mean ± SEM (n = 4). Statistical significance was drawn at *P < 0.05 and **P < 0.01. SEM denotes standard error of the mean.
Effect of fentanyl and its analogs on various physiological parameters in anesthetized rats. Male rats were intraperitoneally treated with fentanyl and its analogs 2, 5, and 6 (0.50 LD50) in the presence of naloxone hydrochloride (5 mg/kg, subcutaneous; -10 minutes). Heart rate, mean arterial pressure, respiratory rate, neuromuscular transmission, and rectal temperature were measured at various time intervals using a polygraph. Values are expressed as percentage of the corresponding control and are mean ± SEM (n = 4). Statistical significance was drawn at *P < 0.05 and **P < 0.01. SEM denotes standard error of the mean.
Discussion
Opioids are widely used as potent analgesic agent. They are safe and effective if taken as prescribed by the physician. However, overdosing can cause coma and life-threatening respiratory depression.22 The present study was designed to determine the acute effect of single sublethal dose of fentanyl and its 3 new analogs, namely, 2, 5 and 6, on various biochemical, oxidative, and physiological variables. The liver and kidney are responsible for drug metabolism and excretion. Therefore, in the present study, AST, ALT, LDH, and albumin were evaluated as markers for hepatic function and creatinine and urea as markers for renal function. The elevated levels of ALP (fentanyl), ALT (fentanyl and analog 2), and urea (fentanyl) are possibly due to hepatotoxic and nephrotoxic potential of these compounds, which however were transient in nature. Previous study reported the increased levels of ALT, AST, LDH, and blood urea nitrogen in rats after long-term administration (30 days) of morphine9 and tramadol.23 In opioid-naive animals, morphine, fentanyl, and methadone have been shown to be responsible for significant dose-dependent decrease in arterial pH and Pao2 and increase in Paco2.24–26 In our study, significant increase in Pco2 and decrease in Po2 were observed in fentanyl- and analog 2-treated groups, and a partial decrease in blood pH was also observed but not of statistical significance. Previous study also showed a significant decrease in arterial pH and Pao2 and an increase in Paco2 after fentanyl (80% of LD50) administration in rats.27 In the same study, it was also reported that opioid-induced alterations in respiratory patterns and blood gases were not uniform and exhibited molecule-specific patterns. In another study, intramuscular (IM) injection of fentanyl (30 μg/kg) was not found to exhibit significant influence on blood gas levels in rats 5 to 10 minutes postexposure.28 In our present study, we did not find significant changes in the hematological variables. However, in a case report of opioid overdose, decrease in RBC count, HCT, and platelet count was observed.22 In another study, fentanyl (30 μg/kg; IM) was not found to significantly affect the HCT in rats 5 to 10 minutes postexposure.28
Opioids are able to induce reactive oxygen species formation in several cells.29,30 Also, opioids are reported to impair the antioxidant defense system, including decrease in the levels of various enzymatic and nonenzymatic antioxidants,31–33 and cause lipid peroxidation.34 In the present study, a single-dose administration of fentanyl and its analogs did not produce significant change in GSH and GSSG levels in the brain, liver, and kidney 7 days postexposure. Moreover, fentanyl and its analogs 2 and 5 did not cause lipid peroxidation, as evidenced by MDA levels. However, a significant increase in MDA levels was observed in the brain, liver, and kidney in analog 6-treated group, suggesting pronounced lipid peroxidation. As such, there is no report on acute effect of fentanyl or its analogs on GSH, GSSG, and MDA levels in experimental animals. However, a transient increase in blood MDA level was reported in a patient of renal colic pain after fentanyl administration.35 A significant depletion of GSH in peripheral organs following acute systemic or central administration of opioids has been reported.36 One study also reported an increase in MDA levels in plasma after long-term administration (30 days) of morphine in rats.9 In another experiment, morphine was found to decrease GSH levels in the brain of rat11 and rabbit.13
