
Abstract
Communities impacted by homicide endure profound loss and trauma, yet the voices of those intimately acquainted with navigating its aftermath are often overlooked and undervalued. In this study, we center the perspectives of community violence prevention specialists (CVPS) to understand the role of community-based violence intervention (CVI) in the aftermath of homicide and identify essential needs for fostering holistic and sustainable safety and healing following homicide. Qualitative data collected from in-person, semi-structured focus groups and interviews between March 2022 and April 2023 with 45 CVPS in Baltimore, Milwaukee, and Sacramento were coded and thematically analyzed. We identified various intersecting ways in which CVPS have unique proximity to and perspective on homicide via personal histories and community relationships, crisis response, preventative peacemaking and community healing, understanding violence drivers, CVI implementation challenges, and policy advocacy. Their perspectives reveal nuanced insights into the dynamics of homicide and its prevention. CVI plays a critical role in the aftermath of homicide, and CVPS have invaluable expertise navigating its multi-tiered dynamics, positioning them as strategic responders to homicide and as experts in identifying community needs and solutions specific to violence recovery. Their voices, work, and wellbeing deserve investment and close attention.
Introduction
Homicide is one of the most urgent public health issues facing the United States (US). In the past decade, the nation has lost more than 200,000 individuals to homicide (the equivalent of 55 deaths per day), with countless more enduring nonfatal yet life-altering violent injuries (Centers for Disease Control and Prevention, 2024). Firearms are the leading mechanism of homicide in the US, and in 2020 and 2021, firearm homicide rates reached heights unseen in 25 years (Centers for Disease Control and Prevention, 2021). Devastatingly, injury and mortality statistics alone capture only a fraction of the impact of homicide, as its consequences are complex and encompassing, extending to individuals, families, and communities, reverberating through neighborhoods, and persisting across generations (Pinderhughes et al., 2015; Wintemute et al., 2022).
Communities impacted by violence and homicide endure profound loss and trauma, which is both a cause and consequence of violence—the structural and social drivers of interpersonal violence result in decreased economic prospects, subquality education and youth development systems, and lower property value and stability, which in turn contribute to a lack of community safety and increase the risk of violence, which further worsens economic and safety conditions (Friedson & Sharkey, 2015; Jacoby et al., 2018; Tita et al., 2006). In addition to the years of potential life lost to homicide in the US (Wang & Xiang, 2023) and the myriad sequelae related to violent injury, exposure to interpersonal violence is associated with short- and long-term psychological effects, including posttraumatic stress, withdrawal, anger, desensitization to violence, anxiety, depression, substance abuse, and suicidal behavior (Bancalari et al., 2022). While solely the accumulation of violence exposure among residents within a community could have a particularly harmful impact, the phenomenon of community trauma encompasses more than the aggregate of individuals’ experiences. Community trauma, defined as “the product of the cumulative and synergistic impact of regular incidents of interpersonal, historical, and intergenerational violence and the continual exposure to structural violence,” manifests at the community level, presenting as symptoms such as a low sense of collective efficacy, disconnected social networks, deteriorated environments and unsafe public spaces (Pinderhughes et al., 2015). Furthermore, community trauma stunts community-level social and economic development and undermines efforts to promote health, safety and well-being, enabling a cycle of individual and collective trauma. Given these long-lasting, far-reaching, and patterned effects, communities with high rates of violence may be considered in a perpetual state of recovery from homicide.
Community violence, or interpersonal violence—including homicide—between non-intimately related parties, is a complex social, health, and safety crisis stemming from social and structural determinants of health, which encompass the conditions in which people are born, develop, live, work, and age, and the systematic forces shaping those conditions (World Health Organization, 2024). Exposure to adverse social determinants of health, such as poverty, environmental pollution, food insecurity, lack of educational and employment opportunities, insufficient healthcare, and unstable housing, impacts risk of community violence exposure and involvement through numerous pathways of stress, divestment, trauma, and necessity (Buggs, Kravitz-Wirtz, & Lund, 2022).
Moreover, one of the strongest predictors of involvement in violence is prior victimization (Costa et al., 2015; Palmetto et al., 2013; Turanovic et al., 2018), whether through direct or witnessed physical or emotional harm, or experiences of structural violence—violence resulting from structural injustice and inequity that stems from oppressive societal relations and arrangements and that subjects people and communities to common forms of lived oppression (Buggs et al., 2023). Structural violence, like structural racism, is inherent in the US, a country founded upon using the construct of race as a tool to leverage power and extract resources via systems, policies, and norms that regulate unearned advantages for white and upper-class Americans and the exploitation of Black, Indigenous, and People of color (Sharif et al., 2021). As a result, adverse social and structural determinants of health, manifestations of structural violence, and in turn, the burden of community violence, disproportionately affect Black and Brown communities in the US (Bailey et al., 2017; Buggs, Kravitz-Wirtz, & Lund, 2022; Poulson et al., 2021). For instance, firearm homicide is the third leading cause of death for all young people aged 15 to 24, but the second-leading cause of death for Hispanic males and Black females of the same age, and has been the leading cause of death for Black males, aged 15 to 34, for the past 30 years (Centers for Disease Control and Prevention, 2016, 2024). Research has also shown that Black and Hispanic youth from middle-to-high income households are almost twice as likely as white youth from low-income households to live or attend school near a firearm homicide (James et al., 2021). The term “poverty-induced gun violence” (coined by Lewis [2024] to differentiate the epidemic faced by Black communities from the gun violence typically highlighted in mainstream narratives) aptly reorients these disparate statistics back to the structural harm concentrating violence in particular communities.
Effective approaches to understanding and solving complex and dynamic social and health phenomena require both perspective and proximity. Perspective—the art of perceiving a situation from a distance and comprehending the interconnectedness of elements—provides insights into different viewpoints and theories, while proximity—the state of being closest to the situation and possessing firsthand, context-specific knowledge—provides invaluable depth and authenticity. Despite the inherent value of proximity, government approaches to “public safety” too often overlook this crucial aspect, disregarding the perspectives of those most impacted by violence. As such, these approaches tend to over-prioritize reactionary and punitive methods, disproportionately allocating resources to police and prisons versus the essential needs of affected communities (Dawson et al., 2023). This prevailing paradigm fails to address the drivers of violence and support sustainable community healing.
