
Abstract
Witnessing violence and injury in research can elicit affective and cognitive reactions. It is imperative that research teams develop trauma-responsive interventions, but little is known about their effectiveness. A convenience sample of violence and injury scholars (n = 64) was recruited through listservs and social media. Scholars answered an online survey about their experience managing research teams and the perceived effectiveness of interventions. Strategies and their perceived effectiveness were described, and a linear regression indicated factors associated with the number of strategies used. Qualitative responses were analyzed using content analysis. This study found that supervisors used a variety of intervention techniques. Most methods were perceived as moderately effective, while requiring time off and having a team member dedicated to well-being programing were rated as highly effective. Qualitative data indicated that to be effective, these strategies needed to be paired with genuine, expressed care for supervisees’ well-being and behavior modeling. The number of strategies used was influenced by supervision experience and one’s belief that researchers could be impacted by trauma exposure. This study indicated that researchers need a variety of strategies to intervene in vicarious trauma. More experimental research is needed to test the long-term effectiveness of such interventions.
Introduction
Researchers who examine injury and violence are exposed to traumatic materials in their work through data collection and analysis. This exposure, known as vicarious trauma, can lead to changes in an individual’s cognitive schema, behaviors, and affect (Molnar et al., 2017). These changes, natural empathic responses to traumatic stimuli, can be negative, called vicarious traumatization, or positive, called vicarious resilience (Cohen & Collens, 2013; Engstrom et al., 2008; McCann & Pearlman, 1990). In addition to the potential negative personal impact on an individual, traumatization can limit one’s ability to effectively perform research tasks and cause individuals to prematurely leave research teams, potentially decreasing the sustainability and accuracy of research (Cummings et al., 2021; Miller Reed et al., 2023; Regehr et al., 2002). Studies on frontline practitioners (e.g., social workers, victim advocates, fire and emergency medical services, police, medical staff) have shown that there are organizational-level interventions that promote resiliency and prevent traumatization, such as training on vicarious trauma (Ben-Porat, 2015; Douglas, 2013b; Habeger et al., 2022) and regular supervision (Bell, 2003; Cohen & Collens, 2013; Ting et al., 2006). Such interventions could be easily translated to research teams; yet there is comparatively little empirical work on how research teams manage traumatic exposure in their scholarship, nor whether such means are effective.
Theoretical Orientation: Vicarious Traumatization and Resilience
Vicarious traumatization was first conceptualized in the 1990s by McCann and Pearlman, two psychologists working with survivors of sexual and domestic violence. A cognitive theory, vicarious traumatization investigates how traumatic exposure changes how one understands their world (i.e., cognitive schema) and the related affective, behavioral, and psychological changes (McCann & Pearlman, 1990). Even when professionals are not exposed directly to violence and trauma, McCann and Pearlman (1990) found that by listening to and accompanying those who directly experience it, workers experience the same impacts. Attending to these psychological safety risks is critical, as the human brain reads psychological danger similarly to physical danger; meaning that psychological trauma can also lead to mental health issues like post-traumatic stress disorder (American Psychiatric Association, 2022; Herman, 2015). McCann and Pearlman (1990) identified seven schemas specific to sexual and domestic violence that may be affected by exposure: feeling safe, believing others are inherently good, feeling in control, feeling independent, trusting others and one’s environment, feeling connected to others, and believing that experiences have meaning. When one of these schemas is disrupted, one may, for example, become obsessed with perpetrators of violence being punished or feel stigmatized by their work (McCann & Pearlman, 1990). In other fields similar schema (e.g., a homicide researcher feeling unsafe in a neighborhood) or different schema (e.g., a child welfare worker’s understanding of family) may be affected by their unique exposures. This secondary exposure can also lead to memory disruptions, like dissociation or memory blanks, affective responses like sadness, and behavioral changes like social isolation or substance use (McCann & Pearlman, 1990). When a worker becomes overwhelmed with this traumatic exposure, it can lead to burnout, or the inability to process what one is experiencing, which can make one feel numb, cynical, and ineffective (Maslach et al., 2001; McCann & Pearlman, 1990).
More recently, researchers have also studied the positive impact of working with individuals experiencing trauma, or vicarious resilience. Among frontline workers, vicarious resilience is conceptualized as when working with clients “motivates [workers] to continue their service” (Barrington & Shakespeare-Finch, 2013, p. 18). Workers experiencing vicarious resilience report feeling grateful for their work, feeling in awe of the fortitude of the human spirit, feeling proud of their own strength and of their work, and engaging in meaning making and personal growth (Barrington & Shakespeare-Finch, 2013; Cohen & Collens, 2013; Engstrom et al., 2008; Pack, 2014). Together, vicarious resilience and traumatization describe potential impacts of vicarious trauma (Molnar et al., 2017). Vicarious resilience and traumatization are parallel processes, and many scholars call for the study of both constructs simultaneously in order to best understand the complex impact of trauma exposure and to better inform intervention development (Barrington & Shakespeare-Finch, 2013; Cohen & Collens, 2013; Engstrom et al., 2008; Frey et al., 2017). Importantly, research indicates that the promotion of resiliency and prevention of traumatization are not individual worker responsibilities, but that organizational policies can limit the negative impacts of working with traumatized populations and maximize the positive effects (Cohen & Collens, 2013; Frey et al., 2017; Molnar et al., 2017; Regehr et al., 2002). For example, the U.S. Office for Victims of Crime (2018) created a toolkit grounded in vicarious traumatization and resilience (Molnar et al., 2017) for organizations to review their existing policies and procedures and identify areas for improvement, like including staff in funding decisions and having clear policies for time off. These theories underline that exposure to trauma impacts all workers in positive and negative ways, and that far from being the responsibility of the individual to manage this exposure, organizational-level strategies can be adopted to promote resiliency and prevent traumatization.
