
Abstract
Key Points
Prevention of bone stress injury should have a ‘bottom up’ and a ‘top down’ approach, spanning from recreational through to professional populations.
Bone stress injury prevention for professional dancers may be facilitated by improving access to onsite multidisciplinary health services, annual health evaluations, refining safeguarding policies, and investigating wearable technology.
Bone stress injury prevention for dancers in the community may be facilitated by ballet companies role modelling and providing education and workshops for dancers, parents, and teachers.
Introduction
Bone stress injuries, including stress fractures and stress reactions occur in active populations as a result of repetitive mechanical loading, causing pain and reduced function. 1 These injuries present a high injury burden for pre-professional and professional classical ballet dancers. 2 They require lengthy periods of training modification or complete rest to heal, with reported median recovery times of 135 days for classical dancers and are often recurrent.3,4 Many factors contribute to BSI risk in physically active populations, including cumulative or fluctuating training load exposure,5,6 low energy availability and eating disorders,7,8 low bone mineral density, and periods of growth in adolescence. 9 For classical dancers, repetitive jumping, and specialised activities such as dancing en pointe may also contribute to BSI risk.10,11 Injury and physical pain is normalised in dance culture and is at times, glorified, 12 which may present as a barrier to dancers seeking early care. Thus, there is a strong case for investigating prevention of BSI in classical dancers.
Preventing BSI in dance is possible yet complex, and implementation of prevention strategies must be context-specific. 13 Prevention of injury resulting from dance activity can be conceptualised in three tiers, as either pathology-based or risk-factor based (Figures 1 and 2). 14 In a pathology-based model, primary prevention involves implementing prevention strategies for all dancers without a clinical diagnosis, regardless of an individual’s injury risk, for example, pre-participation screening and group education. Secondary and tertiary tiers focus on clinical constructs, with early diagnosis and early intervention forming the key basis for secondary prevention, and treatment of a presenting condition the basis of tertiary prevention. Rehabilitation and mitigation of risk of future health problems is the focus of tertiary prevention (Figure 1). In a risk-factor based model prevention strategies target established injury risk factors. Universal prevention involves intervention to reduce dance participation injury risk or policy change, whereas selective and indicated prevention focus on risk reduction strategies for those who may carry risk factors for injury at either a sub-group or individual level (Figure 2).
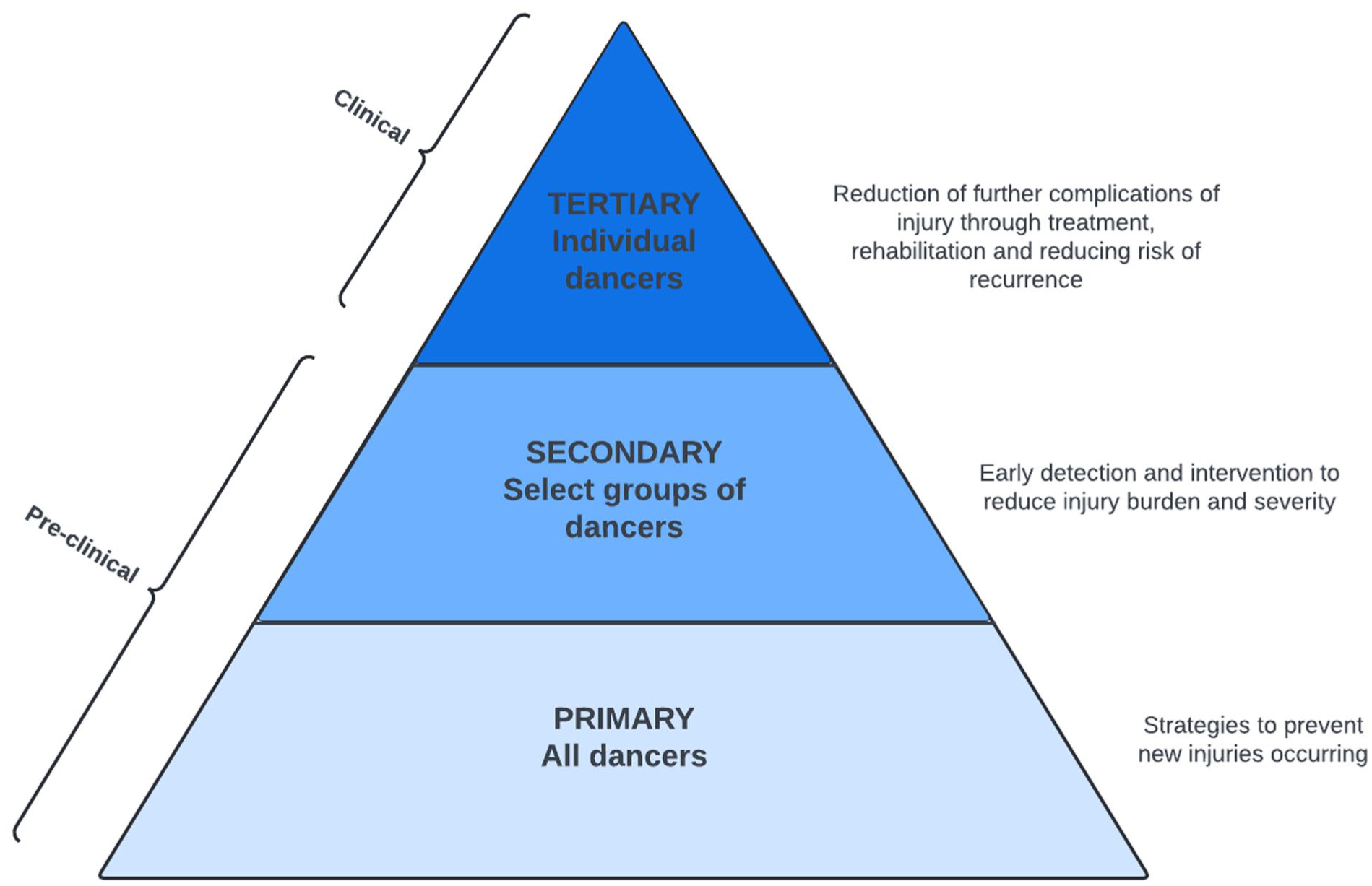
Pathology-based prevention.
