
Abstract
This study aimed to examine the concept of Managed Long Term Care service from a care manager’s perspective. The Walker and Avant concept analysis approach was applied. The defining attributes include (1) chronic disease or disability, (2) coordination of care, and (3) services. Core components of Managed Long Term Care service were found to be a network of providers and capitation. A conceptual model of Managed Long Term Care service was developed with Managed Long Term Care service operationally defined as “a program with a set of services delivered to patients who have a chronic illness or disability and wish to stay safe and healthy at home in the community. The services or benefits are coordinated by a care manager who serves as a point of contact for the patient and provider(s), and are delivered by providers in the network.” Care management is a core concept of Managed Long Term Care. The triple aims of Managed Long Term Care are to deliver the right care at the right time at the right cost to Managed Long Term Care eligible patients. This paper sought to illuminate and clarify varied perspectives on the concept of Managed Long Term Care service. Without a clear understanding of a community-based service or program, delivery of nursing care may be less effective. This study was the first to examine this widely used but often imprecisely defined community health service from a case manager’s point of view.
Introduction
Managed Long Term Care (MLTC) service is a term that was introduced in the 1990s and used widely in several states in the United States. Saucier et al.
1
explain the context in which MLTC service originated as follows: Long term care users need a variety of services across numerous settings (e.g., home, doctor’s office, hospital, day center, nursing home), but in the Medicaid and Medicare fee for service systems, no single person or organization is responsible for or can impact all needed care, resulting in services that are often characterized as fragmented, uncoordinated and rife with unintended financial incentives. . .. Avoidable hospital admissions, unnecessary use of nursing home care, and medication mismanagement are among the risks faced by the population.
1
Although MLTC programs vary across target populations, enrollment voluntariness, benefits covered and other aspects, the goal of such programs is the same across the states where they are implemented. For example, a New York State Managed Long-Term Care Final Report to the Governor and Legislature 2 states that “all MLTC plans in New York share the same goal: to assist people who are chronically-ill or have disabilities and who need health and long-term care services to remain in their homes and communities as long as possible.” While the goal of MLTC programs is clearly stated by each state where the service is implemented, the definition of MLTC service appears to be more ambiguous in practice. For this reason, a concept analysis as described Walker and Avant 3 was performed to systematically analyze the concept of MLTC across disciplines and practices.
Background
In the United States, the proportion of the population aged >65 years is projected to increase from 35 million in 2000 to 74 million in 2030 and representing nearly 21% of the total U.S. population. 4 In this population, two out of every three have multiple chronic conditions that need some care coordination. 5 According to the Congressional Budget Office, 6 the vast majority—80%—of elderly people receiving assistance, including many with several functional limitations, live in private homes in the community, not in institutions. This corresponds with what most Americans prefer, which is to remain in their home and community—not in nursing homes. 7 To meet this population need, Managed Long-Term Care (MLTC) service was introduced. MLTC plans include services covered by Medicare and Medicaid (dually eligible) or only by Medicaid. As most care for patients with chronic diseases is covered by Medicaid, MLTC service under Medicaid payments (called MLTSS: Managed Long-Term Services and Supports) has been expanding. As reported by the CMS report from Lewis et al., 8 total enrollment in MLTSS programs more than doubled, from 800,000 in 2012 to 1.8 million in 2017.
Definitions of Related Terms
It is important to discuss the established definition of words that make up the term MLTC. Here is a survey of dictionary definitions for the words “Managed,” “Long Term,” and “ Care.”
Definition of “Managed”
The term “managed” is not only used in healthcare but also in government, business, information technology, and other settings. When searching the term “managed,” the verb “manage” comes first. “Manage” has two main definitions from the Cambridge English Dictionary, which are “to succeed in doing something, esp. something difficult” and “to control or organize someone or something, esp. a business.” In the Merriam-Webster dictionary, “manage” has three main definitions, which are: “to have control of (something, such as a business, department, sports team, etc.)”; “to take care of and make decisions about (someone’s time, money, etc.)”; and “to direct the professional career of (someone, such as an entertainer or athlete).”
