
Abstract
Keywords
Key points
Hungarian female dancers perceive a high level of stress in their everyday lives.
Hungarian female dancers suffer from acute musculoskeletal complaints.
There is a positive relationship between the stress level and pain experience.
Introduction
Most research on the etiology of musculoskeletal injury among dancers has been focused on the biomechanical properties.1 -4 Classical ballet involves repetitive movements in non-physiologic positions that require significant neuromuscular control and balance, which places heavy loads on the joints and their supporting structures.1 -3 Overuse injuries reportedly account for approximately 75% of injuries in amateur ballet dancers,2,3 higher than in the case of adult professional ballet dancers (66%). 4
Extrinsic risk factors—hypothesized as contributors to dance injury—extend from poor technique, improper training, inappropriate scheduling to prevent fatigue, a lack of strengthening to prevent muscular imbalances, suboptimal equipment, including footwear and floor type, 5 to social support, financial and medical availability, as well as the cultural climate of the team or company. 6 While these factors are already creating a multifactorial etiologic background of physical injuries, other factors may also contribute to injuries, such as environmental temperature and humidity, nutrition, and sleep behaviors. 7
Although many studies examine the extrinsic risk factors, no report makes definitive conclusions about the exact intrinsic risk factors for musculoskeletal injury in dancers. 8 Endogenous (intrinsic) factors (genetics, training to manage biomechanical forces, gender) also influence injury risk, for example, individual appraisal of genetic risk, trait anxiety, and attentional processes.6,7
Despite the limited availability of scientific evidence in this field, previous injuries, perfectionism, and insufficient psychological coping skills with stress appear to be associated with an increased risk of injury in pre-professional young dancers. 9 According to our current knowledge, no research publications investigate the injury etiology or possible connection between stress factors in Hungarian professional dancers. However, a stress-injury model for athletes was created more than 30 years ago. 10 This model identifies stress as a significant risk factor for injury. 6 Despite its age, it remains the predominant model explaining the connection between psychological factors and injury risk, prevention, and incidence. Accordingly, athletes under psychological stress were significantly more likely to sustain acute injuries during performance, 11 while the influence of psychological variables on injury incidence derives primarily from stress (ie, distress). 10 Since these studies confirmed the connection between injury and stress among athletes, we were interested in whether we could also prove this phenomenon in professional dance. This cross-sectional study aimed to identify and assess the relationship between stress and musculoskeletal complaints among Hungarian professional dancers. At the same time, we were also motivated to evaluate the level of perceived stress among this population, including classical ballet, modern, and theatrical dancers.
Material and Methods
Power Calculation
The estimated sample size, determined by using the sample size calculator, 12 is 162, with the population number being 280; when α = .05 for a 2-sided test, β (power) equals .8. According to the power calculation the recruitment was possible from this population.
Study Population
For this study, we recruited 191 Hungarian professional dancers from Hungarian dance companies and online closed dance profile social media groups to fill out the questionnaire. After the first data review, we excluded those who did not fill the questionnaire by at least 50%, as well as 16 answers made by male dancers since the male gender representation amounted to only 9%. In total, we worked out of 168 answers (N = 168). The mean age of the sample was 32 (µ = 32.43, SD = 10.89); 25% were classical ballet, 51.2% modern, and 23.8% theatrical dancers. The participants had more than 15 years of professional experience in the dance industry (µ = 15.52 years, SD = 10.9). 91.7% of respondents received professional training in the same educational institution in Hungary, 74.4% had university or college degrees in professional dance, and 16.6% owned dance-specific high school diplomas.
Procedure
We primarily recruited via an online platform using thematic, closed social media groups and by advertising the research to Hungarian professional dance companies and educational institutions. Our target audience comprised classical ballet, contemporary, modern, and theatrical dancers. We have entirely applied the Helsinki Declaration to our study. All participants signed a written consent via the online questionnaire platform.
Questionnaires
According to the study aims, we collected 3 validated psychometric questionnaires, translated to and validated in Hungarian. We uploaded the questionnaires to the online survey platform Qualtrics, where participants could answer the questions. In the description of the questionnaires, we suggested to participants to give their answers in a calm, private space, excluding any disturbing stimuli or another person.