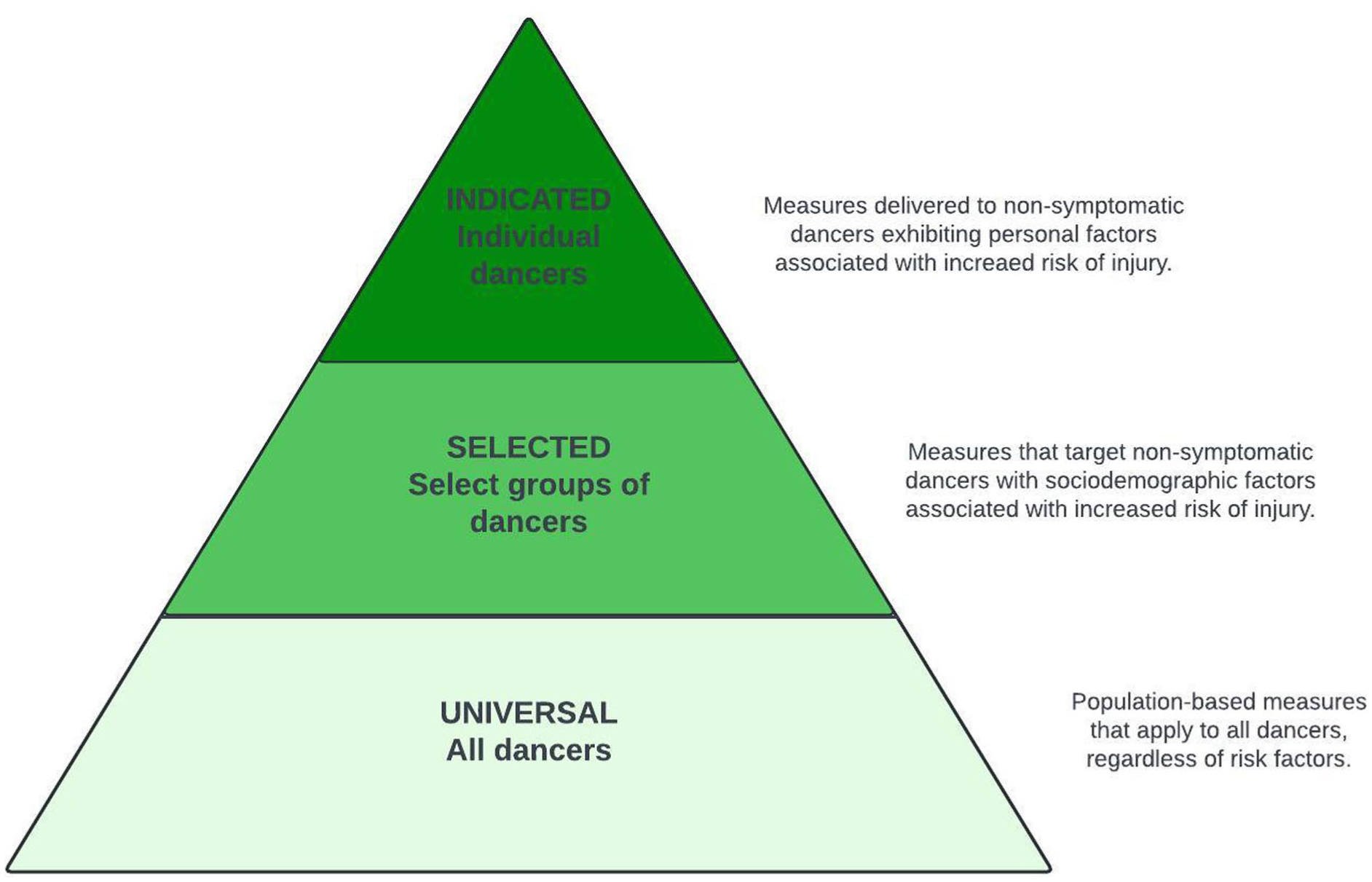
Risk factor-based prevention.
The Translating Research into Injury Prevention Practice (TRIPP) framework 15 presents a six-stage structure for researchers and health practitioners to consider when implementing injury prevention in a sports setting. The recently updated International Association for Dance Medicine and Science Standard Measures Consensus Initiative recommends use of the TRIPP for injury risk reduction in dance environments. 16 Stage one and two pertain to injury surveillance and understanding risk factors relating to problematic injuries. Of note, the third stage of the TRIPP is focused upon developing potential injury prevention strategies, before these are tested in a controlled environment, and therefore this study is positioned within stage three of the TRIPP. Consideration of potential barriers to implementation of injury prevention is usually not discussed until stage five of the TRIPP, following scientific evaluation of a proposed program. However, understanding potential barriers to injury prevention, through consultation with stakeholders, may be useful in the earlier stages of planning, especially where implementation of primary or universal prevention strategies is a goal.
