
Abstract
Domestic Violence Fatality Reviews/Domestic Homicide Reviews (DVFRs/DHRs) are multi-agency reviews aimed at reducing domestic homicides. This study systematically reviews research that examines DVFR/DHR recommendations, impact of these recommendations and proposals for improving DVFR/DHR processes. A narrative synthesis was adopted due to the diversity of the 11 studies reviewed. Themes identified from recommendations included: training and awareness; service provision and coordination; and recommendations for children. Regarding DVFR/DHR processes, standardization, diverse teams, and additional resources were highlighted. There was little evidence of whether DVFR/DHR recommendations were implemented. Findings can strengthen DVFR/DHR operationalization and impacts.
Keywords
Despite increasing awareness of, and efforts to prevent, domestic violence-related homicides, deaths from intimate partner or other family related homicide have increased worldwide. Globally domestic homicides have risen from an estimated 48,000 to 50,000 annually between 2012 and 2017 (United Nations Office on Drugs and Crime [UNODC], 2019) with further increases anticipated due to continuing austerity and restrictions from the global COVID-19 pandemic (Grierson, 2020; Rahim, 2019; WHO, 2020). Women continue to be the victims in most cases (82% for intimate partner homicides; UNODC, 2019; UN Women, 2020). However, these are likely to be an underestimate (Campbell et al., 2007; UNODC, 2019).
An initiative that has been implemented in several jurisdictions, which may offer long-term benefit, is the domestic homicide review (Bugeja et al., 2015). Described as domestic homicide reviews in England and Wales, these are known as Domestic Violence Fatality Review Teams (DVFRT) in the US and Domestic/Family Death Review panels/committees in Australia, New Zealand, and Canada (D/FVDR). We use the term DVFR/DHR throughout this paper. Instituted in the USA in 1990, DVFR/DHRs have subsequently been adopted both by federal and national governments (Pow et al., 2015; Websdale, 1999). These multi-agency reviews undertaken following a domestic homicide aim to identify lessons to be learned, develop services, and prevent future domestic homicides (Benbow et al., 2019; Bugeja et al., 2013; Websdale, 1999). They offer, as part of a public health approach to domestic violence and abuse (DVA), the opportunity for systemic and structural changes, as well as increased public awareness, particularly in the local areas where the domestic homicide occurred, although they have utility beyond the local context. Although domestic violence review teams in different countries vary in their governance and operation (Bugeja et al., 2015; Pow et al., 2015), sufficient commonality exists to gain an understanding of the approaches taken and learning generated. Previous reviews have focused on factors thought to influence domestic homicides and on comparisons of core elements of different DVFR/DHR processes (Bugeja et al., 2015; Campbell et al., 2007). This systematic review builds on this work but focuses on analyzing (i) the types of recommendations made by DVFR/DHRs to improve policy and practice, (ii) the impact of these recommendations, and (iii) recommendations to improve DVFR/DHR processes themselves.
Context of Domestic Homicide Fatality Reviews/Domestic Homicide Reviews
Several high-income countries, including the United States, Canada, Australia, New Zealand, Portugal, and England and Wales, now hold multi-agency reviews following a domestic homicide. More recently, South Africa has been considering developing domestic violence homicide review processes (Dawson et al., 2017) and such a process is also under development in North Ireland and Scotland. Importantly, these reviews aim to avoid blaming individual practitioners, but rather identify ways in which systems can better respond to DVA victims and perpetrators.
Bugeja et al.’s (2015) systematic review used Google to identify 25 national and state jurisdictions implementing DVFRS/DHRs. They found considerable variation in the composition and funding of review teams, definitions of domestic violence homicides, case identification and selection, ethical considerations, and family and friends’ involvement in DVFR/DHRs (see also Dawson, 2017).
Remit and Membership of Review Teams
Membership of review teams can include health professionals, criminal justice professionals, emergency services, social workers, DVA service providers and sometimes family members, friends, the perpetrator or survivor representatives. Some states in the US and Australia include representatives from the Medical Examiners or Coroner’s Office (Albright et al., 2013). The formality of review teams also varies. In England and Wales, homicide review panels are convened anew for every review so that representatives of relevant local services can be involved while trained chairs are independent and bring expertise to the process. In the US, Canada and Australia, some teams have an established membership occasionally inviting other professionals to share expertise for the review of a specific or complex case (Albright et al., 2013; Jaffe et al., 2013). There are also differences between team membership in neighboring jurisdictions within each country. The lack of consistency in processes has also been linked to limited funding (Albright et al., 2013; Jaffe et al., 2013; Reif & Jaffe, 2019). Many teams in the US and Canada have previously been found to operate on a voluntary basis without funding (Albright et al., 2013; Jaffe & Juodis, 2006), particularly for smaller committees with lower numbers of homicides (Jaffe et al., 2013).
Variations in funding for DVFRs/DHRs affect the numbers of cases selected for review, processes used, and may result in difficulties in conducting reviews systematically (Jaffe et al., 2013; Reif & Jaffe, 2019; Websdale, 2003). Resources and legal complications are also cited as restricting the number of reviews in the US (Websdale et al., 2017). Similarly, the definitions of domestic homicide used (and therefore which cases are selected for review) vary. Whilst definitions in Canada and the US are not uniform across states, more commonly, the focus of DVFR/DHR teams is on intimate partner homicide only (Dawson et al., 2017; Websdale, 2020). Domestic homicide reviews in England and Wales also cover familial violence between those aged over 16 as mandated by statute. A broader definition of domestic homicide allows for exploration of the specificities of this type of domestic homicide as well as its overlaps with intimate partner homicide (Tolmie et al., 2017).