Similar to our previous studies in mice,17,18 in the present study, also analogs 2, 5, and 6 were found to be less toxic compared to fentanyl in rats. Analogs 2, 5 and 6 were almost 100, 79, and 63 times less toxic compared to fentanyl, respectively. Further, the present study showed that acute administration of fentanyl and its analog 2 caused a significant decrease in HR, MAP, RR, and NMT, while analog 5 caused a significant decrease in RR only. Influence of opioids, including the cardiovascular effects, is dependent on the type of opioid agent and the type of receptor stimulated.37 At therapeutic doses, fentanyl has no major effects on the BP or cardiac rate and rhythm. Such doses do produce peripheral vasodilation, reduced peripheral resistance, and an inhibition of baroreceptor reflexes. Massive doses of fentanyl (5-200 times the clinically recommended dose) result in slight to moderate decreases in cardiac output, HR, and BP.38 In another experiment, bradycardia was also observed after fentanyl administration.14,39 Moreover, Gardocki and Yelnosky15 also reported a decrease in BP after fentanyl administration. The mechanism of opioid-induced bradycardia is not fully understood, but a centrally mediated increase in parasympathetic tone, direct negative chronotropic action at the sinus node, potentiation of vagally released acetylcholine at the sinus node, and reduction in sympathetic activity have all been implicated.40–44 Fentanyl produces a dose-dependent respiratory depression, which is similar to that observed with other μ-opioids, but here the onset is more rapid.27 In our present study, fentanyl and its analog 2 caused significant decrease in RR between 15 and 120 minutes, while analog 5 caused a significant decrease in RR between 30 and 120 minutes. Analog 6 also decreased RR, but it was nonsignificant compared to control or other analogs. Our results are in agreement with several previous reports where a decrease in RR was observed after fentanyl treatment.14,45 In one of our recent studies, fentanyl and its analogs 2, 5, and 6 were also found to decrease respiratory frequency and cause respiratory depression following inhalation of smoke of these compounds in a static exposure assembly.46 All μ-opioid receptor agonists, including fentanyl, produce dose-dependent respiratory depression. Respiratory depression is the main hazard of opioid use because of the obvious risk of fatal outcome.16,27 The degree of respiratory depression varies between different opioids, and there are currently no opioids available that are devoid of respiration-related side effects.16 In the present study, all the analogs caused respiratory depression, which was of lesser magnitude compared to fentanyl. Therefore, this observation seems important as most unwanted effect of the opioids is respiratory depression. As with analgesia, respiratory depression induced by fentanyl after small doses is of shorter duration compared to morphine but is of similar duration after large doses. Morphine-like opioids cause respiratory depression by a direct effect on the brain stem respiratory center and it is noticeable even with doses too small to disturb consciousness and increases gradually as the dose is increased. In human beings, death from opioid poisoning is nearly always due to respiratory arrest.47 In our study, fentanyl and its analog 2 caused a significant decrease in NMT; analog 5 also decreased NMT but not of statistical significance. Previous study also showed a decrease in NMT after fentanyl administration.15 Furthermore, a dose-dependent depression in diaphragmatic twitch tension was observed at a concentration >150 ng/mL of fentanyl in response to phrenic nerve stimulation.48 Opioids have been found to act on neuromuscular junction to inhibit acetylcholine release. The effect was suggested to be both opioid receptor-mediated and nonspecific actions.49 Opioids have a direct and dual effect on the skeletal muscle.50 The stereospecific opioid receptor has been shown to be present on the skeletal muscle membrane51 and is suggested to be located on the inner opening of the sodium gate. When opioids bind to the receptor, the sodium conductance is inhibited. Large doses of opioids possess a local anesthetic effect on the skeletal muscle membrane and thus inhibit the sodium conductance.50 The receptor-mediated and local anesthetic-like effects induce the depression of action potential, which consecutively reduce the amount of calcium release from intracellular sarcoplasmic reticulum. Therefore, the force of muscle contraction is depressed.48 In the present study, fentanyl and its analogs did not produce significant change in the RT. However, previous study reported hyperthermia at low doses and hypothermia at higher doses after fentanyl administration in rats.52 The effects of opioids on the body temperature have been shown to be complex and dependent on numerous factors such as species, strain, dose, route of administration, receptor specificity, age, degree of restraint, handling, and environmental temperature.53,54 The present study also confirmed that the physiological changes, particularly the respiratory depression, caused by fentanyl and its analogs were found to be reversed by naloxone hydrochloride (a μ-opioid receptor antagonist), indicating μ-receptor-mediated effects of the compounds.
