
Abstract
Complex biological processes such as inflammation, cell death, migration, proliferation, and the release of biologically active molecules can be used as outcomes in phenotypic assays during early stages of drug discovery. Although target-based approaches have been widely used over the past decades, a disproportionate number of first-in-class drugs have been identified using phenotypic screening. This review details phenotypic assays based on inhibition of microglial activation and their utility in primary and secondary screening, target validation, and pathway elucidation. The role of microglia, both in normal as well as in pathological conditions such as chronic neurodegenerative diseases, is reviewed. Methodologies to assess microglia activation in vitro are discussed in detail, and classes of therapeutic drugs known to decrease the proinflammatory and cytotoxic responses of activated microglia are appraised, including inhibitors of glutaminase, cystine/glutamate antiporter, nuclear factor κB, and mitogen-activated protein kinases.
Introduction
Advances in molecular biology and genetics in the 1980s, in addition to the publication of the human genome sequence in 2001, led the pharmaceutical industry to consider every functional protein as a potential therapeutic drug target. Moreover, unwanted side effects to drugs have been attributed to nonspecific interactions between drugs and proteins or systems other than the anticipated target. In that respect, for more than 20 years, drug discovery efforts have been focused on the rational tailoring of high-affinity drugs capable of selectively and specifically inhibiting a particular target known to play a role in disease pathology.1,2
Target-based drug discovery led to the production of many of the drugs currently on the market. 3 This approach is most appropriate when there is a clear understanding of the molecular basis of a disease and the structure, function, and regulation of the therapeutic target. However, present levels of productivity in the pharmaceutical industry are suboptimal, and it has been suggested that productivity could increase if a shift from solely target-based assay approaches to inclusion of phenotypic assays (PAs) occurs in the early stages of compound screening. 4
In support of this concept, from 1999 to 2008, most new molecular entities approved by the Food and Drug Administration (FDA) were identified using PAs. 3 Considering that the number of pharmaceutical programs that used PAs as primary screening assays was much smaller than those employing target-based assays, the implications are that the former strategy is significantly more successful at producing new drugs.3,5,6 PA-based approaches have been particularly effective in challenging therapeutic areas such as the central nervous system (CNS). Seven of the eight small-molecule new molecular entities for CNS pathologies approved between 1999 and 2008 were discovered using PAs. 3 However, these two drug discovery approaches have unique advantages and disadvantages; therefore, case-by-case evaluation of each new target or disease is necessary.
Pharmaceutical companies such as Lilly, Novartis, and GlaxoSmithKline have championed the renaissance of phenotypic screening. Examples of some of the recently approved CNS first-in-class drugs discovered using PAs include Chantix (varenicline), a drug prescribed for smoking cessation; the antipsychotic Abilify (aripiprazole); Namenda (memantine), prescribed for dementia; and the antiepileptic Inovelon (rufinamide). 3 Out of the four examples mentioned, memantine was identified via in vitro cell-based PAs, varenicline was identified using both cell-based and in vivo PAs, and rufinamide’s anticonvulsive and aripirazole’s antipsychotic properties were tested directly in animal models (in vivo PAs). Therefore, both in vitro and in vivo PAs have been fundamental for the discovery and development of successful CNS drugs.
Williams and Enna7,8 argued in favor of phenotypic screening for CNS therapeutics based on the high attrition rate for small molecules identified using a target-centric drug development process. These authors point out that historically, much of the successful CNS drug development has been an empirical and in many cases serendipitous process. For example, drugs such as diazepam (anxiety), chlorpromazine (schizophrenia), and iproniazide (depression) were all initially developed for other conditions. It was later found, in patients, that these drugs were able to control the conditions for which they are currently used.
The discovery and development of drugs for complex neurodegenerative diseases such as multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), human immunodeficiency virus 1 (HIV-1)–associated neurocognitive disorders (HAND), Parkinson disease (PD), and Alzheimer disease (AD) could benefit from the use of PAs. The inflammation and neurodegeneration seen in these diseases have been linked to the uncontrolled chronic activation of microglial cells9–16; therefore, use of small molecules to block the deleterious effects of these cells could be therapeutic. This article will review both the role of activated microglia in neurodegeneration and the current methodologies to monitor its inhibition for the identification of novel neurotherapeutics.
Microglial Cells and Their Activation
Microglial cells, as the brain-resident macrophages, are one of the key players in the immunity of the CNS. They are distributed throughout the parenchyma and account for approximately 10% to 20% of the total glial cell population in the brain.17,18 These cells were first described in 1932 by Pío del Rio Hortega. 19 Their origin, characteristics, and role under both physiological and pathological conditions have been tirelessly debated since their discovery. However, the general consensus is that microglial cells are derived from primitive yolk sac macrophages that migrate to the brain and become resident cells during early embryo development (E10 to E19 in rodents and between the first and second trimester in humans).20,21
Under normal physiological conditions in a healthy mature brain, microglial cells display surveillance behavior and morphology, exhibiting low cell body mobility and an extensive display of fine processes that are constantly scanning their surroundings.22,23 These cells are sensitive to changes of the brain microenvironment, and as soon as an alteration of homeostasis occurs, activation is triggered. This causes changes in cell shape, behavior, and gene and protein expression, leading to the release of an array of factors that include cytokines (interleukin [IL]–1β, tumor necrosis factor [TNF]–α, IL-6), chemokines (MCP-1), excitatory neurotransmitters (glutamate), complement factors, prostaglandins, and reactive oxygen and nitrogen species (ROS and RNS, respectively). Moreover, activated cells adopt amoeboid morphology, their cellular processes disappear, and their capacity to move, proliferate, and phagocytose increase. Expression levels of membrane receptors and ability to present antigens increase upon activation as well (for an in-depth review of microglia physiology, refer to Kettenmann et al. 24 ).