More recently, activists and family members in the US, England and Wales, Canada, and Australia have called for the inclusion of suicides by victims of domestic violence and abuse (DVA) in domestic homicide reviews and several jurisdictions have the scope to review DVA related suicides. DVA is well documented as a precursor to depression and attempted suicide globally (Devries et al., 2011; McLaughlin et al., 2012). However, establishing DVA as causal in suicide can be difficult, as is obtaining a verdict of suicide. For example, in England and Wales, a coroner can only attribute a death as suicide where there is sufficient evidence (on the balance of probabilities) that a person intended to take their own life.
Ethical Considerations
Three key points need to be considered regarding the ethical considerations embedded in the production of DVFR/DHRs. Firstly, anonymity is adopted to ensure respect and sensitivity for the victim and their family. However, at least in the English/Welsh contexts, media reports frequently contain the names, ages, and details of the crime so it is relatively easy to connect media reports with the publicly available review report. A second question relates to the level of detail and timeframe for “looking back” required for review purposes whilst providing maximum anonymity to the family involved. Chantler et al. (2020) found that the quality of DVFR/DHRs varied in England and Wales and that the timeframe for reviews differed despite having common terms of reference. In the US and in Canada, privacy laws restrict what information agencies can provide to the review team (Dawson et al., 2017; Websdale, 2020). The balance between what information is required to learn from domestic homicides and the need for confidentiality varies between jurisdictions and poses important ethical challenges. The third key ethical issue lies in case selection. As Dale et al. (2017) highlight, if only one “type” of case is always reviewed, the knowledge and learning generated will be restricted. They also argue for the importance of ensuring that case selection is representative of different types of domestic homicide in diverse communities.
Family and Friends’ Involvement in DVFR/DHRs
The involvement of family/friends is recommended in England and Wales, and some states in the US, Australia, and Canada. Family/friends may provide a perspective on antecedents, family relationships and experiences of help-seeking that may not otherwise be available to review teams (Mullane, 2017). Their involvement can help to center the victim’s experience and ensure that her story is not erased. Stanley et al. (2019) note the limited involvement of children in DVFR/DHRs despite their active role in experiencing DVA, witnessing the homicide and calling for help. Alisic et al. (2017) note that adults may wrongly assume that children did not directly witness or “take in” a domestic homicide. However, review teams are sometimes anxious about involving family members out of concern for their privacy and about the potential for retraumatization. Post-homicide support to surviving family members does not generally fall within the remit of DVFR/DHRs, but children’s experience of the aftermath of domestic homicide is a growing field of study (Alisic et al., 2015).
Methods
Our systematic review followed recognized guidance and reporting standards (Aromatris & Munn, 2017; Higgins et al., 2019). We identified studies through searches of 11 electronic databases specifically: Academic Search Complete, Assia, Criminal Justice Abstracts, Criminal Justice Database, ERIC, Scopus, Social Policy and Practice, Social Work Abstracts, SOCIndex, Web of Science, and Westlaw (see Appendix A for search strategy). All electronic searches were limited to articles published in English between 2001 and August 2019. Additional references were identified through screening reference lists and forward citation tracking of included articles, as well as through contact with experts. We scoped the grey literature, finding that it focused on domestic homicide cases rather than DHR processes or impact and, as a consequence we excluded it from the review.
Studies were eligible if they: outlined the implications for agencies, policy, or practice; examined the different approaches used to produce DVFR/DHRs (e.g., people and organizations involved, types of homicides included, sources used, timing of review); or provided recommendations for effective operation of the DVFR/DHR process; or assessed the impact of initiatives to reduce the occurrence of domestic homicides (e.g., interagency communication, training, and education). We included research studies, but not the reviews themselves. The focus of included studies was on adults aged 16 years or older who were killed by a family member or (ex-)partner. Study designs could include systematic reviews and any experimental or quasi-experimental design that used quantitative, qualitative, or mixed methods approaches. Those studies that focused only on child homicides or were either non-systematic reviews, opinion pieces, editorials, or letters were excluded. Studies that described characteristics of victims and perpetrators of domestic homicide were excluded as this review addressed systems and processes for reviewing these deaths. Individual reports of domestic homicides were also excluded as our review was primarily addressing systems and processes. Abstracts and conference proceedings were only considered if sufficient detail of their methodology and results were published.
Study selection occurred through two stages. First, one reviewer (KB or CJ) screened the titles of papers from the searches, using criteria specified prior to screening. A second reviewer checked a random 10% sample of decisions (KB or AC). Any discrepancies were discussed between the reviewers. Second, those studies appearing to meet the selection criteria at the first stage were retrieved. These were then screened independently by two reviewers (KB, CJ, AC, KC) using the same criteria. Any discrepancies were discussed between the two reviewers, with arbitration by a third reviewer where required (NS).
Data were extracted using a pre-piloted form by one reviewer (KB, CJ, AC, KC, NS). We extracted data on: study characteristics (e.g., place of study, design, and time period); characteristics of DVFR/DHR process (e.g., type(s) of homicide included; process for identifying homicides, DVFR/DHR review team members, sources of information, timing of process); recommendations from the DVFR/DHR process; barriers to DVFR/DHR process; and, implementation and impact of recommendations. Primary research studies were appraised using the Mixed Methods Appraisal Tool (Hong et al., 2018), which focuses on assessing the methodological quality of mixed-methods, quantitative descriptive, nonrandomized, randomized control, and qualitative studies. Any systematic reviews were assessed using recommended criteria for judging quality (Pettigrew & Roberts, 2006). Interpretation was through reporting for each component rather than reporting an overall quality score (Egger et al., 2001). Studies were assessed independently by two reviewers (KB, CJ, AC, KC, NS), with any differences discussed and arbitration by a third independent reviewer where necessary.