Challenges associated with implementing injury prevention strategies may extend widely throughout a ballet company as an organisation. Adherence and acceptance by dancers and teaching staff alike may present as barriers to implementation of exercise interventions aimed at injury prevention in ballet.17,18 Further, ballet company management staff likely prioritise a cost-effective organisation, and may value the business case of injury prevention. 19 Community outreach officers employed by ballet companies, who may engage with dance schools and families in the community, are also in a unique position to promote safe dance practice alongside an appreciation for the artform. Qualitative methods such as participatory action research (PAR) allow for consultation with those within an organisation in early planning stages of injury prevention.
Participatory action research (PAR) is a post-positivist qualitative paradigm, developed through critical theory, feminist theories, and systems thinking. 20 The goal of PAR is to conduct research leading to social action, involving participants as researchers themselves to plan, act, and evaluate research outcomes. 21 PAR has also been described as ‘spirals of self-reflection’, with fluid and responsive overlapping stages, including planning, acting/observing, and replanning. 22 Previous application of PAR in sport has been for means of general health promotion, concussion recognition and prevention, as well as mental health service delivery.23-26 These consultative processes may lead to a clearer conceptualisation of the way BSI affect a ballet company as a system and enable author-researchers to engage in collaborative practice alongside stakeholder-researchers from within the organisation to formulate a BSI prevention strategy with greater prospects for implementation.
Therefore, this study aimed to engage stakeholder-researchers from a classical ballet company to co-create and prioritise BSI prevention strategies for both professional and recreational ballet dancers, via participatory action research (PAR) qualitative methodology.
Methods
Study Design and Setting
This PAR was conducted within an Australian professional ballet company. During the year in which the study was conducted, the company employed 60 dancers. The company has an in-house health care team, an affiliated academy for secondary school students and a pre-professional (post-academic school) program. The dancers, artistic staff, health team, music, production, and wardrobe are overseen by the Artistic Director. The Executive Director manages finance, philanthropy, business and development, marketing, human resources, communications, and venue/facilities. This present study was initiated following a comprehensive review of injury epidemiology in the company, 3 and a 6-month-long cohort study examining potential causal factors of BSI. Results of these preceding studies were shared with health staff, dancers, and artistic staff prior to recruitment for the present study. All permanent employees (n = 205) and healthcare contractors (n = 8) aged over 18 years were invited to participate in a working group as stakeholder-researchers. Participants were recruited through study advertisement in staff newsletters, town hall meetings and flyers displayed in common areas. The aim was to recruit as diverse a group as possible. 27 Written informed consent was gained from stakeholder-researchers. Institutional ethics approval from the University of Canberra (#11963) was granted and the research was conducted in accordance with the Declaration of Helsinki. If stakeholder-researchers experienced discomfort related to the research process, they were advised that they may withdraw without penalty, and/or to contact the external employee assistance service available to all staff at no cost. Reflexivity statements of the author-researchers are included in Supplemental File 1.
Participants
Seventeen staff within, or contracted to, the ballet company volunteered to participate as stakeholder-researchers. Their roles within the organisation were professional dancer, ballet master/mistress, sports and exercise medicine physician, podiatrist, physiotherapist, Pilates instructor, wellbeing manager, philanthropy manager, events co-ordination, musician, sports dietitian, academy administration and community engagement officer. Eight of 14 non-dancer stakeholder-researchers were previously professional dancers or had trained in classical ballet pre-professionally, and four were male. Attendance at each meeting (number of participants and professions) is outlined in Table 1.
Meeting Attendance of Stakeholder-Researchers and Author-Researchers.