The meaning of the term “managed” seems to shift depending on the sector where it is applied. According to the Macmillan Dictionary, “managed” means “controlled by the government.” The examples provided to demonstrate usages were “a managed currency” and “a managed economy.” The Business Dictionary uses the term in “managed service,” defined it as “Management, typically by an outside third-party, of an organization’s services and equipment related to computers, networks, or software. Web hosting providers and internet service providers are examples of entities that provide a managed service.” 9 In the Medical Dictionary “managed” is found in the phrase “managed care,” defined as “a method of health care delivery that focuses on collaboration among and coordination of all services to avoid overlap, duplication, and delays and to reduce costs. There is an emphasis on efficacy and timeliness of interventions to prevent unnecessary delays in discharge from the hospital or agency.” 10
Definition of “Long term”
“Long term” as defined by the Merriam-Webster Dictionary is “occurring over or involving a relatively long period of time.” The Cambridge English Dictionary definition for “long term” is “happening, existing, or continuing for many years or far into the future.” In the Business Dictionary the term is defined as “Generally, a time frame for investing in which an asset is held for at least 7 to 10 years. The measure of a ‘long term’ time frame can vary depending on the asset held or the investment objective. In business accounting measures, long term can be a period of time that exceeds 12 months.” 11 In relation to healthcare, the Medical Dictionary uses the term combined with “care” and defines it as “Health care services required for an extended period of time by individuals unable to fully execute Activities of Daily Living (ADL); it can be provided by a variety of agencies in outpatient settings as well as on an inpatient basis.” 12
Definition of “Care”
Definitions of “care” from the Merriam-Webster Dictionary include “effort made to do something correctly, safely, or without causing damage; things that are done to keep someone healthy, safe, etc.; things that are done to keep something in good condition.” The two main definitions for “care” in the Cambridge English are “the process of providing for the needs of someone or something” and “serious attention, esp. to the details of a situation or a piece of work.” Other definitions found in the Macmillan Dictionary are “to be interested in someone and want them to be well and happy” and “to be interested in something and feel strongly that it is important.”
This survey of definitions provides the general semantic context in which the specialized term MLTC is situated. Nonetheless, MLTC service has meaning that is not fully captured by the definitions of the individual words that compose it. Therefore, to completely address its meaning, a concept analysis of MLTC is necessary. The goals of this paper are to (a) analyze the concept of MLTC; (b) propose a theoretical model of MLTC; and (c) explore its implications for professional practice, research, and patient education.
Literature Review
A comprehensive literature review was conducted using the Cumulative Index of Nursing and Allied Health and Medline to identify how MLTC has been defined and used in the literature. A combination of “managed care” and “long term care” as headings (Cumulative Index of Nursing and Allied Health) and map terms (Medline) were searched in each database, as keyword searches in both databases yielded thousands of irrelevant articles.
A total of 158 articles were found under these search terms from the two databases. After removing duplicates and screening for titles, 42 were left for abstract and full-text screening. Many of the articles examined program elements of the Program of All-Inclusive Care for the Elderly, which is has been deemed as the one of first MLTC programs in the U.S., and evaluated and compared the Program of All-Inclusive Care for the Elderly to other program models. Some articles discussed funding sources in delivering long-term care, focusing on public funding sources such as Medicare and Medicaid. Only one paper discussed MLTC as a whole and provided a definition: “. . .managed long-term care (MLTC) that integrates all or most long-term-care funds under a capitated rate for all services offered by a managed care organization (MCO).” 13 However, this definition still focuses on the financing aspect while not considering the delivery of care component.
Methods
An eight-step methodology suggested by Walker and Avant 3 was used in this concept analysis, shown in Table 1. 3
Walker and Avant Model.

Data Sources
The Cumulative Index of Nursing and Allied Health and Medline were used in the concept analysis. No year limitation was placed. Google searches of the same terms was also performed to examine how MLTC is used more generally outside of the literature and thus capture a broad use of the investigated concept.
Results
Uses of the Concept
MLTC service in literature
Evaluating and comparing care delivery model within MLTC
Many of the articles covered the Program of All-Inclusive Care for the Elderly, which is the oldest MLTC model that is center-based and all-inclusive. The articles used MLTC to explain, examine, and evaluate the Program of All-Inclusive Care for the Elderly 3 and checking its effectiveness compared to different approaches to MLTC, including partially capitated models.14-17
Comparing MLTC model to traditional fee for service model
The MLTC service concept is also used in the public health sector by policy makers at the federal level (e.g., Center for Medicare and Medicaid Services) or at the state level (such as in New York, Maine, and Pennsylvania) to develop each state’s own long term health care program. In the literature, MLTC service is used when comparing its effectiveness in delivering long term care to traditional fee for service regarding improvement in quality of care, service utilization related to cost management.18-20
Discussing the qualifications of Managed Care Organizations
Some articles21-23 discussed who the MLTC service provider should be, as MLTC service straddles the otherwise two distinct areas of managed care and long term care. This usage of the term exactly reflects a finding of the 2012 CMS report, that the development of the MLTSS market was initially hampered by a very limited supply of organizations. 24 These articles examined and recommended non-profit home care providers as Managed Care Organizations (MCOs) that have the experience and resources to provide long term care service in the community.