As the studies differed in terms of their designs, we combined the evidence through a narrative synthesis with tabulation of results of included studies. We identified key themes among DVFR/DHRs recommendation, separating them into those assessing implications for either policy and practice or DVFR/DHR process and evidence on the impact of any recommendations on reducing domestic homicides. The methodological quality of the different studies and the implications for our findings were considered. This provided an understanding of the possible biases and uncertainties that may underlie the conclusions drawn. Meta-analysis was not undertaken due to the limited evidence base and heterogeneity among the studies.
Other limitations included exclusion of the grey literature and first-stage selection of paper by title only. Contact with study authors provided limited information. Strengths of the review included: comprehensive searches, checking of reference lists, and forward citation. Despite differences in legal arrangements, team composition, funding arrangements, case-selection processes, family involvement, and availability of materials available (e.g., interview transcripts, case reports from agencies etc) for conducting reviews, they all have the common aim of strengthening responses to DVA. Whilst direct comparisons are not possible given the different contexts, the types of key recommendations made appear to be remarkably consistent between and within jurisdictions. Importantly, the process of working together to produce the review may in itself facilitate the implementation of recommendations.
Findings
The multiple search strategies yielded a total of 22,531 records. After duplicates were removed (n = 10,089), the titles of 12,442 records were assessed, with reviewers excluding 12,390 records which did not meet the criteria. Of the 52 records that potentially met the inclusion criteria, four journal articles could not be located. After full text screening, 11 records were included in the review (see Figure 1). Six papers used qualitative designs, three used a quantitative design, and one used mixed-methods. The findings from the systematic review are presented in Table 1. Quality assessment is discussed below followed by the narrative synthesis which is organized according to the key questions of the literature review.
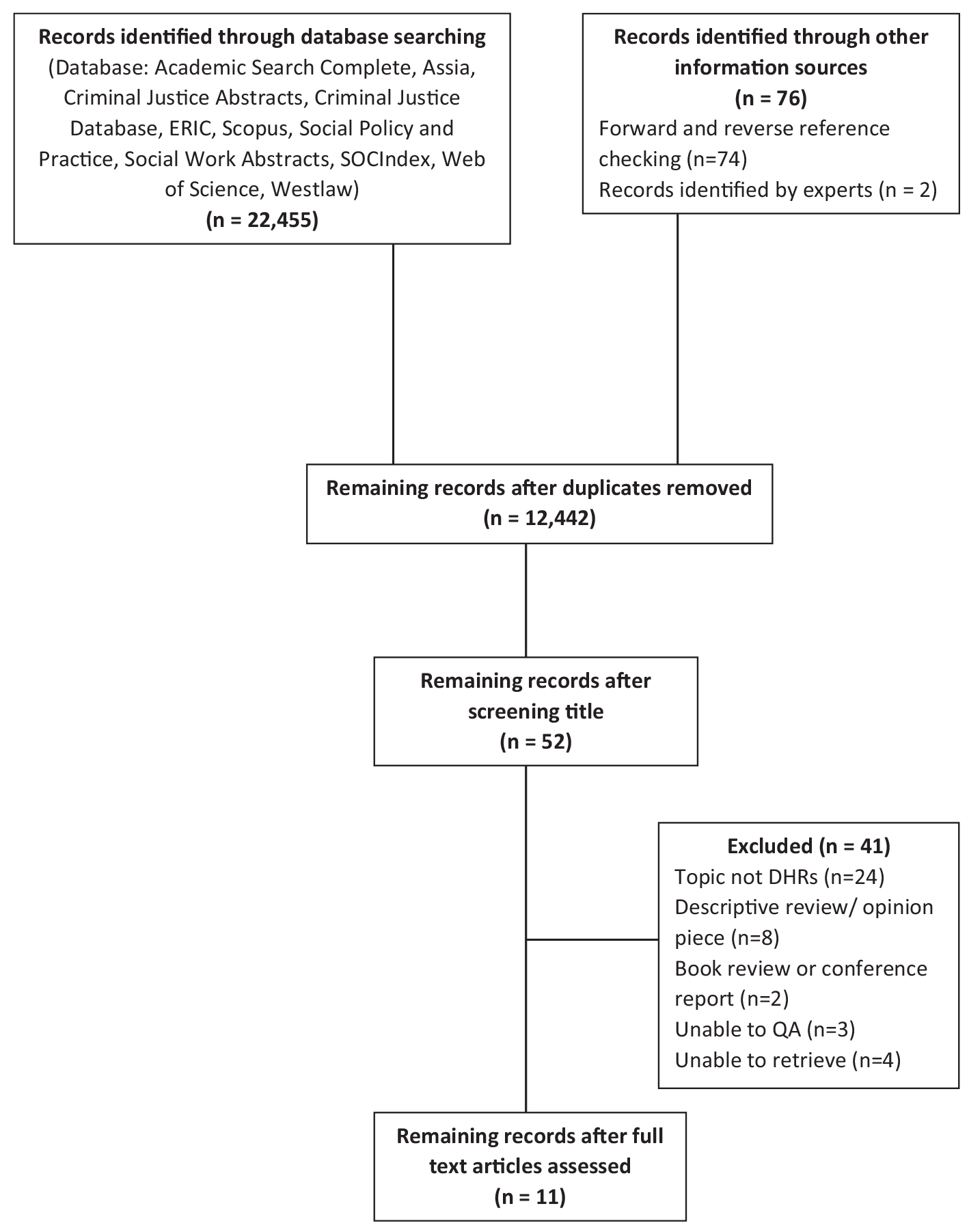
Flow diagram of selecting records for this study.