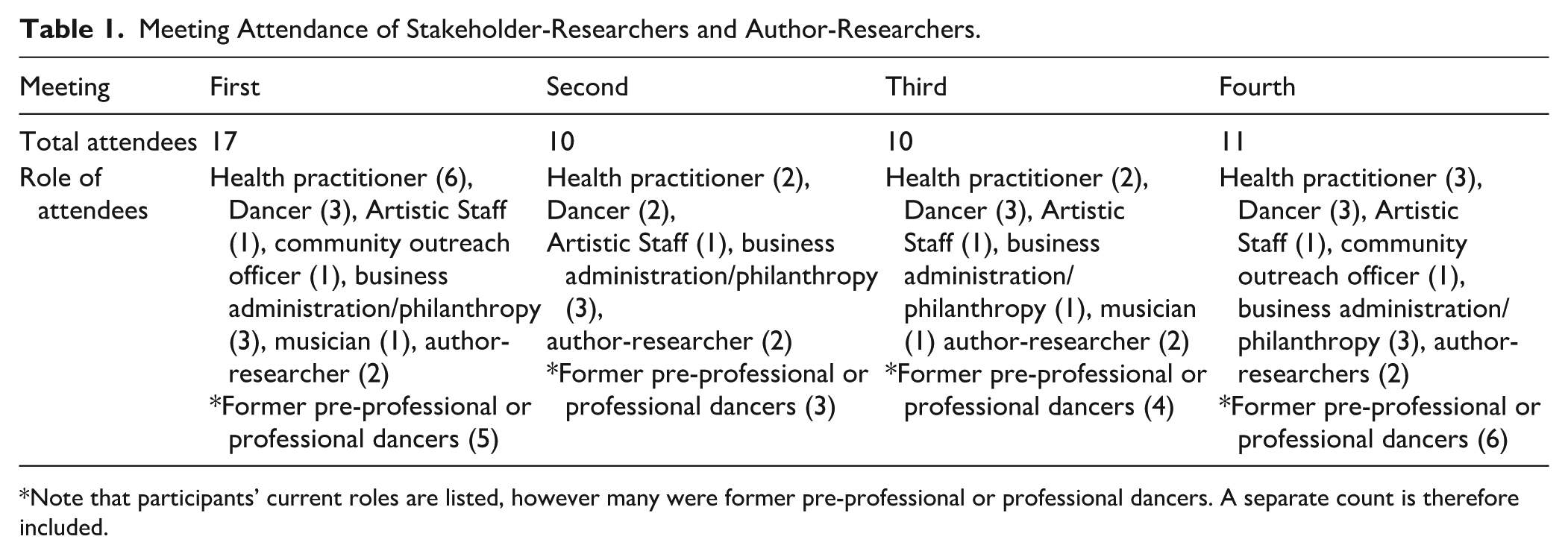
Note that participants’ current roles are listed, however many were former pre-professional or professional dancers. A separate count is therefore included.
Data Collection and Analyses
Four sequential focus group meetings, each an hour long, were scheduled between March and June 2023, attended by two author-researchers and facilitated by the first author. Stakeholder-researchers were invited to attend the meetings either face-to-face or virtually. Each meeting was audio and video recorded using Microsoft Teams (Microsoft Corporation, USA). Meetings were reviewed by two author-researchers and transcribed using the Microsoft Teams ‘transcribe’ function. Transcriptions were verified by the first author. Coding of each meeting transcript was conducted using ATLAS.ti (ATLAS.ti Scientific Software Development GmbH, version 23) software as part of the reflexive thematic analysis. 28
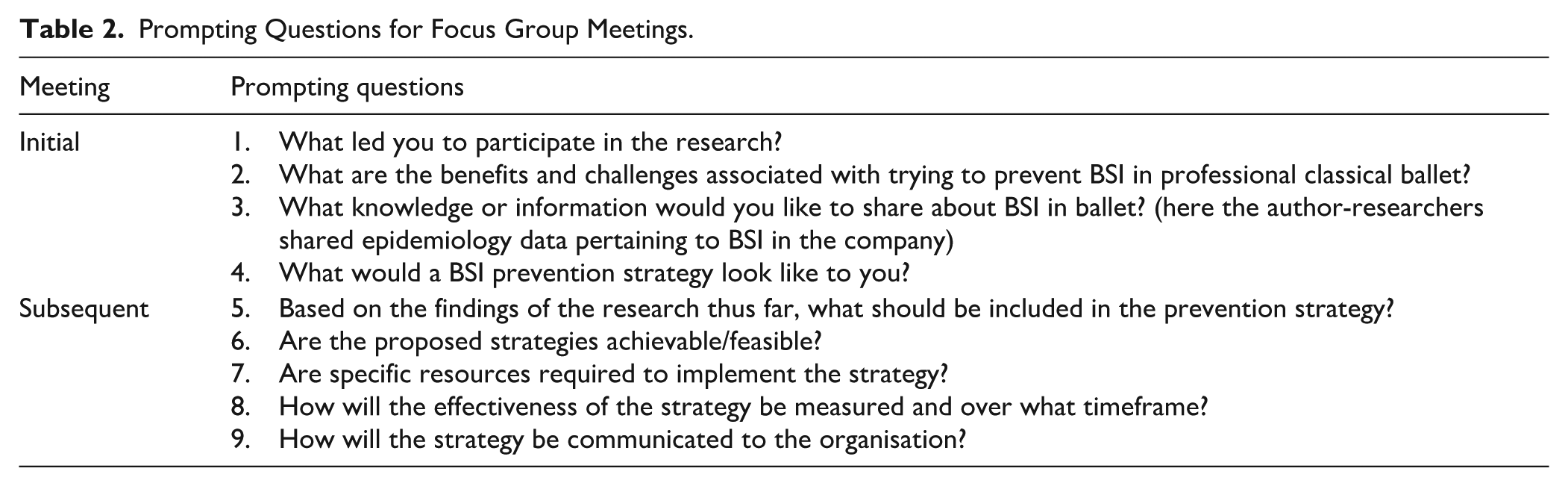
In providing written consent to participate, each participant agreed to read and adhere to the ballet company’s Code of Conduct and engage respectfully with fellow participants. Each meeting was conducted as one focus group with all attending participants (Table 1). A plan for each meeting was formulated by the author-researchers, however stakeholder-researchers guided discussion. 21 Prompting questions for each meeting are included in Table 2. After each participant was asked to answer the initial prompting questions, and more in-depth discussion had commenced, the first author encouraged each participant to share their thoughts using open questions, especially in cases where they had not yet spoken in that particular meeting. All participants were emailed a recording of each previous meeting and prompting questions in advance of subsequent meetings.
Prompting Questions for Focus Group Meetings.