Vicarious Trauma and Research Teams
Across disciplines, there have been calls to attend to vicarious traumatization risk to researchers, including in environmental studies (Pihkala, 2020), social science (Fenge et al., 2019; Miller Reed et al., 2023), political science (Loyle & Simoni, 2017), nursing (Butler et al., 2017), child welfare research (Coles & Mudaly, 2010), homicide and violence research (AbiNader et al., 2023; Cullen et al., 2021), and public health research (Dickson-Swift et al., 2008). Some particularly emphasize the risk of traumatization for qualitative researchers due to their immersion into others’ lives and their direct interactions with research participants (Butler et al., 2017; Coles & Mudaly, 2010; Dickson-Swift et al., 2008; Wallace & County, 2024), although existing research has also examined the impact of secondary data analysis of potentially graphic data, such as law enforcement casefiles (AbiNader et al., 2023). While many codes and guidelines exist regarding the protection of human subjects, codified guidance on protecting researchers is limited, particularly for psychological safety risks. Two non-profit agencies have issued guidance for researchers to adopt for their own practice, but, to the author’s knowledge, these have not been formally adopted by any university or governing body. The United Kingdom’s Social Research Association (2001) developed a “code of practice” regarding the, primarily physical, safety of social scientists collecting field data, and the global Sexual Violence Research Initiative developed guidelines for gender-based violence researchers attending to both psychological and physical safety risks (Billings et al., 2015).
Qualitative studies of researchers have indicated that they experience many of the same impacts from trauma exposure as frontline workers. Like frontline workers (Aldrich & Kallivayalil, 2013; Bell, 2003; McCann & Pearlman, 1990), researchers report secondary traumatic stress symptoms like hypervigilance, dissociation, and numbing (AbiNader et al., 2023; Dickson-Swift et al., 2008; Miller Reed et al., 2023; Wallace & County, 2024). They have also reported impacts to cognition as described by McCann and Pearlman (1990): intrusive memories, such as nightmares, and changes to their cognitive schema (AbiNader et al., 2023; Dickson-Swift et al., 2008; Miller Reed et al., 2023). For example, researchers have reported that they became less trusting in others, found it challenging to make sense of the world given what they studied, and felt isolated from others (AbiNader et al., 2023; Miller Reed et al., 2023). Similar to practitioners (Cohen & Collens, 2013; Regehr et al., 2002; Ting et al., 2006), researchers have reported experiencing a range of affective responses including sadness, anger, fear, hopelessness, and confusion (AbiNader et al., 2023; Dickson-Swift et al., 2008; Miller Reed et al., 2023; Wallace & County, 2024). A qualitative study of public health researchers reported that scholars felt guilty for and were troubled by the discordance of asking participants to share traumatic parts of their lives while feeling excited to collect data (Dickson-Swift et al., 2007). Researchers have also reported a sense of weighty responsibility to accurately represent the stories of their research participants and to lift up their voices (Dickson-Swift et al., 2007; Miller Reed et al., 2023). Taken together, the distressing impacts of trauma exposure through scholarship can make trauma-focused research agendas difficult to sustain over time (AbiNader et al., 2023; Miller Reed et al., 2023). Much less is known about the vicarious resilience responses experienced by researchers. In one qualitative study, public health researchers reported feeling honored by the trust of their research participants (Dickson-Swift et al., 2007).
Research that has examined predictors of vicarious traumatization and resilience among scholars mirrors the predictors found among frontline workers. Among frontline workers and researchers, increased hours of exposure to traumatic materials through client or participant stories have been shown to increase feelings of burnout and secondary traumatic stress symptoms (AbiNader et al., 2023; Baird & Jenkins, 2003; Bemiller & Williams, 2011; Brady & Hayes, 2018; Miller Reed et al., 2023). A lack of preparation for how to do the work and to manage the exposure to traumatic materials is associated with an increase in traumatic impact among researchers (Dickson-Swift et al., 2008; Fenge et al., 2019; Miller Reed et al., 2023) and frontline workers (Berger & Gelkopf, 2011; Douglas, 2013a; Vrklevski & Franklin, 2008). Like research on frontline workers (Benuto et al., 2018; Frey et al., 2017; Ghahramanlou & Brodbeck, 2000), the qualitative evidence on researchers is mixed about whether having a personal trauma history is protective against or magnifies vicarious traumatization (AbiNader et al., 2023; Miller Reed et al., 2023). Researchers with prior clinical experience have reported distress related to challenges in turning off their clinical instincts and switching to a more neutral, hands-off research approach, and in the lack of guidance on how, why, and when to do this (Dickson-Swift et al., 2008; Fenge et al., 2019).
Vicarious Trauma Interventions
Two of the most salient organizational-level interventions identified in the literature on vicarious trauma among frontline workers are training (AbiNader et al., 2020; Ben-Porat, 2015; Brady & Hayes, 2018; Cohen & Collens, 2013; Douglas, 2013a; Ghahramanlou & Brodbeck, 2000; Habeger et al., 2022; Kim et al., 2022; Maslach et al., 2001; Molnar et al., 2017) and social support (AbiNader et al., 2020; Barrington & Shakespeare-Finch, 2013; Bell, 2003; Cohen & Collens, 2013; Frey et al., 2017; Ghahramanlou & Brodbeck, 2000; Habeger et al., 2022; Kim et al., 2022; McCann & Pearlman, 1990; Ting et al., 2006). Unsurprisingly, qualitative research on scholars and agency guidance have promoted both strategies. For researchers, past scholarship indicates that early-career training needs to expand beyond analysis and research design to include training on traumatic impact for the researcher and on clinical skills for working with research participants who have experienced trauma (AbiNader et al., 2023; Billings et al., 2015; Dickson-Swift et al., 2008; Fenge et al., 2019; Miller Reed et al., 2023; Social Research Association, 2001). In terms of social support, past qualitative research indicates that team science, regular check-ins with supervisors or peers, formal mentoring for early-career researchers, and debriefing promote well-being (AbiNader et al., 2023; Billings et al., 2015; Dickson-Swift et al., 2008; Miller Reed et al., 2023; Social Research Association, 2001; Wallace & County, 2024). Some studies suggested that therapy was a potential avenue of intervention, but noted that seeking professional help is often considered taboo, as researchers are supposed to be neutral and unaffected by their work (Dickson-Swift et al., 2008; Miller Reed et al., 2023; Wallace & County, 2024; Women’s Aid, 2020). As has been shown in research with frontline workers (Babin et al., 2012; Cummings et al., 2021; Frey et al., 2017; Tham, 2006), it is not sufficient to merely have opportunities to connect with others; the interactions must feel positive, authentic, and supportive to combat traumatization and increase resiliency (AbiNader et al., 2023; Dickson-Swift et al., 2008; Miller Reed et al., 2023).