In contrast, community-based violence intervention (CVI) is a well-documented approach for reaching marginalized and underserved individuals and groups at high risk of community violence involvement by employing trained professionals, sometimes called “community violence prevention specialists” (CVPS), 1 embedded within and trusted by communities, to mitigate interpersonal violence by helping to alleviate acute and chronic drivers (Buggs, 2022; Butts et al., 2015; Corburn et al., 2021; Dawson et al., 2023; Dickinson et al., 2021; Webster et al., 2022). Diverse in theory and design, CVI programs prioritize relationship building, particularly with those at highest risk of community violence involvement, to help address complex needs and support change. The integration of CVI professionals into a city’s safety infrastructure varies by city, influenced by local governance, organizational frameworks, and resources. Not all cities have CVI programs, but where they do exist, they may be funded via diverse mechanisms including local government budgets allocations, competitive grants, private donations, non-profit support, or integration within healthcare systems. CVPS may be supervised by government officials, non-profit leaders, or healthcare administrators, and can be either paid employees or volunteers with varying levels of job security. Across contexts, CVPS embody a unique fusion of perspective on and proximity to violence and homicide, possessing not simply the theoretical understanding but also lived, personal and professional experiences crucial for creating solutions to address the complexities of community violence and trauma.
The analysis presented here stems from a larger research project that seeks to expand understanding of the experiences of frontline CVPS and the individuals they serve. The broader study probes CVPS’ perspectives and insights related to topics such as drivers and mitigators of violence, challenges associated with violence intervention and CVI program implementation, and the needs of CVPS as well as their clients. In this paper, we center and recognize CVPS as experts in navigating the aftermath of homicide, contextualizing their experiential wisdom with our understanding as researchers. By exploring and documenting CVPS’ proximity to and perspectives on homicide, this paper aims to inform deeper and more nuanced understandings of community violence and effective prevention strategies.
Acknowledgment and Appreciation for Participants
The research team is deeply grateful to the CVI professionals who graciously and frankly shared their experiences for the purpose of this project. Though not identified to protect confidentiality, all were hopeful that their expertise and lessons learned will be leveraged to elevate the field of CVI and to honor the professionals who put their lives on the line to prevent another homicide. We thank them for all that they do and the sacrifices they have made to support their teams and help save lives.
Positionality Statement
The authors acknowledge that our identities, social positions, and personal histories play a role in the research process and outputs. We also recognize the inherent power imbalances in research and the potential for academic knowledge production to reinforce harm. Thus, we engaged in reflexive practices, both individually and collectively, throughout the research process (Abdelnour & Abu Moghli, 2021). Approaching the work with informed perspectives of the racist and capitalist underpinnings of community violence, we iteratively and continuously engaged in critical self-reflection and self-inquiry, conducted analyses in close collaboration with each other, and presented findings using participants’ own words as much as possible. While these practices likely reduce bias, the reader should be aware of the authors’ positionalities, which are detailed in Appendix A.
Methods
The data used in the current analysis were drawn from a qualitative research project which engaged CVPS, as individuals with personally and professionally informed perspectives on the aggregate experiences and needs of people involved in community violence, to gather knowledge and insights about the drivers and mitigators of violence involvement and the resources and opportunities existing or lacking to facilitate community safety. CVPS were recruited from Milwaukee, Wisconsin; Baltimore, Maryland; and Sacramento, California to participate in focus groups and interviews that explored the experiences, successes, challenges, existing resources, and needs of both CVPS and the individuals they serve. Recruitment spanned multiple cities and programs to include a breadth of perspectives, increase the generalizability of findings, and enable comparisons of the aggregate experiences and needs across place. Sacramento, Baltimore, and Milwaukee were selected because all have higher-than-average rates of violence compared to their respective states. They also have made local investments in recent years in community-based efforts for violence reduction, and the senior author (SB) had preexisting connections in these cities to leverage for recruitment. Purposive and convenience sampling methods (Penrod et al., 2003) were utilized to ensure all participants had content and experiential expertise, with CVPS identified from the author’s relationships with CVI program leaders and their referrals.
The senior author (SB) conducted 11 interviews and nine focus groups with a total of 45 CVPS, representing 11 distinct CVI programs, between February 2022 and March 2023. Participant characteristics are in Table 1. After obtaining verbal consent from each participant, a semi-structured qualitative data collection approach was used to guide interviews and focus groups while allowing flexibility to delve deeper into certain topics and ask follow-ups based on participants’ answers. The interviewer employed trauma-informed practices, including building rapport to establish a comfortable and safe environment, obtaining informed consent to ensure participants understood their roles and rights, regularly checking participants’ willingness to continue, and having flexibility to adjust the interview process based on a participant’s emotional state (Alessi & Kahn, 2022). The decision between utilizing a focus group versus an interview was determined based on whether the participant’s CVI responsibilities were primarily team-based or individually directed (e.g., coordinated outreach versus case management). The interviews and focus groups were held in the CVI programs’ respective cities, with specific locations chosen by CVI leaders or participants to ensure data collection occurred in places where participants felt comfortable and safe. Each interview or focus group lasted about 60 to 90 minutes, and participants received a $100 gift card for their time. Interviews and focus groups were audio recorded, and recordings were transcribed using a professional transcription service (Rev.com). All transcriptions were reviewed and edited for accuracy by the study team, cross-referencing with the audio files and consulting with the interviewer for clarity, when needed.
Participant Characteristics.
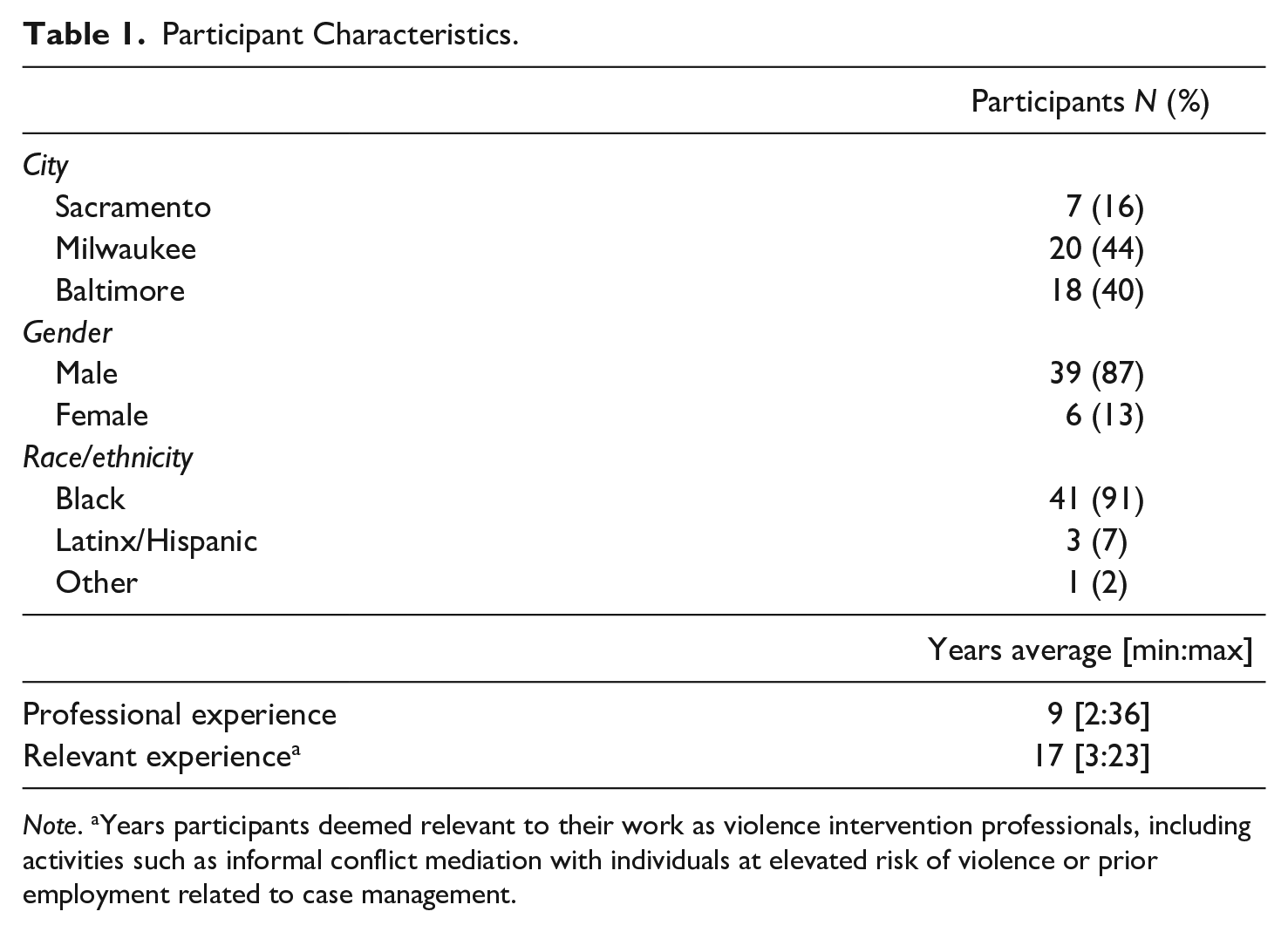
Note. aYears participants deemed relevant to their work as violence intervention professionals, including activities such as informal conflict mediation with individuals at elevated risk of violence or prior employment related to case management.
