
Abstract
Objective
This study aimed to systematically review studies that reported factors associated with the risk of cardiovascular disease (CVD) in family caregivers of people with dementia (PWD).
Methods
Literature was searched in PubMed, Medline, CINAHL, and PsycINFO using keywords generated from the terms “dementia”, “caregiver”, and “cardiovascular disease”. We included studies that examined factors associated with CVD risk in family caregivers of PWD, those with longitudinal or cross-sectional study designs, and those published in English.
Results
A total of 34 studies were included in this review. Stress and depressive symptoms, pleasant leisure activity, coping self-efficacy and coping strategy, physical activity, and social support were the main modifiable associated factors of CVD risk in family caregivers of PWD. However, the association between sleep and CVD risk was unclear. Caregiving status, the duration of caregiving, genes, and race, were the main non-modifiable associated factors of CVD risk in family caregivers.
Conclusion
This review showed seven modifiable factors of CVD risk. In particular, leisure activities, physical activity, and social support were significantly negatively associated with the risk of CVD. Researchers and clinical professionals are recommended to consider these risk factors when they develop interventions to reduce CVD risk in family caregivers of PWD.
Keywords
Background
Dementia is one of the major causes of disability and dependency in older people; and it is currently the seventh leading cause of death worldwide. 1 Most people with dementia (PWD) receive care at home from family caregivers 2 who are responsible for most daily activities, including feeding, bathing, assisting with toileting, and dressing. 3 The term “family caregivers” refers to non-professional people who provide unpaid care for others at home. Family caregivers have a major challenge in taking care of their relatives with dementia because the behavioral and psychological symptoms of dementia are difficult to deal with. 4
Family caregivers of PWD are usually considered to be “invisible second patients”. Caregiving tasks have a negative effect on family caregivers’ physical health. 5 Two meta-analyses reported that informal caregivers suffered poorer physical health conditions than did non-caregivers.5,6 Furthermore, caregivers had lower scores on a self-reported general health questionnaire and the Health-Related Quality of Life questionnaire than did non-caregivers. 7 Family caregivers of PWD also engage in fewer physical activities, experience more sleep disturbance, and have a higher risk of malnutrition than do non-caregivers.8–10
There is a growing body of research that has focused on impairment of cardiovascular health of caregivers.11–14 Cardiovascular disease (CVD) is the leading cause of death worldwide, and approximately 17 million people die from CVD each year. 15 Recent studies have reported that caregivers have a higher risk of developing CVD than do non-caregivers. 16 Long-term exposure to chronic stress may also produce changes in the emotional and physiological responses that affect susceptibility to disease, especially CVD. 17 Caregivers of PWD experience a higher level of stress and depressive symptoms compared with caregivers of loved ones with other chronic diseases and disabilities.18,19
Family caregivers of PWD show a higher risk of suffering from hypertension than do non-caregivers.20–22 Hypertension is the main risk factor for CVD. 23 Caregivers also have higher pro-coagulant molecule D-dimer (DD) 24 and pro-inflammatory cytokine interleukin (IL)-625 concentrations relative to non-caregivers, which may result in a pro-thrombotic and pro-inflammatory status. Elevations in serum levels of IL-6, DD, and C-reactive protein (CRP) are associated with higher risks of cardiovascular disorders, autoimmune diseases, frailty, and mortality.26,27
Family caregivers of PWD who suffer from CVD experience a higher risk of morbidity and mortality, 15 which in turn decreases their ability to take effective care of their relatives. Understanding the risk factors of CVD in family caregivers of PWD before implementing interventions is important. However, there have been no systematic reviews that examined factors associated with CVD in family caregivers of PWD. Therefore, this study aimed to systematically review studies that reported associated factors of CVD risk to determine the factors of CVD in family caregivers of PWD.