Transcripts were reviewed by two author-researchers after each meeting and before subsequent meetings. The first author’s embedded role as a health provider was recognised and debriefs were held between the first author and last author after each meeting, alongside keeping of reflexive notes. Keywords were identified in each participant statement in the transcript and coded by the first author using an inductive, data-driven approach, from which initial themes were proposed to the stakeholder-researchers. 28 During subsequent focus group meetings two and three, member checking occurred where code frequencies and associated themes from previous meetings were presented visually to stakeholder-researchers in a ‘Treemap’ (ATLAS.ti) for validation and used reflexively to invite reflection and further discussion within the group. For example, in the second meeting, themes presented were simply ‘culture’, ‘barriers’ and ‘facilitators’, however with stakeholder-researcher input and dataset checking, these expanded by the third meeting (were split) to the themes presented in the Results, as the stakeholder-researchers began to delineate professional and recreational/community environments in the context of BSI prevention.
In the fourth (final) meeting, a draft proposal was presented to the group encompassing injury prevention strategies generated in previous focus groups for both community and professional ballet populations. Stakeholder-researchers were asked to adjust or remove any prevention initiatives they felt were not representative and add or detail any that may be missing via consensus discussion. They discussed any current processes in place that would facilitate (or limit) each strategy and prioritised (ranked) each strategy according to feasibility (for example, existing access to a resource, or financial cost). All participants were invited to electronically edit and contribute to three drafts of the final injury prevention proposal.
Results
The primary aim of the research was to develop prevention initiatives for professional dancers. However, during the inductive coding process, it became apparent that participants consistently emphasised the importance of a ‘bottom up’ approach for BSI prevention, starting with measures that need to be considered for recreational dancers in the community. Thus, the scope of proposed initiatives was expanded to include these groups. Key themes that emerged were culture (as an overarching theme), and within this narrative, barriers to BSI prevention in the community (pre-professional and recreational dancers), and barriers to prevention for professional dancers were frequently discussed. Additionally, in exploring solutions to overcome barriers, facilitators to prevention in the community and facilitators to prevention for professional dancers were highlighted. The key action in this PAR process was the collaborative development of a BSI prevention proposal strategy document that was delivered to the (non-participant) Artistic team, Executive staff and distributed to the wider organisation via a staff intranet and newsletter.
Ballet Culture
Ballet ‘culture’, dancer identity and the uniqueness of classical ballet as an artform were discussed. Dancers often identify strongly as dancers rather than athletes from a young age. 29 This was identified as a reason that dancers tend not to access health practitioners who serve athletic populations (such as ‘sports dietitians’ or ‘sports and exercise medicine physicians’), or sports science principles, despite the elite physical nature of classical ballet and the physiological demands placed on the body being akin to sport.
Differing expectations contribute to fear of reporting injury, hiding, or working through pain, especially to impress teachers or artistic staff where performance casting would be affected. The group felt at times, pain and injury may be glorified by teachers, ballet coaches and professional dancers.
These behaviours may be adapted by aspiring dancers, which was highlighted as a potential reason that students might push to perform through injury and, to further detriment, carry these behaviours forward into professional settings.
In the case of a stress reaction or stress fracture, delayed reporting of injury can lead to progression of the injury and result in a dancer requiring lengthier healing times, 30 paradoxically leading to less time performing long term.
Barriers to BSI Prevention for Community Dancers
Stakeholder-researchers identified that they felt health literacy in the recreational and pre-professional dance community to be generally poor. That is – their ability to access, understand, evaluate, and use health information or services in the context of identifying and managing a BSI. 31 Dancers may not be aware that health professionals who work with athletes are also well-equipped to provide dancers with specialised care. For example, specialised medical training is required for sports physicians to understand how to best help athletes who may experience relative energy deficiency in sport (REDs) and menstrual irregularities, which are known risk factors for BSI. 8
Equally, health professionals in the community without specific dance knowledge may not understand the physical demands of their training to be similar to athletes.
The importance of providing education to parents and teachers in the community as well as dancers themselves was emphasised, especially as dancers may seek health information from their teachers/coaches rather than from qualified health professionals.
Intensive training and competition schedules were also considered barriers to young recreational dancers seeking healthcare and having appropriate rehabilitation time for such injuries.
Doubt that much could be done to prevent BSI during adolescence and periods of rapid growth was also expressed by one dancer.
Health professionals who are dance-literate, either within ballet companies, or working with recreational dancers, have an important role to play in educating dance teachers, parents, and dancers themselves. Teachers have a unique and trusted relationship with their students and the need for connection with these teachers to improve the quality of health information being delivered to dancers at the recreational level was highlighted.
Barriers to BSI Prevention for Professional Dancers
The mismatch between sports science principles that are often proposed as part of injury prevention strategies in dance, and the artistic process was discussed. Barriers unique to the context of professional classical ballet, such as the choreographic process and rehearsal timelines that may challenge successful implementation of injury prevention strategies were identified by stakeholder-researchers.
References to timely delivery and access of health information, for example, nutrition information in the professional space, were made by the group, particularly regarding education around BSI, aligning with primary and universal prevention principles. 14
Additionally, psychological pressures and stress were highlighted as being contributing factors to injury:
Therefore, having limited access to psychology and wellbeing support onsite was identified to be a barrier in the context of BSI prevention. Notably, lack of time and heavy scheduling may impede dancers from accessing onsite health services that may assist with primary or secondary BSI prevention, although these are accessible to those who may already be injured (tertiary prevention).
