
Abstract
Introduction:
In the home care sector, remote care monitoring (RCM) is emerging as a solution to improve client health outcomes and wellbeing, and support system capacity. Previous research has identified that patient and provider perspectives on RCM impacts its implementation, yet these dynamics have received little attention in home care research. This exploratory qualitative descriptive study aimed to understand home care nurses’ pre-implementation perspectives on RCM to support its future use.
Methods:
Fourteen nurses at a home care organization in Ontario, Canada were interviewed. Interviews were analyzed using inductive content analysis.
Results:
Four descriptive categories were identified: (1) participants viewed their role in supporting RCM through the lens of what they valued as home care nurses: supporting client health and wellbeing and forming connections with clients. Participants expressed positive sentiments about the potential to participate in RCM as part of their educator role. (2) participants had perspectives on clients’ readiness for participating in an RCM program, and caregivers were viewed as playing an important role supporting clients to use RCM. (3) participants expressed concern about supporting RCM if it led to a reduction in in-person care and (4) identified a need for clarity around responsibilities for responding to RCM alerts.
Conclusions:
These findings suggest examining RCM programs through a person-centered and relational lens. Further, home care organizations should consider aligning education and training for healthcare providers with what matters most to them: client wellbeing and the quality of care.
Introduction
Canadian health systems are increasingly using remote care monitoring (RCM) to support system capacity and strengthen patient care.1,2 RCM involves the remote tracking of patients’ health data, which is then shared with healthcare providers. 1 Research on RCM has demonstrated its potential to support access to care and the management of chronic conditions, improve patient safety, 3 and reduce acute care use.1,4 As RCM programs in the home care sector develop as a way to improve care quality, coordination, and system capacity,5-7 there is a need to identify and understand best practices related to their implementation.4,8
Digital programs like RCM are complex interventions, with multiple, intersecting factors impacting their implementation, including those beyond the technology itself.4,9,10 In particular, recent research has examined patients’ and providers’ perspectives on digital health to identify enablers and barriers related to usability.9-11 RCM can facilitate improved communication between providers and patients, which in turn supports adherence.3,4 Patients also report increased feelings of safety and comfort from being monitored by health providers.12-15 Simultaneously, face-to-face care can help establish rapport and trust with providers, and patients are concerned about the replacement of in-person care with RCM. 14 Healthcare providers play an important role in supporting patients’ acceptance of RCM.11,16,17 A recent systematic review identified that health providers thought RCM improved patient education and self-empowerment, contributed to effective communication, and supported the earlier identification of health issues. 17 However, providers also expressed concerns related to increased workload, RCM’s appropriateness for some patients, and data accuracy and security. 17
While there is substantial research on RCM, the home care sector is underrepresented in this literature. Home care is highly relational and person-centered: providers care for clients over extended periods, leading to clients and families viewing them as close and trusted advisors. 18 The home care setting also allows providers to adopt a person-centered approach to care and well-being that is built around the individual and their family’s needs in a holistic way. 19 How RCM will impact these dynamics in the home care setting remains largely unknown. With RCM implementation in its early stages, there is an opportunity to improve our understanding of the potential role of home care nurses to support clients in adopting and sustaining use of RCM. This study examined home care nurses’ perspectives on the future implementation of RCM. While at times the terms patient and client are used interchangeably, the term “client” will be used when referring to the home care context of this study.
Methodology
Study Design and Aims
This study adopted a pragmatic, exploratory qualitative design20,21 using semi-structured interviews with home care nurses, analyzed with inductive content analysis. 22 Ethics approval was obtained from the University of Ottawa Research Ethics Board. Reporting of this study follows the SRQR guidelines. 23
This study occurred in partnership with a large, not-for-profit home care service organization in Ontario, Canada that provides nursing, personal support, rehabilitation, and community support services. At this organization, registered nurses (RNs) and registered practical nurses (RPNs) provide care to a diverse client population. At the time of the research, the organization had selectively piloted RCM, so most nurses did not have RCM experience. Nurses had experience with other technology including virtual care and e-health records. Collaboration with the study site included consulting with organizational leaders and support for participant recruitment.