Methods
Search strategy
Articles were identified from four electronic databases, including PubMed, CINAHL, Medline, and PsycInfo, published from 31 December 1987 to 31 December 2017. The key search terms were generated from the terms “dementia”, “caregiver”, and “cardiovascular disease”. The search keywords were (dementia OR Alzheimer OR “cognitive disorder”) AND (caregiver* OR carer OR “caring personnel”) AND (“cardiovascular diseases” OR “myocardial ischemia” OR “coronary artery disease” OR infarct* OR ischemic OR heart diseases OR hypertension OR “blood pressure”). The search process was conducted between November 2017 and December 2017. During the search process, the authors first browsed the title and the abstract of each article. If the title and the abstract were related to the review topic (with an overall agreement found to be 90%), the full text was extracted to research the details of each study. Each study was retrieved according to the PRISMA guidelines (http://www.prisma-statement.org/).
Inclusion and exclusion criteria
This review included primary studies that examined the risk factors of CVD among family caregivers of PWD. Those studies were designed as longitudinal or cross-sectional studies and were published in English. The factors associated with the risk of CVD were found in cross-sectional studies, and the causal relationship between caregiving situation-related factors and CVD risks were determined from longitudinal studies.
The exclusion criteria were studies that did not primarily focus on the risk factors associated with CVD in family caregivers of PWD, and studies that were published in a language other than English. Systematic reviews, editorials, letters to the editor, theses, and practice guidelines were excluded from this review. Interventional or experimental studies were also excluded because the outcomes were likely to be changed after the intervention.
Data extraction and synthesis
The authors reviewed the titles, abstracts, and the content of the selected articles. One reviewer extracted data from each study while the other read each article to check the accuracy and completeness of the extracted data. The study type, population, number of participants, age, factors associated with the risk of CVD, measurements of study outcomes, and results were extracted from the selected papers and incorporated in an evidence table according to Cochrane’s guidelines. 28
Quality appraisal
The study quality was evaluated by a standardized critical appraisal instrument from the Study Quality Assessment Tools offered by the National Institutes of Health of the United States. 29 Two reviewers assessed the quality of the reviewed studies separately under this standardized critical appraisal instrument. Discrepancies were solved by a third researcher. The criteria of the National Institutes of Health 29 were used to assess the quality of the studies. Each study was assigned an overall quality rating of good, fair, and poor according to the above-mentioned criteria. This overall rating was determined by the number of criteria that the study met and the risk for potential bias. One cross-sectional study 30 and one longitudinal study 31 were rated as fair because of their small sample sizes (n < 40).
Results
Search outcome
Figure 1 shows the results of the search (PRISMA flow chart). A total of 756 records were identified from four databases. Of those, 236 duplicate studies were excluded, as well as another 473 irrelevant studies after screening titles and abstracts. After reviewing 47 full texts, 13 studies were excluded. The excluded studies included six theses, one book section, four randomized, controlled trials, one study in which the population did not comprise family caregivers of PWD, and one study that did not examine the associated factors of CVD risk. Finally, 34 studies were included in this systematic review. Among the selected studies, 25 of them were cross-sectional studies.

PRISMA flow diagram of the study.
A total of 4638 participants were included in this review, including 3689 family caregivers of PWD and the other participants were non-caregiving controls. Most of the family caregivers were older (age ≥55 years), spousal caregivers (>55%), and women (75%). Nearly 90% of the participants were from the United States. Table 1 shows the table of evidence of the reviewed studies.
Characteristics of the reviewed studies.

*Cross-sectional study; #longitudinal study; †significantly positively related to; ‡not significantly related to; Δsignificantly negatively related to
ADL: activities of daily living; AR: activity restriction; BP: blood pressure; cBRS: cardiovagal baroreflex sensitivity; CHD: coronary heart disease; CI: confidence interval; CRP: C-reactive protein; CVD: cardiovascular disease; DD: D-dimer; DBP: diastolic blood pressure; EPI: epinephrine; HDL: high-density lipoprotein; HR: heart rate; IL-6: interleukin-6; IMT: intima-media thickness; MAP: mean arterial pressure; MetS: metabolic syndrome; MSE: mean square error; NA: not available; NE: norepinephrine; OR: odds ratio; PAI-1: plasminogen activator inhibitor 1; PP: pulse pressure; SBP: systolic blood pressure; TAT: thrombin-antithrombin III complex; t-PA: tissue-type plasminogen activator assay; vWF: von Willebrand factor.