Establishing a workload balance between strength and conditioning for injury prevention and managing class and rehearsals was described as an experimental challenge for some professional dancers, rather than a measured or informed progression. This can become a further challenge when dancers are also injured and attempting to balance cross training during rehabilitation with safe rehearsal participation.
On the note of balancing workload, the length of time spent in pointe shoes and whether or not they need be worn during specific parts of technique class was also discussed, with an agreement reached that this was highly individual and depended on the repertoire one was preparing. However, dancers and former dancers reflected on challenges with pointe shoe fit, customisation, and management as being factors that could influence risk of BSI.
Although it was recognised that preventing injuries may be cost-saving to individuals and organisations in the longer term, initial outlay of funding to action prevention strategies was recognised by the stakeholder-researchers as a large barrier. For example, to increase access to health services in the professional setting.
Facilitators to BSI Prevention for Community Dancers
Researchers identified scope for the ballet company to contribute to education and improving health literacy within community settings. In particular, the benefits of cross training, sports dietetics advice to support dance training, and seeking appropriate health care from dance-informed practitioners.
The stakeholder-researchers reflected positively on their own experiences specialising in ballet during late adolescence, and cross-training in other sports both in their youth and as professionals. Subsequently, the group felt a reluctance to engage in cross-training and a perceived increasing trend in early specialisation amongst dancers in the community was thought to contribute to BSI risk.
Therefore, encouraging cross-training amongst young dancers in the community may have a role in BSI prevention. Assisting dancers in the community to find dance-informed practitioners and dance-specific information for injury prevention and rehabilitation was determined by the group to be an important step for future injury prevention.
Professional ballet companies can be influential role models to community dance schools and programs in cases of health promotion, especially promotion of accessing early care for health issues. Stakeholder-researchers identified several opportunities to educate at the grassroots level that may have an onflow effect of BSI prevention at the professional level.
The community outreach officers spoke of upcoming workshops that were planned to be held in regional towns and considered the possibility of integrating specific education about BSI.
Facilitators to BSI Prevention for Professional Dancers
There was recognition that attitudes towards health and wellbeing in professional classical ballet companies and affiliated academies have improved in recent years, and continue to evolve, which was perceived to be an enabler for future injury prevention strategies. Increasing access to and encouraging dancers to utilise available services was recommended.
Difficulties with monitoring training load were recognised as a key contributor to BSI, and thus a potential avenue for intervention.
Given that the information from wearable devices may not represent a dancer’s perceived recovery, it was decided that further validation of wearable devices was deemed to be a priority, as well as considering how such data would be managed in this setting. Stakeholder-researchers were also in favour of a proactive approach, where dancers were empowered through understanding their bodies through continued and improved access to health services and health evaluations.
Specifically, improved health service access for the company should include psychological support, strength and conditioning, and pointe shoe mentoring.
Finally, the importance of having clear policies and communication strategies in place for addressing situations where dancers were ill, injured, or required modified rehearsals was emphasised, including a commitment to review these on a regular basis.
Overall, the group were open to discussing primary and secondary prevention initiatives that may facilitate ‘stopping injury from happening in the first place’, acknowledging benefits of investing in injury prevention strategies in financial cost-saving for the organisation. The BSI prevention initiatives agreed upon by the stakeholder-researchers indicate priorities for future funding allocation within the company.