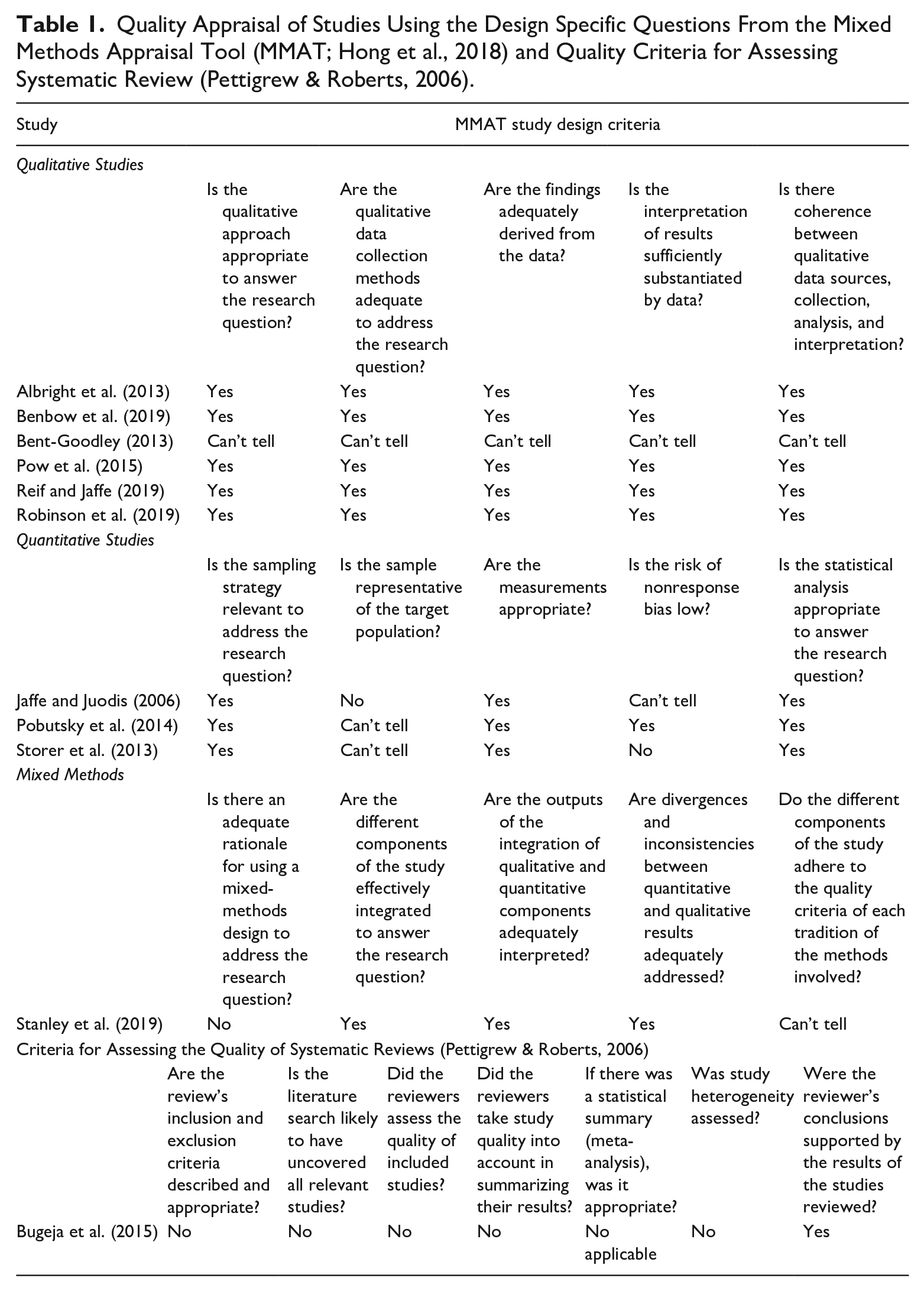
Quality Appraisal of Studies Using the Design Specific Questions From the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018) and Quality Criteria for Assessing Systematic Review (Pettigrew & Roberts, 2006).
Quality Assessment
Ten studies were appraised using the MMAT (Hong et al., 2018) and Pettigrew and Roberts (2006) criteria for assessing systematic reviews was used to appraise the eleventh study. Table 1 shows that, of the six qualitative studies, five were judged to be high quality as they appropriately addressed all quality criteria and for one study the quality was uncertain as insufficient information was provided. All three quantitative studies adopted a suitable sampling strategy, measured outcomes appropriately and conducted appropriate statistical analysis. It was unclear if the sample was representative in two studies (Pobutsky et al., 2014; Storer et al., 2013) and was found not to be representative in one study (Jaffe & Juodis, 2006). The risk of bias from nonresponse was considered low in one study (Pobutsky et al., 2014), uncertain in one study (Jaffe & Juodis, 2006), and was high in another study (Storer et al., 2013). The quality of the Google-based systematic review (Bugeja et al., 2015) included in our study was judged using standard criteria (Pettigrew & Roberts, 2006). While the review did not provide adequate information on selection criteria, search strategy, quality assessment, synthesis, and assessment of heterogeneity (Bugeja et al., 2015), the results were supported by the information presented (Bugeja et al., 2015).
Recommendations From DVFR/DHRs
The 11 studies analyzed DVFR/DHRs and the processes used to produce them from several perspectives, either focusing on individual DVFR/DHRs (Benbow et al., 2019; Pobutsky et al., 2014; Robinson et al., 2019; Stanley et al., 2019), annual reports from different jurisdictions (Bugeja et al., 2015; Jaffe & Juodis, 2006; Pow et al., 2015; Reif & Jaffe, 2019), undertaking a survey of those involved in DVFR/DHRs (Storer et al., 2013) or presenting personal reflections on the DVFR/DHR process (Albright et al., 2013; Bent-Goodley, 2013). All made recommendations about the approaches made to producing DVFR/DHRs in their respective jurisdictions and to preventing DVA and future domestic homicides. Despite the variation reported between the papers, common themes are evident that provide a basis for future action. The overarching themes identified include prevention activities including training and awareness regarding DVA and domestic homicides; provision and coordination of services; recommendations for children impacted by DVA and domestic homicide; and processes and teams involved in DVFR/DHRs. Many emphasize the necessity for increased resources and service provision to enhance services to DVA victims (see Table 2).