MLTC service in practice
Consumer guide
The Google searches for MLTC term displayed government and state department of health websites as well as many MCO websites and brochures that described MLTC programs geared toward target consumers. Providers must develop easily understood consumer guides for eligible patients to educate them about the programs and to sell them to the health care market. These usages of the MLTC concept focus on the benefits covered under the programs and eligibility to enroll in a given program.
Defining Attributes
Chronic disease or disability
To be eligible for enrollment in an MLTC program, a patient must have a chronic disease or condition that require continuous care. MLTC is to provide care for an extended period of time to individuals unable to fully execute activities of daily living. This is in contrast to acute care, in which the symptoms and disease are treated for a short period of time and patients recover at discharge. Chronic disease or disability is the core component of care that is rendered in MLTC.
Coordination of care
In MLTC, care coordination or care management is provided by a care manager. Care coordination is intended to avoid overlap, duplication (right care), and delays (right time) in necessary care. The New York State Managed Long-Term Care Final Report 2 states that care management activities are the very heart of managed long term care.
Care coordination has been defined as “the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services.” 25 Another article analyzed the concept of care coordination and defined it as “a function and product of a team approach to providing seamless, safe, quality care for an individual. . . .. Care coordination is a team effort with the patient as an active central decision maker.” 26
Services
In other words, “covered benefits” in MLTC vary by program. Depending on capitation type and source, some major services are not covered by certain programs.
Core components of MLTC services
To identify in more detail the actual MLTC service provided currently, program core components analysis was performed. There are several different types of programs under the MLTC concept with different payer sources and covered services. CMS has reported that all program contractors and plan services are covered under MLTSS. 24 The total number of MLTSS programs more than doubled from 19 programs in 2012 to 41 programs in 2017.
Medicaid capitated services mostly cover primary and acute care (except Wisconsin Family care and the Michigan Medicaid Managed Specialty Support and Services Program). A majority of programs cover behavioral therapy and prescription drugs. Substantial differences in Long Term Service and Support (LTSS) components were found. Nonetheless, the vast majority of programs provide the following services under Medicaid capitation: nursing facility, case management, adult day health, assisted living services, personal care, house-keeping, respite care, home delivered meals, transportation, medical supplies and equipment, and personal emergency response system.
Network of providers: CMS requires MLTSS plans to have an adequate network of qualified providers to meet the needs of their enrolled beneficiaries. 24 Nadash 27 noted, “As a managed-care entity, the Plan does not provide services directly. Rather, it arranges and pays for them, contracting with a broad network of providers and exerting influence through these contractual relationships.” Examples of providers in a network include nursing facilities, primary care physicians, pharmacies, physical or occupational therapists, and medical suppliers.
Capitation: Capitation is the method employed to manage health care cost in MLTC. One of the innovative aspects of MLTC is the use of an insurance or “risk” model, where plans are paid a predetermined amount per member per month by the government, referred to as the monthly capitation rate, and in return the provider must manage all services included in the benefit package. 2 Nadash 27 reports that capitation of covered benefits creates incentives for providers to keep plan members out of long term care institutions and keep them as functionally independent as possible.
Antecedents
This concept analysis identified three required antecedents of MLTC: chronically ill or disabled patients at home or in the community, Medicare or Medicaid coverage for community care, and professional understanding and development for coordination of care. If one of these antecedents is absent, there would be no opportunity to provide MLTC service.
Consequences
Consequences of MLTC are obvious and closely related to MLTC program goals. The most immediate consequence of MLTC is reduced hospitalization rates that eventually lead to improved or maintained health conditions of individuals with chronic illnesses or disabilities. Reduced hospitalization and prolonged stays at home or in the community leads to achieving the congruent goals of patients wishing to stay home and government’s and state goal of reduced health care cost per capita.