Common risk factors of CVD in family caregivers of PWD and in non-caregivers.
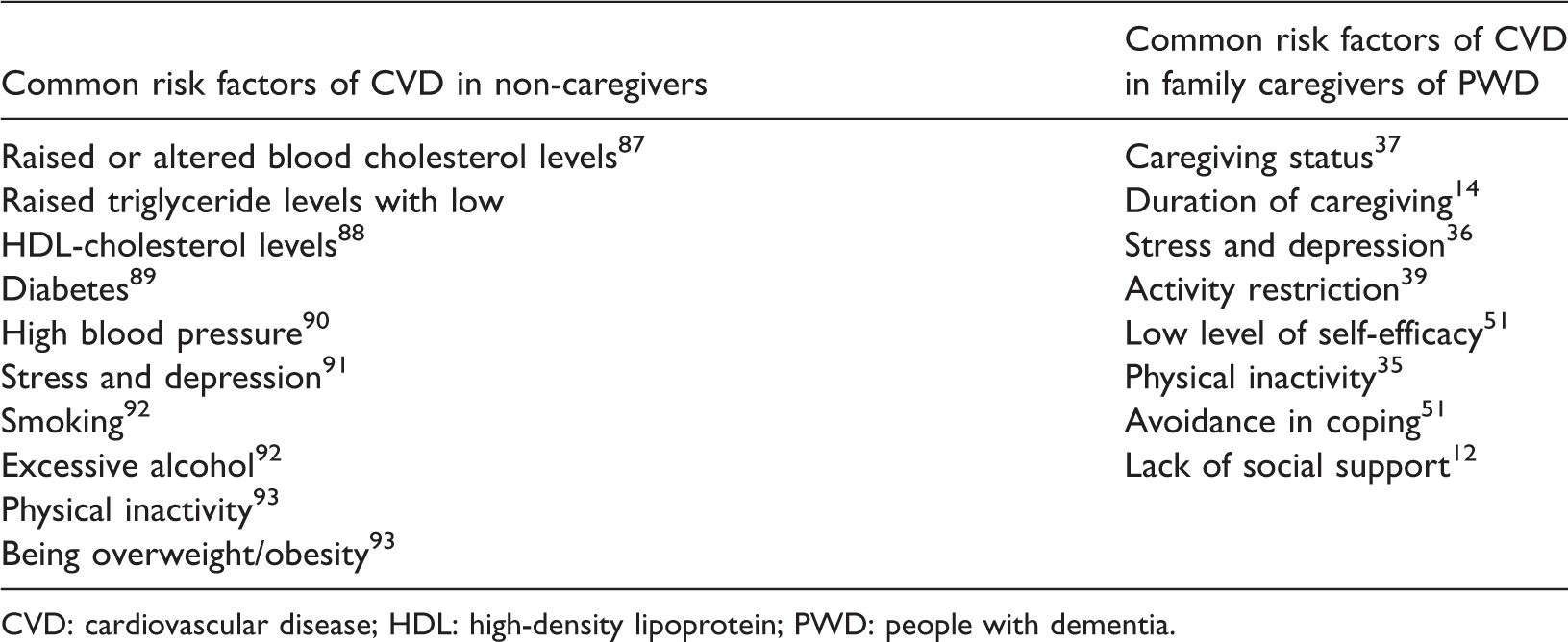
CVD: cardiovascular disease; HDL: high-density lipoprotein; PWD: people with dementia.