Reflexivity
The principal researcher (TT) conducted this research as part of her graduate education and was also employed at the study site in a senior leadership role. She had no supervisory relationship with nurses at the organization. Participants were informed at the time of recruitment and before each interview that participating in the study was voluntary, confidential, and would not have an impact on their employment. To consider her insider role in the organization, she engaged in reflexive journaling throughout data collection and analysis to thoughtfully explore how the research process or analysis was impacted by her role in the organization.
Sampling and Recruitment
Convenience sampling techniques were used to recruit participants. RNs and RPNs were eligible to participate if they had been employed at the study site for at least 3 months. Participants did not need to have prior RCM experience. Recruitment lasted from October 2023 to January 2024. Approximately 500 nurses were emailed a study invitation through the organization’s internal email listserves. Follow-up emails were sent throughout the recruitment period. [TT] attended 2 virtual nursing team meetings to supplement recruitment. Recruitment occurred alongside data analysis and ended when there was sufficient data to answer the research questions and no further insights were identified with subsequent interviews.
Data Collection
Potential participants emailed to volunteer for the study and were provided with additional study information. Twenty-four individuals expressed interest in the study, and of these, 14 decided to participate. Standard informed consent procedures were followed and informed consent was obtained in writing and verified verbally at the beginning of each interview. Each participant received a $40 gift-certificate for participating. Interviews lasted between 30 and 60 minutes and were conducted by the principal investigator. One interview occurred via telephone and the remaining were conducted over Microsoft Teams. All interviews were audio-recorded and transcribed verbatim. Participants were offered the opportunity to review their transcripts; however, none edited their transcript.
An interview guide was developed based on a literature review and discussions with organizational stakeholders. Open-ended questions included topics such as: participants’ understanding of RCM, their perspectives on clients who might benefit from RCM, and perspectives on their potential role in supporting RCM implementation. All participants were provided with a general definition of RCM and, for participants who were unfamiliar with RCM, the principal investigator reiterated the explanation as necessary and adapted interview questions to encourage participants to consider the potential future use of RCM. RCM was described to all participants in the consent materials and during the interview as: “the tracking of symptoms and vital signs and the electronic transmission of that information to a healthcare professional.” The complete interview guide is included in an Supplemental Appendix. Reflexive and analytical memos were taken during and after the interviews and were included as part of the analysis.
Data Analysis