Cases
Model case
Mrs. A is a 70 year-old participant in an MLTC program who lives alone in a private house with multiple chronic conditions, and is occasionally visited by a Community Health Nurse as covered by the program. She recently tripped and fell outside the home and fractured her hip. She was hospitalized for surgery and discharged to a rehabilitation center. Her case manager in a MLTC program communicated with the hospital staff on her status throughout the transition and arranged her safe discharge to home. She was provided transportation to return home with an accompanying aide at the time of discharge. Her case manager also referred her to a physical therapist and occupational therapist to assess her at home at the time of discharge for any durable medical equipment and therapy needs. The physical therapist requested grab bars and a walker for her and physical therapy sessions three times per week. The case manager ordered the equipment as requested and also referred the patient to a social worker to check her emotional status and help with any social issues that she might encounter due to physical restrictions. The community health nurse visited Mrs. A’s home and reconciled her meds from hospital discharge. The community health nurse reported changes in medications to the case manager and primary care physician. The community health nurse set up a regular schedule for a general health check for Mrs. A. As a result of a meeting with several relevant care providers in which they reviewed the community health nurse’s Activities of Daily Living report, the case manager increased Mrs. A’s home health aide hours temporarily to meet her needs at home. The case manager and the community health nurse also contacted the primary care physician to provide an update on Mrs. A’s progress and to make sure Mrs. A has a follow-up appointment scheduled with her primary care physician as well as her surgeon at the hospital. After several months of continued physical and occupational therapy combined and the assistance of the home health aide, Mrs. A improved her condition and agreed to resume visiting the adult day health center that she loves. Her aide hours were reduced to the previous level and she attends the center twice a week to socialize and maintain her health.
In this case, everyone involved in Mrs. A’s care, including Mrs. A herself, proactively performed their duty and communicated well throughout the care delivery, enabling Mrs. A to recover and return to the community.
Borderline case
Ms. B is 25 years old and lives with her mother in a house. Ms. B has mental retardation with a physical disability that requires her to use a wheelchair. Her mother requested something to support Ms. B’s coccyx area, as she sits for long periods of time in her wheelchair and the area gets red. The case manager requested a physical therapist to visit their home and identify what type of support would best fit Ms. B’s needs. The physical therapist examined her condition and he requested a gel cushion for her wheelchair to relieve pressure on the buttocks. The case manager needed a prescription from a primary care physician to order the item and so contacted the primary care physician, but the doctor wanted to see Ms. B before prescribing anything. The case manager told Ms. B’s mother to take her to see the primary care physician soon but Ms. B’s mother was busy working and had no time to take her to the doctor’s office anytime soon. The case manager could not refer Ms. B to a visiting doctor service as no such service provider was within the network. The case manager forgot to follow up with the mother and primary care physician for a few weeks. After a few weeks, a community health nurse found a stage 2 ulcer on Ms. B’s coccyx.
This borderline case shows how a failure in one part of the whole system can affect a patient’s condition in MLTC. Although the case manager initiated appropriate care for the patient and the physical therapist did his job properly, the delay in a prescription from the provider side, a network issue, and the case manger’s poor follow-up made Ms. B develop a wound that was avoidable.
Contrary case
Mr. C is a 75 year-old Russian speaking male in an MLTC program. His arthritis recently worsened, making it more difficult for him to get in and out of the bathtub when taking a shower. He contacted his case manager, who also speaks Russian, to request a grab bar and shower bench. This case manager went on vacation while the covering case manager, who does not speak Russian, ordered the equipment but forgot to check the order delivery status. Mr. C’s regular home health aide, who speaks Russian, was out sick during this time period and was temporarily substituted with another aide who does not speak Russian. At the time when Mr. C was originally enrolled in the MLTC program, he was given the program’s general number, which has a menu option for a translator, but he did not bother to call to follow up on the delivery. A few weeks later, the equipment was finally delivered to Mr. C’s house, but because the covering case manager did not consult with the program’s physical therapist to determine the correct size and type of equipment, the grab bar and bench did not fit in Mr. C’s bathtub and thus had to be returned. One day, Mr. C took a shower early in the morning without the assistance of an aide, fell in the bathtub, and had to be taken to the hospital.
This contrary case illustrates how failure of core attributes of MLTC services can result in serious consequences. Issues with communication, negligence by the case manager and the patient himself, and problems with delivery of supplies or equipment from network providers brought significant danger to the patient’s health, resulting in hospitalization.
Empirical Referents
Walker and Avant 3 stated that determining the empirical referents is the final step in concept analysis. According to them, empirical referents are “the means by which you can recognize or measure the defining characteristics or attributes” and in many cases, the defining attributes and the empirical referents will be identical. Thus, empirical referents for the concept “MLTC” are the existence of programs delivering service under the MLTC concept, individuals who have a chronic condition or disability, who live at home in the community, and who effectively manage their health as participants in the MLTC program provided in the area.