Proposed Prevention Initiatives
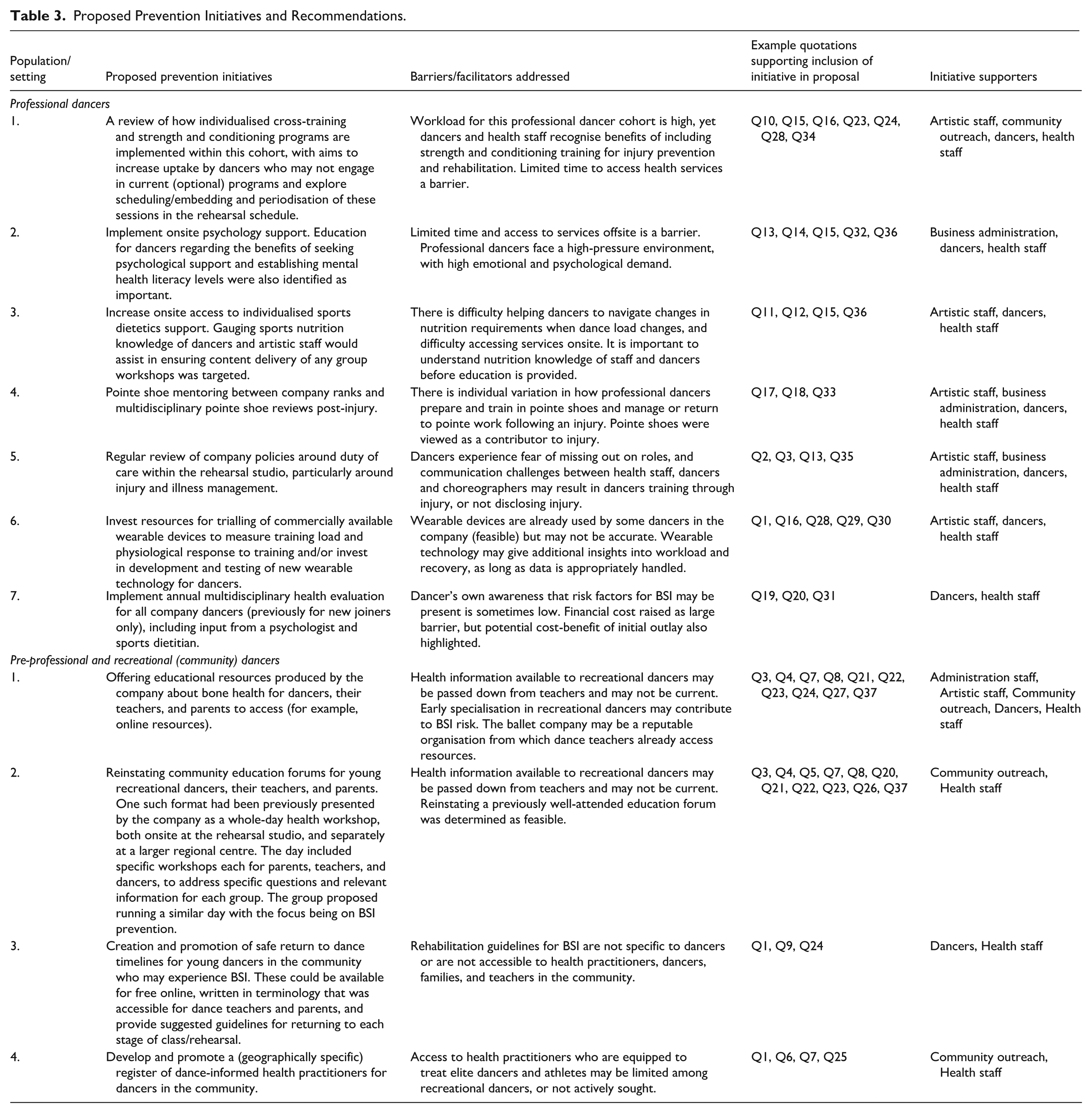
The group prioritised BSI prevention initiatives that may be implemented in the professional environment and in the community, including specific participant groups who supported each initiative (Table 3).
Proposed Prevention Initiatives and Recommendations.
Evaluation of Prevention Strategies
For the professional environment, evaluation methods such as comparison of incidence and time lost to BSI and musculoskeletal injury over a specified timeframe post-intervention were agreed to be appropriate, as per the TRIPP framework. 15 For example, if a rehearsal schedule change that included dedicated time for strength and conditioning for the professional cohort was implemented for a period of time (Recommendation 1 for professional dancers in Table 3), then comparing number of days’ time loss due to BSI pre and post implementation would be important to evaluate the effectiveness of this intervention. Health literacy questionnaires or further qualitative research involving a wider group of dancers and artistic staff to determine health knowledge specific to BSI were also suggested. The group identified that in the community, evaluation of prevention strategies will differ due to the larger outreach and difficulties collecting injury epidemiology data from a broad community population.
For example, if a workshop is run for dance teachers and parents within the community to educate about what BSI are, and the risk factors that may be present in recreational dancers, health literacy surveys with specific questions about bone health and healthcare access could be administered prior to and after the workshops (as suggested in Recommendation 2 for pre-professional ad recreational dancers). Similarly, these could be administered after any online resources (Recommendation 1 for pre-professional and recreational dancers) are accessed.
The stakeholder-researchers suggested that a community-based focus group comprising dance teachers, pre-professional dancers and their parents may assist in determining content to be delivered in education programs and to evaluate these programs. The group also suggested that prospective longitudinal research could journey-map dancers moving from the community into full-time training programs and into professional careers, specifically tracking training and injury throughout.
Discussion
In this participatory action research, stakeholder-researchers from a single classical ballet company collaborated to create a schedule of BSI prevention priorities for both professional and recreational ballet dancers. This study uniquely engaged participants from a variety of artistic, clinical, and non-clinical backgrounds from within a professional ballet company to discuss BSI prevention and develop a concrete proposal for the organisation.
The cultural landscape of classical ballet, and associated power structures may potentially contribute to a culture where injuries are hidden, which in turn, becomes a barrier for injury prevention. It is acknowledged by the authors that some stakeholder-researchers may reserve their opinions in a discussion where their supervisors (or in this case, their coaches) are present. However, the implementation of PAR in this case provided a platform for dancers, to voice their thoughts as equal contributors to a discussion about injury prevention that may benefit themselves and their colleagues. 21 Pre-professional dancers hide injuries from their teachers due to fear, or to maintain their social identity, and may not always feel supported by teachers during rehabilitation. 29 Similarly, in a professional setting, dancers are employed in a hierarchical company system and may feel shame or stigma when seeking healthcare. 32 Furthermore, opportunities to discuss injury prevention via a systems approach outside a medical and allied health team may also be uncommon, however PAR in this application allowed for collaboration across a variety of disciplines, including community education/outreach and philanthropy. These disciplines bring additional perspectives regarding the feasibility of a potential prevention strategy, particularly in areas requiring a coordinated approach from both the managerial and artistic departments of an arts company. As the first author was an embedded staff member, who was familiar to participants, with prior understanding of the company structures and services, this may have contributed to cohesion and co-operation in meetings.