Past research additionally calls for clear and specific policies that support well-being (Maslach et al., 2001; Molnar et al., 2017). Some have noted that as employees of institutions, researchers are entitled to safety protections under national organizational health and safety regulations, which could include policies that attend to the psychological and physical risks of trauma research (Billings et al., 2015; Dickson-Swift et al., 2008; Social Research Association, 2001). These could include clear guidelines around physical safety during in-person data collection, like requiring data collection to be done in pairs (Billings et al., 2015; Social Research Association, 2001), and psychological safety measures, such as policies on work hours that allow for flexible schedules so that researchers can pace their exposure to the material (AbiNader et al., 2023; Billings et al., 2015; Social Research Association, 2001). Past work has also indicated that policies that allow researchers to cease their exposure to the traumatic materials, by taking extended breaks or quitting, are also of potential import (AbiNader et al., 2023; Billings et al., 2015; Miller Reed et al., 2023; Social Research Association, 2001). More research is needed to evaluate the effectiveness of interventions to promote resiliency and decrease traumatization used with research teams.
Current Study
As an initial step toward meeting this gap, this mixed-methods study surveyed injury and violence research supervisors recruited through listservs and social media. The study aimed to identify specific strategies used to promote resiliency and prevent traumatization, and the participants’ perception of the effectiveness of these strategies. Managing trauma-informed research teams that minimize risk to both participants and researchers is critical to conducting ethical, sustainable, and quality studies on violence and injury.
Methods
Approach
A convergent parallel mixed-methods design was used to assess researchers’ perspectives on managing research teams conducting violence and injury research, an understudied area of scholarship (Creswell & Creswell, 2017). The participants answered a quantitative survey that assessed their experience, their use of management methods identified in the existing literature for frontline workers, and their perception of strategy effectiveness. They also answered open-ended questions that allowed them to describe their approach and offer insight into managing a violence and injury research team. The results were then analyzed and interpreted in tandem, allowing the qualitative data to enrich and contextualize the quantitative data (Creswell & Creswell, 2017; Tashakkori & Teddlie, 1998).
Sampling
A convenience sample of self-identified violence and injury scholars was recruited through multiple strategies. Recruitment flyers were posted on X (i.e., Twitter) twice per week for 1 month in Spring 2024. The reasons for using X were twofold: first, at the time, it was a primary tool for academic dissemination (i.e., “academic twitter”), and second, it was the social media platform available to the research team (Klar et al., 2020; Taylor & Francis Author Services, 2025). Recruitment emails were sent to listservs of research societies for injury scholars, CDC-funded injury