
Abstract
Background:
ADHD is highly prevalent in adolescents. ADHD is characterized by heightened impulsive behavior and is often associated with increased risk-taking behavior in adolescence. Previous research has mostly focused on negative aspects of risk-taking behavior. However, recently two other types of risk-taking behavior have been identified: positive and prosocial risk-taking.
Objective:
Here, we tested whether youth with ADHD are more inclined toward positive and prosocial risk-taking.
Methods:
We assessed the self-reported likelihood of engaging in negative, positive, and prosocial risk-taking in a sample of 50 adolescents with ADHD (Mage = 16.3, SD = 1.18) and 54 typically developing adolescents (Mage = 16.9, SD = 0.73). Regardless of group, we found that positive, prosocial, and negative risk-taking behavior were positively correlated, higher risk-taking in one domain was associated with higher levels of risk-taking in another.
Results:
Crucially, we found that adolescents with ADHD were more likely to engage in prosocial risk-taking behavior compared to typically developing adolescents. We did not find group differences for negative and positive risk-taking behavior.
Conclusion:
Together, these results show a first indication of the upside of risk-taking in ADHD.
Introduction
ADHD is a highly prevalent condition characterized by inattentive, hyperactive, and impulsive behavior, which causes impairment to the individual (American Psychiatric Association, 2013). In many adolescents with ADHD, a substantial part of the impairment is caused by their excessive engagement in risk-taking behaviors. Risk-taking behavior is defined as behavior with outcomes that are both variable and uncertain (Crone et al., 2016; Duell & Steinberg, 2019). Although theoretically this implies that risk-taking behavior can be either beneficial or detrimental, the large majority of research focused on the detrimental, that is, negative, aspects of risk-taking behavior. Research has shown that adolescents with ADHD engage in more negative risk-taking behavior, such as substance abuse and criminal behavior (see Pollak et al., 2019 for an overview), compared to their typically developing peers. Recently two other types of risk-taking behavior were identified: positive (Duell & Steinberg, 2019) and prosocial risk-taking behavior (Do et al., 2017). These types of risk-taking behavior have not been tested in an ADHD population and it is currently unknown whether adolescents with ADHD are also more likely to engage in positive and prosocial risk-taking behavior. In this study, we test differences in negative, positive, and prosocial risk-taking behavior in adolescents with ADHD and typically developing adolescents.
In general, adolescents take more risks than adults (Defoe et al., 2015). At the root of this phenomenon, developmental research suggests an imbalance between the relatively early development of affective reward-oriented brain regions and the later development of cognitive control-oriented brain regions (Steinberg et al., 2018). This imbalance is suggested to be even larger in adolescents with ADHD (Dekkers et al., 2022). Indeed, ADHD is often linked to heightened reward sensitivity and lower cognitive control (Sonuga-Barke, 2002). Adolescents with ADHD are therefore particularly prone to risk-taking behavior. An extensive body of research demonstrates that they disproportionately often engage in many different expressions of risk-taking behavior, such as risky traffic behavior, substance abuse and dependence, gambling and other financial risk-taking behaviors, sexual risk-taking behavior, criminal behavior, and food-related risk-taking behavior (Pollak et al., 2023). Higher levels of negative risk-taking behavior are potentially driven by impulsivity and proneness to boredom (Kılıç et al., 2020; Romer, 2010), traits that are often observed in ADHD populations (Malkovsky et al., 2012; Patros et al., 2016).
However, the tendency toward risk-taking behavior could also have an opposite, more positive side as some risk-taking behaviors are legal, socially acceptable, and have the potential to benefit the well-being of self and others (Duell & Steinberg, 2019). Risky behavior that is potentially beneficial for the well-being of the risk-takers themselves is regarded as positive risk-taking (Duell & Steinberg, 2019). Examples of positive risk-taking behaviors are asking others on a date, trying out a new hobby, and talking with strangers. Positive risk-taking is related to extraversion and sensation seeking (Patterson et al., 2019). Where positive risk-taking behavior is defined as risk-taking for oneself, prosocial risk-taking is defined as taking risks, either social, health, or financial risks, for someone else (Do et al., 2017). Examples of prosocial risk-taking are standing up for someone being bullied or protesting against climate change. Literature suggests that prosocial risk-taking is related to higher levels of prosocial behavior, empathy, and sensation seeking (Armstrong-Carter et al., 2021).
The current study tested differences in how adolescents with ADHD and their typically developing peers differ in the self-reported likelihood of engaging in negative, positive, and prosocial risk-taking behavior. Likelihood of negative risk-taking was measured using by the Health/Safety subscale of the Domain Specific Risk-Taking (DOSPERT) questionnaire for adolescents. As there were no questionnaires available to assess the likelihood of positive and prosocial risk-taking behavior, we designed a positive and prosocial risk-taking questionnaire for this study. These questionnaires were designed to be similar to the DOSPERT to ensure optimal alignment between the measures. Our first and primary aim was to test whether adolescents with ADHD were more likely to engage in negative, positive, and prosocial risk-taking behavior compared to their peers without ADHD. Many prosocial and positive risk-taking behaviors are expressions of some of the most frequently reported positive characteristics of individuals with ADHD, such as spontaneity, open-mindedness, and an openness to challenges and new experiences (Schippers et al., 2022). Therefore, we hypothesized a positive correlation between all three manifestations of risk-taking behavior, suggesting that adolescents with ADHD are more likely to engage in prosocial and positive risk-taking behavior than their peers without ADHD.
As a secondary aim, we investigated whether negative, positive, and prosocial risk-taking behavior have similar or distinct correlates. To assess whether risk-taking behavior is a general concept, unrelated to the type of risk-taking, we tested whether negative, positive, and prosocial risk-taking behavior were correlated. We expected that all risk-taking behaviors were positively correlated in both groups. Additionally, we tested whether each of the three types of risk-taking behavior was related to distinct correlates. We assessed impulsivity, boredom proneness, empathy, and prosocial behavior. Given the relatively new research topics positive and prosocial risk-taking behavior, this hypothesis was pre-registered as an exploratory hypothesis and no expectations regarding the direction of the effects were formulated. Together, these analyses are a first investigation of more positive sides of risk-taking in adolescents with ADHD and generally give insight into the overlapping and distinct aspects of negative, positive and prosocial risk-taking behavior.