Indicators for assessing CVD risk
Most studies showed that blood pressure (BP) and heart rate (HR) were factors that reflected cardiovascular status, and these were measured by noninvasive BP monitors following a standard procedure. To avoid diurnal effects of the participants, most of the BP measurements were taken in the morning. Some studies defined hypertensive status by participants’ self-reports and current use of an antihypertensive prescription.32–34 Metabolic syndrome (Mets) factors, which include adiposity, dyslipidemia, hypertension, and hyperglycemia, were also used to reflect cardiovascular status.35,36 One study adopted the Framingham coronary heart disease risk score, which includes age, sex, smoker, total cholesterol, high-density lipoprotein (HDL) cholesterol, systolic BP, and BP being treated with medication, to measure the CVD risk in family caregivers of PWD. 37
Several studies also applied plasma indicators as biomarkers for showing cardiovascular status. The resting plasma norepinephrine (NE) level predicts incident cardiovascular events in patients with end-stage renal disease, 38 and it was applied in two cross-sectional studies.39,40 Seven studies used IL-6 and DD levels to evaluate the risk of CVD. Carotid intima-media thickness (IMT), a marker of subclinical atherosclerosis, 41 was applied in a cross-sectional study. 42
Modifiable associated factors of CVD risk
Stress and depressive symptoms
Stress and depressive symptoms were modifiable associated factors of CVD risk among family caregivers of PWD. Daily stressors were positively related to an elevation of IL-6 (p = 0.04) and CRP (p = 0.04) levels in Gouin et al.’s study. 43 Similar findings suggested that speech stress significantly increased HR (p = 0.017), systolic BP (p = 0.002), and diastolic BP (p < 0.001) among spousal Alzheimer caregivers as reported by Von Känel et al.’s research team in cohort studies. 24 Mausbach et al. 44 also found that after adjusting for sociodemographic and health risk factors in a cohort study, greater depressive symptoms (p = 0.04) and distress from problem behavior of patients (p = 0.03) were significant predictors of incident CVD diagnoses. A significant decrease in the number of MetS factors after nursing home placement of the spouse only occurred in caregivers with lower levels of depressive symptoms (p = 0.01). 36 Additionally, the number of negative life events, which are positively associated with stress, also predict higher plasma DD levels (p = 0.01).31,45
Pleasant leisure activity
Three reviewed studies showed that engagement of pleasant leisure activities (e.g., watching TV, going on outings, shopping or buying things, having coffee, tea, etc. with friends) was likely to reduce the CVD risk in family caregivers of PWD. In Mausbach et al.’s 44 study, greater engagement in pleasant leisure activities predicted reduced mean arterial BP (MAP) (p = 0.04) and reduced diastolic BP (p = 0.03) over 5 years. This positive effect of pleasant leisure activities on physical health among caregivers was also found by Chattillion and colleagues. 46 In their study, participants with high engagement in pleasant events plus low perceived social and recreational activity restriction (AR) (being restricted from engaging in activities, such as going shopping, visiting friends, working on hobbies) had significantly lower MAP compared with those with low pleasure plus high restriction (p = 0.01) and those with high pleasure plus high restriction or low pleasure plus low restriction (p = 0.023). Another study showed that the duration of caregiving was significantly associated with epinephrine levels when social and recreational AR was high (p = 0.008), but not when AR was low (p = 0.799). 39
Coping self-efficacy and coping strategy
Two studies showed that family caregivers with higher levels of coping self-efficacy had a lower risk of CVD.47,48 High levels of self-efficacy for problem-focused coping were associated with lower MAP and systolic BP. 49 Self-efficacy further buffered the relationship between risk factors and CVD risk. In Mausbach et al.’s 50 study (2007), when self-efficacy was low, stress was significantly related to IL-6 levels (β = 0.43). However, when self-efficacy was high, stress was no longer significantly related to IL-6 levels (β = −0.10). Coping strategy was associated with CVD risk among family caregivers of PWD in the two following studies. Active coping was shown to be negatively related with diastolic BP (p < 0.01), 49 and similarly, greater avoidance in coping was related to a greater level of BP reactivity (p < 0.001). 13
Physical activity and social support