science centers, and university-based gun violence research centers in the United States that were identified through Google searches and targeted due to their large concentration of injury scholars. Scholars were recruited to answer a 5 to 10-min Qualtrics survey to share their experience of managing research teams. To be eligible for the survey, participants had to study violence and/or injury, have supervised at least one other researcher (including students, research assistants, research staff, and co-investigators), be over 18 years of age, be able to consent to research, be non-institutionalized, and speak English. All recruitment strategies and the research design were approved by the University of Pennsylvania Institutional Review Board. Seventy survey responses were recorded by Qualtrics; three responses were dropped because Qualtrics labeled them as bots (Qualtrics XM, 2024), and three responses were dropped due to non-completion (missing values for >90% of the questions). The final sample included 64 researchers.
Researcher Characteristics and Attitudes
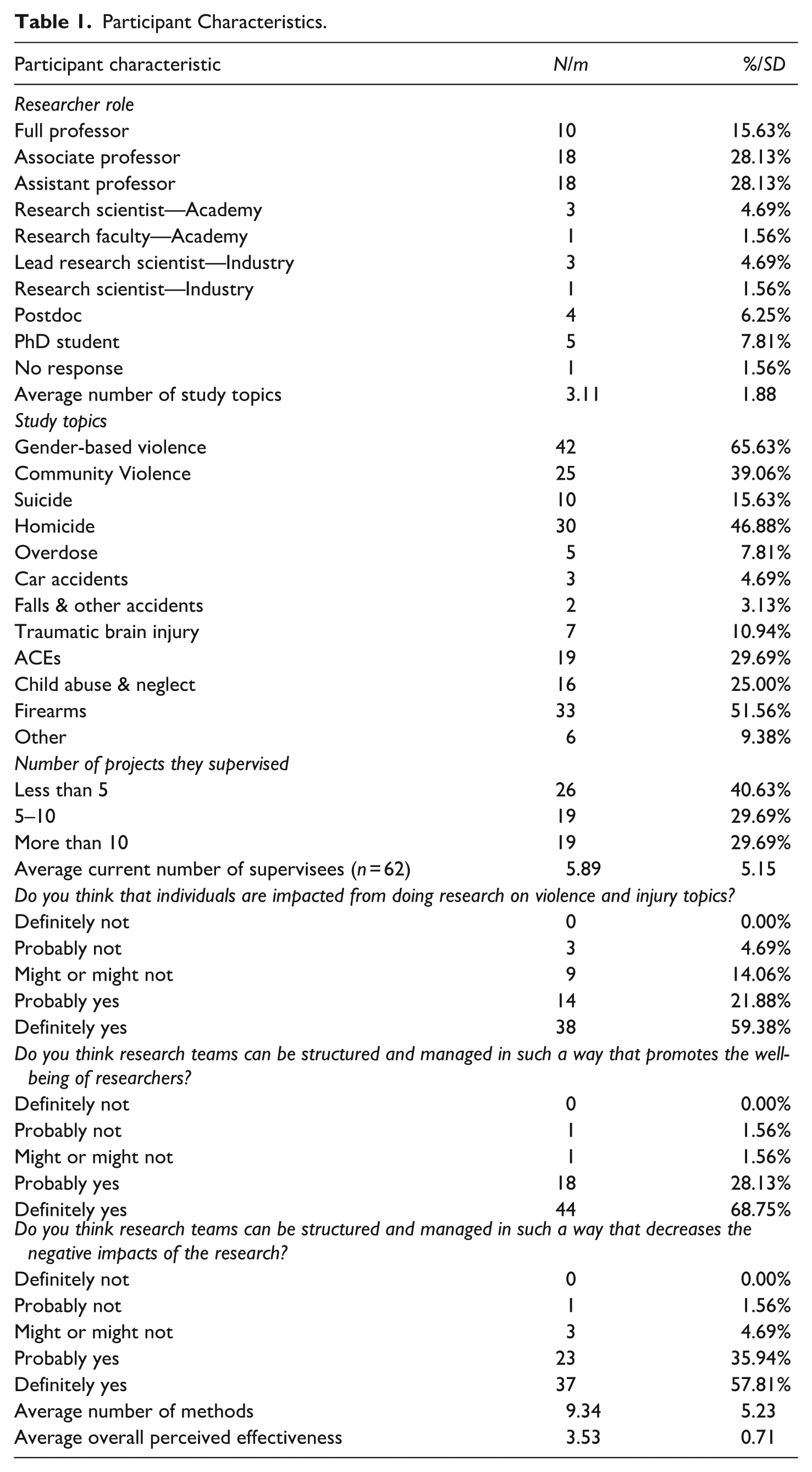
The researchers’ roles, topics of study, total number of projects where they’ve supervised others, and their current number of supervisees were recorded (variable levels presented in Table 1). For later analyses, researcher role was condensed into five categories: senior and mid-career academics, early-career academics, academic research scientists, industry scientists, and trainees. The number of study topics was summed for each participant, creating a continuous variable indicating researchers with more specialist (one topic) and generalist (11 topics) interests. Participant attitudes toward vicarious traumatization and resilience were assessed on a 5-point Likert scale from “definitely not” to “definitely yes.” Specifically, participants were asked: “Do you think that individuals are impacted from doing research on violence and injury topics?”, “Do you think research teams can be structured and managed in such a way that promotes the well-being of researchers?”, and “Do you think research teams can be structured and managed in such a way that decreases the negative impacts of the research?”. For later analyses, the attitude Likert scales were reduced to dichotomous variables: yes, no/maybe.
Participant Characteristics.
Management Strategies and Their Perceived Effectiveness
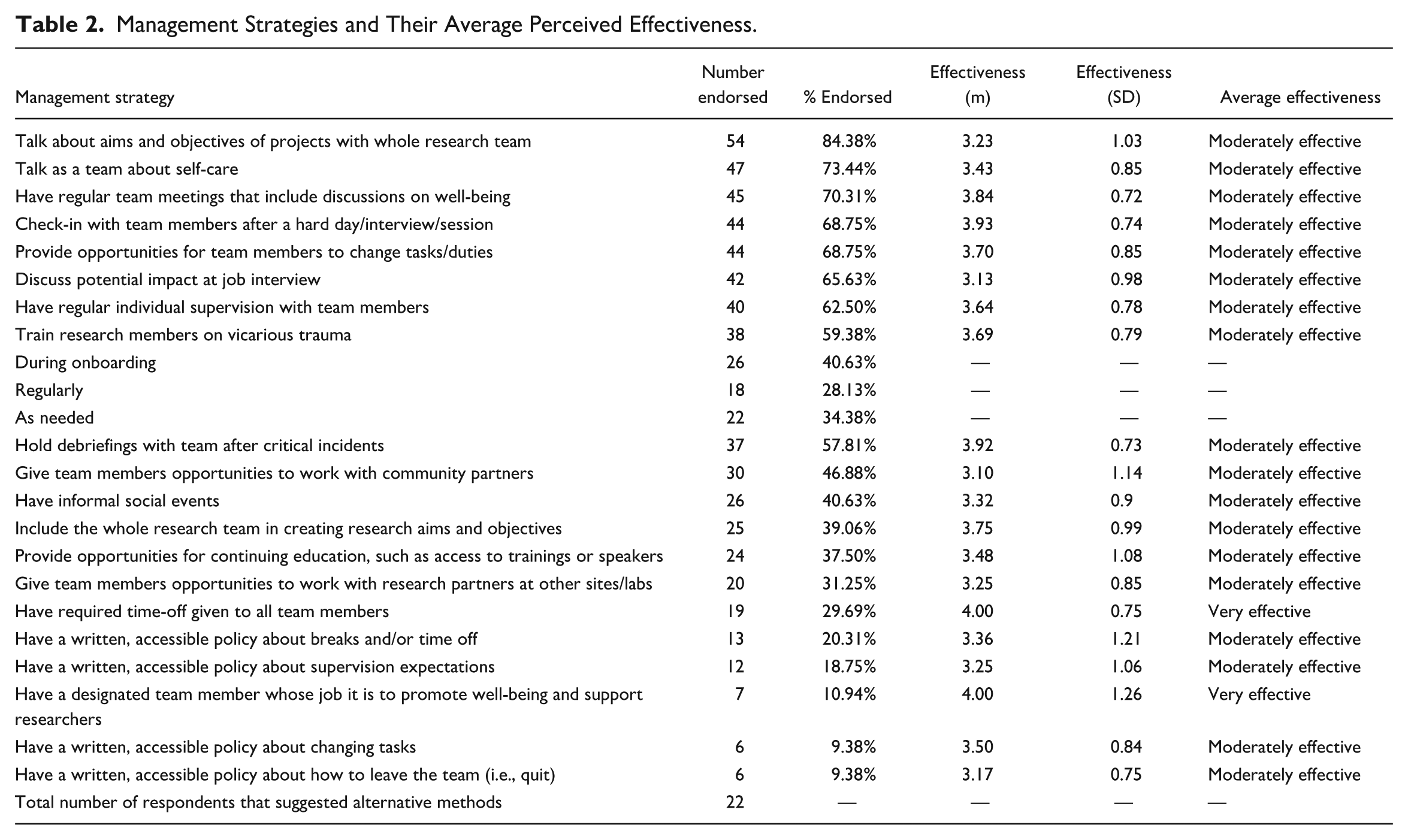
To develop the survey instrument, exisiting literature on vicarious trauma was reviewed to identify effective organizational interventions used in practice- and research-based settings. This literature review yielded a list of 20 strategies for managing traumatic exposure (strategies listed in Table 2). Participants were asked to select strategies from this list that they had used and to enter up to five additional strategies used. For each strategy endorsed, the participant was then asked to indicate how effective they perceived that method on a five-point Likert scale ranging from “not effective at all” to “extremely effective.” The average perceived effectiveness rating per method was also calculated. Finally, an open-text box allowed participants to share any final thoughts about managing research teams exposed to traumatic material.