An acute response of activated microglial cells allows the clearance of the stimulus that originally caused the activation and the repair of the resulting tissue damage. This constitutes a beneficial activation or healthy response designed to effectively reestablish brain homeostasis.25–29 However, when the insults, stresses, or infections cannot be controlled, a prolonged, self-propagating chronic microglial response occurs. Both experimental and epidemiological evidence suggests that this type of response is associated with neurodegenerative diseases, as described in detail below.15,30–32
Activation of microglial cells can be triggered by pathological conditions in vivo or by stimulation with proteins, cytokines, and chemical agents both in vivo and in vitro ( Table 1 ). The most widely used method of triggering microglia activation is the treatment with lipopolysaccharide (LPS), a Gram-negative bacterial immunostimulant that triggers a cascade of proinflammatory events that mimic pathological responses.17,33 Microglial cells, like macrophages and other cells that belong to the innate immunity response, express Toll-like receptors (TLRs), nucleotide-binding oligomerization domain (NOD) proteins (NLRs), and C-type lectin receptors (CLRs) ( Fig. 1 ). These receptors give cells the ability to recognize activating stimuli such as pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs). 34 PAMPs capable of inducing microglia activation include bacterial, fungal, parasitic, and viral molecules such as α- and β-glucan, O-linked mannan, viral RNA and DNA, flagellin, chitin, and microbial cell wall components. DAMPs include molecules not normally found in healthy CNS, such as blood-clotting factors, RNA and DNA released by necrotic cells, phosphatidylserine externalized on apoptotic cells, immunoglobulin-antigen complexes, opsonizing complement, and abnormally folded proteins or aggregates.33,35
Examples of Treatments and Conditions That Induce Microglial Cell Activation In Vitro and In Vivo.
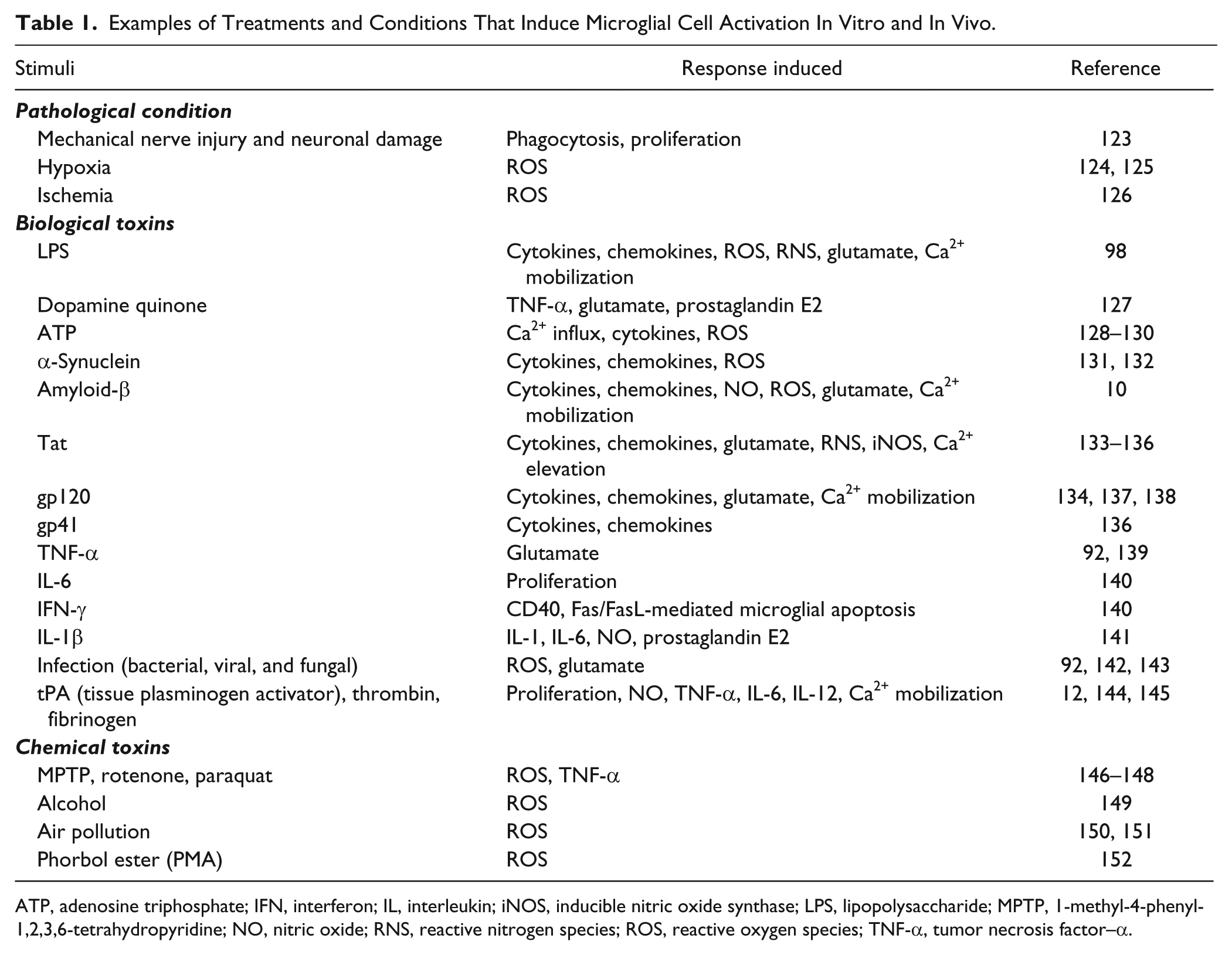
ATP, adenosine triphosphate; IFN, interferon; IL, interleukin; iNOS, inducible nitric oxide synthase; LPS, lipopolysaccharide; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; NO, nitric oxide; RNS, reactive nitrogen species; ROS, reactive oxygen species; TNF-α, tumor necrosis factor–α.