Methods
Participants
In total, 51 adolescents with ADHD and 56 typically developing adolescents aged 14 to 18 years participated. One adolescent with ADHD and two adolescents from the typically developing group were excluded as they did not finish most of the questionnaires. The final sample consisted of 50 adolescents in the ADHD group (58% girls, 38% boys, 4% identified as “other,” Mage = 16.3, SD = 1.18) and 54 adolescents in the typically developing group (46% girls, 54% boys, Mage = 16.9, SD = 0.73). Adolescents with ADHD were recruited at Dokter Bosman, a specialized youth mental healthcare institution in The Netherlands. All adolescents in the ADHD group were diagnosed by their clinicians following evidence-based practice guidelines, which means that semi-structured interviews were used and multiple informants reported on the adolescents’ behavior in multiple settings. Typically developing (TD) adolescents were recruited at schools, using flyers and social media. Participants in the TD group were part of a larger study investigating risk-taking behavior in adolescence. The presence of any officially diagnosed mental disorder, including ADHD, was an exclusion criterion for the TD group. All adolescents provided active informed consent. The study was approved by the institutional review board of the University of Amsterdam (for the ADHD group) and the Vrije Universiteit Amsterdam (for the TD group).
Materials
Demographics
Demographic information was obtained via a brief online questionnaire asking adolescents their age, gender, and education level. We tested whether groups differed in terms of age, gender distribution, and education level. A two-sample t-test indicated that participants in the ADHD group were significantly younger than participants in the TD group (t(80) = −3.04, p = .003, d = 0.61). As age is related to risk-taking behavior, we tested whether inclusion of age in our analyses changed our results. Inclusion of age in our analyses did not change the results, also see “Data analytic approach.” A chi-squared test indicated no differences in gender distribution across the two groups (χ2 (2) = 4.23, p = .12). Education level was significantly higher in the TD group compared to the ADHD group (χ2 (2) = 47.69, p < .001). Education level was not included in the analyses as education level differences are an inherent property of the difference between adolescents with ADHD and TD adolescents (Dennis et al., 2009). Demographic information is reported in Table 1.
Demographic Information and Descriptive Statistics.
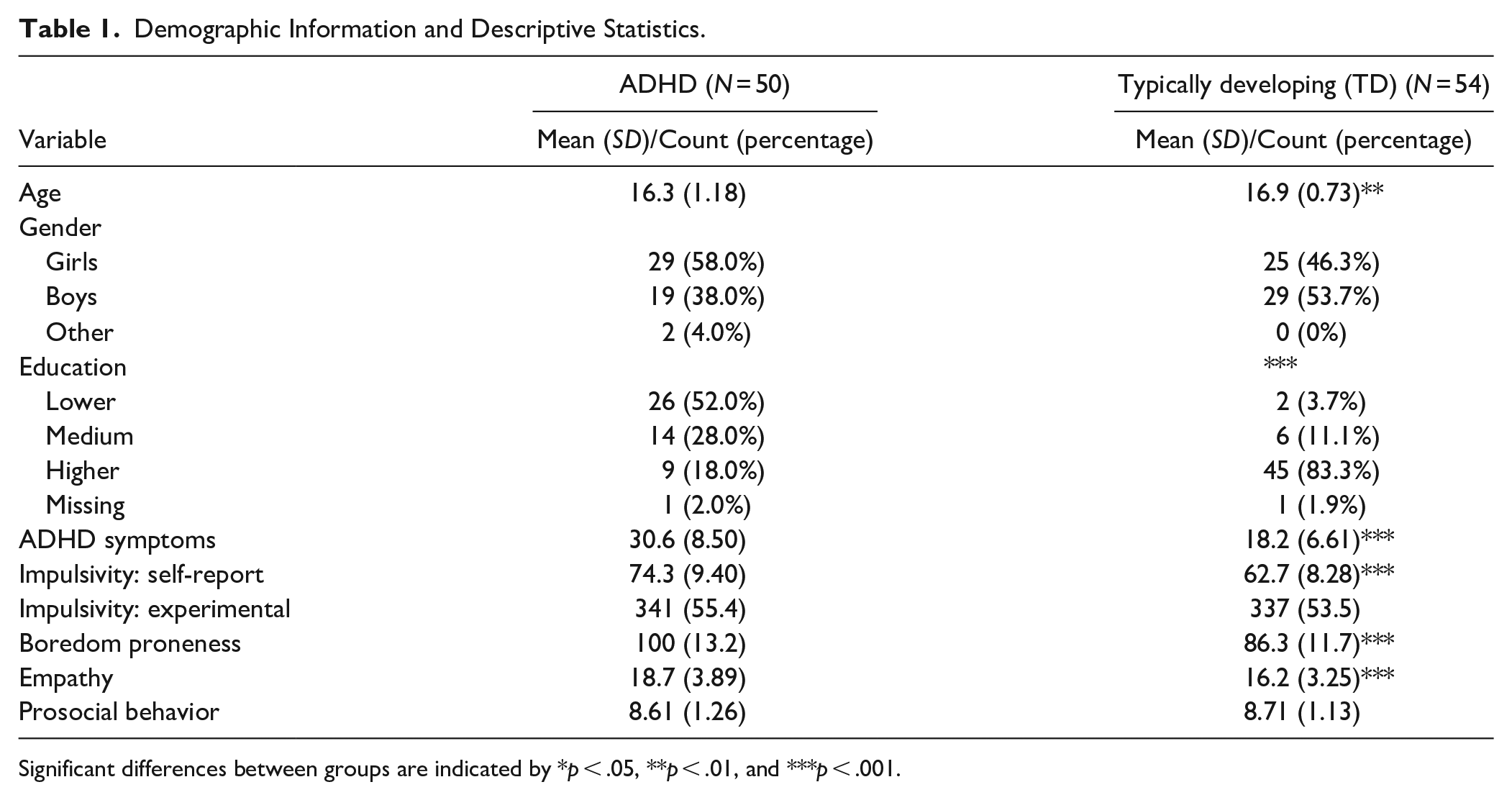
Significant differences between groups are indicated by *p < .05, **p < .01, and ***p < .001.