Management Strategies and Their Average Perceived Effectiveness.
Data Analysis
Descriptive statistics were run to describe the distribution of all study variables. To describe factors associated with the number of management methods used, a linear regression was performed. Prior to regression, multiple imputation was used to estimate missing values in the variables researcher role (n = 1) and the participants’ current number of supervisees (n = 2). Five imputed datasets were generated using Stata 18’s “mi impute chained” command, as about 5% of cases had missing data (White et al., 2011). Pooled estimates were calculated using the “mi estimate” command. The results from the regression analysis using multiple imputation were similar in magnitude and direction to those using listwise deletion. The imputed results are described here. Qualitative results were analyzed using conventional content analysis, identifying themes in the qualitative questions about additional tools and other concerns (Hsieh & Shannon, 2005). This approach allows the researcher to use answers to open-ended questions to describe a phenomenon without a priori assumptions (Hsieh & Shannon, 2005). Open-text responses to additional strategies used and the final open-text field were analyzed together, as some responses to “other method” included commentary, and some responses to the final qualitative question included additional strategies. Twenty-six participants provided qualitative answers, seven responded to both qualitative questions, seven to alternative strategy questions only, and 12 to the open-text question only. Quotes are used to add depth and trustworthiness to the results (Creswell, 2013); speakers are indicated by a randomly assigned identifier 1 to 64.
Results
Research Characteristics
Characteristics of the participants are displayed in Table 1. A majority of the sample were senior or mid-career academics. Researcher-participants studied between 1 and 11 topics, with an average number of study topics of 3.11. The most frequently studied topics were gender-based violence (intimate partner violence, sexual violence, and stalking), homicide, and firearms. On average, participants currently supervised about six individuals, and 40.63% of the sample had supervised individuals on fewer than five projects. On average, researcher-participants used 9.34 management strategies and perceived them to be moderately effective.
Management Strategies and Their Perceived Effectiveness
Table 2 presents the distribution of management strategies used and the average perceived effectiveness of each strategy. Perceived effectiveness was rated on a five-point Likert scale from 1, not effective at all, to 5, extremely effective. The majority of strategies were perceived as moderately effective; a finding that was further emphasized in the qualitative data (qualitative results are presented in Table 3). Eight respondents noted that the perceived effectiveness of these strategies was context-dependent, varying based on the supervisee characteristic (e.g., an undergraduate) or the data characteristics (e.g., survivor stories). Others also emphasized that no single strategy alone was sufficient: “I think none of these strategies alone are more than moderately effective. It’s using these strategies simultaneously that is most helpful & creates a trauma-informed culture in the lab,” (Participant 5). Thus, using multiple strategies seemed to create a structural environment, or “culture,” that promoted well-being and prevented traumatization.
Themes From Qualitative Analysis (n = 26).