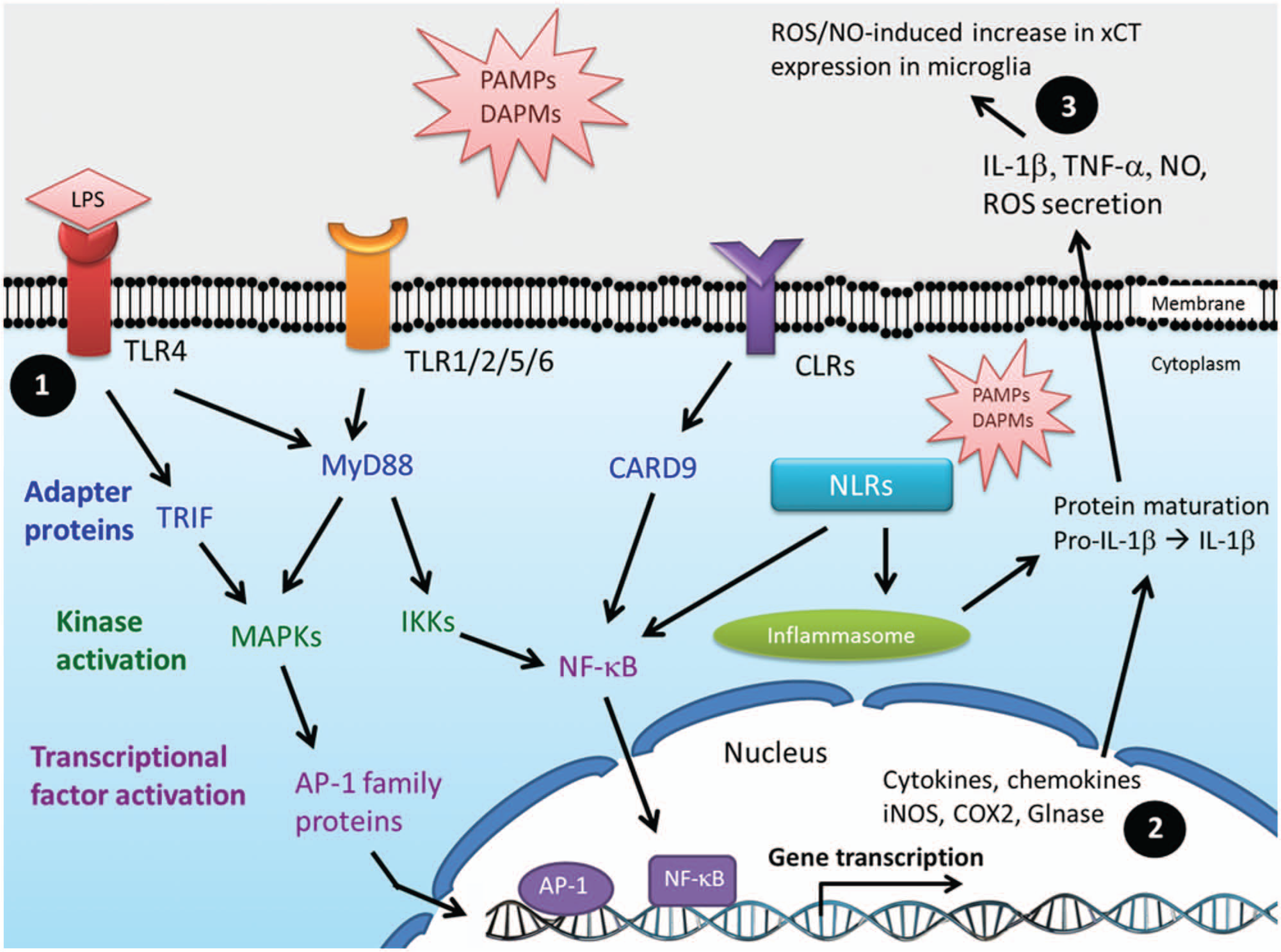
Microglial cell activation signaling pathways. Pathogen-associated and damage-associated molecular patterns (PAMPs and DAMPs, respectively) are recognized by membrane receptors such as Toll-like receptors (TLR1–9), C-type lectin receptors (CLRs), and cytoplasmic sensors like nucleotide-binding oligomerization domain (NOD)–like receptors (NRLs). PAMPs and DAMPs include RNA, DNA, proteins, bacterial and fungal cell wall components, and microbial antigens such as lipopolysaccharides, lipoproteins, peptidoglycan, glycolipids, α- and β-mannan, β-glucan, fucose, and glycosylphosphatidylinositol. (1) Ligand binding to TLRs triggers events dependent on myeloid differentiation primary response protein 88 (MyD88) and TIR domain-containing adaptor protein inducing interferon β (TRIF). MyD88 activates nuclear factor–κB (NF-κB) and mitogen-activated protein kinase (MAPK) pathways, inducing transcriptional activation of proinflammatory genes such as interleukin (IL)–1β, tumor necrosis factor–α (TNF-α), IL-6, inducible nitric oxide synthase (iNOS), and cyclooxygenase 2 (COX2). (2) Glutaminase (Glnase) levels and activity have been shown to be increased during inflammatory responses in a NF-κB–dependent manner. (3) Reactive oxygen species (ROS)/nitric oxide (NO) released by activated microglia induce increased expression levels and activity of cystine/glutamate antiporter (xCT) on nearby microglial cells.
There are at least 13 different TLR family members in humans, 9 of which (TLR1–9) have been reported in microglial cells. 36 In general, ligand binding to TLRs leads to the activation of signaling pathways that involve the cytoplasmic adapter proteins MyD88 and/or TRIF. These events are followed by the activation of multiple kinases such as IRAK1/4, IKKs, and MAPKs and subsequent activation of transcriptional factors nuclear factor–κB (NF-κB) and AP-1. Ultimately, expression of an array of proinflammatory and neurotoxic genes occurs, and levels of cytokines, chemokines, and enzymes such as cyclooxygenase 2 (COX2), inducible nitric oxide synthase (iNOS), 37 and glutaminase 38 increase ( Fig. 1 ). Despite the diversity of stimuli that activate microglial cells ( Table 1 ), there is a convergence of signaling pathways that leads to common steps and similar responses downstream ( Fig. 1 ). Induction of microglial cell activation by LPS treatment is considered a broad overarching approach due to the simultaneous triggering of responses dependent on the two main TLR signaling pathways, TRIF and MyD88. From the biological processes evoked in activated microglia, perhaps cell proliferation and the release of biologically active molecules such as cytokines, chemokines, glutamate, ROS, and RNS are the most amenable to in vitro monitoring and manipulation.