Type of Recommendation From DVFR/DHRs for Policy and Practice and for the DVFR/DHR Processes and Teams.
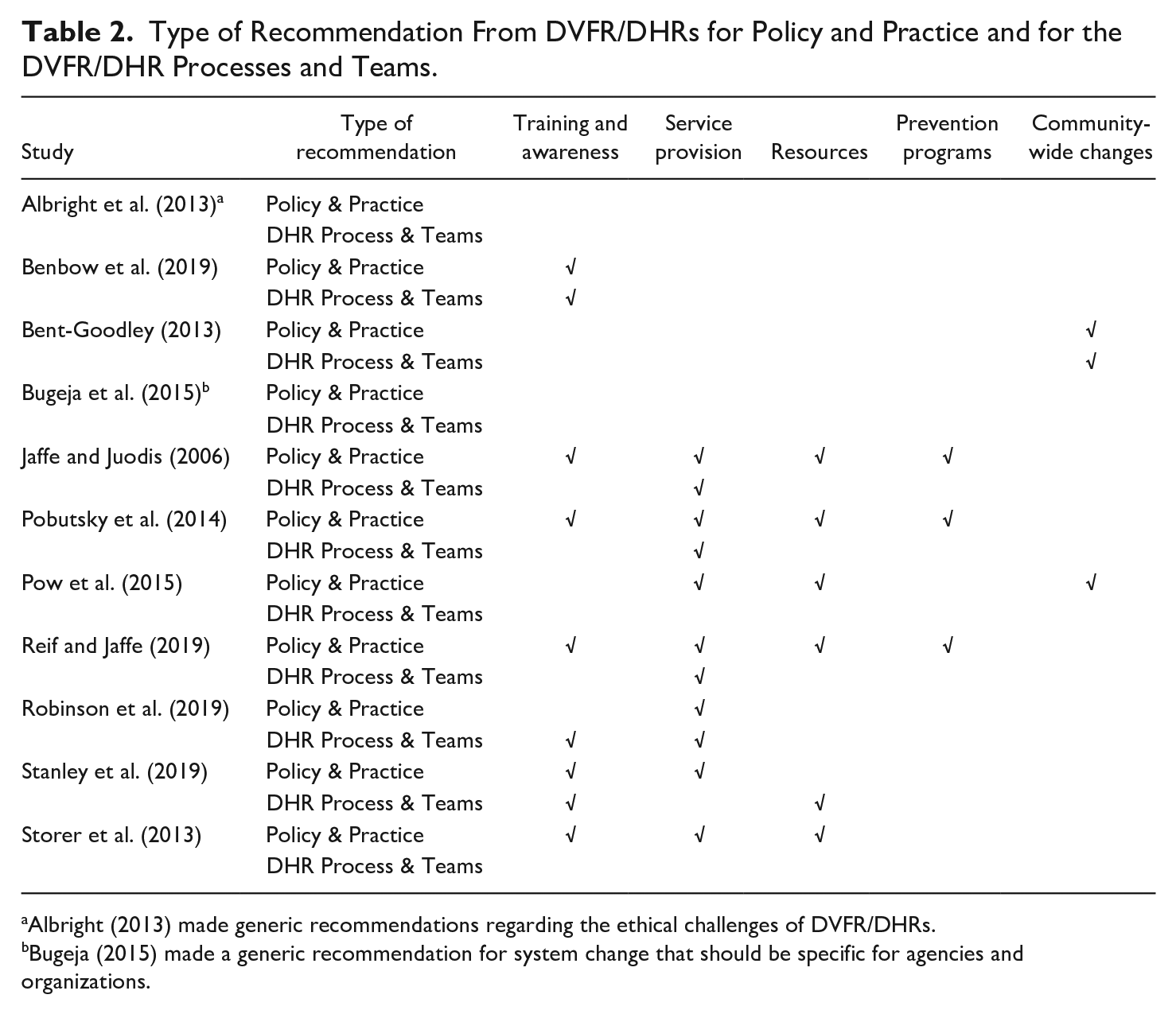
Albright (2013) made generic recommendations regarding the ethical challenges of DVFR/DHRs.
Bugeja (2015) made a generic recommendation for system change that should be specific for agencies and organizations.
Training and awareness
Improving awareness and understanding of the dynamics of DVA was a recommendation in seven studies (see Table 2). This was identified as important for professionals across the different sectors involved in DVA and domestic homicide (Robinson et al., 2019) including: education and childcare practitioners to improve early identification of DVA (Jaffe & Juodis, 2006; Reif & Jaffe, 2019); law enforcement officers (Jaffe & Juodis, 2006; Storer et al., 2013), DVA practitioners (Pobutsky et al., 2014), and judges and court evaluators involved in DVA cases (Jaffe & Juodis, 2006; Storer et al., 2013). Although any training should provide an understanding of the dynamics of DVA, child risk, screening, risk assessment, and the different approaches for intervening (Reif & Jaffe, 2019), some aspects require particular attention. Professionals need to be attuned to the different needs of different groups (Benbow et al., 2019; Storer et al., 2013) to avoid stereotyping. Training that alerts professionals to perpetrators’ controlling tactics and develops their ability to encompass wider underpinning evidence, was considered essential (Robinson et al., 2019). Addressing professionals’ different training needs may be augmented through good-quality supervision (Stanley et al., 2019). Increasing public awareness regarding DVA prevention and services was also recommended by Pobutsky et al. (2014), Pow et al. (2015), and Reif and Jaffe (2019).