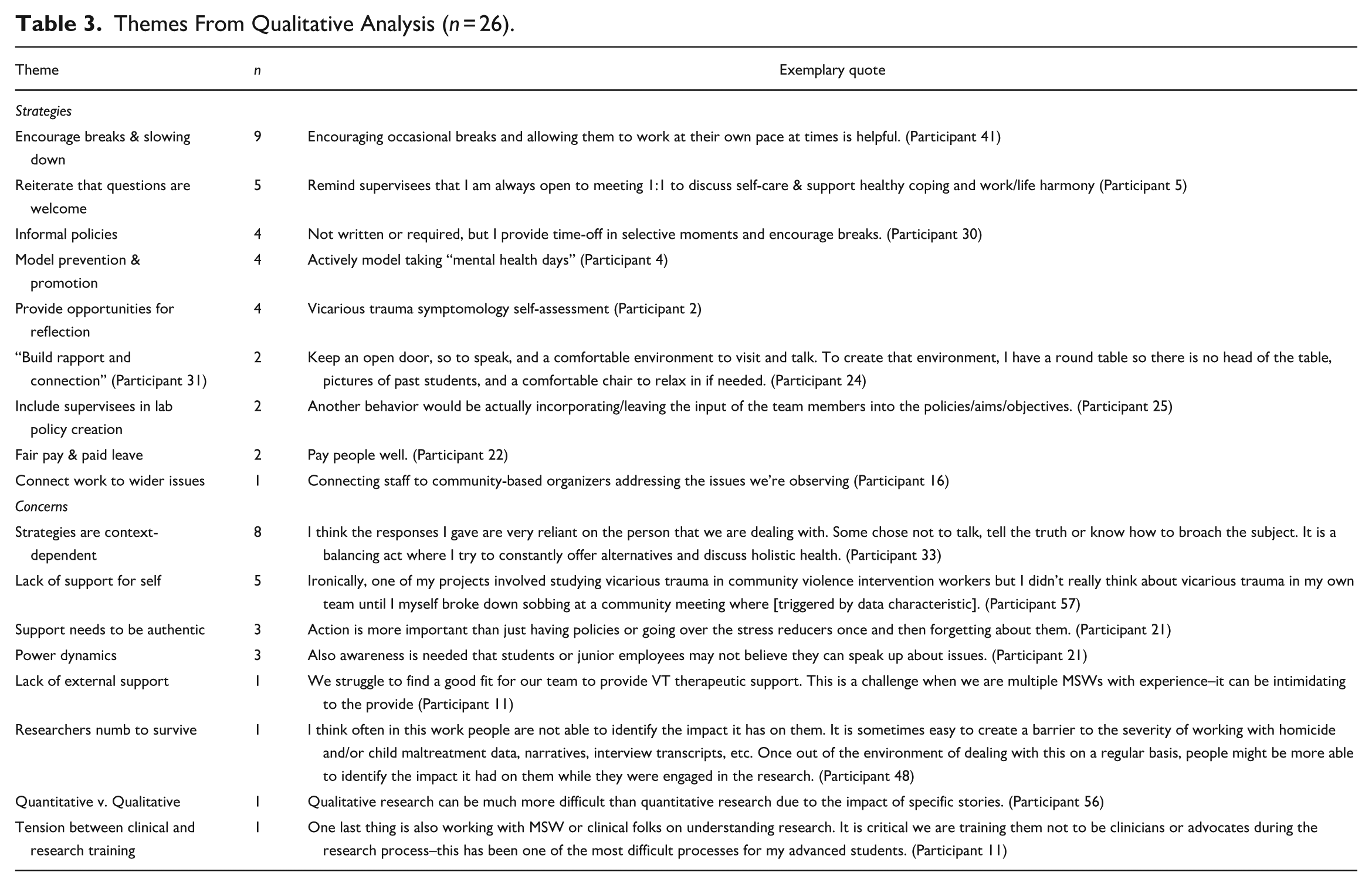
Two strategies were rated “very effective” on average: having a designated team member who looks after researcher well-being and required time off. Having a designated team member for was one of the least endorsed strategies (n = 7), but was highly rated by those who used it. Two participants further highlighted in qualitative responses that having a therapist available was critical to team well-being. The strategy of requiring time off was endorsed by 19 participants. Qualitative data re-emphasized taking breaks and time off (n = 9) as an effective strategy, with four participants indicating that these were informal or oral policies rather than formal, written ones.
Several others indicated that simply having the strategies or policies in place was insufficient—team leaders needed to cultivate an environment of support through “build[ing] rapport and connection” (Participant 31), modeling the behaviors, and proactively reminding supervisees about the opportunities in place or ensuring that they are used. Participant 25 explained, I think a major point is the behavior following these actions. For example, asking and discussing vicarious trauma and then labeling/“modeling” when that happens to you and normalizing taking time, engaging in self-care (e.g., modeling not responding to emails over break, etc.).
Three participants explicitly emphasized that the power dynamics between supervisor and supervisee made these extra steps beyond policy necessary; “encouragement is needed” (Participant 21) to emphasize that these strategies are not only available, but that supervisors really want supervisees to use them. Several widely endorsed strategies could contribute to creating a collegial environment, including talking with the team about self-care (n = 47), check-ins (n = 44), debriefings (n = 38), and informal social events (n = 26).
Five participants noted that while they had strategies for supporting supervisees, they lacked structural support for themselves. As Participant 11 stated: “As for me, I also need support. I carry the burden of caring for the team and worrying about the impact of the research, but do not have much of my own support.” Taken together, the quantitative and qualitative results indicated that participants used a variety of strategies to manage trauma exposure in research and that variability, flexibility, and consistency in strategies were needed to increase their perceived effectiveness.
Researcher Characteristics Associated With the Number of Strategies Used
Table 4 displays characteristics associated with the number of strategies one employs to manage trauma exposure on research teams. The linear regression found that the participants who indicated that they believed people were impacted by the work utilized 4.40 more strategies than those who were unsure or denied impact (p = .008). Researcher-participants who had supervised others on 5 to 10 projects used 3.21 more strategies than those who had supervised others on fewer than five projects (p = .032). There was no significant difference in the number of strategies used by those who had supervised more than 10 projects and those who supervised fewer than 5 projects, nor between those who had supervised more than 10 projects and those who supervised 5 to 10 projects (β = −1.10, p = .496).
Participant Characteristics and the Number of Management Strategies Employed.