Physical activity also moderated cardiometabolic risk in caregivers in one study. Among participants with low levels of physical activity, caregivers had greater cardiometabolic risk scores than did non-caregivers (p = 0.017); there was no group difference in participants with high levels of physical activity (p = 0.81). 35 Furthermore, social support moderated the CVD risk in family caregivers of PWD and systolic BP did not vary as a function of age in subjects with relatively high levels of social support. 12
Sleep conditions
Whether the sleep conditions of family caregivers of PWD have an effect on their cardiovascular reactivity is debatable. In Schwartz et al.’s cross-sectional study, nighttime sleep duration, the percentage of time spent sleeping at night, and daytime naps were not significantly associated with the likelihood of having hypertension (odds ratio [OR], 0.97; 95% confidence interval [CI], 0.62–1.52; OR, 1.02; 95% CI, 0.93–1.11; OR, 1.10; 95% CI, 0.44–2.74, respectively). 33 However, Mausbach and colleagues 40 (2006) found that after controlling for the number of cardiovascular risk factors (e.g., age, sex, BP, body mass index), increased awake time after sleep onset was positively associated with NE levels (p = 0.020) and plasma DD levels (p = 0.038).
Non-modifiable associated factors of CVD risk
Caregiving status and duration
Caregiving status is a significant non-modifiable factor associated with the risk of CVD. Four longitudinal studies reported that the risk of developing CVD was significantly higher among people who were caregivers of PWD compared with non-caregivers.24,36,50,51 Shaw et al. 20 (1999) found that caregivers of PWD were 67% more likely to develop hypertension than non-caregivers. In Von Känel et al.’s 37 study, spousal caregivers of PWD had higher Framingham coronary heart disease risk scores compared with non-caregivers. Other studies also showed some molecular and cellular changes, which may explain the increased risk of CVD in family caregivers of PWD.32,43 Longitudinal studies have also reported that both DD 52 and IL-6 51 levels were significantly increased over time in family caregivers of PWD. Another study showed that accumulation of IL-6 levels in caregivers was approximately four times higher than that in non-caregivers. 51 After nursing home placement of patients, the risk of CVD was significantly reduced. 36
A study showed that, when caregiving ended, after the death of the spouse, the number of MetS factors was significantly reduced (p = 0.003) and was no longer different from that of non-caregivers. 36 The duration of caregiving also increases the risk of developing CVD. Wu et al. 14 showed significant impairment of cardiovagal baroreflex sensitivity, which was negatively associated with the CVD risk in long-term caregivers (caregiving ≥4 years) compared with short-term caregivers (caregiving <4 years). Another study reported that the duration of caregiving was significantly positively associated with epinephrine levels, which were positively connected with NE levels (p = 0.008). 39 A cross-sectional study conducted by Roepke and colleagues 42 also showed that the duration of care was positively associated with IMT of the carotid artery (p = 0.044).
Other factors that may increase the risk of CVD in family caregivers of PWD are TT genes, sex, and race. In one study, the TT genotype was associated with more adverse levels of waist circumference (p = 0.026), triglycerides (p = 0.001), and HDL cholesterol (p = 0.001) in caregivers, which indicated that the TT genotype was associated with a higher risk of CVD. 53 Four studies reported that African American caregivers were at higher risk of suffering from hypertension and CVD than Caucasians.30,49,54,55 One study also showed that female caregivers showed greater systolic BP and diastolic BP reactivity to a laboratory-based stress task (i.e., discussing caregiving difficulties) compared with male caregivers (p ≤ 0.01). 56 This finding suggests that female caregivers experience greater BP reactivity to caregiving-related stress than do male caregivers.
Discussion
The results of this systematic review showed 10 factors that were associated with the risk of CVD in 3689 family caregivers of PWD. These factors were sex, genes, race, caregiving status, duration of caregiving, stress and depressive symptoms, negative life events, self-efficacy, coping strategy, engagement in pleasant activity, and physical activity. Identifying and understanding the risk factors before implementing interventions is important. This protects caregivers from the negative consequences of caregiving tasks.