Provision of services and inter-agency coordination
Seven studies made recommendations concerning the provision and coordination of different services (see Table 2). The importance of social support systems and calls to provide adequate funding for services to respond to victims, perpetrators, and their children were emphasized throughout the papers reviewed (see Table 2). Three of the eleven papers (Jaffe & Juodis, 2006; Reif & Jaffe, 2019; Stanley et al., 2019) focused on children impacted by domestic homicide and made a raft of recommendations related to this. Child protection services were identified as requiring review, and possible revision, regarding victims’ contact with the service and subsequent domestic homicides, their handling of families with a history of DVA, their practices when a parent has a serious mental illness and their effectiveness in sharing information (Jaffe & Juodis, 2006).
Several recommendations focused on reviewing and enhancing service quality (Reif & Jaffe, 2019), increasing the provision of and referral to services (Pobutsky et al., 2014), and improving the coordination between existing services (Jaffe & Juodis, 2006; Reif & Jaffe, 2019). Others identified the need to: ensure services reflect cultural, language and religious diversity (Pobutsky et al., 2014; Storer et al., 2013), improve transitions between services and geographical boundaries (Robinson et al., 2019) and extend provision to include outreach and follow-up services (Reif & Jaffe, 2019). Engagement with DVA perpetrators was also recognized as important, with services working with them to locate responsibility for their behaviors (Stanley et al., 2019) and probation services providing adequate post sentence supervision (Storer et al., 2013). Concerns about inadequate assessments (Robinson et al., 2019), a lack of communication between criminal justice and family courts (Jaffe & Juodis, 2006), limited civil legal services for DVA victims (Jaffe & Juodis, 2006), and a need to increase safety planning (Pobutsky et al., 2014) were also highlighted in recommendations.
Children
The impact of domestic homicide on children, their involvement in DVFR/DHR processes, and their role in informing future policy was emphasized (Stanley et al., 2019). Separation of families (Stanley et al., 2019), disputes over access and custody (Jaffe & Juodis, 2006), and child abuse and neglect are recognized risks for DVA (Jaffe & Juodis, 2006). Policy and practice should address these risks, ensuring that guidance is provided to identify, report, and manage them effectively and that mothers are not assigned sole responsibility for children’s safety (Stanley et al., 2019). Mental health services for children (Jaffe & Juodis, 2006) and support for new caregivers for children who had lost parents to DVA would benefit from additional funding (Jaffe & Juodis, 2006).
Impact of Recommendations
We concur with Bugeja et al. (2015) that there is as yet no evidence that the practice of reviewing domestic homicides has impacted on the numbers of these deaths and they suggest that this reflects the difficulty of forging a causal chain between the work of reviews, their recommendations and the incidence of deaths. DVFR/DHRs bring together local agencies, which is consistent with the coordinated community response model (Chanmugam, 2014; Websdale, 2020). Evaluating this model has proven difficult due to its complex and localized nature, as well as different understandings of what constitutes “success” (Johnson & Stylianou, 2020). Similar logic can be applied to the work of DVFR/DHRs. Their focus on identifying gaps in local service provisions and interagency working may lead to different “successful outcomes” that are not captured in traditional studies such as randomized control trials. This means it may not be feasible to link outcomes from recommendations with a reduction in DH.
Another challenge may be the lack of tracking of the implementation of DVFR/DHR recommendations. Reif and Jaffe (2019) point out that, in North America, agencies are not usually mandated to respond to or implement the recommendations of these reviews. Storer et al.’s (2013) study reported that, although participants considered that DVFR/DHR recommendations were consistent with agencies’ priorities, they were less likely to report that implementation of these recommendations was a priority. The researchers argue that organizations need incentives to act on recommendations and suggest that positive media coverage of good practice or innovation grants might function in this way. Support and training are identified as necessary for individual organizations to make the shift from prioritization to implementation of recommendations (Storer et al., 2013). Such support might be derived from national networks such as the National Domestic Violence Fatality Review Initiative cited by Reif and Jaffe (2019) or international networks such as the WHO (Bugeja et al., 2015). These networks can also facilitate the sharing of resources and promote dialog between those undertaking DVFR/DHRs (Reif & Jaffe, 2019). .
DVFR/DHR Processes and Teams
Seven studies addressed DVFR/DHR processes and teams directly (see Table 2), identifying limitations in the DVFR/DHR processes and proposed new or improved protocols and policies (Bent-Goodley, 2013; Pobutsky et al., 2014; Reif & Jaffe, 2019). DVFR/DHRs recommended a focus on victims and perpetrators (Bent-Goodley, 2013) and utilizing standardized data collection processes (Albright et al., 2013). Processes should acknowledge that a balance is required between the dual roles of the team members as evaluators and system experts (Albright et al., 2013). Albright et al. (2013) advocate transparency on issues such as team membership and representativeness, case selection, and integrity and honesty about the tensions that can arise between members of a review team. These tensions relate to different organizational priorities, professional practices, and the potential for conflict, particularly where one service system is seen as having scope for improvement in their responses to victims or perpetrators of DVA.
The importance of diverse review team membership was highlighted as a key recommendation for improving the process of review teams (Albright et al., 2013; Pow et al., 2015). Three papers identified specific areas for development around issues of diversity: representation of older people, ethnic minority communities, and children. Benbow et al.’s (2019) analysis of DVFR/DHRs in England identified how processes could be improved for adults over 60 years of age. This included addressing ways in which stereotypes may affect how homicides are approached, reviewed, and reported, since stereotypes and assumptions about aging influence health and social care assessments and interventions. They also highlighted that terminology needs to be standardized as multiple terms are used interchangeably in relation to abuse and older adults. Bent-Goodley (2013) argued that teams must work with Black communities to ensure that there is diverse representation and cultural competence included in the review team to ensure both the processes and outcomes are culturally sensitive. This is important in the US given that fatalities disproportionately affect Black women (Bent-Goodley, 2013). Finally, Benbow et al. (2019) highlight the tension between speed and thoroughness in the production of DVFR/DHRs. Robinson et al. (2019) argue against separate review processes such as those undertaken in mental health cases or adult practice reviews due to the duplication of evidence-gathering. They argue for a unified multi-disciplinary approach to review. Several studies recommended a single repository to maximize learning from DVFR/DHRs (Benbow et al., 2019; Robinson et al., 2019; Stanley et al., 2019).