The initial research aim was to focus upon BSI prevention for professional dancers, however stakeholder-researchers felt a bottom-up as well as a top-down approach worthwhile. Thus, a need for improving health literacy of recreational dancers and ideas for prevention in the community were also shared. These ideas are supported in that BSI are often recurrent, 3 and therefore pre-professional dancers who sustain injuries in their training may be at greater injury risk as professional dancers. 33 Further, a solely top-down approach to health messaging may result in lack of uptake at a grassroots level. 23 As emphasised by the stakeholder-researchers, there is merit in acting to prevent a dancer’s first BSI, potentially occurring during adolescence.
Onsite health services are becoming the norm, if not an expectation of professional ballet companies. 34 Barriers to professional dancers accessing onsite health support such as time, stigma, and ballet culture itself were identified in this research, in keeping with previous findings indicating less than half of dancer cohorts (professional and pre-professional) reporting they would seek professional help for mental or general health issues. 35 Psychological and dietary risk factors for injury such as stress or lack of nutrition periodisation36,37 were recognised by the stakeholder-researchers. A periodic multidisciplinary health evaluation may help dancers access dietetics or psychology support where it would otherwise not be sought prior to a physical injury occurring.
According to the updated IADMS SMCI and stage six of the TRIPP model, continuation of injury surveillance using consistent methodology is essential to evaluate any implemented injury prevention program, such as a reduction in injury incidence rates, or time lost to injury.15,16 Funding health onsite health services in professional dance companies has been shown to reduce injury compensation costs. 38 Although included in the proposal, it is not yet known whether a prevention intervention involving multidisciplinary expansion of health services beyond those focusing on physical health (such as physiotherapy) in a classical ballet environment would influence BSI incidence, severity or reduce the associated cost of injury claims. As recommended in the updated IADMS SMCI, new research should focus on implementation and evaluation of injury prevention strategies, such as those proposed by the stakeholder-researcher group.
Limitations
This study was conducted within a single ballet company, and it is recognised that the agreed prevention initiatives may have limited transferability into different ballet environments, or companies that are differently resourced. A further limitation associated with self-selection of participants into the study was that no communications (publicity), technical/production staff, Academy teachers, or wardrobe staff participated as stakeholder-researchers. Whilst former principal dancers, soloists and company artists participated, no current principal dancers or young artists participated. In recognition of the hierarchy often present in a ballet company, representation from dancers across all ranks and staff from each department may have yielded different results. It is probable that staff with an interest in health and wellbeing were more likely to participate, and as the first author was known to those eligible to participate, prior relationships may have influenced recruitment.
Additionally, perspectives of young dance students, community-based teachers and parents of dancers were not heard in the stakeholder-researcher group, as it was not expected that community-based or grassroots interventions would become a focus of the proposal. It would be appropriate to conduct specific research with these groups to ensure the proposed strategies were accessible and feasible to community-based or pre-professional dancers.
Some (but not all) stakeholder-researchers were employed in roles where they would have ongoing access to injury data from both the company and affiliated academy cohorts, however informal triangulation with injury data was not specifically utilised to support trustworthiness in the analytic process. Aside from member checking, the analytic process did not, for example involve formal audit trails or thick contextual description. Much of the focus group time was spent discussing barriers to BSI prevention, which are important to understand from multiple perspectives, especially prior to implementation of prevention strategies. However, this did not leave as much focus group time for detailing and mapping solutions that formed the proposal, which may present a challenge for future implementation. Discussion of several barriers to implementation may also have been a respectful way of disagreeing with the concept that BSI prevention in these contexts was possible. Whilst measures were taken by the author-researchers to facilitate open, respectful, and fair discussion in each focus group, it is still likely that some participants did not feel comfortable sharing the full breadth of their views in a mixed-discipline group. If stakeholder-researchers were not comfortable sharing their views wholly, this may also explain the relatively low disagreement amongst the stakeholder-researchers. Only one member of the Artistic Staff was present at each meeting which, acknowledging traditional company hierarchy, could lead others to feel more confident in a focus group, yet it could also mean implementation of proposed initiatives may be unsuccessful without leadership support.
Conclusion
Participatory action research productively engaged a stakeholder-researcher group within a classical ballet company to develop a prioritised proposal for BSI prevention. Bone stress injury prevention strategies in this specific setting may address both professional dancer populations as well as community or recreational dancers, their parents, and teachers. The proposed BSI prevention initiatives provide a foundation for future implementation research in this company environment. These may include education and outreach programs, scheduled cross-training, use of wearable technology, pointe shoe mentoring, and expansion of multidisciplinary onsite care.
Supplemental Material
sj-docx-1-dmj-10.1177_1089313X261430396 – Supplemental material for A Participatory Action Research Approach to Develop Bone Stress Injury Prevention Strategies in Classical Ballet
Supplemental material, sj-docx-1-dmj-10.1177_1089313X261430396 for A Participatory Action Research Approach to Develop Bone Stress Injury Prevention Strategies in Classical Ballet by Louise Drysdale, Liam Toohey, Kate Pumpa and Phil Newman in Journal of Dance Medicine & Science
Footnotes
Acknowledgements
The authors would like to thank Queensland Ballet for supporting this research, in particular the stakeholder-researchers who volunteered their time and knowledge and wish to be recognised in this publication: Kirsten Baumback, Vito Bernasconi, Zara Gomes, Kali Harris, Lauren James, Julia Lebiocka, Dr Bonnie McRae, Kent Sweeting, Jillian Vanstone.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author is the recipient of an Australian Commonwealth RTP Scholarship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.