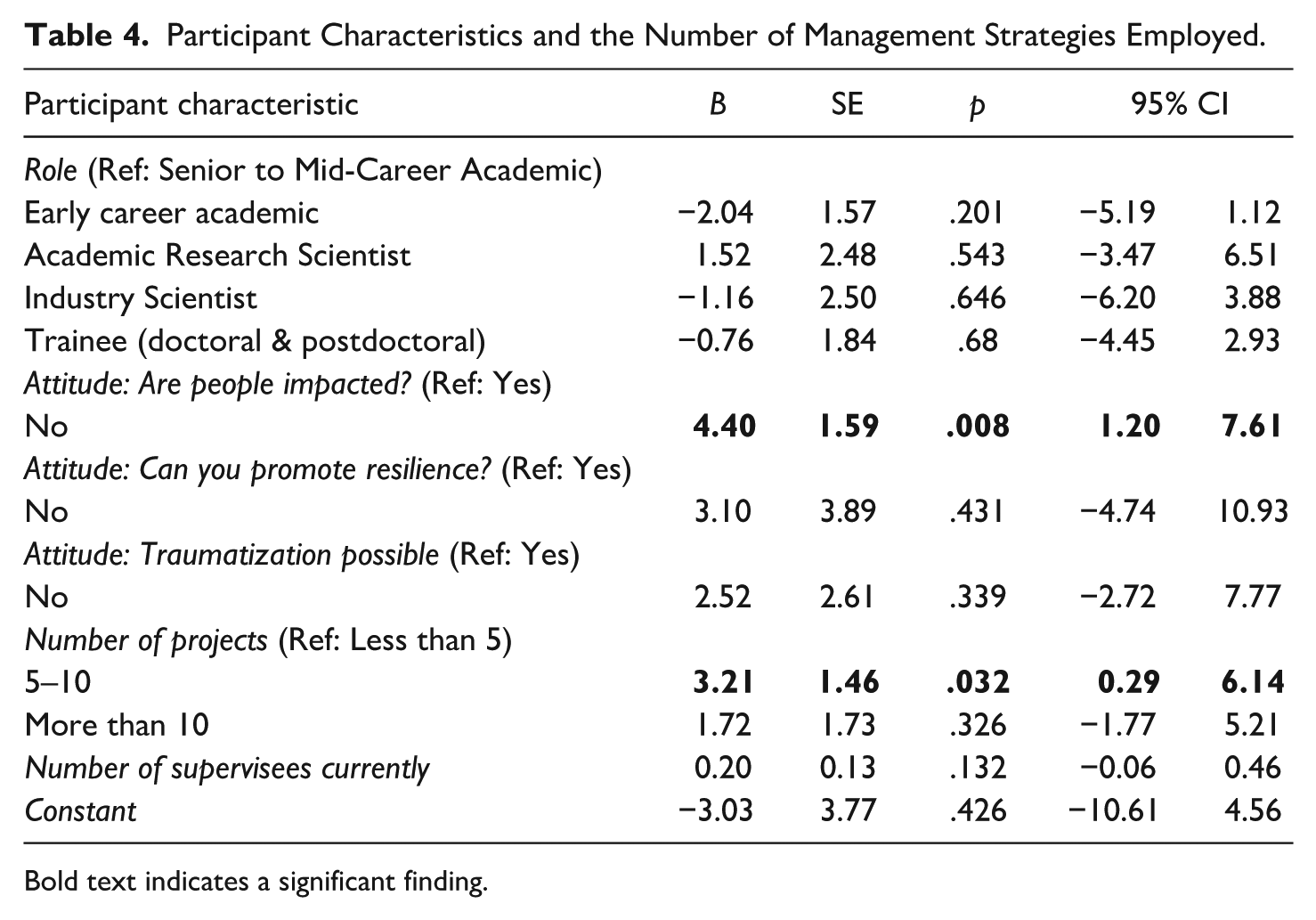
Bold text indicates a significant finding.
Discussion
To summarize, this mixed-methods study found that supervisors used a variety of techniques to promote resilience and prevent traumatization, and these methods were perceived overall as moderately effective. Findings from the qualitative data indicated that perceived effectiveness was context-dependent, varying by research design and research team makeup. Participants further noted that these strategies needed to be paired with genuine, expressed care for team members’ well-being and modeling of the behaviors (e.g., taking breaks) to be effective. Only two strategies were perceived as highly effective: requiring time off and having a team member whose job is supporting team well-being. The number of strategies one used was associated with believing that the work could impact research well-being and having previously supervised others on 5 to 10 projects.
Researcher-participants had used about 10 strategies to respond to vicarious trauma, and findings from the qualitative data emphasized that multiple strategies were needed to foster an environment responsive to traumatic exposure. Studies of interventions with frontline workers have rarely investigated a single strategy but rather examined the impact of multiple interventions, such as training, policies, and social support. Notably, these strategies emphasize interventions implemented by the organization, not individuals. The Vicarious Trauma Toolkit, an evidence-based tool to support community-based agencies to create a vicarious trauma-informed workplace, underlines the importance of a multi-prong approach by examining five areas for intervention: leadership and mission, management and supervision, employee empowerment and work environment, training and professional development, and staff health and wellness (Office for Victims of Crime, 2018). If one were to construct a management approach combining the toolkit domains and the strategies with higher perceived effectiveness ratings found here, one could, for example: include the whole research team in creating research aims and objectives, have regular team meetings that include discussions on well-being, have required time-off given to all team members, train research members on vicarious trauma, and have a designated team member whose job it is to promote well-being and support researchers. This study further underlines past findings that several strategies should be used in tandem to support researcher well-being.
The number of strategies researchers endorsed varied significantly by the number of projects on which they had supervised others. Those who had supervised others on 5 to 10 projects used significantly more strategies than those who had supervised on fewer than five projects. This could be explained by a supervisor seeing the impacts of vicarious trauma on their research team over time and proactively seeking strategies to improve outcomes. However, researcher-participants who worked on the greatest number of supervised projects did not use significantly more strategies than the other, less experienced, researchers. There are a few possible explanations here. First, these researcher-participants may have tried many strategies earlier in their career but have now identified a smaller subset that works well for them. The majority of respondents who reported having supervised others on 10 or more projects were mid-career to senior faculty (68%). It is possible that this lack of difference may also reflect generational differences regarding the responsibility of a researcher to support supervisees in this manner (Austin, 2002) or that later career faculty may be experiencing burnout, decreasing their motivation for intervention (Maslach et al., 2001; McCann & Pearlman, 1990). More work is needed to understand the sustainability and effectiveness of interventions over time and on generational differences in attitudes toward and training on vicarious trauma.