Thematic analysis was conducted at a semantic and latent level using grounded theory. Thematic analysis was used as it is a flexible method for identifying and organizing patterns across a dataset and making sense of collective meanings and experiences (Braun & Clarke, 2012). The grounded theory approach was applied to ensure hypothesis generation was driven from the data and thus grounded in and reflective of the reality of the participants (Chapman et al., 2015). Starting with a list of potential parent codes drawn from the interview guide, a codebook was collaboratively derived from the data. Each author open-coded two transcriptions, the team met to compare and rectify discrepancies, the codebook was updated accordingly, and this process was repeated until synergy was achieved. Once the codebook was considered comprehensive and succinct, all transcripts were inductively coded, meaning codes were applied based on the content of the data rather than based on any preconceived ideas or concepts brought by researchers (Braun & Clarke, 2012). All coding was done by the junior authors (JL, AA, AI) using Dedoose qualitative software.
For the purposes of this paper, we analyzed a subset of codes most relevant to CVPS’ experiences with and perspectives on homicide and its aftermath. The analysis process involved reviewing all relevant excerpts, interpreting the main takeaways directly from the CVPS’ perspectives (semantic-level analysis), and noting any pertinent research or contextual understandings to the emerging themes (latent-level analysis). Theme generation was an iterative process which involved identifying themes from meaningful patterns in the analyzed data—such as recurring concepts or clustering code groups—that were relevant to the research questions. The relationships between themes were explored to ensure they were clear, distinctive yet interconnected, and created a coherent narrative about the data. Once final themes were determined, they were named, summarized with insights from code analyses, and illustrated with relevant data excerpts. To enhance readability and protect participant anonymity, quotations were carefully and minimally edited (removed duplicate words, filler words, and potentially identifiable information), without modifying their underlying meaning. Periodic and frequent team meetings allowed authors to integrate learnings from each other, raise questions, and exercise reflexivity, ensuring consistency and rigor throughout the coding and analysis process. This study was approved by the UC Davis IRB as exempt research.
Findings
We identified various intersecting ways in which CVPS have proximity to and perspective on homicide via personal histories and community relationships, crisis response, preventative peacemaking and community healing, understanding underlying drivers of violence, CVI implementation challenges, and policy advocacy. Notably, these findings were recurrent and prevalent across all cities studied.
Personal Histories and Community Relationships
One way that CVPS are connected to homicide is through their own lived experiences, both personal and professional. All 45 CVPS had some level of direct or indirect exposure to, and sometimes involvement in, violence prior to their work in CVI. Furthermore, CVPS are often native to the communities they serve and have similar backgrounds and experiences to those they seek to engage. They themselves are often surviving family members or friends of homicide victims. This proximity sharpens their understanding of homicide and the needs and perspectives of those affected by violence, positions them to build trusted relationships that can be leveraged for prevention and intervention efforts, enables their trauma-informed approach and fuels their dedication to community healing.
As described by one participant in Milwaukee: Lived experience, meaning that you’ve lived the life, you’ve been in- uh, I hate to say it like this, you’ve been in very hood situations, (laughs) you know, you’ve been in very challenging situations, meaning you may have did some time, you may have formerly been the shooter at one point, you may have formerly been the co-conspirator of violence in the neighborhood. You may have been that, and you’ve made a change in your life and now you have an opportunity to go back into it and now you can save the lives. Now that makes you credible because you can’t really go in and build these relationships in the neighborhoods without having some type of inroad or some type of, um, street cred is what they call it, you know? And. . . the best violence interrupters are those that have that street cred.
Having trust and credibility is an asset in CVI work (Wical et al., 2020), facilitating effective networking, mediation of conflicts, engagement and influence with those at risk of violence involvement, and linkage of individuals to essential support systems. One participant in Baltimore, drawing from their own experience turning away from criminal activity, underscored the profound role that credibility and relatability play in mentoring an individual to desist from violence: If better opportunities was presented to me, I woulda took ‘em only if the messenger had been a person who understood me, understood my condition, understood my reality and my circumstances. ‘Cause therefore, he woulda had to have came right from outta the same stuff that I was stuck in. And he would have to be presentable. He would had to have been successful, right? He woulda had to been a model for me, see? For me to say, “Damn, if I give up this. . . ‘cause if Ima give this up, I gotta have something in return,” Right? . . . and he gotta have the right message, right? . . . I woulda listened and I’d a gave it a shot.
Moreover, CVPS’ shared experience and connection to the community drives a passion for the work, as many are motivated to give back and steer individuals away from lives of violence. For some, this commitment stems from a sense of responsibility to atone for past contributions to harm (LeBel et al., 2015), driving them to tirelessly strive for positive change. As one participant in Baltimore described, they “try and lead by example, show people that you could change. ‘Cause a lotta us come from being a part of the problem, and now we’re trying to help them, help them fix it. So that’s like, just showing other people that they can change too. It ain’t ever too late.”