ADHD Symptoms
All participants completed the Dutch adult ADHD Self-Report Scale (ASRS; Kessler et al., 2005; Kooij & Buitelaar, 1997), which contains 23 items that are answered on a 4-point scale ranging from 0 (“rarely or never”) to 3 (“very often”). Each DSM-5 ADHD symptom was reflected by one item, except for five symptoms which were reflected by two items. For the analyses, these double items were averaged (Kooij et al., 2008). An example of an item is “I get distracted quickly.” The psychometric properties of the ASRS range from α = .72 to .83 (Kooij et al., 2005), and also in the current sample, internal consistency was good to excellent for both groups (ADHD α = .91, TD α = .85). Self-reported ADHD symptoms were higher in the ADHD group compared to the TD group t(88) = 8.09, p < .001, d = 1.6)
Impulsivity: Self-reported
Impulsivity was measured with the adolescent version of the BIS-11 (Barratt Impulsiveness Scale; Barratt, 1965), which is a self-report questionnaire consisting of 30 items. Items are answered on a 4-point scale ranging from 1 (“seldom/never”) to 4 (“almost always”). The BIS-11 is extensively studied, the reported Cronbach’s alpha values ranged from .62 to .83 (for a systematic review, see Vasconcelos et al., 2012). In the current sample, internal consistency was acceptable for the ADHD group and good for the TD group (ADHD α = .56, TD α = .71). BIS-11 scores were higher in the ADHD group compared to the TD group t(94) = 6.58, p < .001, d = 1.32).
Impulsivity: experimental
As an experimental measure of impulsivity, a temporal delay discounting task was used. Temporal delay discounting and the tendency to prefer smaller immediate rewards over larger delayed rewards is related to impulsivity (Barkley, 1997; Critchfield & Kollins, 2001; Green & Myerson, 2004). The delay discounting task included in the present study was previously used by Scheres et al. (2006). In the task, participants were presented with two planes. Each plane carried a load of money. Participants selected one of the planes and received the money carried by that plane. Participants chose between two planes, one plane with a smaller amount of money (2, 4, 6, or 8 cents) that was received immediately, and one plane with a larger amount of money (always 10 cents) that was received after a delay. Money dropped by planes that fly higher takes longer to reach the participants basket. Planes could fly on five different heights representing a delay time of 5, 10, 20, 30, or 60 s. During the instructions they experienced the delay for each of the different heights. Participants were not informed about the exact duration of the delay. All delays were presented for all values of the immediate reward resulting in a total of 40 trials. The outcome measure of the delay discounting task is the total money won during the task: more money indicated lower delay discounting (i.e., lower impulsivity). Money won during the task was paid out to the participants after the test session. We selected this task with delay experienced in real time rather than often used hypothetical delay discounting tasks, as this models real-life scenarios better. Delay discounting scores, that is, amount of money won, did not differ between the groups t(94) = .33, p = .74, d = 0.07).
Boredom Proneness
Proneness to boredom was measured with the sum of four subscales of the Dutch Scale for Boredom Proneness (NSGV; Zondag, 2007): restlessness, concentration, disinterest, and sensation seeking. In total these subscales consist of 22 items answered on a 7-point scale ranging from 1 (“certainly not the case”) to 7 (“certainly the case”). An example of an item is “When I’m in a line, I get irritated quickly.” Internal consistency and congruent validity were adequate (Zondag, 2007). Cronbach’s alpha for the subscales used in this study range from .63 to .82 (Zondag, 2007). In the current sample, internal consistency was good for both groups (ADHD α = .79, TD α = .73). Proneness to boredom was significantly higher in the ADHD group compared to the TD group t(92) = 5.44, p < .001, d = 1.10).
Empathy
Empathy was measured with the Dutch version of the Empathic Concern subscale of the Interpersonal Reactivity Index (IRI; Davis, 1980). Participants responded to seven items (e.g., “I often have tender, concerned feelings for people less fortunate than I”) on a 5-point Likert scale ranging from 0 (“does not describe me at all”) to 4 (“describes me very well”). Previous research indicated good reliability of the IRI: α = .72 and .84 for early and late adolescents, respectively (Hawk et al., 2013). In the current sample, internal consistency was acceptable to good for both groups (ADHD α = .74, TD α = .61). IRI Empathic Concern scores were significantly higher in the ADHD group compared to the TD group t(92) = 3.47, p < .001, d = 0.70).
Prosocial Behavior
Prosocial behavior was measured with the Prosocial subscale of the Dutch self-report version of the SDQ (Strengths and Difficulties Questionnaire; Van Widenfelt et al., 2003) for adolescents. This subscale consists of five items (e.g., “I am helpful if someone is hurt, upset, or feeling ill”), which are answered on a 3-point scale ranging from 0 (“not true”) to 2 “certainly true.” The Cronbach’s alpha value for the SDQ prosocial subscale as reported by youth is .66 (Goodman, 2001). In the current sample, internal consistency was acceptable for both groups (ADHD α = .61, TD α = .53). SDQ Prosocial scores were not significantly different between the two groups t(90) = −0.40, p = .69, d = −0.08).
Negative Risk-taking Behavior
Likelihood of negative risk-taking behavior was measured with the Health/Safety subscale of the adolescent version of the DOSPERT (Blais & Weber, 2006), which consists of eight items (e.g., “Not fastening your seatbelt in the car”), measured on a 7-point Likert scale ranging from 1 (“extremely unlikely”) to 7 (“extremely likely”). The reported Cronbach’s alpha for the risk-taking likelihood Health/Safety subscale was α = .77 (Blankenstein et al., 2024). In the current sample, internal consistency was good for both groups (ADHD α = .62, TD α = .68).
