
Abstract
The availability of personal support workers (PSWs) is a limiting factor for home care system capacity, as this workforce provides 70% to 80% paid care in this sector. Without sufficient support to live at home, many seniors and people with disabilities experience poorer outcomes and require care in more expensive and less preferred institutional long-term care or hospital settings. Insufficient PSW availability is limiting access to necessary care in the community. Capacity challenges are particularly pronounced on weekends. The Essential Care on Weekends (ECoW) program was co-developed as one solution to adapt current PSW scheduling practices to increase the number of clients with high-intensity care needs who can be served within the constraints of PSW availability. ECoW focused on increasing weekend capacity and care consistency, particularly for clients with the highest care needs, through prioritizing essential care and moving less time sensitive tasks to weekdays. ECoW was operationalized through 4 activities: communication and engagement, clinical care plan review, geographic review of PSW schedules and the creation of the ECoW schedule. Implementation of ECoW demonstrated success in increasing access to and consistency of care for clients with the highest care needs: weekend capacity increased, access to care improved for clients requiring daily or near-daily care and missed care rates decreased both on weekends and weekdays. This strategy represents a change in scheduling practices that organizations can use to provide consistent service to a growing number of clients with high-intensity care needs in the context of increasingly limited health human resource capacity.
Keywords
Introduction
Demand for home care is increasing with an aging population that values remaining at home,1,2 and with growing recognition of the health, social and economic benefits that home care offer.3-5 The availability of personal support workers (PSWs) is a limiting factor for home care system capacity, as this workforce provides 70% to 80% paid care in this sector. 6 PSWs are direct care workers who provide personal care, assistance with medications, complex lifts and transfers, home exercise routines and meal preparation to support people to remain safe in their communities and are also referred to as home support workers, homecare workers, and home health care aids in other jurisdictions. 7 As of 2022, demand for home care in Canada exceeded supply by 50%, 7 and growth in demand for personal support services is projected to outpace growth in the PSW workforce by a factor of nine. 1 Already, access to care is worsening as indicated by falling referral acceptance rates in the home care setting, 8 linked to insufficient PSW availability.
Without sufficient support to live at home, many seniors and people with disabilities experience poorer outcomes and require care in more expensive and less preferred institutional long-term care or hospital settings,8-10 which are also facing substantial capacity strain. 11 In Ontario, this has contributed to an estimated 15% of hospital beds being occupied by patients who no longer require acute care but remain in hospital due to the “reduced and insufficient capacity in institutional long-term care and home and community services.”12,13
To increase the home care sector’s capacity to meet demand, innovative operational approaches are needed to provide as much care as possible given current health human resource challenges. Essential Care on Weekends for personal support (ECoW) was developed as one solution with a goal of revising current scheduling practices for weekend personal support (PS) to increase the number of clients with high-intensity care needs who can be served within the constraints of PSW availability. This paper shares the ECoW program structure and findings from implementation to guide other home care organizations who wish to consider this approach.
Intervention Development
In Canada, where healthcare is a provincial responsibility, the provinces and territories fund home care services which are often privately delivered. In Ontario, the agency with primary responsibility for home care is Home and Community Care Support Services (HCCSS), which contracts with the service provider organizations that deliver publicly-funded care. 1 Service provider organizations employ healthcare providers, including PSWs, to deliver authorized hours of service to clients based on their needs as assessed by HCCSS. 1 These service provider organizations are experiencing increasingly acute health human resource challenges which were exacerbated by the COVID-19 pandemic and related public health measures, such as school closures. 14
The ECoW program was developed and evaluated within one large Ontario not-for-profit, home care provider organization that delivers approximately 3 million care visits per year. At this organization, the shortage of PSWs raised concerns about the ability to accept new clients – particularly those being discharged from hospital and requiring a higher intensity of service—and concerns about rising rates of missed care, particularly on weekends. The intervention was developed through a rigorous engagement program involving (1) interviews and focus groups with client partners, supervisors and point-of-care staff and (2) multiple facilitated “FastLabs” sessions (rapid modified design sprints) with point-of-care providers, supervisors, managers, and scheduling coordinators, to brainstorm and identify promising solutions to address ongoing weekend PSW human resource shortages. The draft model was thoroughly reviewed in collaboration with stakeholders at the regional HCCSS to ensure alignment of goals and approaches.