However, their closeness to the work can also pose challenges (Bocanegra & Aguilar, 2024), as CVPS navigate the complex position of having hindsight on past experiences while remaining in close physical proximity to the triggers, trauma, and reputations of their past lives.
[It’s a misconception] that because I have lived experience, it’s that much easier. “You got it, it’s not a big deal. You should know everything about it. It should be that much more easier for you, because you have lived experience.” But. . .it actually is a little bit more challenging, because previous experience just don’t end. You just don’t say, “Yes, I have previous experience. I’m done.” I’m still experiencing this, not even professionally, but personally you still experience, because this is where you come from, and it just doesn’t get wiped away. You just figure out a way to live with it and give back to your community. But I’m still living with it.—Sacramento professional
Particularly among professionals who have recently turned away from violence or are earlier in their “healing journey,” sending them back into environments without appropriate training, safety considerations, connections, and relationships with the individuals they are engaging can be additionally damaging, as described by a Milwaukee participant: Like we’re asking people who, in some cases, have been harmed, including incarceration, for being . . . actively involved in the environments that we’re sending them back to. And so for some, they’re not ready for that. And we’re setting them up for failure or relapse.
Even experienced CVI professionals noted challenges in navigating certain interpersonal dynamics while remaining consistent with their messages of nonviolence: I’ve been presented in those situations, too, where they, the younger guys challenged me. . . And I always try to just be quiet and let them vent because it’s usually something else happening. You know, that’s what I’ve learned over time, but it’s hard. It’s hard for me too . . . And I’m . . . I consider myself educated, I consider myself understanding and empathetic, um, but it’s hard. It’s hard if somebody is calling you a bitch in, in front of people and, you know, I know what I’m capable of, you know. . . So, it’s like it’s hard to not hurt someone who’s, who’s deliberately trying to hurt you, you know, in the culture that we grew up in.—Baltimore professional
Crisis Response
CVPS are often among the first responders at the scene of a homicide, playing a crucial role in promoting healing and preventing further violence in the immediate aftermath (Giffords Law Center, 2021; Hureau, Wilson, Jackl, et al., 2022). Shortly after a homicide occurs, they may be a source of support for surviving family or community members, connecting individuals to resources when available and helping to navigate the grief of the loss.
We don’t fear being in a neighborhood where people were just shot the day before, we just know that God is with us, and when we’re out there taking care of it like that, it’s an amazing feeling, when we have people come to us and they say, “We knew y’all would be here, thank you so much.” Um, we pay for a funeral, we’ve got pastors who give up their churches because the families don’t have any money. We’ve got pastors that will do a eulogy. And, again, just little pieces of the components that we find that we do that you may not necessarily see on the news.—Baltimore professional
Another element of their immediate response to a homicide or shooting is preventing retaliatory violence, which they do by gathering information, engaging their networks, and offering support to individuals on both sides of a conflict. As said by a CVI professional in Milwaukee, “We’re not here to. . . you know, to make the judgment call on who shot who and why they shot ‘em. We’re just here to assess for that retaliation and then also be that support to them and their families.”
CVPS spoke to the complex dynamics and unique challenges surrounding situations where “blood has been shed” or someone has been killed: Once blood is spilled, it’s hard to stop other blood, you know what I mean? Because that family member [says] “No, he killed my cousin”. So, it’s hard to reason. So. . . we engage, we go to the hot areas, we go. . . If somebody got killed [in a certain neighborhood], we go actually right where they got killed at and talk to the people, try to settle it and cool heads and make them look at things a little more logical.—Baltimore professional
They emphasized the importance of leveraging social networks to assess these situations before intervening to ensure the greatest chance of keeping CVPS safe and successfully interrupting violence; in the words of a CVI professional in Baltimore, “[not] diving in head first not knowing what’s going on. . . [but] always try[ing] to assess the situation before you run into it.” CVPS’ proximity to the harm and trauma caused by homicide, and the unique challenges and dangers that emerge post-homicide, deepens their commitment to prevention or intervening before conflicts have escalated to such a challenging point.
Preventative Peacemaking and Community Healing
Both preceding and following a homicide, CVPS engage in preventative peacemaking and community healing as an ongoing practice (Corburn et al., 2021). They are constantly embedded in communities experiencing violence and implement a wide array of innovative strategies to help cultivate social ties, mediate conflicts, negotiate ceasefires, and connect individuals to needed supports.
CVPS take a holistic approach to healing (Corburn et al., 2021), recognizing the need to tend to both individuals and their broader communities, who are perpetually recovering from the effects of homicide. This unique approach sets CVI apart from traditional forms of public safety by empowering communities from within and fostering long-term resilience and recovery.
The police’s job is to come in and enforce the law. You know, our job is to come in and do engagement, you know, and they’re not coming in saying, “Hey, um, you know, clean this up,” or anything. They coming in guns a blazing, you know, they’re coming in to enforce what they want to enforce, whereas we come in and say, “Hey, we want you to take ownership of your community and . . . Engage your own community in practices that are healthy, that are safe and that people can know that they still can have a quality of life, you know?” And so that’s kind of where our goal is when we talk about that transformative piece, ‘cause we’re doing the transformative piece, not just to the individual, but to the community as a whole, you know?—Milwaukee professional
The effects of their peacemaking and conflict mediation ripple throughout the community; by stopping a single violent incident, they are fostering broader community safety, stability and peace. As illustrated by a participant in Milwaukee, this type of conflict mediation requires a unique strategy rooted in community understanding, trust, and strong social capital: We may have a situation where we in the neighborhood and we hearing rumblings about two different sets getting ready to beef, you know, and we know that they’re in tune with each other. So, we’re like, “Hey, what can we do to help?” You know, like, “What’s the beef?” You know, if it’s over money, if it’s over whatever, we want to come in and try to help navigate that because we still got elderly people that live in the neighborhood, we still got young people that are living in the neighborhood, we still got. . . you know, and this type of violence is gonna do nothing but damage both sides. So how do we help? So that’s kind of our angle and a person that has lived experience understands the dynamics of that particular life and what the street rules are. . . And then also your social capital, social network. “Okay, how do I put you in connection with people” to where we can help navigate how to either do conflict resolution, or if it’s over resources or lack of resources, “Hey, let’s put you in tune with some people that we know that can get you what you need so that this type of stuff don’t continue to happen.”
Attuned to the needs of community and the underlying drivers of violence, a critical tenet of CVI is connecting clients and their families to crucial resources and support systems (Dawson et al., 2023; Dickinson et al., 2021; Goodwin & Grayson, 2020). This may look like offering therapeutic services or referring clients to appropriate systems of care for physical and mental health problems, connecting them to employment services or other economic support programs, or helping to secure safe housing. As one Milwaukee professional explained, violence is often the byproduct of attempts to secure one’s basic needs: “If you’re not eating and you don’t have a way to eat, I mean, nine times out of 10 you gonna go and make a way. Whatever that may look like for that individual. So. . . the goal is to go and prevent [violence] by supplementing with a resource.”