Positive Risk-taking Behavior
Positive risk-taking behavior was measured with the positive risk-taking questionnaire (posRT). The posRT was developed for this study and was based on the DOSPERT (Blais & Weber, 2006). The posRT consists of 13 items, see OSF project https://osf.io/7nax3/ for all items. For each item, the participants were presented with a hypothetical behavior and had to indicate the likelihood of demonstrating this behavior (e.g., “Auditioning for a band or theater group”). All items were answered on a scale ranging from 0 (“extremely unlikely”) to 100 (“extremely likely”). Internal consistency was acceptable to good in both groups (ADHD α = .67, TD α = .77). Convergent validity was investigated by assessing the correlation patterns between positive risk-taking behavior and related constructs. Convergent validity for the posRT was supported by a positive correlation with negative risk-taking behavior (r = .23; p = .013) and the expected absence of correlations with impulsivity (r = −.08; p = .442), prosocial behavior (r = .08; p = .403), and empathy (r = .02; p = .814). Detailed results can be found in the Supplemental Materials.
Prosocial Risk-taking Behavior
Prosocial risk-taking behavior was measured with the Prosocial Risk-Taking (PSRT). The PSRT was developed for this study and was based on the DOSPERT (Blais & Weber, 2006). The questionnaire consists of 13 items, see OSF project https://osf.io/7nax3/ for all items. For each item, the participants were presented with a hypothetical behavior and had to indicate the likelihood of demonstrating this behavior (e.g., “Invite someone you like but who is unpopular to your birthday party”). All items were answered on a scale ranging from 0 (“extremely unlikely”) to 100 (“extremely likely”). Internal consistency of the PSRT was acceptable to good in both groups (ADHD α = .66, TD α = .69). Convergent validity for the PSRT was supported by positive correlations with empathy (r = .34; p < .001), impulsivity (r = .38; p < .001), and negative risk-taking (r = .31; p = .002) that correspond with the literature (Armstrong-Carter et al., 2021; Blankenstein et al., 2020; Eisenberg & Fabes, 1990; Wood et al., 2014). Unexpectedly, prosocial risk-taking behavior did not correlate with prosociality (r = .131; p = .197) as measured by the SDQ prosocial behavior subscale. Detailed results can be found in the Supplemental Materials.
Procedure
After expressing their interest, we informed the adolescents and, in case adolescents were below 16 years old, one of their parents or other legal caretakers about the aim of the study and the procedure. After providing informed consent, we made an appointment with the adolescents to complete all questionnaires and the task. All measures were administered digitally. A research assistant was always available to explain procedures. The session lasted between 40 and 60 min. In addition to the reward for the delay discounting task, all adolescents received 10 euros reimbursement.
Data-analytic Approach
This study was preregistered at AsPredicted (https://aspredicted.org/R9F_XVJ). Chi-square analyses and t-tests were used to compare groups on demographic variables. For all analyses, in case assumptions were violated, non-parametric alternatives were used. We preregistered three main research questions. To test the convergent validity of the newly designed questionnaires for positive and prosocial risk-taking behavior, Pearson’s correlations were performed. The results of these analyses supported convergent validity, as can be read in the Supplemental Materials. Convergent validity for the PSRT was supported by positive correlations with empathy, impulsivity, and negative risk-taking. We did not find the expected positive correlation between prosocial risk-taking behavior and prosociality. Convergent validity for the posRT was supported by a positive correlation with negative risk-taking and the expected absence of correlations with impulsivity, prosocial behavior, and empathy. This allowed us to use the questionnaire to study prosocial and positive risk-taking in ADHD and typically developing adolescents respectively.
Research Question 1
Do adolescents with ADHD and typically developing adolescents differ in negative (1a), positive (1b), and prosocial (1c) risk-taking? We tested research questions 1a, 1b, and 1c using a between subjects t-test comparing the ADHD and TD groups. An a priori power analysis was preregistered and conducted using G*Power (version 3.1) to determine the required sample size for an independent samples t-test, assuming a medium effect size (d = 0.5), a significance level of ⍺ = .05, and a desired power of 1 − ß = .80. The analysis indicated that a total sample size of 102 participants (51 per group) would be required. Participants in the ADHD group were significantly younger than the participants in the control group (see demographics section). We did not preregister to include age as a covariate in our analyses. However, as age is significantly related to risk-taking behavior, we also performed our primary analyses for RQ1 with inclusion of age. Including age as a covariate did not change the results. We follow our preregistration and report analyses without inclusion of age in the results section. All analyses with inclusion of age are reported in the Supplemental Materials available on OSF (https://osf.io/7nax3/).
Research Question 2
Is positive risk-taking in adolescents related to negative risk-taking? We tested research question 2 with a regression analysis with negative risk-taking as the independent variable and positive risk-taking as the dependent variable. We also tested the interaction with group (ADHD vs. TD) by including group as the interaction term.
Research Question 3
Which factors are related to negative, positive, and prosocial risk-taking? For both groups separately, we tested which factors were related to each of the different types of risk-taking behavior. The independent variables were impulsivity (BIS11 scores), delay discounting performance on the task, empathy (IRI scores), boredom proneness, and prosocial behavior. We corrected for multiple comparisons using the Benjamini-Hochberg correction. As preregistered, both uncorrected and corrected p-values are reported. Sample size was based on the power analysis for the between-subjects t-tests for RQ1. To assess the sensitivity of the regression analyses, we performed a sensitivity analysis using G*Power. A sensitivity analysis indicates the minimum effect size that can be detected at 80% power. The sensitivity for the regression analysis is .29, indicating that we can detect effect sizes of f 2 = 0.29 which is a large effect size. Zero-order correlations for all variables are reported in Figure 1.