Data analysis followed an inductive content analysis process. 22 The principal investigator began by reading and becoming acquainted with the data, followed by descriptive and line-by-line coding guided by the research objectives. Codes were then organized to identify common patterns, similarities and differences, creating broad categories that were then analyzed to identify sub-categories. In the final stage of analysis (synthesis and interpretation), other members of the research team supported the analysis of the categories and sub-categories in relation to the study aims and generated a narrative for each category. Trustworthiness was achieved by providing detailed information about the study methodology and procedures, engaging in reflective journaling, and presenting findings with quotes to support transparency.24,25
Results
Participant Sociodemographic Information and Experience with RCM
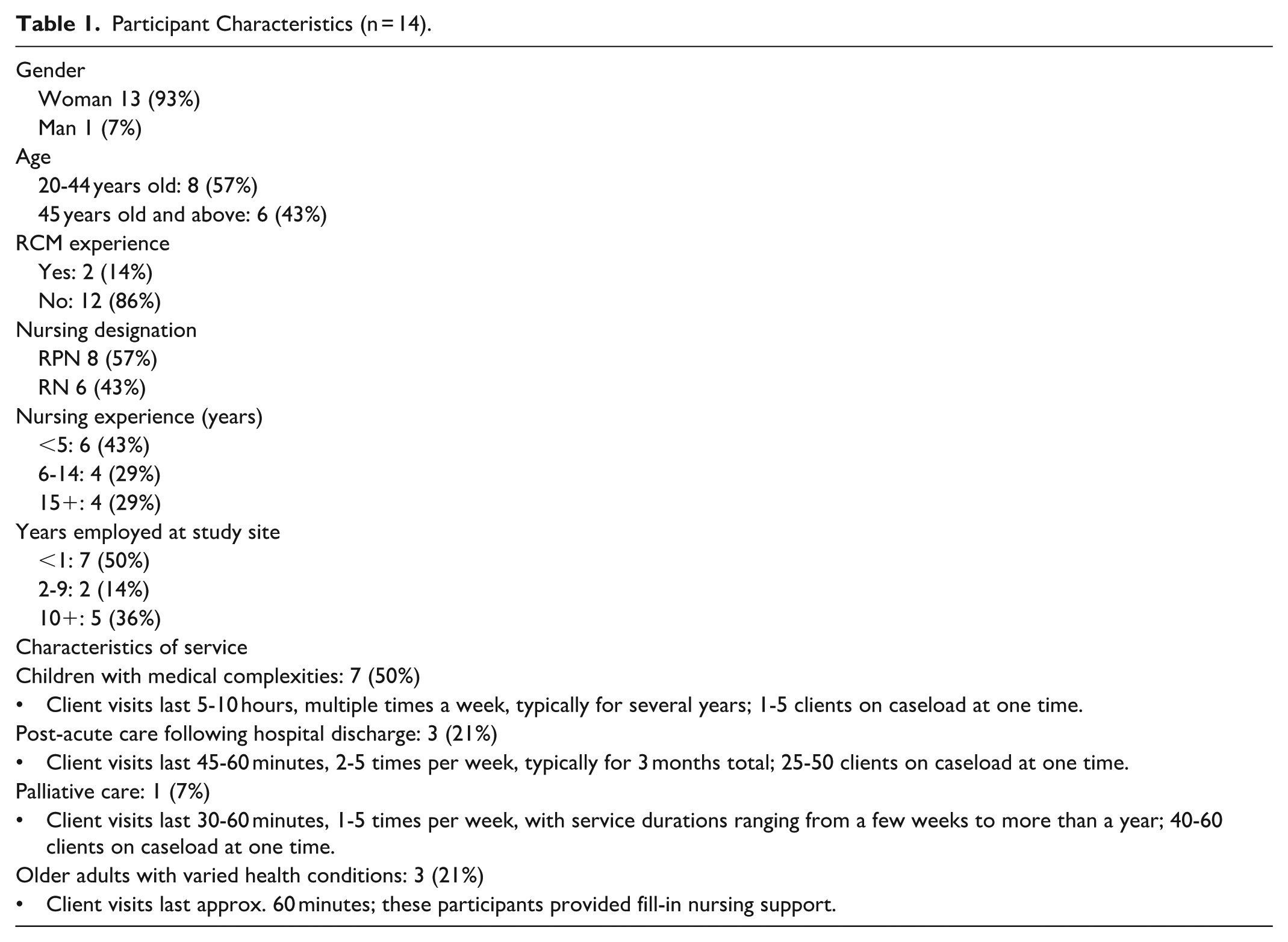
Fourteen nurses participated in this study (see Table 1: Participant Characteristics). Most of the participants were women, and they ranged in age, years of experience, and years employed at the study site. Two participants had experience with RCM programs; the remaining 12 did not have any previous experience with RCM and were reliant on the description provided by the researcher.
Participant Characteristics (n = 14).
Nurses Value Improved Client Outcomes, Wellbeing and Connection
Participants viewed their possible role in using RCM with clients through the lens of what they valued as home care nurses: improving client health outcomes, supporting their overall wellbeing, and forming connections with clients. Participants described that in some cases they provided care for long-term periods: I’ve worked in the same school for 20 plus years, so I get to know the kids, how they grow. You get to know them, what will make them happy and what will make them sad. The parents come to treat you as the child’s second mom. It’s about making a little difference in their lives and you feel good that you have done something for somebody. (Participant 2)
Participants expressed support for the use of RCM if it could allow them to better support clients. Participants shared that they were often concerned about clients’ safety, even outside of visits. Some participants indicated that they regularly received phone calls from clients or family caregivers between visits to discuss health concerns. Some participants saw the potential for RCM to increase their confidence in clients’ safety between visits and the possibility for enhanced connection and communication: I feel like it would form a bond. The client would trust us, and they would have peace of mind that hey, somebody is at least looking out for us, monitoring us, checking for abnormalities. (Participant 14)
Participants felt that the possibility of access to additional client information through RCM could positively impact client care. For example, some participants saw the opportunity for RCM to support clients living with health conditions that required daily self-management. One participant thought that RCM might allow them to have a baseline set of vital signs for their clients or have access to vital signs before client visits to help them prepare. Another participant saw the potential for RCM to identify changes to their client’s health.