Discussion
Organizational and professionals’ responses to DVA are central to operationalizing the learning from DVFR/DHRs. This includes training, interagency working, as well as relationships between these organizations and the community. The wider socio-political context also shapes DVA service provision and the ability to implement recommendations. To maximize learning, DVFR/DHR reports also need to be readily accessible. Each of these are discussed in turn.
Training
As discussed above, a common recommendation in DVFR/DHR reports is for service providers to improve and increase their DVA training. As professionals working with DVA come from different backgrounds (e.g., law, health, or social work), review teams may want to consider tailoring training recommendations to a specific group of professionals. For instance, recommendations tailored to professionals working with children focused on managing DVA risk in custody disputes (Jaffe & Juodis, 2006) and risk assessment and management (Reif & Jaffe, 2019). Alternatively, review teams could focus on a specific group of professionals who may engage with perpetrators, victims, and children and recommend an established training program. However, there are also benefits to inter-agency DVA training.
Studies examining DVFR/DHR recommendations showed that professional training has been a key recommendation for well over a decade, indicating that this recommendation has not been successfully embedded. DVA training needs to be an on-going process rather than a one-off activity, hence the repetition of this recommendation over time.
Interagency Working
As outlined, DVFR/DHRs are part of the interprofessional coordinated response to DVA (Payton et al., 2017; Websdale, 2020) and also focus on the relationships between agencies. Recommendations are often targeted at individual agency level, but it might be helpful if these were also extended across agencies (Reif & Jaffe, 2019). There are benefits to both specific professional group DVA training as well as interagency training as research suggests that professionals have more confidence to speak with victims and take appropriate action following interagency training (Szilassy et al., 2014). This may also help to address some of the challenges surrounding silo-working (Stanley et al., 2019; Websdale et al., 1999). Improved interagency working might also assist in moving from individual to collective responsibility/accountability for combating DVA and lead to more embedded systemic change.
In terms of DVFR/DHR processes, review teams may also want to consider recommendations around interagency working during the fatality review process. As mentioned above, it is important that inter-agency working during fatality reviews operate a culture of “no blame” (Bowman, 1997; Storer et al., 2013; Websdale, 1999) but it is useful to consider how this is operationalized. Working within a “no blame” culture might also contribute to broader impacts, such as improvements in inter-agency working between those involved in fatality review process (Websdale, 2012, 2020). However, this may depend on whether team membership is consistent over time or newly established for a specific case, as well as existing power dynamics between team members and their professional backgrounds (Albright et al., 2013).
Community Involvement
As highlighted above, a common recommendation made by DVFR/DHR teams has been to increase public education and awareness (see Table 2) with the aim of changing social norms surrounding DVA and help-seeking behaviors. Such changes in awareness and community acceptance may assist victims to overcome barriers to seeking formal help and support. Across the DVFR/DHR literature reviewed here, “community” was very broadly conceptualized and included community services/organizations and informal networks. Community trust (or absence of) in organizations or institutions (e.g., Bent-Goodley, 2013; Watt, 2003; Websdale, 2003), but also recognition of responsibility for challenging DVA may be key factors. However, where a recommendation is made to raise community awareness, “community” needs to be clearly defined.
Some US states have public, open death review meetings (Albright et al., 2013) which may go some way to conveying that DVA is a community responsibility. US review teams have also made recommendations to increase the involvement of ethnic minority communities in review processes, creating opportunities to talk about DVA, building greater culturally and linguistically appropriate public awareness about DVA, or policy recommendations to enact community change (e.g., Bent-Goodley, 2013; Chanmugam, 2014; Fawcett et al., 2008; Pow et al., 2015). UK literature (Benbow et al., 2019; Stanley et al., 2019) also highlights the importance of including marginalized voices in DVFR/DHRs.
Recommendations targeted at communities are currently underutilized and under-evaluated (Storer et al., 2013), DVFR/DHRs with close links to community members and professionals, who have in-depth knowledge of the dangers victim-survivors face may have greater success in implementing recommendations (Websdale, 2012).
Interventions, policies and responses to DVA should take place across all societal levels, including communities, but what is most appropriate in which context is currently unknown. Given the importance of the broader community context in which organizations operate, future research should examine the structures, processes and outcomes of DVFR/DHRs with specific consideration of the DVFR/DHR relationships to communities and circumstances which may influence the implementation of community recommendations, including the constraints or obstacles experienced and whether different contexts require difference approaches.
Socio-Cultural Contexts and DVFR/DHR Processes
Turning lastly to the wider socio-cultural context and focusing on DVFR/DHR processes, we consider three key inter-related points. Firstly, in jurisdictions where there is no statutory requirement to conduct a DVFR/DHR for all domestic homicides, decisions must be made about which cases to review and why. This variability reduces the potential for robust international comparisons and recommendations and potentially limits the usefulness of the reviews at an international level. Transparency regarding the definitions of domestic homicide could facilitate cross-jurisdictional comparisons of data (Fairbairn et al., 2017). The varying definitions adopted have an impact on how domestic homicide is framed and the recommendations, policy guidance and practices that subsequently flow from them (Fairbairn et al., 2017). Similar concerns apply in those jurisdictions where only a proportion of cases are reviewed. Where countries have a more centralized and standardized approach to fatality reviews for example, in England, Wales, and New Zealand, this may make both intra-country and cross jurisdictional comparisons easier. Wilson and Websdale (2006) call for the standardization of DVFR/DHR processes in the USA, indicating the benefits of standardization at least at the country level. Whilst standardization globally is constrained by differing social, economic, and political contexts, consideration of what type of standardization is feasible needs to be deliberated. Initial considerations can be drawn from Dawson and Carrigan’s (2021) work highlighting the efficacy and limitations of national administrative data to identify femicide and its subtypes. A similar approach could be explored to define and research other forms of family homicide.