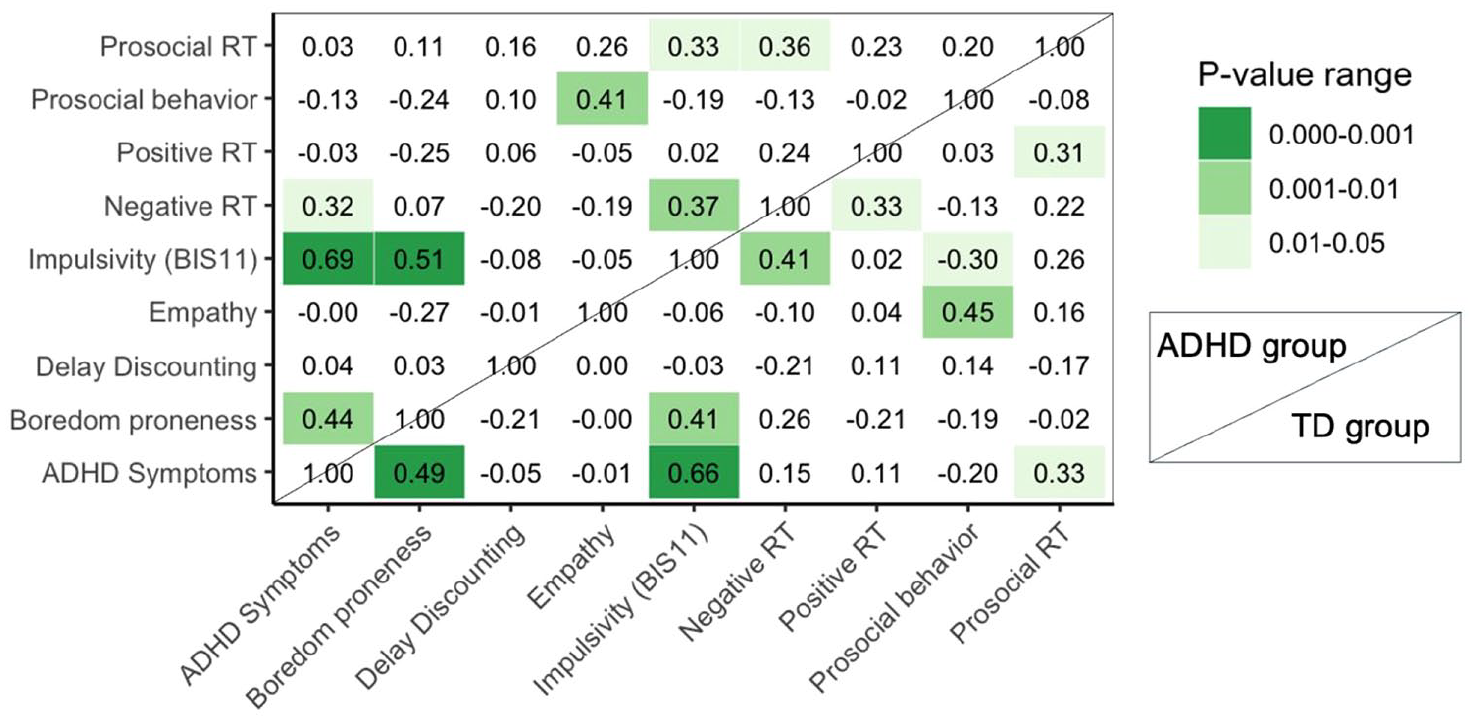
Pearson correlations and significance of correlations between all measures in the ADHD group (above diagonal) and TD group (below diagonal).
Outliers and Missing Data
None of the questionnaires had missing items. Outliers were detected by Median Absolute Deviation (MAD; Leys et al., 2013), using a moderately conservative threshold of 2.5. Detected outliers were removed for DOSPERT (one outlier), ADHD self-report (two outliers), BIS-11 (two outliers), IRI scores (two outliers), boredom proneness (two outliers), positive risk-taking (five outliers), and SDQ scores (six outliers). Analyses were performed with and without outliers. We report analyses without outliers in the manuscript and analyses including outliers in the Supplemental Materials, see https://osf.io/7nax3/. We explicitly indicated when findings differed in terms of statistical significance. We preregistered to exclude data from participants who did not finish the delay discounting task. However, as we experienced some technical difficulties with the delay discounting task, which led to more missing data than expected, we decided to include questionnaire data for participants with missing data on the delay discounting task.
Results
Main research questions, analyses, and exclusion criteria were pre-registered (see Methods section). Any deviations from our pre-registration are indicated when applicable.
Group Differences in Negative Risk-taking Behavior
First, we tested whether negative risk-taking behavior differed between the ADHD group and the TD group (pre-registered RQ1a). We used the Health/Safety subscale of the DOSPERT questionnaire as the dependent variable. There was no significant difference in risk-taking in negative risk-taking behavior between the ADHD (M = 31.1, SD = 9.2) and TD group (M = 29.6, SD = 8.2; t(96) = 0.85, p = .397, d = 0.17).
Group Differences in Positive Risk-taking Behavior
Second, we also did not find significant differences in positive risk-taking domain between the ADHD (M = 60.6, SD = 11.8) and TD group (M = 64.2, SD = 10.5; t(92) = −1.62, p = .109, d = 0.33; pre-registered RQ1b).
Group Differences in Prosocial Risk-taking Behavior
Third, we found that adolescents with ADHD report to be more likely to engage in prosocial risk-taking behavior than TD adolescents (ADHD group: M = 65.3, SD = 12.0; TD group: M = 59.2, SD = 11.1; (t(98) = 2.68, p = .009, d = 0.53, see Figure 2; pre-registered RQ1c).