Microglia Activation in Neurodegenerative Disorders
As the brain’s resident macrophage, microglial cells play a key role in protection against exogenous and endogenous insults. Disruption of brain homeostasis caused by physiological or pathological conditions ( Table 1 ) induces microglial cell activation and the release of cytokines, chemokines, and toxins that lead to inflammation. This appears to be a common process in a number of acute and chronic neurodegenerative diseases such as stroke, 39 AD, 30 PD, 14 MS, 40 ALS, 41 Huntington disease, 15 and HAND, 16 inducing or exacerbating neuronal damage. Postmortem analyses of human tissues and animal models of slow progressing diseases such as ALS, PD, and AD have shown neuronal loss concomitantly with increased levels of activated microglia in areas of the brain with lesions.9,11
A well-documented example of the role of microglial cells in neurodegenerative diseases is represented by HAND. HIV-1 crosses the blood-brain barrier (BBB) and infects CD4+ microglial cells, inducing their activation; triggering the release of NO, cytokines, chemokines, and glutamate; upregulating the expression of membrane receptors; and increasing antigen presentation. Infected cells permit virus replication and release of viral particles and toxins such as Tat and gp120 ( Table 1 ), which in turn induce activation of uninfected microglial cells. One of the mechanisms that contributes to neuronal cell death is the overstimulation of NMDA receptors by extracellular glutamate released by activated microglial cells, leading to increased intracellular Ca2+ levels and apoptotic cell death. Furthermore, proinflammatory cytokines and oxidative factors released by HIV-1–infected microglial cells decrease the capacity of oligodendrocytes and astrocytes to uptake extracellular glutamate, thereby altering their neurosupportive/protective role. All these proinflammatory conditions and cytotoxic events exacerbate the neurodegeneration and cognitive decline seen in HIV-infected patients.13,18,24,42
Activated microglial also play a role in ALS pathology. Increased release of NO and superoxide (ROS) from microglia and neuronal cell death are seen in approximately 20% of the patients with the familial form of the disease. These individuals have mutations in the superoxide dismutase 1 (SOD1) gene, which appear to be associated with microglial cell activation mediated by the MyD88 pathway.43–45 Microglial cells are also implicated in AD. Aβ plaques, one of the hallmarks of the disease, have been shown to be surrounded and infiltrated by activated microglia and astrocytes. Moreover, analysis of both animal models and postmortem brains of AD patients shows upregulation of TLR2, 4, and 7, as well as TLR pathway-related genes in microglial cells. 45 Interestingly, a genetic polymorphism of TLR4 (Asp299Gly) that weakens the response to receptor stimulation in microglial cells is associated with a 2.7-fold reduction in the susceptibility to late-onset AD. 46 Finally, a loss-of-function mutation of TLR4 inhibits Aβ-induced microglial cell activation and reduces levels of released proinflammatory factors NO, IL-6, and TNF-α. 47
Interestingly, patients on chronic nonsteroidal anti-inflammatory drugs (NSAIDs) have a lower incidence of AD and show improved performance in cognitive function tests. 48 Moreover, a delayed onset of AD has been documented for twins and siblings on anti-inflammatory drugs.49,50 Therefore, both clinical and epidemiological evidence suggest that anti-inflammatory drugs can delay the onset of neurodegenerative disorders. However, it is important to mention two points of debate. First, not all the anti-inflammatory clinical trials have resulted in protection against disease such as AD and ALS.51–60 And second, evidence seems to indicate that early rather than late anti-inflammatory intervention in terms of disease progression might be crucial for therapeutic efficacy. 61 These two points highlight the complexity of neurotherapeutics and the challenges that lie ahead in drug discovery. In summary, there is abundant literature supporting the role of activated microglial cells in neurodegenerative diseases; therefore, a reasonable therapeutic approach could involve the neutralization of the harmful proinflammatory responses of microglia.
Assessing Microglial Activation
The most frequently used methods for in vitro activation of microglial cells are shown in Table 1 . Treatment with LPS is by far the most employed activation strategy, and despite the complexity of the signaling processes ( Fig. 1 ), the responses that LPS and other stimuli trigger are reasonably well understood. This has allowed the establishment of methodologies to monitor microglial activation both in vitro and in vivo. 18 Table 2 compiles the most widely used in vitro microglial cell activation assays.
Commonly Used Methods to Monitor Microglia Activation.
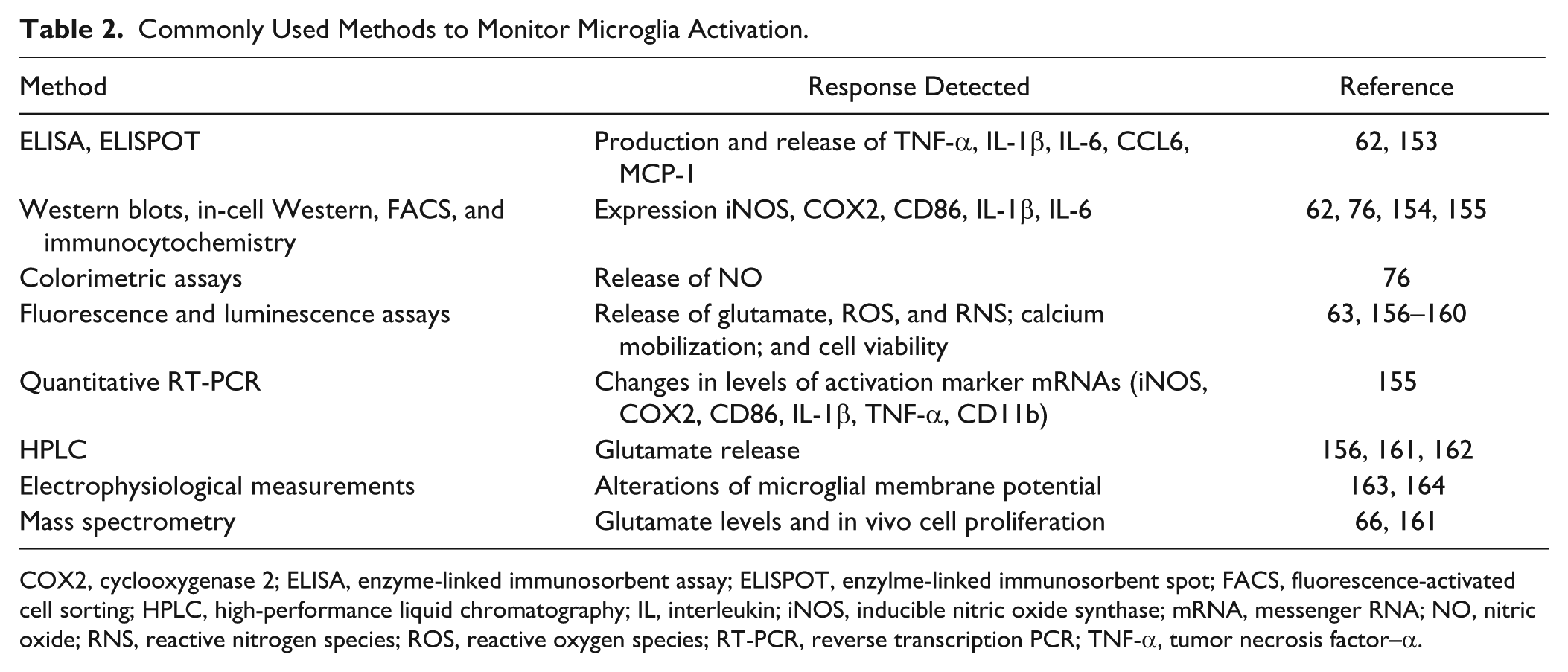
COX2, cyclooxygenase 2; ELISA, enzyme-linked immunosorbent assay; ELISPOT, enzylme-linked immunosorbent spot; FACS, fluorescence-activated cell sorting; HPLC, high-performance liquid chromatography; IL, interleukin; iNOS, inducible nitric oxide synthase; mRNA, messenger RNA; NO, nitric oxide; RNS, reactive nitrogen species; ROS, reactive oxygen species; RT-PCR, reverse transcription PCR; TNF-α, tumor necrosis factor–α.