The Recovery-Stress Questionnaire for Athletes (RESTQ-Sport) 13 is a questionnaire reported to identify the extent to which athletes are physically or mentally stressed, as well as their current capabilities toward recovery.13,14 RESTQ-Sport consists of 12 General Stress and Recovery scales and 7 Sport-specific Stress and Recovery scales. 13 The General Stress component includes 3 scales that measure general, emotional, and social stress and their consequences. Cronbach-α values for each of the 19 separate subscales comprised hypothesized items, ranging from .72 to .93. 13 The test-retest reliability of the individual Subscales achieved correlational values above 0.79.13,14 The Hungarian translation and validation were done by Tóth and Szabó. 15
The basic concept of the Mental Health Test 16 is to obtain a comprehensive picture of the subject’s mental health concerning the 5 pillars—Well-being, Savoring, Creative-executive efficiency, Self-regulation, and Resilience—by using a short questionnaire of no more than 20 items.16,17 It has 2 subscales we analyzed, the results of which—well-being score and resilience score—are included in our study. This questionnaire was created and validated in Hungarian. 16
Self-Estimated Functional Inability because of Pain Questionnaire (SEFIP) 18 The basic structure of the SEFIP consists of 14 items representing body parts: neck, shoulders, elbows, wrists/hands, upper back, lower back, hips, thighs (front), thighs (back), knees, legs (front), calves, ankles, and feet. Points on the SEFIP scale are calculated as follows: “I am entirely free of pain.” =0 points; “I have slight pain, but it is no problem.” =1 point; “I have quite a bit of pain, but I can dance if I am careful.” =2 points; “I have a lot of pain and have to avoid certain movements.” =3 points; “I have great difficulty and cannot take part in the production.” =4 points. Values of reliability (κ ≥ .40, intraclass correlation coefficient = .91), internal consistency (Cronbach’s α ≥ .81), and correlations (rs ≥ −.376) of the total SEFIP-sport score with the numerical rating scale. 19
In addition to the validated questionnaires, we used demographic questions featuring certain highly reported injury types. We defined injuries as acute musculoskeletal conditions, which affect the movement of the dancers, their performance, and general well-being. Injury is often associated with a painful, decreased range of movement conditions including examples of ligament rupture and bone fracture. The questions, Hungarian adaptations, were uploaded to an online questionnaire platform (Qualtrics), from where we collected the data anonymously. The questionnaires were self-reported. The participants did not receive any compensation for completing the questionnaire. The IRB at Eötvös Loránd University, along with the Research Ethics Review Board, approved and supervised the study (Approval number: 2021/419).
Statistical Analysis
For the statistical analysis, we used SPSS 28.0.0. We tested the distribution with either the Kolmogorov-Smirnov Test or graphical methods. For the relationship analysis, depending on the distribution of the variables, we used various regression methods, the curve estimation, the linear, as well as Pearson and Spearmen’s correlation. We applied the Kaplan-Meier Survival analysis Hazard Curves to assess the time-to-event variables. Statistical significance was set to alpha < .05.
Results
Among the distribution of the dance fields (classical ballet 25%; modern dance 51.2%; theatrical dance 23.8%), we did not find a statistically significant difference (P = .143) in injury prevalence. In the acute pathological conditions, we found that ligament rupture (39.3%) had the most frequent occurrence, bone fracture (17.9%) was also prevalent, while stress fractures (5%) were the least reported among professional dancers in this study.
Analyzing the perceived stress scale, it appeared that dancers were experiencing a high level of stress (µ = 12.58 points, SD = 3.78, range = 20 points), with 92.4% of the study population scoring above 10 points.
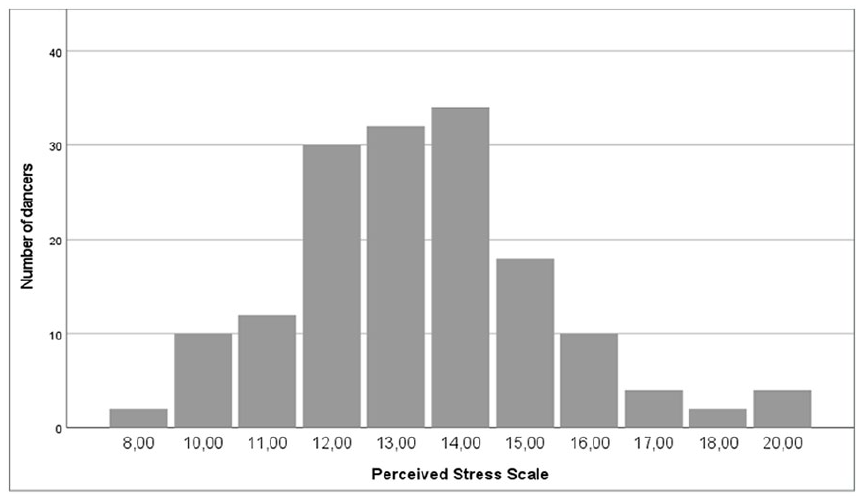
Histogram of Perceived Stress Scale distribution among respondents (N = 168).