The present study shows that (1) fentanyl and analog 2 produced minor biochemical changes indicative of hepatic and renal dysfunction, but the changes were very transient, (2) analog 6 caused significant lipid peroxidation in 3 vital organs, (3) and fentanyl and analogs 2 and 5 caused severe respiratory depression, which favorably responded to pretreatment of naloxone. In conclusion, all the fentanyl analogs were found to be less toxic compared to fentanyl, suggesting their possible role in pain management.
Footnotes
Acknowledgments
The authors thank Dr D. K. Dubey, Director, DRDE, Gwalior, for providing necessary facilities.
Author Contributions
Shiv Kumar Yadav contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, and critically revised the manuscript. Deo Kumar contributed to conception and design and contributed to acquisition, analysis, and interpretation of data. Pravin Kumar contributed to conception and design and contributed to acquisition, analysis, and interpretation of data. Pradeep Kumar Gupta contributed to conception and design, contributed to acquisition, analysis, interpretation of data, and synthesized the fentanyl and its analogs. Rahul Bhattacharya contributed to conception and design, contributed to acquisition, analysis, and interpretation of data, contributed to manuscript writing, and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
1.
DavisMP. Fentanyl for breakthrough pain: a systematic review. Expert Rev Neurother. 2011;11(8):1197–1216.
2.
PengPWSandlerAN. A review of the use of fentanyl analgesia in the management of acute pain in adults. Anesthesiology. 1999;90(2):576–599.
3.
StanleyTH. The history and development of the fentanyl series. J Pain Symptom Manage. 1992;7(suppl 3):S3–S7.
4.
SearJW. Recent advances and developments in the clinical use of iv opioids during the peroperative period. Br J Anaesth. 1998;81(1):38–50.
5.
BaseltRC. Disposition of Toxic Drugs and Chemicals in Man. 6th ed. Foster City, CA: Biomedical Publications; 2002:430–433.
6.
RadovanovićDPjevićMMalbašaZStošićA. The use of transdermal fentanyl in the treatment of cancer pain. Arch Oncol. 2002;10(4):263–266.
7.
DrewesAMJensenRDNielsenLM. Differences between opioids: pharmacological, experimental, clinical and economical perspectives. Br J Clin Pharmacol. 2013;75(1):60–78.
AticiSCinelICinelLDorukNEskandariGOralU. Liver and kidney toxicity in chronic use of opioids: an experimental long term treatment model. J Biosci. 2005;30(2):245–252.
10.
QiushengZYuntaoZRongliangZDeanGChanglingL. Effects of verbascoside and luteolin on oxidative damage in brain of heroin treated mice. Pharmazie. 2005;60(7):539–543.
11.
GuzmánDCVázquezIEBrizuelaNO. Assessment of oxidative damage induced by acute doses of morphine sulfate in postnatal and adult rat brain. Neurochem Res. 2006;31(4):549–554.
12.
XuBWangZLiG. Heroin administered mice involved in oxidative stress and exogenous antioxidant-alleviated withdrawal syndrome. Basic Clin Pharmacol Toxicol. 2006;99(2):153–161.
13.
OzmenINazirogluMAliciHASahinFCengizMErenI. Spinal morphine administration reduces the fatty acid contents in spinal cord and brain by increasing oxidative stress. Neurochem Res. 2007;32(1):19–25.