In this review, four studies showed that caregivers experienced a higher risk of CVD than did non-caregivers.24,36,50,51 A long duration of caregiving (>4 years) is likely to increase the risk of CVD among caregivers. Additionally, female caregivers, older caregivers, and African American caregivers have a higher risk of developing CVD than their counterparts. Even though caregiving conditions, sex, age, and race cannot be changed, there are other ways of decreasing the risk of CVD in family caregivers of PWD. These methods include reducing stress, improving self-efficacy and coping strategies, promoting leisure activities, increasing physical activity, and providing more social support.
Six studies that were included in this review showed that psychological stress and depressive symptoms were likely to increase the risk of CVD in family caregivers of PWD.31,43–45,48,57 Prospective studies that were conducted in initially healthy adults supported the positive relationship between long-term stress and CVD morbidity and mortality.58,59 The positive relationship between the number of recent negative life-events and CVD risk, and the positive relationship between stress and CVD risk31,45 were well established in these studies. Family caregivers normally experience a higher level of stress than do non-caregivers.60–62 Reducing stress is not only beneficial for psychological health, but also helpful for physical health in family caregivers of PWD. Therefore, reducing stress is at the top of the agenda in family caregivers of PWD.
Self-efficacy is negatively related to depressive symptoms in family caregivers of PWD. 63 Improvement of self-efficacy has the potential to reduce BP in family caregivers of PWD. 47 Self-efficacy is an individual’s assessment of his or her ability to successfully master a specific task. 64 Coping self-efficacy is a form of self-efficacy, which is relevant to caregivers, because it relates to the degree to which they believe they can carry out the tasks that are necessary to cope with a challenge. 65 Bandura et al. 66 demonstrated that high levels of coping self-efficacy were able to reduce BP and cardiometabolic reactivity in the short term. Coping self-efficacy is likely to moderate the negative effects of stress on CVD in family caregivers of PWD. 48 Stressed caregivers who experience a higher level of self-efficacy are at lower risk of CVD. 48 This similar condition also occurs at different levels of AR. The duration of caregiving is significantly positively related to cardiac risk when social and recreational AR is high, but not when AR is low. 39 Therefore, clinicians should make the effort to conduct psychological counselling and psychotherapy to improve self-efficacy in family caregivers of PWD periodically. Furthermore, decreasing social and recreational AR, as well as increasing pleasant leisure activities, are required to reduce the risk of CVD in caregivers.
Increasing engagement in pleasant leisure activities has the ability to reduce stress and CVD risk in family caregivers of PWD.22,46 This finding was also proven by a randomized, controlled trial as follows. Moore and colleagues 67 performed a behavioral activation intervention, which aimed to increase engagement in pleasurable activities and then to decrease the depressive symptoms and CVD risk (IL-6) in family caregivers of PWD. Caring for relatives with dementia may increase family caregivers’ perception of not being able to have sufficient time and energy to engage in social and recreational activities, thus increasing their depressive symptoms.68,69 Increasing participation in pleasurable events is the main component of cognitive-behavior therapy, and enhancing positive activities (i.e., behavioral activation) effectively reduces depressive symptoms in different types of people, including caregivers.70–72 Implementing interventions to increase the engagement of pleasurable activities is likely to produce positive results for family caregivers of PWD.
Physical activity clearly reduces the risk of CVD among the general population. 73 The World Health Organization has pointed out that participation in moderate physical activity (e.g., brisk walking, dancing, caring/moving moderate loads [<20 kg] for 150 minutes each week [or equivalent]) is estimated to reduce the risk of ischemic heart disease by approximately 30%.74,75 For family caregivers of PWD, performing physical activity can also decrease the risk of CVD. 35 A study showed that an intervention of moderate-intensive physical activity (four 30- to 40-minute exercise sessions per week of primarily home-based brisk walking) significantly reduced BP in female family caregivers of PWD compared with those who were provided with nutritional education. 76 Performing physical activity can decrease the risk of CVD and lower stress in caregivers of PWD.76,77 Perceived stress in female caregivers of PWD was significantly reduced by telephone-based exercise intervention. 77 However, caregivers were reported to perform less physical activity than non-caregivers.35,78 Finding solutions to increase physical activity of family caregivers of PWD is important. Family caregivers can achieve a great benefit of performing physical activity to improve their physical and psychological health.