In some cases, the provision of resources to the community creates a reciprocal exchange that grants CVPS cooperation and communication with groups at heightened risk of violence, leading to a compounded positive impact. One participant shared, We bring in, like, food boxes, we bring in resources, we bring in, you know, health stuff. . . we coming into the neighborhood, you know, as a peace offering. . . you know, and we get the permission from those that are calling the shots. We may pick up the phone and say, “Hey, hey, we gonna be down by the neighborhood, you know, are people gonna be down there? We doing some stuff for the block. Can you get your guys off the block for a minute, or. . . can we do a ceasefire?”. . . And in exchange for that, in exchange for that type of cooperation, you know, they allow us to bring those resources into the space, you know.—Milwaukee professional
While engaging in efforts to support the community at large, CVPS also actively strive to connect with individuals at the highest risk of violence involvement (Papachristos et al., 2015). Drawing from their own relatable experiences and social capital, they locate individuals that may otherwise be unlikely to engage in services (Boag-Munroe & Evangelou, 2012; Branas et al., 2020), build authentic relationships, and may act as mentors, steering individuals away from harmful paths and preventing further violence. Oftentimes, this requires “relentless engagement” by CVPS, who are driven by their commitment to promote community safety and understanding of what it takes to build trust, as evidenced in this quote: It’s been times where we’ve knocked on a kid’s door for about six months and they will sneak, they will look at, look at us coming, coming through the front door and [they] run out the back door, you know what I mean, but we, you know, we continue to just keep going, keep going. We let them know, you know, like, “You’ll get tired of us before, you know, we get tired of you,” and we just keep trying and then once they, once they finally give in and we got our arms around them, you know what I mean, then it’s like they don’t wanna go nowhere. They get in any kind of trouble, we the first ones that they call. So, it feels good to just know that, you know, they depend on us and we able to have the resources to actually help them with whatever it is that, that they need.—Baltimore professional
Understanding Underlying Drivers
In addition to addressing the proximal antecedents of violence, CVPS are deeply attuned to the structures and conditions that generate homicide and hinder recovery in its aftermath. While structural drivers of violence and trauma are widely documented in the literature (Buggs, Kravitz-Wirtz, & Lund, 2022; Poulson et al., 2021; Sharif et al., 2021) and have long been recognized by the communities most impacted (Cohen, 2024; Forman, 2017; Hunter & Robinson, 2016), CVPS’ personal testimonies go beyond validating this knowledge base and provide nuanced understanding and perspective to inform responses to homicide and its prevention.
Participants commonly pointed attention towards the structural factors perpetuating violence in their communities, including poverty, generational deprivation, housing insecurity, employment deficiencies, and firearm availability. The pathways between these various, intersecting insecurities and the spatial concentration of homicide were illuminated by one Milwaukee participant: I think in Milwaukee, in the neighborhoods where we’re seeing the highest rates and counts of gun violence, those are also the poorest neighborhoods, the least invested in neighborhoods. The neighborhoods with the highest unemployment rates. When people can’t survive, when people can’t thrive, when people don’t have investment, or the things they need to just simply live, that’s a recipe for violence all day long. . . I think at the root of it, it’s like, people are desperate. People are tired. People are angry. People don’t have what they need to not take their frustrations out in a way that is [not] healthy or acceptable.
CVPS also highlighted that trauma at the individual and community levels, whether experienced personally or vicariously, is immensely present in communities dealing with homicide and serves as both a catalyst and sequela of violence (Bancalari et al., 2022; Pinderhughes et al., 2015). Reflecting on their own past, one CVI professional in Sacramento articulated the intricate relationship between unresolved, compounded trauma and risk of violence: [Trauma plays] the most present role. . .So just using me as an example. I’m not intimidated by seeing the wounds that I see now because of the way I was raised, right? So I could definitely tell you when the first time I ever saw an open wound from a stab wound or a gunshot wound, that it was like, whoa, that is deep. Right. But over time it just was really normal for me. Again, when I started in this line of work, and I realized that wasn’t normal. . . And the vicarious trauma that I didn’t know was even a term until I got in this line of work. I now see how that shaped me as I grew up. And. . . I experienced other traumas that then build on the trauma of also me being that person that was assaulting others. Right? So again, it’s not like I just woke up and said, “I’m going to fight people because that’s the one thing I need to do.” It became that because I had so many other traumas in my life, and I didn’t know how to battle them. Right? I didn’t know how to process them. And so it was just so easy for me to make decisions that seemed, I had take matters into my own hands and no one else is going to protect me, but me. And so, with our young people, I see the same effect. Like they been in traumatic situations, didn’t know they were traumatic situations. Then they get violently injured. And now we’re telling them, “There’s a lot of trauma that can come out of this.” And they’re like, “What are you talking about?” Or they’re like, “Oh yeah, they’re talking about just this, like this isolated incident.” And then you talk with them and then you realize, or they realize, “Man, I’ve actually been traumatized before, or I’ve had trauma in my life before.” They work hand in hand.
Their testimony underscores how the challenges facing communities highly exposed to violence can lead to a normalization of violence and a lack of awareness of trauma, its manifestations, and effects. Additionally, a CVPS in Milwaukee identified the stigma associated with seeking mental health care in these communities as a hindrance to healing, perpetuating the cycle of trauma and violence.
Mental health, there’s, like this stigma within the Black and Latino community. We don’t get help, mental help. We don’t get it. So, with that said, it’s like, you see someone murdered or shot, or you’ve been robbed or shot, no one’s thinking like, yeah, I might have PTSD, and that’s why I’m so willing to kill someone that looks like me, now. No one’s thinking about this, at all, whatsoever. So, that creates a major cycle.
The enduring impact of trauma within families and communities affected by harm emerged as a significant concern. The ripple effects of incarceration were explained by one Milwaukee professional as: “that trauma being trickled down to family members which cause that secondary trauma as well.” Alcohol and drug use was frequently described as a coping mechanism for unaddressed traumatic experiences, which, in turn, increased the likelihood and severity of violence. Describing the escalating prevalence and intensity of drug use within their community, one expert from Sacramento remarked: It’s like the regular weed don’t get you high enough, so then you got to go get the other stuff, and then that stuff don’t get you high enough so now you’re going to this synthetic, so concentrated stuff because you can’t reach the high that you want to reach and it’s all because of the trauma. You’re trying to run from this trauma and as soon as your high goes away, guess what? Your problems are staring you in the face. They didn’t go nowhere just because you got high, but if you can escape it for those couple hours that’s good enough for you right now. . .