14.
TsujikawaHShodaTMirotaTFukudaK. Morphine induces DNA damage and p53 activation in CD3+ T cells. Biochim Biophys Acta. 2009;1790(8):793–799.
15.
GardockiJFYelnoskyJ. A study of some of the pharmacological actions of fentanyl citrate. Toxicol Appl Pharmacol. 1964;6(1):48–62.
16.
PattinsonKT. Opioids and the control of respiration. Br J Anaesth. 2008;100(6):747–758.
17.
GuptaPKYadavSKBhutiaYD. Synthesis and comparative bioefficacy of N-(1-phenethyl-4-piperidinyl)propionanilide (fentanyl) and its 1-substituted analogs in Swiss albino mice. Med Chem Res. 2013;22(8):3888–3896.
18.
YadavSKMauryaCKGuptaPKJainAKGanesanKBhattacharyaR. Synthesis and biological evaluation of some novel 1-substituted fentanyl analogs in Swiss albino mice. Interdiscip Toxicol. 2014;7(2):93–102.
19.
DixonWJ. The up-and-down method for small samples. J Am Stat Assoc. 1965;60(312):967–978.
20.
HissinPJHilfR. A fluorimetric method for determination of oxidised and reduced glutathione in tissue. Anal Biochem. 1976;74(1):214–226.
21.
OkhawaHOhishiWYogiK. Assay formulation lipid peroxidase in animal tissue by thiobarbituric acid reaction. Anal Biochem. 1979;95(2):351–358.
22.
WilliamsRHEricksonT. Emergency diagnosis of opioid intoxication. Lab Medicine. 2000;31(6):334–342.
23.
EI-GaafarawiII. Biochemical toxicity induced by tramadol administration in male rats. Egypt J Hosp Med. 2006;23:353–362.
24.
CowanADoxeyJHarryE. The animal pharmacology of buprenorphine, an oripavine analgesic agent. Br J Pharmacol. 1977;60(4):547–554.
25.
McCormickGYWhiteWJZagonISLangCM. Effects of diazepam on arterial blood gas concentrations and pH of adult rats acutely and chronically exposed to methadone. J Pharmacol Exp Ther. 1984;230(2):353–359.
26.
DahanAYassenABijlH. Comparison of the respiratory effects of intravenous buprenorphine and fentanyl in humans and rats. Br J Anaesth. 2005;94(6):825–834.
27.
ChevillardLMégarbaneBRisédePBaudFJ. Characteristics and comparative severity of respiratory response to toxic doses of fentanyl, methadone, morphine, and buprenorphine in rats. Toxicol Lett. 2009;191(2-3):327–340.
28.
PengYZLiXXWangYW. Effects of parecoxib and fentanyl on nociception-induced cortical activity. Mol Pain. 2010;6(1):3.
29.
SharpBMKeaneWFSuhHJGekkerGTsukayamaDPetersonPK. Opioid peptides rapidly stimulate superoxide production by human polymorphonuclear leukocytes and macrophages. Endocrinology. 1985;117(2):793–795.
30.
OliveiraMTRegoACMorgadinhoMTMacedoTRAOliveiraCR. Toxic effects of opioid and stimulant drugs on undifferentiated PC12 cells. Ann N Y Acad Sci. 2002;965(1):487–496.
31.
DaviesKJ. A secondary antioxidant defense role for proteolytic systems. Basic Life Sci. 1988;49:575–585.
GoudasLCLangladeASerrieA. Acute decreases in cerebrospinal fluid glutathione levels after intracerebroventricular morphine for cancer pain. Anesth Analg. 1999;89(5):1209–1215.
34.
ZhouJFYanXFRuanZR. Heroin abuse and nitric oxide, oxidation, peroxidation, lipoperoxidation. Biomed Environ Sci. 2000;13(2):131–139.