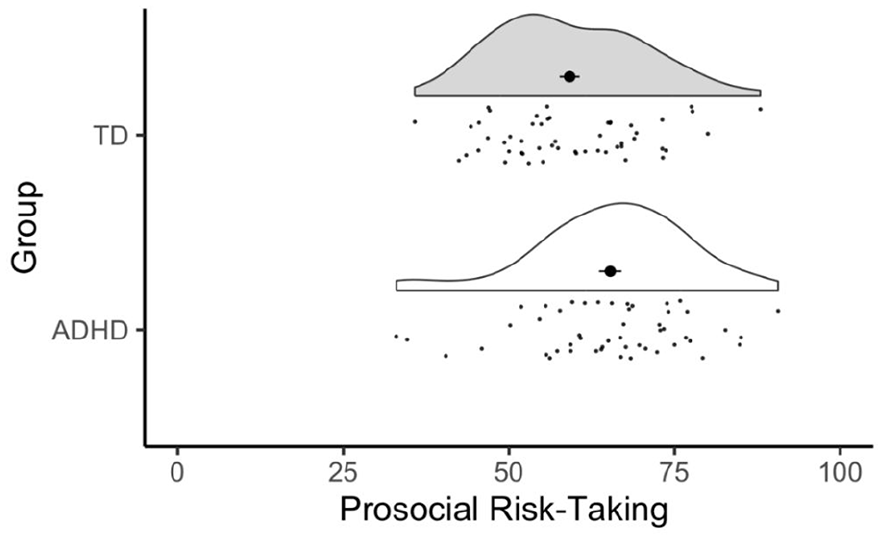
Distribution of prosocial risk-taking behaviors in typically developing (TD) adolescents and adolescents with ADHD. Adolescents with ADHD reported significantly higher likelihood of engaging in prosocial risk-taking behavior compared to the TD group.
Is Positive Risk-taking in Adolescents With and Without ADHD Related to Negative Risk-taking?
We pre-registered to test the relationship between positive and negative risk-taking using a regression analysis (RQ2). We found a significant positive association between positive and negative risk-taking across the full sample of adolescents (b = 0.33, β = .26, t(94) = 2.62, p = .010). Additionally, we tested whether the relationship between positive and negative risk-taking differed between groups using a multiple regression analysis with positive risk-taking as the dependent variable and main and interaction effects for negative risk-taking and group. Results showed no significant interaction effect between negative risk-taking and group, indicating that the relationship between different types of risk-taking behavior did not differ between groups (b = 0.10, t(94) = 0.39, p = .698, r2 = .10).
Although not pre-registered, we also tested the relationship between negative and prosocial risk-taking as well as the relationship between positive and prosocial risk-taking. These relationships were tested in the whole group as well as for differences between groups. Results showed significant positive relationships between negative and prosocial risk-taking (b = 0.41, β = .30, t(99) = 3.18, p = .002) as well as positive and prosocial risk-taking (b = 0.21, β = .21, t(95) = 2.12, p = .037). These relationships did not differ per group (all b’s < 0.17, p’s > .489, r2 < .10, see Figure 3).
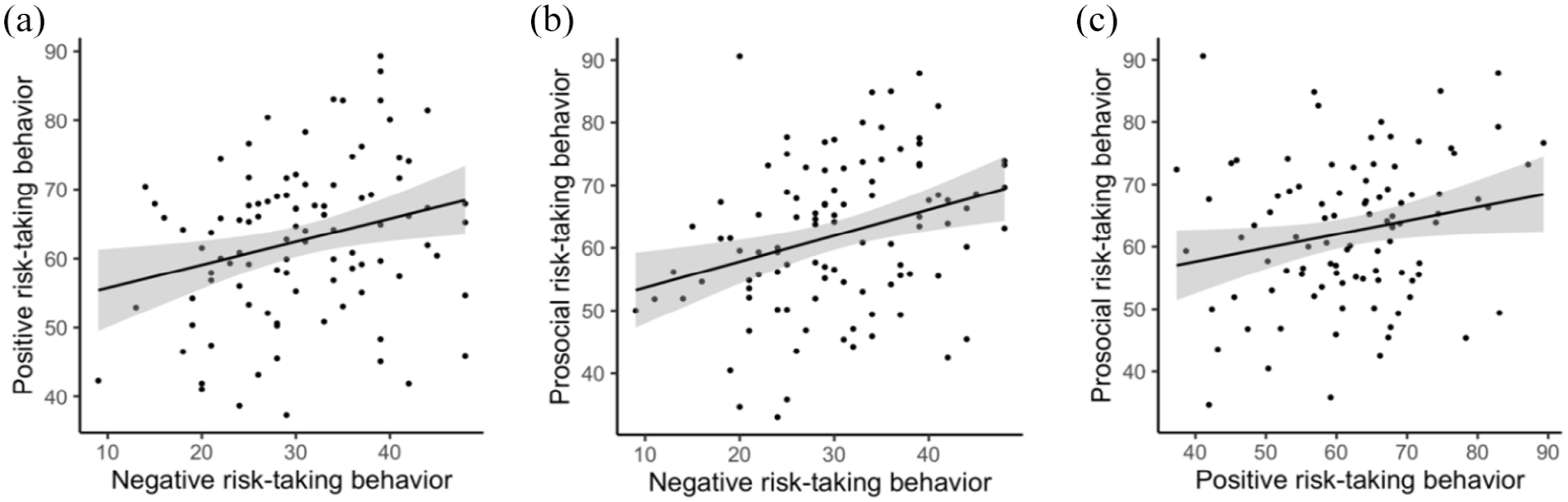
Visualization of the positive relationships between (a) negative and positive risk-taking behavior, (b) negative and prosocial risk-taking behavior, and (c) positive and prosocial risk-taking behavior. All regressions were significant at the p < .05 level. Each panel represents data from the combined TD and ADHD groups as relationships did not differ between the groups.
Which Factors Are Related to Negative/Positive/Prosocial Risk-taking?
Lastly, we tested which factors were related to negative, positive, and prosocial risk-taking behavior. We preregistered three multiple regression analyses per group with empathy, impulsivity, delay discounting, boredom proneness, and prosocial behavior as independent variables (RQ3). Uncorrected and Benjamini-Hochberg corrected p-values are reported. In the TD group impulsivity was positively related to both negative and prosocial risk-taking behavior. Results in a similar direction were found for the ADHD group, but only the relationship between impulsivity and prosocial risk-taking behavior survived the correction for multiple comparisons. All other analyses yielded non-significant results. All results are reported in Table 2.