The most common way of monitoring microglial cell activation is the determination of changes in extracellular levels of cytokines, chemokines, or nitric oxide (NO). There is a broad selection of commercially available cytokine and chemokine enzyme-linked immunosorbent assay (ELISA) kits rendering the detection of TNF-α, IL-6, IL-1β, and MCP-1 a simple, reproducible, and relatively inexpensive process. 62 The diazotization assay (Griess reaction) is one of the quickest, most widely used, and inexpensive methods to estimate extracellular NO levels in biological samples. This assay measures NO2− (nitrite) derived from NO upon reaction with O2. In general, levels of NO2− correlate well with NO levels. For a detailed review on alternative strategies to detect this metabolite, refer to Hetrick and Shoenfisch. 63
One aspect of microglial cell activation that is often undervalued is the change in proliferation rate, an important mechanism of the cellular response implicated in either exacerbation or amelioration of neurodegeneration.64,65 Shankaran et al. 66 developed an elegant mass spectrometry–based method to determine in vivo microglial proliferation rates. By giving 2H2O to mice treated with or without LPS, the authors were able to label the DNA of proliferating cells. Brains were harvested at different time points, and microglial cells were isolated by cell sorting. DNA purification followed by enzymatic hydrolysis, purine derivatization, and mass spectrometry analysis allowed determination of deuterium incorporation into DNA as a function of time, allowing estimation of the percentage of new microglial cells generated as a consequence of LPS-induced activation.
Several of the methods mentioned in Table 2 are routinely used in basic research studies of microglial cell activation; however, PA development can equally benefit from these methodologies. For example, quantitative reverse transcription PCR (qRT-PCR) for high-throughput screening (HTS) has been used to determine the effects of small molecules on messenger RNA (mRNA) levels of a component in a pathway of interest. Due to lower reagent costs, the use of liquid-handling systems, and the miniaturization of reactions, such HTS assays are now cost-effective, rapid, and robust. 67 Since microglial cell activation induces changes in gene expression of proteins such as COX2, iNOS, IL-1R, SOCS3, and CD86, qRT-PCR could be an efficient way to determine if small molecules block activation responses. 68 Ultimately, it is likely that the number of strategies to monitor activated microglial cell phenotypes and functions ( Table 2 ) will only continue to grow, making these assays more accessible, inexpensive, robust, and HTS adaptable.
Microglia Activation Assays
Primary Phenotypic Screening
Use of cell-based assays to identify small-molecule inhibitors of microglial cell activation permits simultaneous probing of multiple targets without bias ( Fig. 1 ). For example, a decrease in the levels of a toxin released by activated microglia could be due to a variety of events such as direct inhibition of the enzyme responsible for toxin production, inhibition of the toxin release pathway, increase in enzyme or toxin degradation, inhibition of enzyme transcription, or translation, blockade of posttranslational modifications, or protein-protein interactions required for enzyme activity.69–74 It is also possible that compound efficacy could be achieved only when multiple pathways or targets are engaged simultaneously. 75 Hence, the power of PAs in primary screenings is underscored in the case of complex and not yet fully understood biological processes and diseases. Figure 2 depicts the basic steps involved in conducting microglial activation PAs.
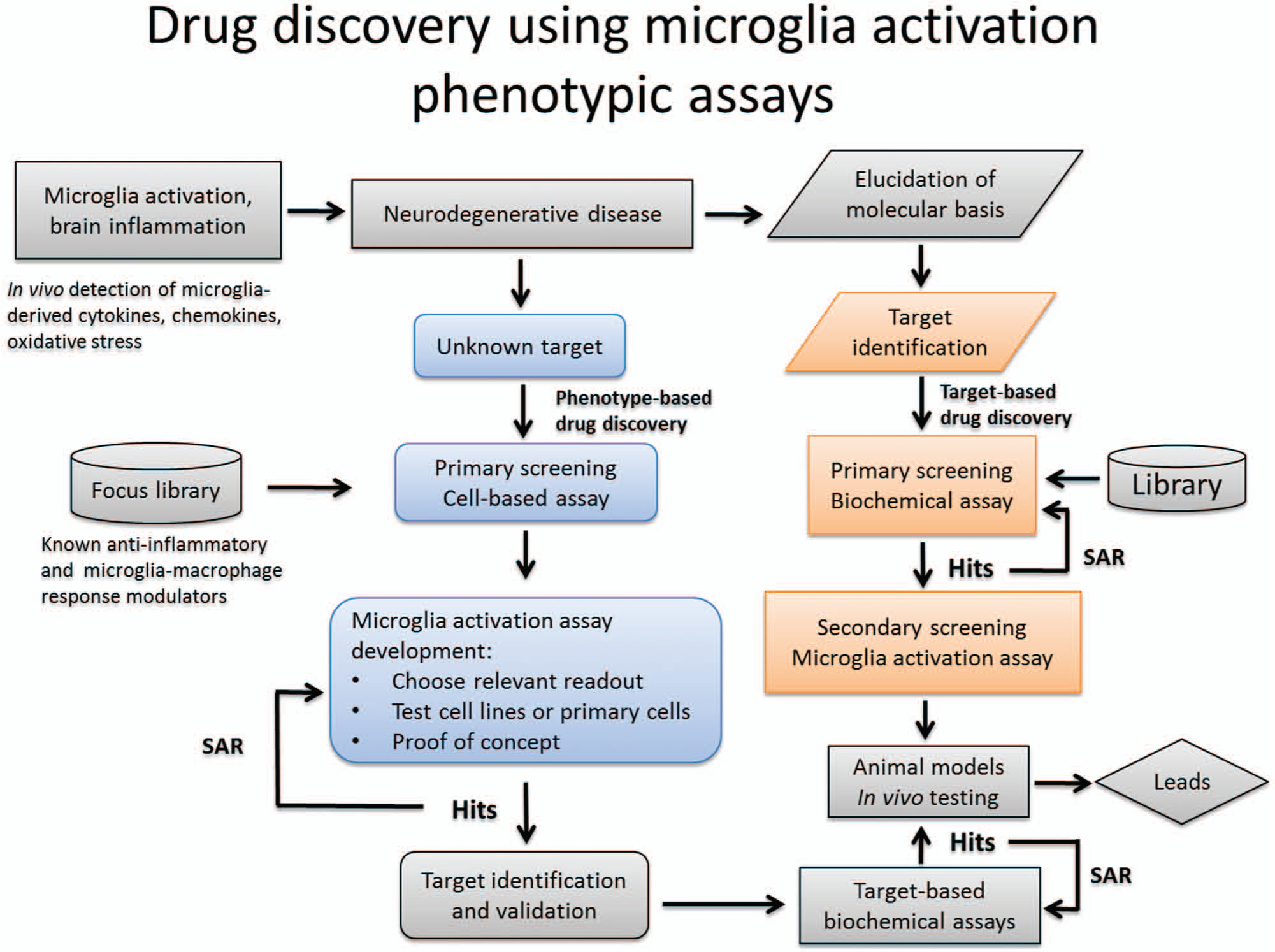
Schematic representation of work flow for primary and secondary phenotypic assay screening strategies based on microglial activation. SAR, structure-activity relationship.