I can see it definitely being useful, especially because the nurse that the family was working with knows the client very well, so they would be one of the first people to also recognize that this is a different symptom or it’s out of the norm. (Participant 1)
Participants anticipated that RCM could facilitate communication across different providers caring for the same client.
It would be useful in terms of having up to date readings and also for transitioning when one nurse is on vacation or when we’re off on the weekend or sick day or whatever the case may be. Continuity of care would improve with a system like that. (Participant 7)
Several participants also said that RCM could enhance communication with clients and their families, particularly outside of in-person visits: I think it will have a positive impact, like you’re working with them more. You’re seeing how their health fluctuates and you’re getting to know their norms more and you’re also communicating with their family more. (Participant 1)
Participants saw the potential for RCM to allow them to further develop their role as educators in the home, which they described as an important part of care. While participants noted that RCM education could increase workload, they did not express concern about this possibility. Rather, participants felt they wanted to be a resource for clients.
I think it would be a great education opportunity for nurses to inform the family about why we’re doing this and how it can help them. (Participant 6)
Nurses’ Perspectives on the Need for In-person Care
Participants felt strongly that their clients needed in-person care and unanimously expressed concerns about supporting RCM if it reduced in-person visits or had a negative impact on the quality of care. A participant who supported a child living with medical complexities and their family stated: My client’s family feels most comfortable with the presence of a nurse. They wouldn’t be happy if it [RCM] led to any reduction in the physical presence of a nurse. (Participant 3)
In part, participants viewed that RCM could not replace the type of in-person care they provided because the nature of the care involved supporting family members or providing respite care: That’s why we’re there, to support the family. Sometimes they just need a break, even to be away from the child for a few minutes. (Participant 2)
Participants described how home visits allowed them to see in their living environment, providing them with information that had an impact on their subsequent care. In-person care allowed them to develop a connection and familiarity with clients that informed their clinical judgment: It’s great to see stats. It’s great to monitor that sort of stuff, but at the end of the day, someone’s blood pressure might be a little lower than normal and that might not raise a red flag if I’m just looking at a set of numbers. But if I’m there and I see it’s lower and then I look at the client and I know him – normally he’s alert and joking and today he seems like he’s barely able to keep his head up – then I know something’s wrong. Technology can’t replace nursing judgement. I wouldn’t feel comfortable replacing a visit with RCM. (Participant 7)
Nurses’ Perspectives on Client Readiness for RCM
Many participants thought that their clients and family caregivers’ comfort and availability to use RCM would be an important consideration for its future use. All participants thought that the availability, ability and openness of family caregivers would be an important consideration for supporting clients to use RCM. Some participants also described situations in which they hoped RCM could offer reassurance and comfort to family caregivers who were worried about their client’s well-being.
At the same time, several participants thought that caregiver burnout could be a possible challenge for RCM implementation. For example, 1 participant described a situation where families were providing constant care for their children with medical complexities, and RCM could be viewed as additional work: Mom would not want to do tracking herself because her workload is quite heavy. It would feel like more work rather than a benefit. (Participant 3)
Several participants believed that some older adults may not be receptive to RCM due to personal preference, barriers to using technology, or the perceived need for interpersonal connection: Someone who was older would rather just call in and speak to a live person because there’s none of that personal concern when you’re just putting symptoms into a system, it feels a little disconnected. (Participant 10)
The Need for Clarity Around Roles and Responsibilities
Throughout the interviews, participants described aspects of RCM requiring clarity should it be implemented in their practice. Several participants were concerned about the potential impact on work-life balance if nurses were able to or expected to check on RCM between shifts: A lot of nurses tend not to be able to balance work and life. So as long as they have that [balance] and they’re not working overtime constantly checking RCM. (Participant 1)
Participants had questions regarding their role in supporting an RCM program and how responsibility and accountability for responding to alerts would be managed. Some participants thought it might be beneficial if a client’s regular nurse was the one to receive RCM alerts. However, others suggested that data should also go to multiple individuals to ensure information wasn’t missed.