Based on the Mental Health Test, we found that 17.9% of the study population belonged to the very high well-being level (5.9-6 points); 26.2% had a high degree of well-being (5.3-5.8 points); 34% scored to the average well-being group (3.6-5.2 points), while the rest of the study population (21.9%) scored in the low and very low well-being state (µ = 4.83 SD = 1.157 range = 4.67). We used the same questionnaire to evaluate the level of resilience, with our findings of 12.2% reaching the highest score and almost half of the population (48.9%) being resilient individuals (µ = 8.9 SD = 2.9 range = 10.67).
The Self Estimated Functional Inability because of Pain questionnaire showed that, at the time, less than 5% (µ = 4.57%) perceived functional limiting pain (“Cannot work in the production because of pain.”) in different parts of their body, almost 10% (µ = 9.58) reported experiencing severe pain, still enabling the dancer to perform (“Much pain, must avoid some movements.”), and 21.4% scored experiencing some level of pain in certain areas of their body, not limiting their functionality (“Pretty much pain, but I can handle it.”). 63.6% of the dancers reported no current pain anywhere. The top areas of pain reported were the lower back (26.1%), the neck (23.7%), the shoulder (19%), the knee (15.5%), and the ankle (10.7%).
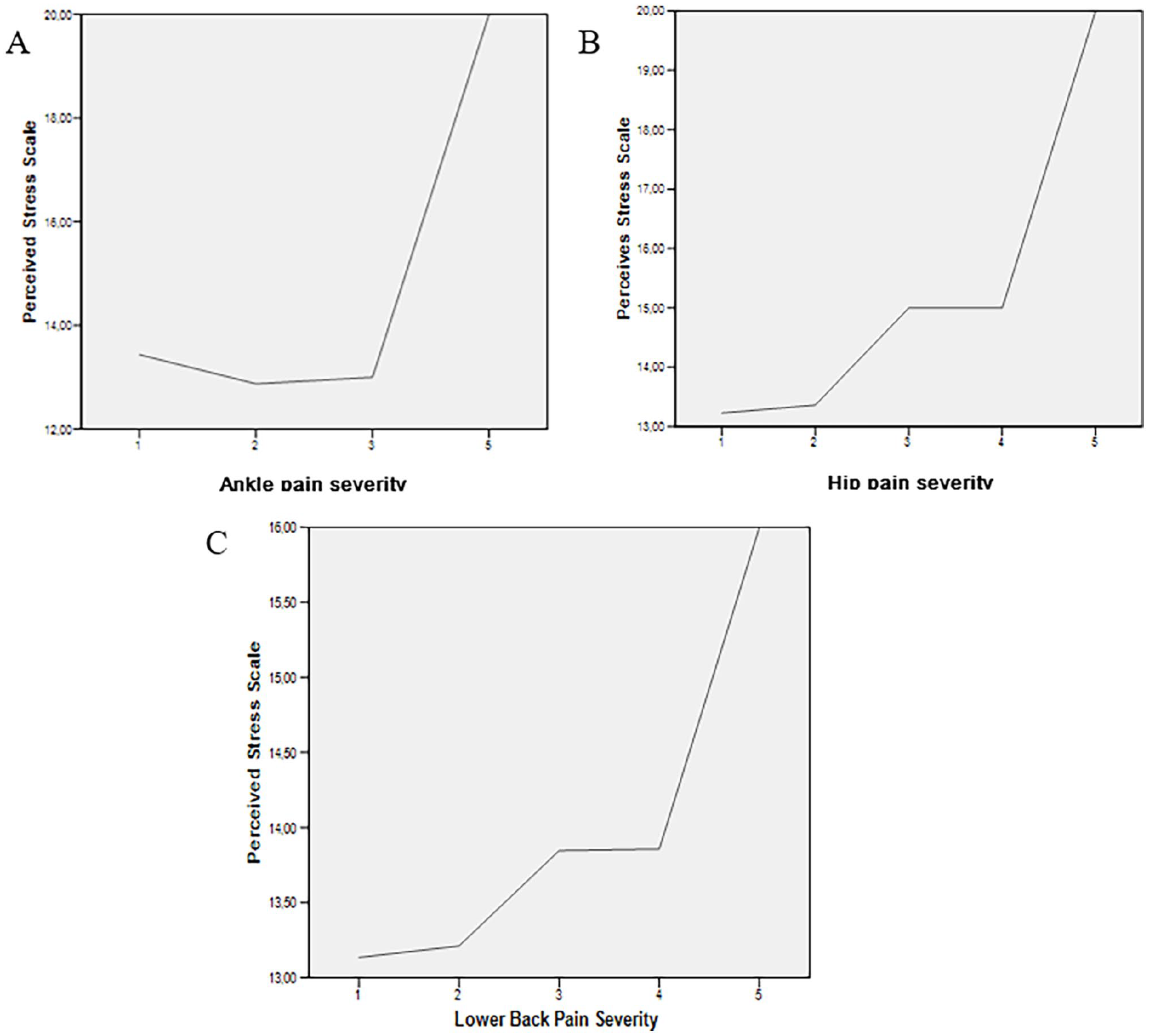
Perceived Stress Scale and Pain Severity graphs: (A) represents the PSS score and the Ankle Pain Severity (P = .045); (B) the PSS score and the Hip Pain severity (P = .042); (C) the PSS score and the Lower Back pain severity (P = .012).
Relationship Analysis
Well-being and resilience are positively correlated (P < .001 r = .501). Correlation also showed a statistically significant relationship between certain body part complaints and perceived stress. Table 1 summarizes the results based on their correlation and significance.
Correlation of Perceived Stress (PSS) with Body Part Complaints.
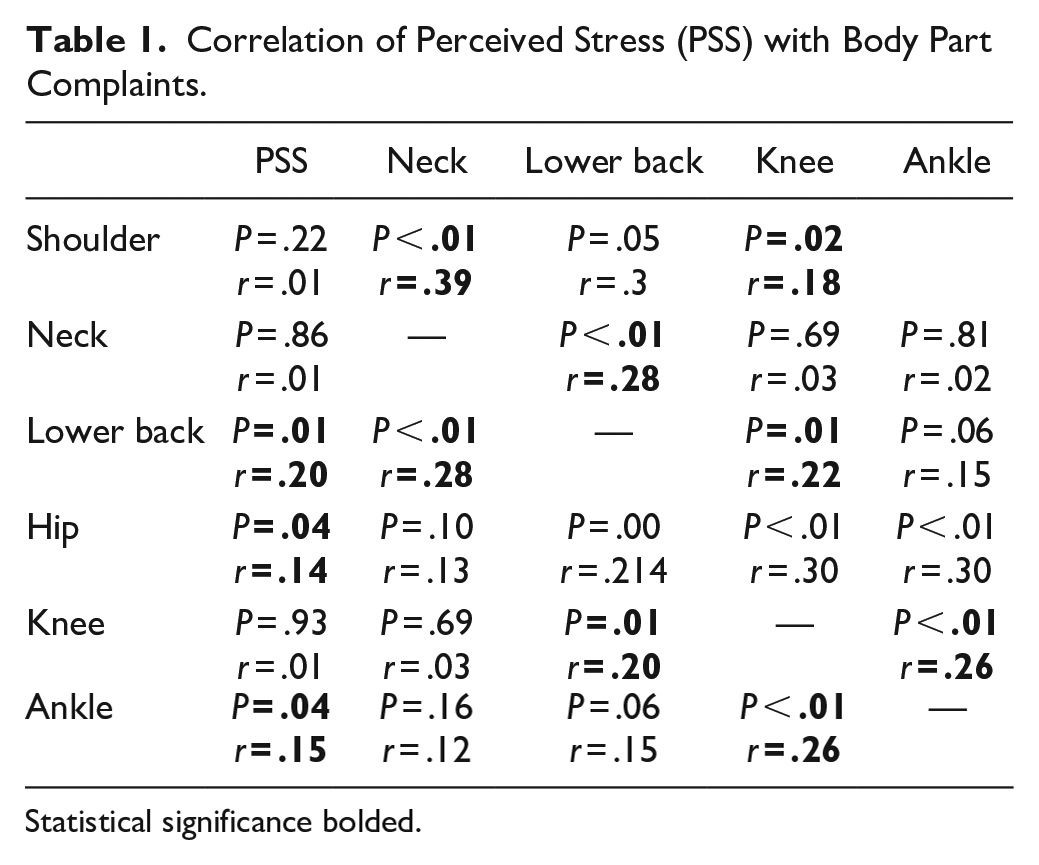
Statistical significance bolded.