Both immortalized cell lines and primary microglia have been used in PAs.76,77 The most widely used rodent cell lines are BV-2, C8-B4, N9, N11, various EOC lines, highly aggressive proliferating immortalized (HAPI) cell line, and MG5.62,78,79 Nagai et al. 80 generated and described the only human immortalized microglial cell line (HMO6) with a phenotype closely related to primary microglia. A human cell line would be preferred for neurotherapeutic studies; however, thus far, only a few groups have used these cells, as reflected by the sparse literature, and due to commercial licensing restrictions, no wide distribution of the cell line is possible.
All these cell lines retain different degrees of the morphological, phenotypical, and functional properties seen in freshly isolated primary microglia. The most popular of those cell lines, BV-2, was generated in 1990 by viral transformation with v-raf/v-myc of murine neonatal microglial cells. 81 Perhaps due to their ease of growth, maintenance, and use, BV-2 are the preferred cells for in vitro assays. LPS stimulation of these cells causes release of cytokines, RNS, ROS, and glutamate with a similar but slightly reduced response as compared with primary microglia, particularly in the case of glutamate production. 62 Nonetheless, there is abundant literature demonstrating that these cells can be used to study activation induced by various stimuli using PAs such as cytokine ELISA or qRT-PCR and NO determination with Griess reagent.62,82 Figure 3A shows modulation of LPS-induced TNF-α levels in BV-2 cells by the flavonoids apigenin and fisetin.
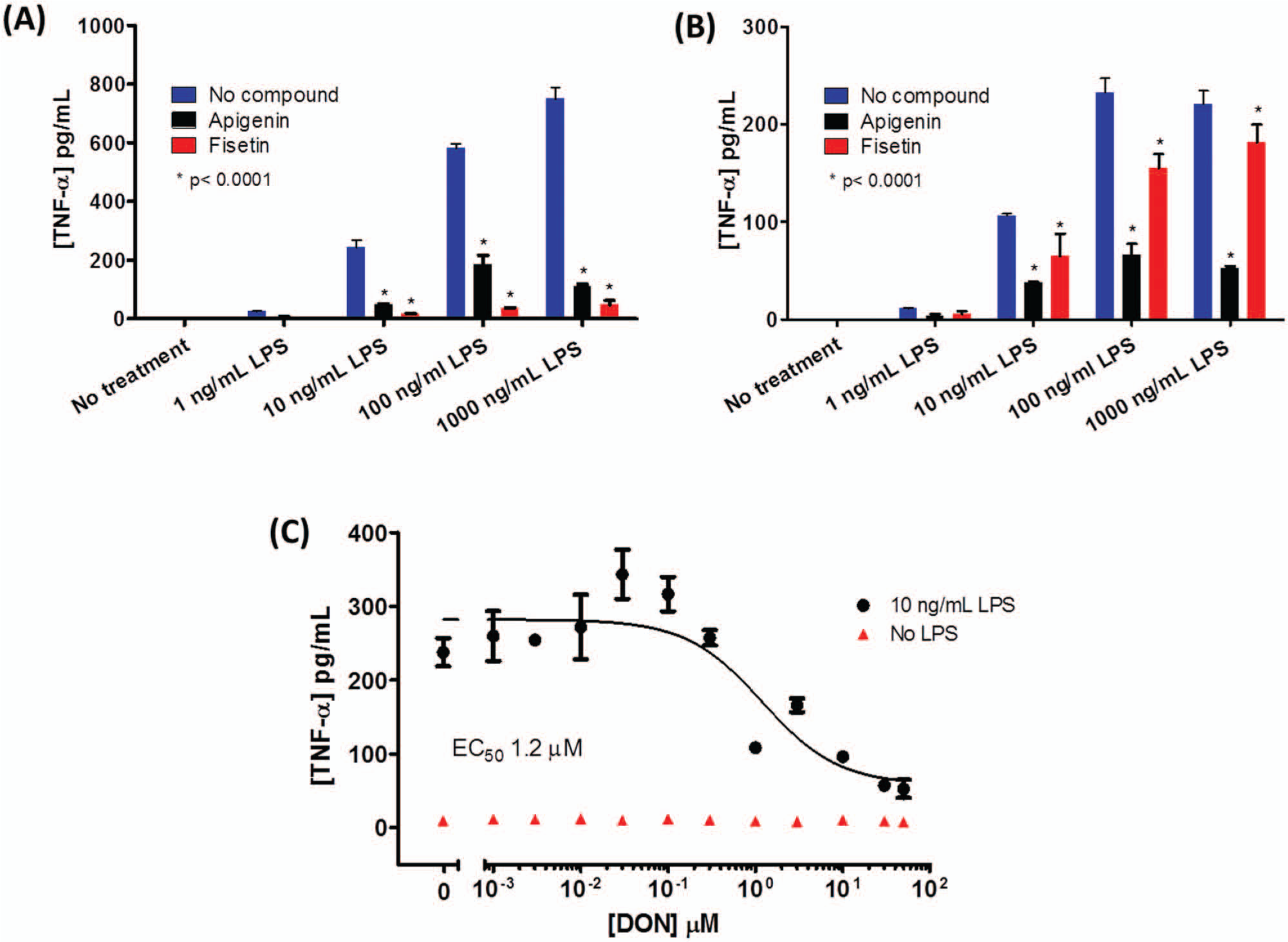
Modulation of tumor necrosis factor–α (TNF-α) release from microglial cell lines. (
Another cell line that has been successfully used is the C8-B4. This is a spontaneously transformed mouse microglial cell line capable of producing cytokines, NO, and glutamate. 83 Figure 3B , C shows how LPS-induced TNF-α release can also be modulated by apigenin and fisetin, as well as the glutaminase inhibitor 6-diazo-5-oxo-L-norleucine (DON). Glutaminase is an enzyme that produces glutamate by catalyzing the deamination reaction of glutamine; it is believed to play a role in HAND and MS38,84 ( Fig. 1 ). Induction in expression of this enzyme has been linked to the MyD88 pathway and NF-κB transcriptional activity.38,85,86 The rest of the microglial cell lines mentioned have not been well characterized, although production of various cytokines and/or NO has been confirmed for most of them.87–90
Experimental evidence shows that compared with cell lines, primary microglial cells more closely resemble both the phenotype and the stimulus responses of microglial cells in vivo.