Discussion
This study found that home care nurses’ perspectives of RCM were centered around client wellbeing, the quality of care, and nurses’ connection with clients and family caregivers. A central finding of this research—that healthcare providers were concerned with how technology impacted the quality of patient care and their interactions with patients—is consistent with existing research on RCM.1,11,26 Healthcare providers may resist using technologies they do not think their patients will be comfortable with, 11 further stressing the importance of understanding providers’ perspectives at the outset of implementation.
This study adds to the literature examining RCM programs from the perspective of relational care. RCM programs consist of a multitude of practices undertaken by patients and providers that are much broader than the technology itself.27,28 Consideration of the practices that surround the use of the RCM technology allow us to understand its nuanced and varying impacts on patient-provider interactions and relationships, 27 and importantly, identify ways to ensure that RCM programs enhance the quality of interactions and communication between providers and patients. Offerman et al’s 29 “caring” framework for RCM offers a potential starting point for ensuring that future RCM programs are grounded in a holistic, relational approach that centers around client and caregiver perspectives and needs. The need for this kind of approach to program design was strongly supported by our participants’ focus on how the use of RCM could influence their relationships with clients and the roles played by family caregivers. Given it is widely acknowledged that understanding and incorporating the perspectives of patients and providers when designing RCM programs is a key step in ensuring RCM programs are effective,1,4,11,14 there is an opportunity for home care sector organizations to design RCM programs using participatory and co-designed approaches.
This study highlights the need to tailor education and messaging about RCM to nurses’ priorities and experiences. For instance, RCM is often positioned as a way to support system-level challenges. 1 However, this study indicates that providers are primarily focused on clients’ health and well-being rather than system-level pressures. This suggests an opportunity for home care sector organizations to align communication about RCM with what resonates most with nurses: improved outcomes and enhanced care for clients and families. Further, this research found that some participants viewed older adults as being less receptive to using RCM. This stands in contrast to prior research conducted directly with older adults which has revealed an openness to using remote monitoring technologies. 30 This suggests that nurses may underestimate older adults’ receptivity to technology which may be based on unfounded assumptions and can create or exacerbate barriers for older adults using health technology. 31
A limitation of this research was that nurses were only sampled from one home care organization, and their views were based on their experiences with the client populations they most commonly served. Many participants did not have prior experience with RCM, and their perceptions of RCM were supported by the definition provided. Future research should consider the perspectives of home care providers with greater experience using RCM, those from other disciplines, and providers at a wider range of care delivery organizations.
Conclusion
This study highlights the importance of understanding nurses’ perspectives on RCM when designing its implementation. By speaking directly with home care nurses, this research identified that their priorities related to RCM implementation were grounded in a deep understanding of the complex and multifaceted support needs of their clients and their families. These findings point to the need for a relational approach to designing RCM programs and the potential role that nurses can play in promoting RCM programs which can strengthen their connections with clients and ability to deliver a high quality of care.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223261424419 – Supplemental material for Home Care Nurses’ Views on Remote Care Monitoring at the Pre-implementation Phase
Supplemental material, sj-docx-1-hhc-10.1177_10848223261424419 for Home Care Nurses’ Views on Remote Care Monitoring at the Pre-implementation Phase by Tracey Turriff, Sandra M. McKay, Madison Brydges, Emily C. King, Sylvie Grosjean and Maria Cherba in Home Health Care Management & Practice
Footnotes
Acknowledgements
Thank you to various members of the leadership team at VHA Home HealthCare for providing helpful guidance and background on organizational processes related to remote care monitoring. Thank you to Sonia Nizzer on the research team at VHA Home HealthCare for contributing to early phases of the study design.
Ethical Considerations
Ethics approval was obtained for this study from the University of Ottawa Research Ethics Board (approval #S-09-23-9516).
Consent to Participate
Informed consent was obtained in writing and confirmed verbally prior to participation.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tracey Turriff, Sandra M. McKay, Madison Brydges, and Emily C. King are employed by the organization at which the research was conducted.
Data Availability Statement
The data informing this study is not available to share as it contains potentially identifiable information about participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.