B-values, Uncorrected, and Corrected p-values for Multiple Regression Models Testing the Relationship Between Negative, Positive, and Prosocial Risk-taking and Impulsivity, Empathy, Prosocial Behavior, Boredom Proneness, and Delay Discounting for the ADHD and Typically Developing (TD) Groups.
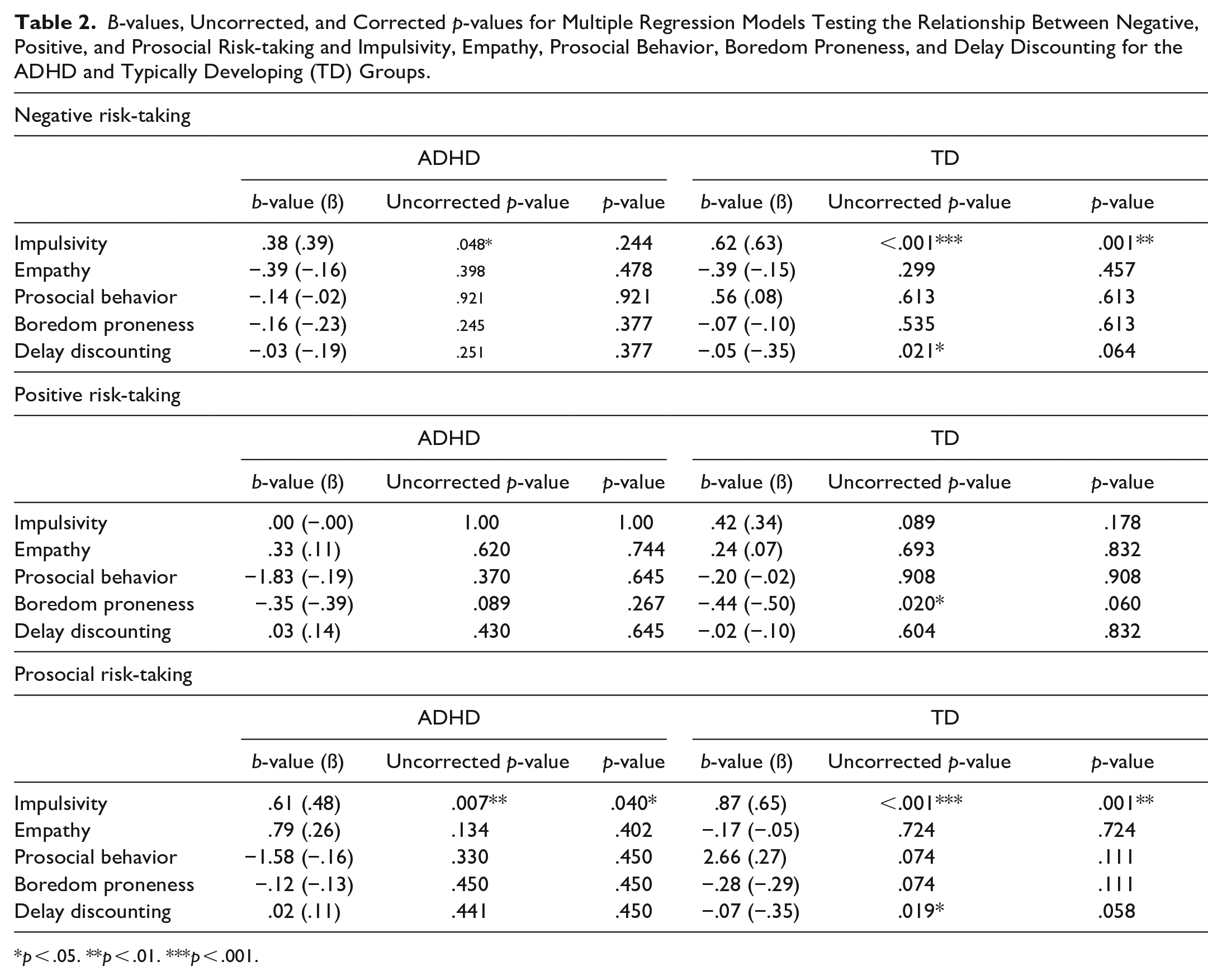
p < .05. **p < .01. ***p < .001.
Discussion
Adolescents with ADHD display heightened impulsivity, which is related to their engagement in many types of negative risk-taking behaviors (Pollak et al., 2019). The primary aim of this study was to test whether youth with ADHD are also more likely to engage in positive and prosocial risk-taking behavior. We assessed likelihood of engagement in negative, positive, and prosocial risk-taking behavior. Results showed that adolescents with ADHD indicated a stronger likelihood of prosocial risk-taking behavior compared to their peers without ADHD. Furthermore, the likelihood of prosocial risk-taking behavior was related to impulsivity. Prosocial risk-taking behavior is beneficial for others. As such, this is the first study showing that a heightened risk-taking tendency in youth with ADHD potentially also has an upside.
Likelihood of Engaging in Prosocial Risk-taking
Our first aim was to test whether adolescents with ADHD report a higher likelihood of engaging in positive and prosocial risk-taking behavior. Our results indeed showed a higher likelihood of engaging in prosocial risk-taking behavior for adolescents with ADHD. Prosocial behavior is defined as behavior in which the actor incurs a risk to benefit someone else. A higher likelihood of engaging in this type of risk-taking behavior suggests a strong prosocial or empathetic component and a strong risk-taking or impulsivity component (Do et al., 2017), which fits the impulsive and outgoing nature typical for adolescents with ADHD (Schippers et al., 2022). However, we did not find differences between the typically developing group and the ADHD group on positive and negative risk-taking. The positive and prosocial risk-taking scales were designed for the current study. It is possible that the positive risk-taking items tapped into more deliberate, intentional processes, such as subscribing to a new class, whereas the prosocial risk-taking items were more related to impulsive actions, such as standing up for a classmate who is being bullied. This explanation aligns with our result that negative and prosocial risk-taking behavior were related to impulsivity, but positive risk-taking behavior was not. Although the lack of group differences in negative risk-taking behavior is at odds with most of the literature, effect sizes are usually small and there are multiple other studies indicating that groups with and without ADHD do not always differ in risk-taking behavior (e.g., Dekkers et al., 2020; Van Hoorn et al., 2022).