35.
TurtayMGOguzturkHColakCPolatATasdemirC. Effect of renal colic analgesia on oxidative stress parameters. Sci Res Essays. 2010;5(20):3160–3163.
36.
GoudasLCCarrDBMaszczynskaI. Differential effect of central versus parenteral administration of morphine sulfate on regional concentrations of reduced glutathione in rat brain. Pharmacology. 1997;54(2):92–97.
37.
ShanazariAAAslaniZRamshiniEAlaeiH. Acute and chronic effects of morphine on cardiovascular system and the baroreflexes sensitivity during severe increase in blood pressure in rats. ARYA Atheroscler. 2011;7(3):111–117.
38.
KukanichBClarkTP. The history and pharmacology of fentanyl: relevance to a novel, long-acting transdermal fentanyl solution newly approved for use in dogs. J Vet Pharmacol Ther. 2012;35(suppl 2):3–19.
39.
GürkanABirgülYZiyaK. Direct cardiac effects in isolated perfused rat hearts of fentanyl and remifentanil. Ann Card Anaesth. 2005;8(2):140–144.
40.
ReitanJAStengertKBWymoreMLMartucciRW. Central vagal control of fentanyl-induced bradycardia during halothane anesthesia. Anesth Analg. 1978;57(1):31–36.
41.
BlairJRPruettJKIntronaRPAdamsRJBalserJS. Cardiac electrophysiologic effects of fentanyl and sufentanil in canine cardiac Purkinje fibers. Anesthesiology. 1989;71(4):565–570.
42.
RomeroMLaordenMLHernandezJSerranoJS. Effects of morphine on isolated right atria of the rat. Gen Pharmacol. 1992;23(6):1135–1138.
43.
WeberGStarkGStarkU. Direct cardiac electrophysiologic effects of sufentanil and vecuronium in isolated guinea-pig hearts. Acta Anaesthesiol Scand. 1995;39(8):1071–1074.
FoneKCWilsonH. The effects of alfentanil and selected narcotic analgesics on the rate of action potential discharge of medullary respiratory neurones in anaesthetized rats. Br J Pharmacol. 1986;89(1):67–76.
46.
YadavSKSwamiDKumarP. Acute inhalation toxicity of smoke of fentanyl and its 1-substituted analogs in Swiss albino mice. Cell Mol Biol (Noisy-le-Grand). 2014;60(3):1–9.
47.
GutsteinHBAkilH.Opioid analgesics. In: HardmanJGLibirdLE, ed. Goodman and Gilman’s the Pharmacological Basis of Therapeutics. 10th ed. New York, NY: McGraw Hill. 2001:569–619.
48.
YehFCShiehJPYenMH. Neuromuscular effects of fentanyl in the rat phrenic nerve-diaphragm preparation. J Med Sci. 1989;10(2):67–72.
49.
SoteropoulosGCStandaertFG. Neuromuscular effects of morphine and naloxone. J Pharmacol Exp Ther. 1973;184(1):136–142.
50.
FrankGB. Two mechanisms for the meperidine block of action potential production in frog’s skeletal muscle; non-specific and opiate drug receptor mediated blockade. J Physiol. 1975;252(3):585–601.
51.
FrankGB. Stereospecific opioid drug receptor on excitable cell membrane. Can J Physiol Pharmacol. 1985;63(9):1023–1032.
52.
VučkovićSIvanovićMProstranM. Higher environmental temperature potentiates cataleptic effect of fentanyl in rats. Jpn J Pharmacol. 2001;78(4):523–527.
53.
AdlerMWGellerEB. Thermoregulation and the opioid system. NIDA Res Monogr. 1989;95:180–185.
54.
GellerEBAdlerMW. Drug of abuse and body temperature. In: Modern Methods in Pharmacology, Vol 6, Testing and Evaluation of Drugs of Abuse. New York: Wiley-Liss, Inc; 1990:101–119.