CVI Implementation Challenges
CVPS are intricately familiar with the political, institutional, and programmatic challenges hindering community-based violence intervention and prevention efforts, and conversely, what is needed to successfully do this work. However, they are often not included or engaged in programmatic and policy decisions that impact them: I see a lot of them pushing the agenda without understanding what it’s like. . . when you’re in it. And I suggest all the time, “Come and see. Come see what it looks like on our end.” So then, when he’s trying to come and implement a process or a policy. . . it’s hard for us to kinda take you serious when you don’t know what the work looks like but then you’re trying to implement a process for it.—Milwaukee professional
CVPS expressed frustrations at being told how to go about their work by people not familiar with the community needs or the unique context surrounding community violence; one Baltimore participant equated this to “[them] going to the hospital and trying to tell a doctor how to implement surgery when [they] know nothing about being a doctor.”
Across cities and programs, CVPS cited difficulties securing funding, defending their credibility to those in positions of power, navigating bureaucratic hurdles, and obtaining sufficient institutional support. These challenges are exacerbated by a lack of standardized structure for organizing CVI programs, along with funding inconsistencies and varying training protocols, professionalization requirements, and service connections. They described how these obstacles undermine the effectiveness of CVI and impede CVPS’ ability to best support individuals and communities post-homicide.
Financial strain, exacerbated by low pay, was described as undermining CVPS’ capacity to fully engage in their crucial roles. Some described being unable to sustain their own needs, referencing housing challenges or needing to take on additional jobs: “Frontline workers don’t get the pay, they don’t get the benefits, right? Um, they barely making it, sometimes have to work two, three jobs” (Milwaukee professional).
CVPS also highlighted the potential detriments of lacking institutional trust, support, and guidance, which sometimes manifested as feelings of anxiety surrounding potential procedural mistakes or liability issues that might jeopardize their job or the CVI program. For instance, one Sacramento professional discussed a risky client intervention where they faced the dilemma of either risking their own safety without adequate backup or failing to fulfill their duty to promote safety for the client: Like, can I call my program coordinator and say, “Hey, there’s these people that want to fight so and so, and I need a reinforcement.” Ain’t nobody going to send nobody to help me. It’s going to be like [Coordinator:] “This is a huge risk and liability, you must not go there.” But I’ve actually done that before [gone in without support] so that’s created a solution. Talking it out with the people who are literally waiting downstairs to fight this person saying, “What do you need from her? What do you need? Why is it that you guys have this interaction?”. . . And so, it’s really, really rare when you have a team or when you have an institution that says, “We’ll find those solutions with you, and we’ll stand behind you.” And so that’s a huge barrier.
Frequently emphasized was the need for more institutional support to facilitate CVPS’ efforts to meet their clients’ pressing needs, including creating new resources where none exist and making available resources more accessible. A Baltimore professional described how reliable delivery of resources would not only support community healing but also foster trust and rapport between CVPS and potential clients, further enhancing CVI effectiveness.
We’d have a bigger impact on our community. . . being able to plug people straight in with different resources. Like, that would just be tremendous for the community, for any community. You know what I mean? That builds trust, that builds rapport. . . That changes a lot of things. When you able to actually, you know, deal what you telling people you can help with, you know what I’m saying? And it gives people that trust and comfortability to come to you for that help too, as well. ‘Cause that’s a lot of the problem as well; people scared to ask for the help, you know what I’m saying? They knowing, like, “Man, if I go talk to somebody with [CVI program name], they going to help me. They not gonna talk about me. My business ain’t gonna be in the streets. . . I go there, I’m gonna get what I need to get.” And that’d definitely help us a lot.—Baltimore professional
CVPS commented that their programs have a responsibility to make sure they are carefully selecting potential candidates for the job and not “leaning too much on lived experience” (Milwaukee professional), but providing the proper training, monitoring, supervision, and support to mitigate any concerns related to worker wellness and effectiveness. But they also perceived a double standard within health and safety systems, in which CVPS lack the autonomy, credibility, and institutional protections afforded to other public servants: We haven’t had a public relations situation where our street outreach worker has done. . . committed some crime and their face is plastered on the news. And like, you know, “peace worker, shoot somebody”. But what I will say is that they should be given the same grace that law enforcement, that doctors and other professions have when they lose someone or there’s an accident or there’s malpractice or intentional, whatnot.—Milwaukee professional
Participants expressed frustration with the necessity to defend their credibility and value through data-driven metrics that narrowly focus on failures (e.g., violence, arrests) (Branas et al., 2020), despite the inadequacy of traditional measures in capturing the nuanced impact of their interventions. For example, one Baltimore professional recounted an interaction with a young person experiencing suicidal ideation, in which they felt they were able to prevent a potential tragedy not by following a precise protocol, but by leveraging their established relationship and rapport with the individual: There’s no teaching for that type of shit. You just gotta figure it out on the fly. . . you know, a social worker or someone who might be armed with the book skills and the technical skills in those situations, and it could possibly work, but the connection is what works for me all the time, right?. . . I had been telling them I love them for two to three months; we had a connection. That’s why he called me when he was in pain. . . And if people don’t wanna say love ‘cause it’s mushy or it’s not a thing we can put on paper and measure with data, it has to be some form of service, I guess, like maybe like if we wanna measure it some kind of capacity, how much service you provide and the language you use when you engage, the level of engagement and the amount of service, maybe we can try to find a way to put it in words and measure it.
Emphasis was placed on the critical need for expanded mental health supports for CVI staff to best fulfill their roles: “the sick guys gotta heal themselves first, the sick can’t heal the sick. We gotta get well first” (Baltimore professional). Not only do CVPS enter the CVI workforce with their own exposures to community trauma and histories of traumatic events, but they must also navigate additional levels of trauma through the inherent risks of their jobs (Free & MacDonald, 2022; Hureau, Wilson, Jackl, et al., 2022; Hureau, Wilson, Rivera-Cuadrado, et al., 2022). Every day in the field, CVPS put themselves in harm’s way, physically and emotionally, risking personal or vicarious exposure to violence and bearing witness to the trauma healing process of their clients.
I be needing some trauma therapy. Like, just going through this every day, just seeing the people that you know, and watch grow up die, and then, you know, it just starts happening over and over, then dealing with things in your family, and you know what I’m saying? . . .It becomes overwhelming. . . And then taking it home. Like, I take the work home, you know what I’m saying? Like, my girlfriend don’t want to hear it. Like, every time I come home, it’s like, “ I don’t want to talk about that. You know, you out there every day. Talk about something else.” And it aint like I be meaning to drop it on her, but it’s just, it becomes natural to me because I’m out there in it every day. . . So, I think we need somebody to talk to sometimes too, just to kinda like vent to.—Baltimore professional
Policy Advocacy
In addition to the institutional supports needed for CVI implementation, participants advocated for a range of policy strategies they believed are essential for breaking cycles of violence and addressing the structural drivers of homicide. The strategies they lifted up are evidenced-based and included economic support policies (Dalve et al., 2022; Rowhani-Rahbar et al., 2022), housing policy and renter protections (Cui & Walsh, 2015; Freedman & Owens, 2011), improved employment opportunities (Blumstein et al., 2000; Schleimer et al., 2022), access to food (R. N. Smith et al., 2020), provision of mental health services for both community members and CVPS (Bocanegra & Aguilar, 2024), implementation of stricter regulations on firearms (Crifasi et al., 2018; Degli Esposti et al., 2023), adoption of pro-healing initiatives for formerly incarcerated individuals (Jones, 2018; J. M. Smith, 2021), investment in programs that foster positive youth-adult connections (Culyba et al., 2016; Fagan & Catalano, 2013), and increased and sustained funding for and advocacy efforts on behalf of CVI (Buggs, 2022; Ross et al., 2023).