After the correlation coefficient, we plotted the data onto curves to estimate the perceived stress and the severity of the complaints in those body parts where we found a significant relationship.
The Kaplan-Meier Hazard curves showed the years spent in professional dance and the reported occurrence of certain acute musculoskeletal injuries. The relationship between the years and bone fractures showed a significance of r = .519, P = .004, and the ligament rupture, which was significant r = .429, P = .003. There is no significant relationship neither between the years spent with dance and the perceived stress results (r = .143, P = .104) nor between the age of the dancer and the perceived stress (r = .291, P = .720).
Discussion
In this study we found that the Hungarian professional female dancers perceive high stress level comparing to the general population, and suffer from musculoskeletal complaints, where the relationship between the 2 entity is positive. Within the acute musculoskeletal conditions, we found that ligament rupture was the most frequent injury type within the study population which finding is similar to the results in the literature.3,8 Other reported injuries were also consistent with the ones found in the literature, where the general injury rate is between 45% and 79% in dancers’ careers.2,3
The Perceived Stress Scale showed a very high general stress level in the population, placing our study population in the high-stress level, 20 which was further supported by the RESTQ test data, where general stress and sport-specific stress level showed elevated results, that could be associated with depression, anxiety, fatigue, and reduced life satisfaction. 21
Although the Hungarian female dancers scored within the high level of perceived stress, almost half of the dancers scored in a high state of well-being. The well-being scale reliably measures the mental (subjective) well-being of the examined person, which itself has several components (biological, psychological, social, and spiritual).16,17
The very high perceived stress and the good functioning general well-being level could reveal resilience. Resilience can be considered very high (above 5.6 points) within the study group since the score for the general population is 3.76. The Resilience scale measures the level of mental resilience and mental reserves, which are most needed when a person faces unexpected difficulties. A person with a higher level of resilience can recover faster from a mental pit or a sudden, unexpected, and stressful situation.16,17 We suppose that the high level of resilience is the reason behind the functioning life maintenance in the high-stress field reported.
In our data, some body parts correlated with others significantly, which we interpret with the complex biomechanical mechanisms. Interestingly, the correlations were mainly found according to the axis of weight-bearing joints and the alignment axes (lower back: knee and neck; knee: ankle).22,23 We posit that these correlations provide additional support for the validity of our datasets, as they underscore the notion that the reported pain levels are not solely attributable to stress levels. Rather, it is likely that stress exacerbates an underlying musculoskeletal condition.
The reported pain sensation in certain body parts showed a positive correlation with perceived stress. Stress can be either an accelerating factor of an already existing physical pain24 -27 or it can create pain sensation by activating certain brain areas, such as the anterior cingulum, resulting in a cognitive conflict. 28 Such results were previously published in connection with lower back pain, associated with the existence of a neural mechanism, where the specific modulation of brain activity enabled manipulation of affective and sensory dimensions of the pain experience.29,30 Prior investigations by other researchers31,32 have identified a correlation between lower back pain and stress levels in the general population. Similarly, athletes have also yielded analogous findings, demonstrating a significant association between lower back pain and perceived stress. 33 In this study, we see that stress, indeed, is a contributing factor in the case of acute musculoskeletal complaints, where the higher the stress level, the more severe the pain sensation can be.
Calculations confirmed that the dancers’ age or the years spent in a professional dancing environment are not resulting in a higher perceived stress level, although the Kaplan-Meier curve showed dancers to have a higher chance of suffering from an injury if they kept dancing for a longer period. Figure 3 demonstrates an estimation calculation on professional dancers injury probability with 2 acute conditions (bone fracture and ligament rupture) regarding the years spent as a professional dancer. This data provided a commonly cited outcome according to which dancers will have at least 1 injury during their careers.1 -4 The results of our study suggest that it was not directly affected by the perceived stress level. It indicates that the presence of stress does not necessarily result in the occurrence of an acute injury, whereas the perception of musculoskeletal pain will more likely be more intense.