One of the highest-rated, but least endorsed strategies to intervene in vicarious trauma was having a team member whose job it was to respond to the psychological needs of the research team. Past literature on researchers has explicitly endorsed access to psychological support through accessing therapy (Dickson-Swift et al., 2007; Miller Reed et al., 2023; Wallace & County, 2024); and agency guidance has called for having a team member responsible for wellness and safety (Billings et al., 2015; Social Research Association, 2001). Among frontline workers, past research has emphasized the need for institutionalized access to support, including a specific staff person for well-being or access to therapeutic resources (Bell, 2003; Ben-Porat, 2015; Douglas, 2013a; Habeger et al., 2022; McCann & Pearlman, 1990; Office for Victims of Crime, 2018). However, in practice, this role is not always accessible or implemented. One notable barrier to hiring an individual to provide care on a research team, as well as in community agencies, is funding. Some have highlighted a need to change grantors’ perspectives in order to allow budgets that include extra supports for individuals who experience negative impacts from trauma research; a budget item that is as critical to completing the research project as participant incentives (Billings et al., 2015; Dickson-Swift et al., 2008; Social Research Association, 2001). In addition to individual grants, researchers could collaborate with others in their school or department to cost-share a specialized interventionist.
Another potential barrier to accessing care is the feeling that seeking psychological support for one’s work is shameful or wrong (Miller Reed et al., 2023; Wallace & County, 2024). Many scholars are taught to approach science from a positivist and objectivist frame, and admitting that one is having affective and cognitive changes in response to one’s data can go against the image of a neutral researcher that one was taught to emulate (Clegg, 2016; Miller Reed et al., 2023; Wallace & County, 2024; Wilson, 2000). However, injury and violence research meets the criteria of jobs that require emotional labor: our work is public-facing; it can produce an emotional response from others, especially through qualitative interviews and surveys of participants; and supervisors direct the emotional experiences of employees by assigning team members to projects with traumatic material (Hochschild, 2012). Thus, it is the supervisor’s role (and their institution’s) to attend to these emotional and traumatic responses experienced by their team and to proactively manage the impact of traumatic exposure (Cohen & Collens, 2013; Gustavsson & MacEachron, 2002; Hochschild, 2012; Kim et al., 2022; Ting et al., 2006). Importantly, vicarious traumatization theory posits that when one ignores this impact, workers are more likely to develop biases, become cynical, and burn out (McCann & Pearlman, 1990). Accessing care, either outside one’s lab or by having a team member dedicated to wellness, is critical for promoting resiliency and preventing traumatization; however, structural and epistemological changes are needed before this strategy can be widely implemented.
The qualitative analyses indicated that these strategies need to be delivered in a way that felt authentic: supervisees required reminders that they were expected to take interventions like time off, and supervisors needed to model the behaviors for which they were advocating. Prior studies among researchers and frontline workers have found that a positive work environment where individuals feel genuine care promotes resiliency and a sense of equity and fairness (AbiNader et al., 2023; Cummings et al., 2021; Dickson-Swift et al., 2008; Frey et al., 2017; Tham, 2006). Importantly, researcher-participants who believed that researchers could be impacted by trauma were more likely to use a higher number of strategies than those who did not. The normalization of vicarious trauma impact from the supervisor could contribute to a genuine culture of care and create a more robust response to trauma exposure (Frey et al., 2017; Ghahramanlou & Brodbeck, 2000; Habeger et al., 2022; Iliffe & Steed, 2000). In addition to genuinely supporting others, part of creating such an atmosphere is proactively investing in structures that support well-being (Frey et al., 2017). Formal, written policies that ensure time-off, access to services, and flexibility in workloads; describe clear pay scales; and outline other interventions indicate to staff that one is serious about responding to trauma exposure and codify workers’ rights (AbiNader et al., 2023; Cohen & Collens, 2013; Maslach et al., 2001; Regehr et al., 2002). A study of Swedish child welfare workers found that this type of proactive, codified approach to supporting well-being decreased the odds of someone wanting to leave the industry by 48%, and was the sole significantly driving factor when controlling for other characteristics like control over work, perceived inequality, supervisor support, and workload (Tham, 2006).
Study Limitations and Future Research Directions
While this article is an initial step toward examining the perceived effectiveness of interventions used with research teams to promote resiliency and decrease traumatization, it is not without its limitations. The sample for this study was on the smaller side and conveniently sampled, meaning that the findings here are not generalizable to a larger population. National research organizations could perhaps run a randomly sampled survey of their members to better capture the trends nationally. While this study measured perceived effectiveness, studies using experimental methods are needed to measure the effectiveness and sustainability of intervention methods. For example, a multisite study of violence and injury could run a parallel study where some sites receive vicarious trauma interventions and others do not, taking advantage of the multisite project to randomize the intervention by site.
This study intentionally studied researchers with supervisory experience to focus on organizational-level strategies for resilience promotion and traumatization prevention. Thus, the sample represented predominantly senior researchers and may lack insights for managing traumatic exposure that early-career faculty or predoctoral researchers may use to regulate their own exposure that could be extended to team science. Furthermore, in order to measure actual effectiveness of these interventions, supervisees must be surveyed to measure and describe intervention impact. Finally, this study recruited participants primarily from U.S.-based injury science centers, which limits its generalizability globally. More research is needed to understand how local contexts and cultures may influence how researchers experience vicarious trauma and how supervisors mitigate risk on research teams.
Conclusion
Witnessing violence and injury in one’s work elicits affective and cognitive reactions due to potential psychological safety risks and natural empathic responses (American Psychiatric Association, 2022; Herman, 2015; McCann & Pearlman, 1990). It is therefore imperative that research teams develop strategies to promote resilience and prevent traumatization, like those studied here. As researchers, we are bound to ethical codes that dictate practices to keep participants safe, and formal guidelines that also consider researcher physical and psychological safety are needed. Training programs that address vicarious trauma should be developed for use across research labs, similar to the trainings one does for research ethics, and should normalize researcher reactivity to violence and injury data. Interventions could collaborate with existing wellness and safety programs—such as employee assistance programs, student counseling services, and occupational safety and health programs—to decrease the burden of initiating and sustaining vicarious trauma interventions. This study indicated that researchers need a variety of tools in their toolbox to intervene in vicarious trauma and that psychological support and time off were key interventions. More experimental research is needed to test the long-term effectiveness of such interventions.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study obtained appropriate ethical approval from the University of Pennsylvania Institutional Review Board, and obtained informed consent from participants prior to their study participation.