CVPS underscored the need for policies and programs, and particularly mental health resources, to be culturally responsive, trauma-informed, and rooted in historical understandings of the harms inflicted on communities disproportionately impacted by homicide. When services are not tailored to the cultural needs of the community, they run the risk of deterring or re-traumatizing individuals seeking help, as exemplified by this Baltimore participant’s experience: “But it can’t be no psychiatrist. Because the last time I talked to a psychiatrist, they called the police on me. I’ll never forget that.”
Recognizing the critical need for those with proximate knowledge to be involved in policy and program choices that impact communities navigating violence, CVPS frequently expressed frustration at the marginalization of their voices and articulated a strong desire and willingness to participate in discussions aimed at crafting solutions.
I don’t think I’ve ever met people who are policy makers that are saying “[CVI professional], can I interview you? [CVI professional], can we hang out with you? [CVI professional], what are your. . .?” It’s always secondhand. It’s always “I have to be far removed from you to be able to validate what you’re doing or saying”. I mean they’re not telling me that, but they’re also not where I’m at. You know? And so, I often wonder if they were, would they really understand how their policies really affect us or don’t? And how do you measure that? How can or do you measure that when you make that policy? . . . Like, who are you inviting to help you create these policies? Do you really have young people at your table? Do you really have people who survive been violence? Do you really have like, or is it just the data? And the research that you’re saying, oh, this I need, we should do this. And how can I care for it when I don’t know about it? Like they do. How can I help people care about it when they’re also not the direct folks who are impacted by community violence, are not being invited to those conversations.—Sacramento professional
For some CVPS, their dedication to policy advocacy stemmed from perceived limitations in what they alone can do to prevent community violence and homicide, when the underlying causes are largely out of their direct control. For example, one participant acknowledged the role, and lack of concern, of the firearms industry and other systems of power in facilitating increased availability of firearms in their city, which was seen as a major driver of violence; yet the CVPS still remained committed to taking action within their sphere of influence: But the root causes about guns, about drugs, we don’t have that power. And the people that do, it’s more lucrative to them. Like, they care more about the money than they do about lives. The NRA, they got so much power. People funding them and they, they just not gonna go away. . .so, we can’t attack how to get the guns or the fact they get them, but we can go in there thinking, right? So that’s what we gotta do. We can’t get to the cause of it, ‘cause it’s so high up. But we can deal with who we got right here, right? And that, and that’s my thing.—Baltimore professional
To significantly reduce homicide and community violence, CVPS called for an urgent, coordinated public health response, equivalent to what has been seen for mass shootings in schools and the COVID-19 pandemic.
What we need is, you know when Columbine got shot up, they brought every resource they could, and they brought psychiatrists in, psychologists in, social workers in. They brought everything in to address the mindset of these people. We need the same thing in our community. We need the same thing in our area. This is a pandemic. This is a[n] epidemic. Whatever ‘demic you wanna call it, trust me, we suffer from all of that. So that’s the kinda stuff we need. This is a serious, a serious situation requires a serious response. So, we gotta treat it as such. . . When COVID hit, they had every scientist all over the world come together to come up with a cure, to address it. And look where we at now. Even Bill Gates had the nerve to say, “Man, shut it all down for three or four years. Economic, yeah, we may suffer. But we can rebuild that. But the lives we gonna lose, that we can’t get back.” It’s the same with this violence.—Baltimore professional
Discussion
Listen to the voices of those who are being violently injured, be realistic and really hear what they’re needing. Not the cookie cutter version or not the version of what we think they may need, but really hear what they need to be successful to recover and to prevent this from happening again. . . And also speaking their language, to hear what they come from, what they experience, and what they need. Just their voices, that’s it. That’s what I would say, policymakers should really listen to their voices, not imagine what they need, but really hear what’s going on in their world.—Sacramento professional
Centering the experiential wisdom of those closest to violence helps ensure that knowledge creation and intervention strategies are informed by on-the-ground realities (Buggs et al., 2023). However, the voices of CVPS and those directly impacted by violence are often marginalized in academic studies of and discussions about violence prevention and intervention strategies. Indeed, a scoping review (Ziminski & Baker, 2024) of existing research on firearm-focused community violence intervention and prevention initiatives found that few studies used community-engaged methods. Though some studies exist (e.g., Frattaroli et al., 2010; Woods-Jaeger et al., 2023), such a general oversight can perpetuate a justified, historically grounded distrust within impacted communities where research is conducted on them rather than with them or for them (Dhaliwal et al., 2020). Further, given the complexity of researching a social phenomenon like violence, with often fluid and rapidly changing contexts, actors, motivations, and residual impacts, researchers aiming to understand violence would benefit from incorporating qualitative or mixed methods approaches to uncover valuable insights into the nuances of community dynamics and perceptions of safety.
Grounded in this understanding, the current study uplifts the perspectives of professionals on the frontlines of community violence prevention and intervention, setting forth a multi-tiered argument for their authority as knowledge experts and solutions-generators. Findings enhance our understanding of the pivotal role of CVI in the immediate and long-term aftermath of homicide, as well as the needs of communities continuously healing from harm and of the CVI professionals that serve them.
CVPS, as the backbone of CVI, are uniquely well positioned to address both proximal and structural drivers of homicide (Buggs, Dawson, & Ivey, 2022). CVPS are connected to homicide in multiple ways including personally—through their past experiences and deep connection to places impacted by violence—and professionally—through their response in the aftermath of homicide and continued engagement with communities impacted. Their effectiveness is rooted in their shared experiences and nuanced understanding of decisions facing individuals choosing whether or not to engage in violence, as well as their deep embeddedness and commitment to the places and people they serve (Buggs, 2022; Dawson et al., 2023).
In service of their communities, CVI professionals undertake multifaceted roles, often at great personal risk, yet face inadequate support systems. As a function of their high-risk jobs, and through their past lived experiences, CVPS in this study described multi-level trauma exposure, aligning with other studies of CVPS (Free & MacDonald, 2022; Hureau, Wilson, Jackl, et al., 2022; Hureau, Wilson, Rivera-Cuadrado, et al., 2022). Further, their closeness and connection to the work and to their clients, though an invaluable asset, also presents potential challenges and risks to their wellbeing and healing (Bocanegra & Aguilar, 2024). To address these challenges, policymakers, program managers, and local leaders must prioritize the economic and mental well-being of CVPS. This includes providing comprehensive mental health services, appropriate financial compensation to acknowledge dangers and offset associated risks, and ongoing training and professional development opportunities (Bocanegra & Buggs, 2024).