Theoretical Model of MLTC Service
Figure 1 depicts the Concept Model of Managed Long Term Care service developed in the present study, encompassing related terms, defined attributes, and findings described in further detail in the results section. In this model, the operational definition of MLTC service is: a program with a set of services delivered to patients who have a chronic illness or disability and wish to stay safe and healthy at home in the community. The services or benefits are coordinated by a care manager who serves as a point of contact for the patient and provider(s), and are delivered by providers in the network.
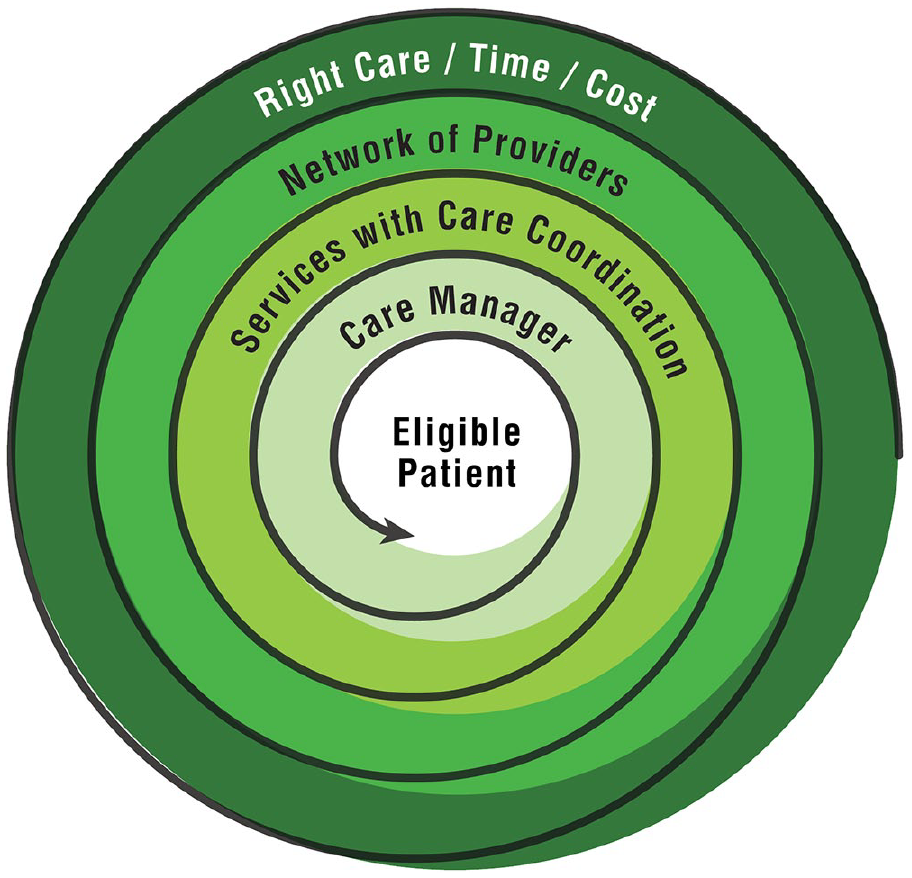
Concept model of managed long term care service.
Care management is a core concept of Managed Long Term Care. The triple aims of Managed Long Term Care in turn are to deliver the right care at the right time at the right cost to Managed Long Term Care eligible patients.
Implications
Each state’s program has different components to their MLTC service as they can design the program depending on the unique needs of their populations. However, the core concept is the same. The individual programs may evolve over time, but the MLTC concept remains constant. This concept analysis provides a conceptualization that can be used across programs and settings. The defined MLTC concept can be used not only in nursing but also in public health and medicine. Researchers can utilize this concept in their study of related areas and topics. Healthcare professionals can use this concept in their work settings to guide their service and care of patients. This concept can also be used as an important part of patient education by MCOs to explain what MLTC means and what patients can expect from the MLTC program they are in.
Conclusion
This concept analysis sought to capture the essence of the MLTC service concept from a case manager’s perspective. A mutually understood and agreed upon concept equips researchers with an essential theoretical foundation for their studies on MLTC program effectiveness, payer sources, and other topics that have been and will be explored in the literature. Such a concept also enables professionals involved in MLTC service to execute their roles more effectively in the system and to educate and guide the populations served by MLTC programs.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: At the time of manuscript development, Kyungmi Woo was supported by Reducing Health Disparities Through Informatics (T32 NR007969) training grant through the National Institute of Nursing Research.