Although we tested three different types of risk-taking behavior, we expected each of these domains to be related. Indeed, we found that negative, positive, and prosocial risk-taking behavior were all positively correlated, meaning that a tendency toward risk-taking behavior may simultaneously manifest itself in a negative and positive way (Duell & Steinberg, 2019). This aligns with research indicating a relative consistency of risk preferences across domains (Frey et al., 2017). To further test the differences between these types of risk-taking behavior we assessed which correlates were associated with each of the different types of risk-taking behavior as a secondary aim.
Correlates of Prosocial Risk-taking Behavior
We tested whether impulsivity, delay discounting, proneness to boredom, empathy, and prosocial behavior correlated with the different types of risk-taking behavior. We expected that impulsivity would be a general construct underlying each of the three different types of risk-taking behavior. Results showed these expected correlations for negative and prosocial risk-taking behavior in both groups. Positive risk-taking behavior was not associated with impulsivity. As discussed previously, the positive risk-taking items might be related more to deliberate processes, compared to the items measuring negative and prosocial risk-taking behavior.
Against our expectations, we did not find that empathy or prosocial tendencies were related to prosocial risk-taking behavior. A possible explanation for this, is a strong social justice element underlying the prosocial risk-taking items. Whether to stand up for someone being bullied can be an empathic choice, but also a sense of social injustice telling you that bullying is not right. Individuals with ADHD have the motivation to follow social norms but can have some difficulty doing that, heightening the sense of justice sensitivity (Schäfer & Kraneburg, 2015). Research shows that all ADHD subtypes are more sensitive to social injustice, relative to TD individuals (Schäfer and Kraneburg, 2015). This might explain the higher tendency for prosocial risk-taking without the expected accompanying heighted empathy and prosocial characteristics.
Strengths and Limitations
Our study included a substantial group of adolescents with and without ADHD, who completed a battery of questionnaires and tasks covering risk-taking behaviors and their potential correlates. Research on positive and prosocial risk-taking is novel in ADHD populations. The questionnaires used were designed for this study and display good internal consistency. Despite its strengths, this study also had some limitations. Firstly, some of the established, validated questionnaires such as the BIS-11 (measuring impulsivity) and SDQ (subscale measuring prosocial behavior) display somewhat low internal consistency, only reaching (almost) acceptable reliability. Secondly, we used hypothetical measures for risk-taking behavior, although previous research in youth found intuitive associations between such measures and ADHD symptoms (Shoham et al., 2016), meaning that outcomes of hypothetical risk-taking measured correspond with real-life measures. Future research should include more experimental or observational methods for determining actual engagement in different types of risk-taking behavior.
Thirdly, our risk-taking measures relied on self-report, which could be biased in adolescents with ADHD (Owens & Hoza, 2003). We deliberately selected these measures because we believe that the disadvantages of parent-report measures (who may have no or limited knowledge about the risk-taking behavior of their child) or laboratory tasks (low ecological validity; Frey, Pedroni, Mata, Rieskamp, & Hertwig) are larger. Future work could use other designs to measure prosocial risk-taking, for example by testing the proportion of adolescents with ADHD in a random sample of youth protesting for climate change. Fourthly, we did not find group differences on negative risk-taking, which might indicate that our ADHD sample was a relatively high-functioning sample, potentially not fully representative for the larger population of people with ADHD. This means that findings should be interpreted cautiously, until further replicated. Lastly, as this study was the first to assess relationships between positive and prosocial risk-taking measures and used a relatively small sample size, future work should replicate our findings.
Conclusion
The current study showed higher self-reported likelihood of engagement in prosocial risk-taking behavior in a group of adolescents with ADHD compared to their typically developing peers. The findings of this study have meaningful clinical implications. Logically, when working with adolescents with ADHD, clinicians are predominantly focused on preventing or treating negative types of risk-taking behaviors such as substance abuse or delinquent behavior. In addition, it is valuable to consider that a potential upside to these negative behaviors might be that these adolescents may also be inclined toward more prosocial types of risk-taking behaviors. Clinicians as well as other adults may encourage and assist adolescents with ADHD to create opportunities to channel their risk-seeking propensity in a beneficial, prosocial direction.
Supplemental Material
sj-docx-1-jad-10.1177_10870547251321882 – Supplemental material for The Upside of ADHD-related Risk-taking: Adolescents With ADHD Report a Higher Likelihood of Engaging in Prosocial Risk-taking Behavior Than Typically Developing Adolescents
Supplemental material, sj-docx-1-jad-10.1177_10870547251321882 for The Upside of ADHD-related Risk-taking: Adolescents With ADHD Report a Higher Likelihood of Engaging in Prosocial Risk-taking Behavior Than Typically Developing Adolescents by Barbara R. Braams, Rebecca van Rijn, Tessa Leijser and Tycho J. Dekkers in Journal of Attention Disorders
Footnotes
Acknowledgements
We thank all participants in the study. We are grateful to Nina Zuidema, Ceyda Dilek, Eline Jacobs, and Rosalie Ursinus for their assistance during data collection.
Author Contributions
BRB and TD developed the study concept. BRB, RvR, TL, and TD were involved in study design. TL and RvR collected the data. BRB carried out the analyses. BRB and TD wrote the initial draft of the paper. RvR and TL provided feedback on the draft. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BRB and RvR were funded with the support of the Ammodo Science Award 2020 for Social Sciences. The funders had no role in this study design, data collection, analysis and interpretation of the results.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.