Throughout this study and others (Bocanegra & Aguilar, 2024; Buggs, Webster, & Crifasi, 2022; Goodwin & Grayson, 2020; Ross et al., 2023), individuals directly impacted by homicide shared invaluable insight into the causes, consequences, and solutions to community violence. Aligning with prior research, the CVPS in this project identified and articulated the risks of their job and the burden of trauma associated with their work (Hureau, Wilson, Jackl, et al., 2022; Hureau, Wilson, Rivera-Cuadrado, et al., 2022), the complex pathways intersecting community trauma and violence reproduction (Buggs, Kravitz-Wirtz, & Lund, 2022; Pinderhughes et al., 2015), the structural harms plaguing their communities and driving violence (Buggs et al., 2023; Poulson et al., 2021), and the immense resilience and wisdom of communities impacted by violence (Hunter & Robinson, 2016; Reese, 2018). They went on to provide concrete suggestions for supports, strategies, and interventions to promote safety and healing for themselves and their communities, which should be uplifted in public narratives, prioritized in policymaking processes, and explored in greater depth in future research. Yet, realizing sustained investment in CVI and ensuring meaningful engagement of CVPS in structural decision-making requires a paradigm shift in public safety narratives.
Despite increasing acknowledgment and advocacy for holistic, community-centered interventions addressing the underlying drivers of violence (Dunivin et al., 2022; Kass & Rocco, 2024), CVPS and the organizations that employ them still face substantial hurdles in securing funding and defending their credibility (Bocanegra & Buggs, 2024). They are often undervalued, underpaid, and underappreciated compared to traditional safety systems like law enforcement and emergency medical services (EMS). Like EMS responders, CVI professionals are often confronted with high-stakes situations where they must make quick decisions to promote health, yet they are not afforded the same flexibility and confidence in their day-to-day operations. This stands in stark contrast to the unwavering support granted to police, whose budgets remain largely unchanged and credibility relatively unchallenged even amid concerns about their effectiveness and evidence of their harm (Friedman, 2022; Kass & Rocco, 2024; Norris, 2021). To better understand the barriers and opportunities for CVPS to become more integral and congruent parts of the public safety solution in cities where they operate, future research should investigate the perspectives of relevant stakeholders with decision-making power, including policymakers, criminal legal system professionals, victim services, and reentry programs. Such research could provide valuable insights into how to enhance the role of CVPS and ensure their contributions are fully recognized and utilized.
The constant need for CVPS to justify their value and actions with little flexibility or support is not only potentially dangerous for the communities they serve but also undermines the heroic work they undertake, which should be recognized as a crucial component of public safety and public health. While financial compensation is just one measure of value, in our capitalist system it signifies a collective recognition of inherent necessity and worth. As one CVI professional in Milwaukee recounted, a community member they tried to recruit to their program replied: “It’s not worth y’all life and worth what they paying y’all. You know, what they paying y’all is not worth your life to do this job.”
Integrating CVI into the fabric of public safety and health systems is pivotal for nurturing safety and healing in communities disproportionately impacted by homicide. Doing so may require a profound reevaluation of our collective understanding of violence, broadening it to encompass structural violence (Buggs et al., 2023), and of safety, extending it to include freedom from structural violence and trauma as well as secure access to food, housing, education, and employment (Norris, 2021). Additionally, this integration calls for a reimagination of public protection, prompting reflection on the elements of broadly defined safety that governments should be obligated to invest in (Friedman, 2022) and a critical evaluation of who public systems protect, recognizing the need to prioritize healing promotion in overly criminalized areas and for formerly incarcerated individuals, including many CVPS. With such a paradigm shift, the multi-faceted role of CVI not only in providing physical safety in a healing centered way but also in addressing many other aspects of safety typically overlooked in punitive approaches, is unequivocally a collective good, a public safety necessity, and an invaluable investment in public health.
I think they declare violence as a, um, what you say? Violence as a public health crisis. Well, if it’s a public health crisis, that means that this is healthcare. And so, because this is a healthcare profession, then, you know, this is a healthcare issue. Then at some point then we need to get paid as healthcare professionals, you know, that go into the neighborhood and do the care, the healthcare of our neighborhoods, you know.—Milwaukee professional
Strengths and Limitations
The field of community violence intervention and prevention is evolving and expanding, which is reflected in the range of voices captured in this study. While the authors are aware of no other study to-date that has interviewed CVPS across program models and across cities to gather aggregate-level data, given limitations consistent with qualitative research, this work may not capture in totality the views and perspectives of all CVPS in the field.
Further, this paper contributes a novel multi-city examination of the role of CVI in the aftermath of homicide. Yet, given that the original research protocol did not specifically center homicide and its aftermath, it is notable that participants’ perspectives on homicide and their engagement with pertinent forces in its wake may not be entirely captured in the data. To fully appreciate the complex experiences and lives of homicide victims and their families, this work should be absorbed in concert with other qualitative studies that advance these narratives.
Lastly, as each author is imbued with their own set of biases and assumptions that can color the qualitative research process from data collection to data analysis, subjectivity was a prioritized consideration. All authors contributed a positionality statement describing how their intersectional identities coupled with their subject-matter expertise and inherent privileges informed their interpretations of participants’ responses and consequently, their key takeaways from the data. Additionally, while we did not calculate interrater reliability, the coding strategy employed multiple primary coders per transcript and final oversight from the senior author. Although the research team was intentional in their approach to assuage subjectivity concerns, some bias is inherent in qualitative research and further supports the recommendation to consider this work in tandem with other empirical pieces centering homicide, its victims and the critical and structural approaches needed to mitigate systemic community-based harm.
Conclusion
Community-based violence intervention and prevention programs serve as a valuable mitigation tool in the ongoing violent conflicts that encapsulate divested communities across the nation. CVPS emerged as critical actors for intervening in the community after a homicide occurs. Their insights in focus groups and interviews illuminated how uniquely positioned CVPS are, personally and professionally, and how this proximity allows them to leverage their expertise to navigate the myriad factors that emerge in the wake of a homicide. Their personal and professional proximity to homicide, coupled with their trauma-informed approaches, and firsthand knowledge of the structural challenges facing CVI implementation, situates CVPS as strategic responders to homicide and field experts in identifying community needs, providing recommendations, and contributing to policy development for redress in the aftermath of homicide. Community violence, and firearm homicide more specifically, continues to be a significant public health and safety concern, particularly for Black and Brown youth. As more federal dollars are directed toward community violence intervention and prevention strategies, it is vital for pertinent field research to critically examine the specialized role of violence intervention and prevention specialists.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was supported by The Joyce Foundation, the California Wellness Foundation, and the Violence Prevention Research Program at the University of California, Davis.