79
The simplest and most inexpensive method of primary microglial isolation (>95% purity) consists of establishing a confluent mixed glial culture from the brains of neonate rodents. Isolation of the microglia can be accomplished by gentle shaking of the flask containing the cells and collecting the detached cells.
91
Levels of extracellular glutamate released by mouse or rat primary microglial cells can be determined using an assay that consists of two reactions, one catalyzed by glutamate oxidase and the following one by horseradish peroxidase (HRP). In the presence of Amplex Red, these reactions generate the fluorescent product resorufin.
Figure 4
shows how it is possible to modulate in vitro the levels of glutamate released from rat primary microglia using the flavonoids apigenin and fisetin, the tetracycline derivative minocycline (
Fig. 4A
), and a cystine/glutamate antiporter (xCT) inhibitor, erastin (
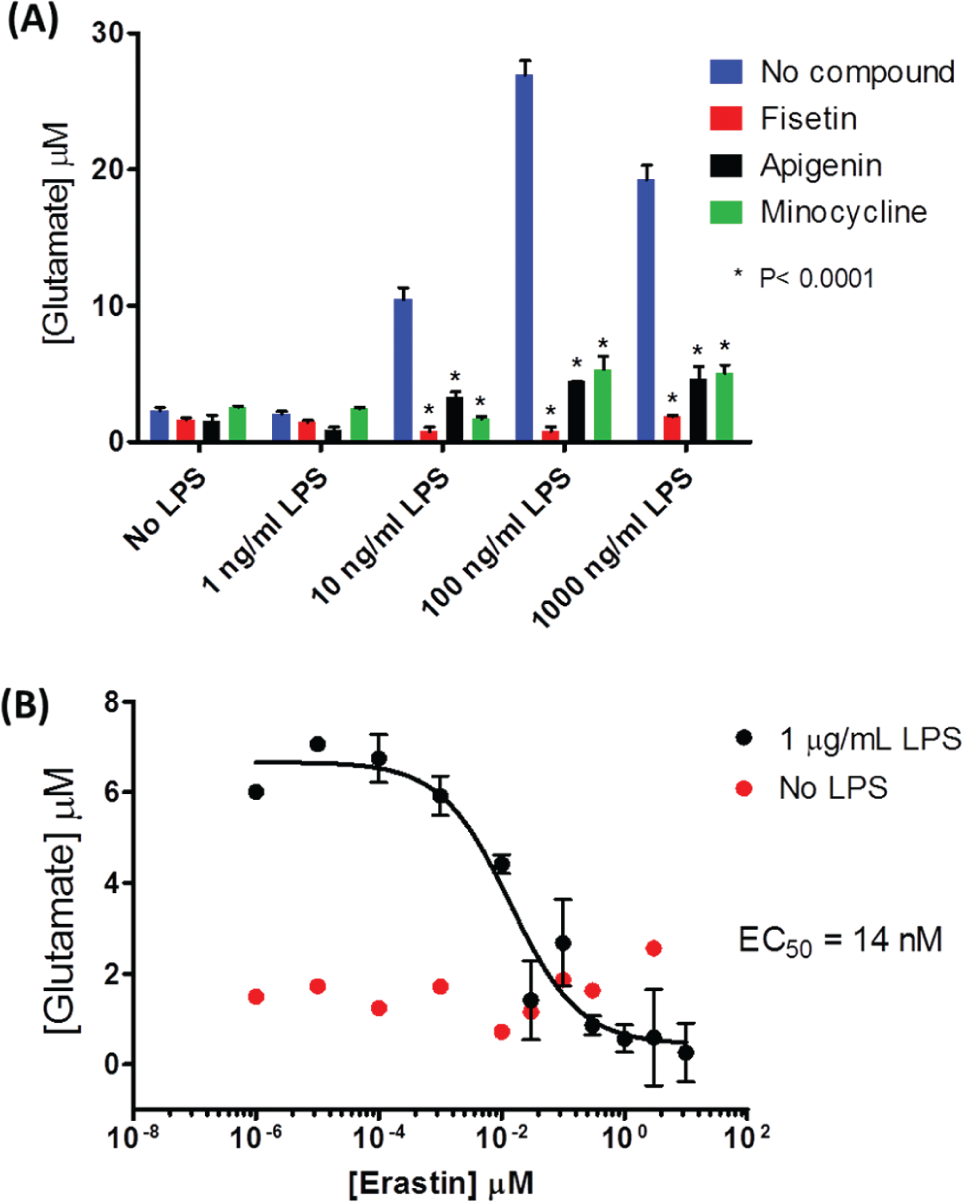
Modulation of lipopolysaccharide (LPS)–induced glutamate levels in rat primary microglia-conditioned media. (
Recently, it has been possible to produce microglial cells from stem cells using a modified neuronal differentiation method.97–99 From a pathophysiological point of view, these microglial cells are more relevant than immortalized cell lines due to their similarity to freshly isolated primary microglia, essentially displaying undistinguishable morphology, functions, and cellular markers. In addition, a virtually unlimited supply of these cells could be generated by in vitro proliferation, eliminating the need to euthanize large numbers of animals and making achievable the HTS of thousands of compounds. Despite advances in the development of protocols for stem cell–derived microglial cell generation, access to these cells, technology, and expertise is still limited.
The mass spectrometry–based method developed by Shankaran et al. 66 to determine microglial cell proliferation rates previously described has been used as a primary screen PA to test a panel of approved drugs with pleiotropic activities in the search of compounds capable of inhibiting in vivo LPS-induced microglial cell proliferation and neuroinflammation. This strategy allowed the identification of isotretinoin as an antiproliferative compound that was also shown to delay clinical symptoms in the experimental autoimmune encephalomyelitis (EAE) model.