Secondly, the funding of DVFR/DHRs also varies across jurisdictions and this impacts on the number of cases reviewed, particularly in the US where numbers of domestic homicides are high (Pow et al., 2015). Whilst acknowledging that this makes it unfeasible for all cases to be reviewed, aiming to review a sample that is both representative and embraces diversity is desirable (see Albright et al., 2013; Lehrner & Allen, 2009; Websdale, 2003). It is acknowledged that DVFR/DHRs are resource intensive and the instability of funding in some jurisdictions makes it difficult for the review teams to consistently produce reports (Sheehy, 2017). However, Sheehy (2017), writing from a Canadian context, also highlights the challenges of state funding such as inadequate resourcing to conduct reviews, a reluctance to enact laws to ensure compliance from state agencies, and difficulties in critically analyzing the policies and practices of other state actors. Robinson et al. (2019) recommend an integrated approach to reviews incorporating adult protection and mental health reviews in Wales. Whilst this approach has the advantage of reducing duplication in a small resource-poor jurisdiction, the centering of victims’ experiences of DVA may be in danger of being obfuscated.
Thirdly, the question of whether scarce resources are being well utilized is pertinent, specifically regarding the accessibility of DVFR/DHRs and the implementation of their recommendations. For relevant organizations to utilize the learning from DVFR/DHRs, access to the published reports is necessary. UK studies (Benbow et al., 2019; Chantler et al., 2020) suggest that DVFR/DHR reports should be readily accessible for research and subject to regular review so that learning from DVFR/DHRs is maximized. The difficulties in obtaining DVFR/DHRs in England and Wales for research purposes has been documented (Benbow et al., 2019; Bridger et al., 2017; Sharps-Jeff & Kelly, 2016). Jaffe et al. (2013) propose a national website similar to the US National Domestic Violence Fatality Review Initiative which provides technical assistance to review teams as well as state reports, documents, and resources.
Implementation shortfalls represent a lost opportunity to embed learning, new policies and practices and to understand subsequently whether systems have changed or responses to those experiencing DVA have improved. DVFR/DHRs offer a unique opportunity to assess recommendations over time and to make a real difference to victims of DVA. Even in jurisdictions such as England and Wales, where there is a statutory requirement to carry out a DVFR/DHR, there is no statutory requirement to report on whether recommendations made in the review have been implemented or on the barriers and enablers to implementation. Bugeja et al. (2015) found that only seven jurisdictions globally mandated a response to recommendations or had mechanisms for monitoring recommendations. The recommendations may well have financial costs and the wider socio-political environment is also key as different nation-states make different choices about provision of specialist DVA services. Pow et al. (2015, p. 216) highlight the political implications of moving forward to implement recommendations. The austerity-driven policies of the last 10 years have not been conducive to implementing recommendations of DVFR/DHRs. Further, as our review found, few papers discuss evaluations of the impact of recommendations made (see also Chanmugam, 2014) and this is also a major gap in the domestic homicide field. To capitalize on learning from DVFR/DHRs, monitoring the recommendations themselves, their implementation as well as evaluating them for impact appears to be key. This requires adequate resourcing for the conduct of reviews as well as for implementing change. Incorporating feedback loops into the review process (Fish et al., 2008) could increase the likelihood of recommendations being implemented and used to strengthen practice and policy.
Conclusion
This systematic review of the recommendations, impact and processes of DVFR/DHRs has generated valuable messages concerning selection of cases for review, the membership of review panels and review funding mechanisms for those jurisdictions currently in the process of introducing these reviews and for those seeking to refine and strengthen current review processes and outcomes. DVFR/DHR findings represent a key aspect of a public health response to DVA. Importantly, DVFR/DHRs bring together information about the individuals involved (i.e., victim and perpetrator) and the nature of their relationships (including family, friends, and partners), the setting or community in which the violence occurs and the wider societal context (e.g., health, economic, education, social environment). In doing so, they help to facilitate (i) identification and monitoring of the extent of problem, (ii) recognition of possible risk and protective factors, (iii) informing of the development and testing of strategies to prevent DVA and, (iv) support implementation and evaluation of the adoption of evidence based approaches to tackling DVA and DH (Dahlberg & Krug, 2002).
As well as allowing the development of recommendations from individual DVFR/DHRs that are relevant to specific community contexts, our review illustrates the benefits of looking across cases to identify common themes to support evidence-based approaches to tackling DVA and DH more widely. Based on existing literature and our review, future research recommendations include (i) further understanding of how DVFR/DHR processes influence implementation of recommendations; (ii) research on the impact of involvement in DVFR/DHRs on family members; (iii) further research on the relationship between suicide and victims and perpetrators of DVA. DVFR/DHRs have the potential to improve public awareness and responsiveness to DVA. Publishing DVFR/DHR figures and narratives serves to highlight the gendered nature of DVA and provides a powerful driver for governments to introduce relevant legislation and resource DVA services. To this end, it is essential that these reports are centrally available and can be utilized to inform policy, public awareness, professional training, and practice. Attending to the way in which DVFR/DHR recommendations can best be implemented and resourced might yield further benefit by strengthening responses to DVA
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the support provided by the Economic and Social Research Council, UK under grant number ES/S005471/1. Andrew Clegg is part-funded by the National Institute for Health Research (NIHR) Applied Research Collaboration North West Coast (ARC NWC). The views expressed are those of the authors and not necessarily those of the NIHR or Department of Health and Social Care.