This is the first study to review the factors that are associated with CVD risk in family caregivers of PWD. Compared with risk factors of CVD in non-caregivers, factors that are associated with CVD risk in family caregivers of PWD are focused more on psychological aspects (Table 2). There are similar risk factors of CVD among caregivers and non-caregivers alike, such as physical inactivity and depression. However, researchers have previously focused their attention on psychological effects, such as AR and self-efficacy on CVD risk in family caregivers of PWD.
This review has several limitations. First, this review only included studies that were written in English. Studies that were written in other languages were excluded. Therefore, risk factors of CVD in family caregivers in other non-English speaking countries may not have been fully represented in this review. Second, this review aimed to examine risk factors of CVD in family caregivers of PWD. Therefore, only cross-sectional and longitudinal studies were included. The causal relationship between risk factors and the risk of CVD needs to be further confirmed in randomized, controlled trials. Third, to improve the effect of interventions, understanding the mechanisms between caregiving situation-related factors and CVD risk is important. Without knowing the mediating effect, developing an appropriate intervention will not be possible. Even though this review reported some moderating factors (e.g., self-efficacy and AR) between stress and the risk of CVD, the mediating effect should be investigated further. An example of this effect is that family functioning is significantly associated with psychological distress in family caregivers of PWD, and partially mediates the relationship between objective burden and psychological distress. 79 Therefore, further study could investigate the relationship between family functioning and the risk of CVD in family caregivers of PWD, and then develop appropriate interventions accordingly. Fourth, various measures of CVD risk were included in this review, which limited the consistency of the study results. Many CVD guidelines have recommended some forms of risk scoring for planning primary prevention interventions.80–82 However, physicians’ attitudes towards CVD risk assessment, economic issues, challenges when communicating with patients, and patients’ understanding of risk affect the selection of assessment tools. Therefore, all studies are unlikely to choose the same measurement of CVD risk in family caregivers of PWD. However, future studies should consider whether their assessment is comprehensive enough to measure the risk of CVD.
Implication for future research and clinical practice
Family caregivers of PWD experience a higher risk of developing CVD compared with non-caregivers. Psychological and physical interventions have shown a promising probability of improving CVD and psychological stress in family caregivers of PWD. Further interventional studies should investigate whether the risk of CVD can be significantly reduced after decreasing the risk factors. More comprehensive interventional studies are required to examine what type of intervention is more effective in decreasing the risk of CVD, as well as psychological stress in family caregivers of PWD. More longitudinal studies should also be performed to investigate the causal relationships between other factors (instead of caregiving status) and CVD risk in family caregivers of PWD.
To decrease the risk of developing CVD in family caregivers of PWD, psychologists and psychotherapists are required to help family caregivers to decrease their stress level and depressive symptoms. Psychologists and psychotherapists could also help caregivers to adopt ways of improving their self-efficacy, such as providing cognitive-behavior therapy and other psychological and psychosocial intervention (e.g., educational interventions, individual coping strategies, supportive therapy). 83 Social and clinical workers could also use behavioral activation intervention 84 and leisure education 85 to promote pleasant leisure activities among family caregivers of PWD, and thus reduce CVD risk among them. Additionally, physical activity programs 86 should be provided to family caregivers to reduce their risk of developing CVD. Support for the findings of this systematic review is likely to encourage new approaches to promote techniques focused on reducing the risk of CVD and to lessen the negative health consequences associated with caring for a family member with dementia over a long period of time.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.