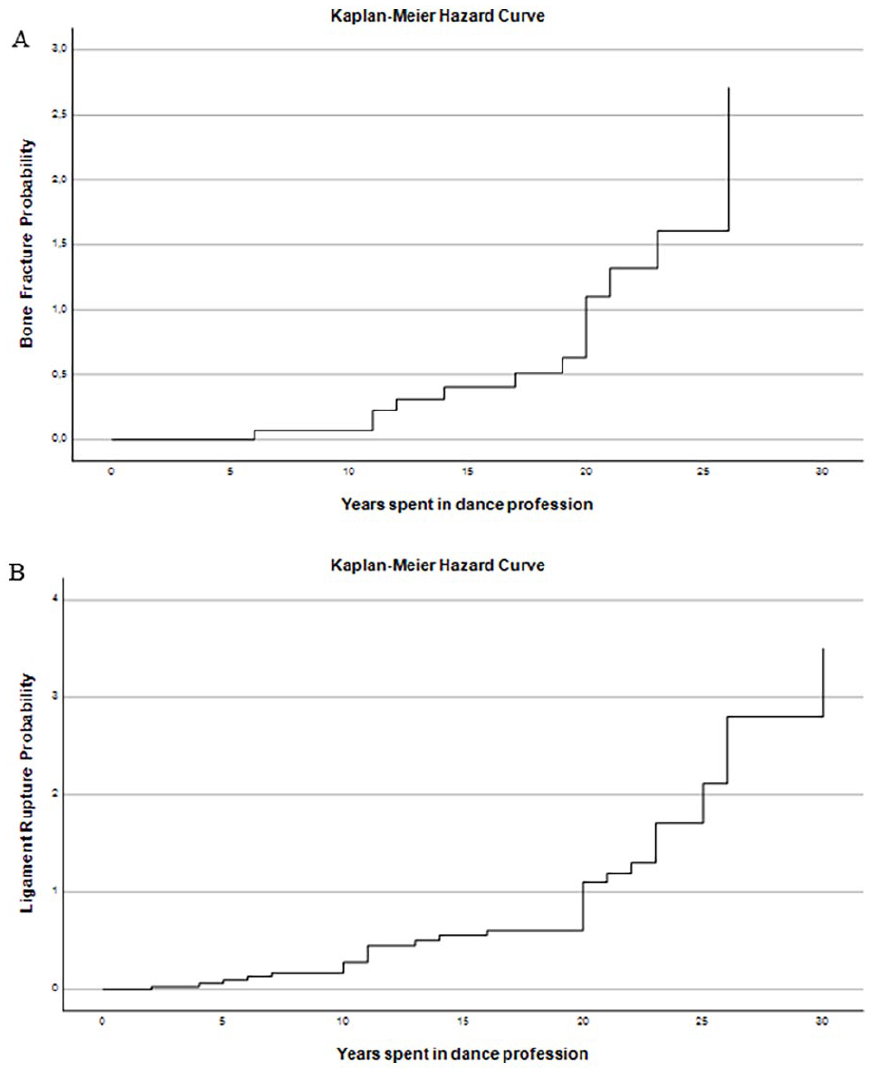
Kaplan-Meier Hazard Curve (A) Years spent in the dance profession as a working dancer, plotted with Bone Fracture Probability; (B) Years spent in the dance profession, plotted on a hazard curve with Ligament Rupture Probability.
Future perspectives entail an in-depth examination of stress factors that may trigger musculoskeletal conditions, thereby facilitating a comprehensive understanding of the precise mechanisms behind this phenomenon. Building upon our present findings, we aim to inspire professionals in the field to prioritize stress-relieving interventions for professional dancers and to incorporate stress as a contributing element in injury management and rehabilitation protocols.
Limitation
This study is limited by the lack of male dancers represented in the study population. Therefore, the results cannot be extended to the general population of professional dancers in Hungary. The authors consider the number of participants a limitation, although the power calculation showed appropriate sampling and the self-reported questionnaires as well as self-recall bias.
Conclusion
In this study, we were interested in the Hungarian professional dancers’ perceived stress, the factors of their general mental health status, and their acute musculoskeletal complaints. We found that the female professional dancers in Hungary have a very high level of perceived stress but also scored high on general well-being and resilience scales, which would suggest a successful coping mechanism. However, when dancers suffer from musculoskeletal conditions, the higher perceived stress results in more intense pain experience which correlates with those results found in the literature. With our study, we would like to highlight and raise attention to stress as an important contributing factor to musculoskeletal complaints, while we wish to encourage company leaders to decrease the sources of stress in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.