To date, efforts to find compounds capable of inhibiting microglial cell activation, including the few HTS campaigns carried out so far, have yielded a set of drugs, natural products, and synthetic derivatives that exhibited anti-neuroinflammatory properties. These compounds have been identified using nitrite assays, cytokine ELISAs, and/or monitoring cytokine mRNA levels in microglial cell lines (BV-2 cells mostly) activated with stimuli such as LPS, Aβ, or necrotic neuronal cells. Some of the identified compounds include nonsteroidal anti-inflammatory drugs (NSAIDs), 48 dexamethasone, pentoxifylline, 100 tetracycline derivatives (minocycline),101,102 flavonoids (apigenin, fisetin, luteolin), 103 extracts of ginger, 104 tetrandrine from Stephania tetrandra (Menispermaceae plant) acting via NF-κB inhibition, 105 3-amino-6-phenyl-pyridazine derivatives inhibitors of protein kinases,76,106 KT-15073 and KT-15087 causing NF-κB and MAPK inhibition, 77 senkyunolide A and Z-ligustilide from Ligusticum chuanxiong (traditional Chinese herbal medicine), 107 cannabinoids, 108 and triamcinolone acetonide and amcinonide. 109 Once a compound has been identified in a primary screen as an inhibitor of microglial cell activation, it is imperative to show if this inhibition is accompanied by neuroprotective effects. Assays with microglial/neuronal cell co-cultures have shown the neuroprotective properties of KT-15073, KT-15087, apigenin, luteolin, and minocycline. Further-more, animal models and clinical trials have shown efficacy and tolerability for NSAIDs, pentoxifylline, and mino-cycline.56,77,101–103,110–114
Secondary Screening in Target-Based Drug Discovery
PAs can also play a critical role in target-based drug discovery as confirmatory functional assays for compounds identified by primary screening. If a target is known to be involved in the activation of microglia, a phenotypic assay such as those described above would allow testing the effects of the compounds in a biological context ( Fig. 2 ).
As an example of target-based primary screening, Benicchi et al. 115 described a novel homogeneous time-resolved fluorescence assay to identify small-molecule inhibitors of the TWEAK-Fn14 protein-protein interaction, which is involved in activation of the NF-κB pathway in models of microglia-dependent CNS inflammation. Even though it has not yet been done, this target-based primary assay could be followed by a secondary microglial activation PA to assess the functional efficacy of identified hit compounds.
PAs can also be used to determine the effects of modulation of microglia activation on other cells in the brain by assaying co-cultures of microglial and other cells such as neurons, astrocytes, and oligodendrocytes. For example, to assess if neuronal protection occurs when activation of microglial cells is inhibited, the viability of neurons could be monitored with assays such as lactate dehydrogenase activity, caspase activity, or MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide) in microglia-neuron co-cultures. 116
When experimental and/or epidemiological evidence supports the role of a target in disease pathology, validation of this target can be carried out using PAs with either chemical or genetic probes. Manipulation of the target using small molecules (chemical probes) or genetic approaches such as protein overexpression, gene knockouts, and RNAi (RNA interference) can be used to induce changes in target function or expression levels inducing a loss-of-function or a gain-of-function phenotype. The phenotypic outcome can then be monitored, validating the target’s role in the functional assay system.
Similarly, chemical and genetic approaches are useful in pathway elucidation and unraveling the molecular mechanisms of a disease. An interesting example that illustrates the use of microglial cell activation assays as a tool in pathway building was published by Burguillos et al. 117 In this work, activation of BV-2 cells by LPS was shown by RT-PCR and Western blots to induce increases in expression of iNOS and IKK-β and to produce ROS. Moreover, activation of the key apoptosis executioners, caspase 3 and 7, in the absence of poly(ADP-ribose) polymerase (PARP) cleavage and cell death was required for microglial activation. Downregulation of caspase 3/7 and caspase 8 expression by gene silencing with small interference RNA (siRNA) and inhibition of their enzymatic activity using chemical probes demonstrated reduction of microglial cell activation as monitored via ROS production and iNOS expression. Similarly, the activity of protein kinase C-δ (PKC-δ) and its cleavage by caspase 3/7 were required for microglial activation. Finally, both LPS and MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) treatment of rats and postmortem analysis of brains of AD and PD patients showed microglial activation and caspase reactivity in regions of the brain with lesions. Based on these results, it could be of interest to conduct target-based screening for inhibitors of caspase 8, 3/7, or PKC-δ to control microglia-dependent chronic inflammation in the brain.
Once an active compound has been identified by phenotypic screening, it is important to find its molecular target so that lead optimization can be directed ( Fig. 2 ). Some of the common methods used for target identification include (1) affinity purification of the target with beads coupled to the compound, (2) the use of expression libraries (phage display or bacterial libraries) to identify the protein(s) capable of interacting with the compound, and (3) protein microarrays of full-length expressed recombinant proteins to screen those capable of binding to the compound. For the use of protein microarrays in target identification, readers can refer to the work of MacBeath and Schreiber, 118 in which the authors test three well-known small molecule–target interactions: streptavidin-biotin, anti-digoxigen antibody–digoxigen, and FKBP12-AP1497. A thorough review of these and other strategies to accomplish target identification was done by Hart. 119 Last, it is important to point out that target identification is not strictly required for structure-activity relationship (SAR) studies and that elucidation of a compound’s mechanism of action is not necessary for FDA approval of a drug.3,5,120–122
Challenges and Perspective
Swinney and Anthony 3 looked at the first-in-class new molecular entities approved by the FDA between 1999 and 2008 and found that a shift in drug discovery strategies has occurred from target to phenotype based. In that period, 28 (37%) of the 75 approved drugs were discovered using PAs, in contrast to 17 (23%) discovered using target-based approaches. Moreover, of the 8 CNS small-molecule drugs approved, 7 were discovered using PAs, highlighting the success of this approach in perhaps one of the most challenging therapeutic areas.
Although PAs can have significant utility in drug discovery, it is important to note their limitations. First is the inherent variability of using living cellular systems. Although this can be somewhat minimized by carefully controlling experimental conditions, the assay variability will likely be more significant relative to a biochemical assay with purified proteins. The second concern is that modulation of a response in a PA could be due to the ability of a compound to simultaneously block the activity of multiple targets, making SAR studies for compound optimization challenging.
However, on balance, PAs can aid the early drug discovery process, focusing on compounds that have functional implications in a pathologically relevant biological system. PAs can precede HTS as a means to validate therapeutic targets or to test the capacity of a library of compounds to inhibit a specific biological process. Moreover, PAs can also follow HTS as a tool to confirm lead compounds that are active in a functional cellular assay ( Fig. 2 ). Improved success rates in drug discovery might be imminently achievable if diversification of screening strategies is implemented.
The use of activated microglia PAs has demonstrated that inhibition of targets such as glutaminase, xCT, NF-κB, and MAPKs 101 is correlated with decreased release of toxic factors from activated microglia. Identification of safe and efficacious compounds capable of inhibiting microglial activation, as well as protecting neuronal cells, may provide a novel therapeutic approach for some of the most prevalent neurodegenerative diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research is supported by the National Institute of Mental Health (NIMH), Center for Novel Therapeutics for HIV-Associated Cognitive Disorders (P30 MH075673-06) and the Johns Hopkins Brain Science Institute.