These sessions aimed to find a balance between the needs of clients and the availability of providers. While meeting client needs has always required some weekend care, the increasing complexity of homecare clients, a greater number of whom require daily or multiple daily visits, increased the intensity of weekend demand on the personal support workforce. The organization faced an ethical and contractual responsibility to ensure clients whose needs required high-intensity services (daily, or near-daily personal support as identified by HCCSS) were prioritized for weekend care. These clients often have complex needs associated with medical frailty, functional deficits and requiring support for activities of daily living such as transfers, toileting, feeding, and medication management. For clients with limited family and social supports, access to PSW care is essential for safety. For care providers, there was a recognition of the need to respect their physically and emotionally demanding role, their personal and family responsibilities, and the logistical and financial challenges that weekend work presents (e.g., cost of childcare).15-18 In light of these considerations, and recognizing that, for clients and families, care was more than a “visit” to be scheduled, it was determined that weekend care would be restricted to what was essential and could not be addressed during the week to allow care to be provided to as many high-intensity clients as possible.
Intervention
ECoW focused on increasing weekend capacity and care consistency to provide service to clients with the highest care needs through prioritizing essential care. One strategy was rescheduling PSWs into smaller geographies to increase the efficiency of PSW schedules by decreasing gap times between clients, thereby increasing the number of clients they could visit. A second strategy was to assess whether clients scheduled for weekend care could have their care safely rescheduled to weekdays when higher capacity was available. The third strategy was to focus on providing essential care required for client safety; less time-sensitive services, such as laundry, routine bed linen changes and exercise routines were moved to the weekday care plan. The fourth strategy involved collaboration with the HCCSS responsible for the pilot region which supported needs-based care and agreed with travel of less than 15 minutes as part of the “visit” when 1 hour of care is provided. This shift in focus from hours of service to needs-based care was communicated to clients and families as part of a joint review of the weekend care plan to understand each client’s and family’s essential weekend care needs.
With HCCSS’ approval, ECoW was operationalized through 4 activities: communication and engagement, clinical care plan review, geographic review and the creation of the ECoW schedule (Figure 1).
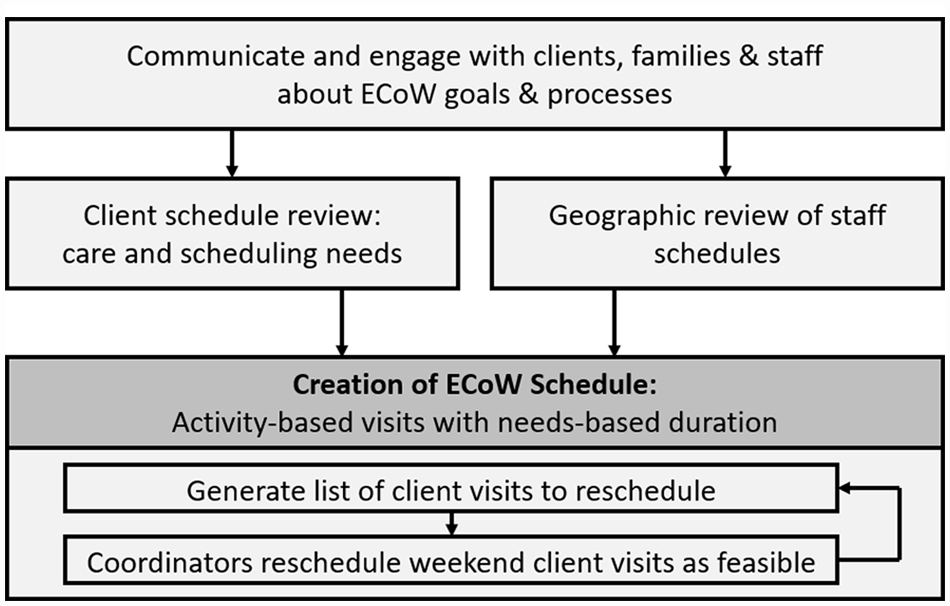
Operational steps required to review and generate ECoW schedules.
The first essential element of the intervention was to communicate the new model for weekend care with clients, families and staff. A robust client and family communications plan included a personalized information letter summarizing the rationale for and possible impacts of ECoW and individual one-on-one conversations and/or home visits regarding potential changes to care or providers. For staff (including scheduling coordinators and PSWs), team meetings specific to ECoW were hosted by supervisors, managers and the regional director to share the program and answer questions.
The decision process presented in Figure 2 was used by the scheduling coordinator and care team supervisor to determine which client visits could safely be rescheduled to weekdays, or assigned to a new PSW whose core geography included the client’s home. To guide clinical and geographical review of client and PSW schedules, the ECoW implementation team provided weekly reports detailing: (1) clients scheduled for weekend care who were receiving service for fewer than 6 days per week, and (2) PSWs scheduled to work outside their core geographies during the weekend. Based on this, the scheduling coordinator and care team supervisor worked together to review the care needs of each client to determine if there were any risks or concerns that could be associated with shifting all visits to weekdays, when greater PSW capacity was available. In cases where PSWs were scheduled to work outside their core geographies on the weekend, and travel could not be completed within 15 minutes, the coordinator and supervisor assessed whether a PSW from the core geography could be assigned. Based on these reviews, the supervisors and coordinators generated a list of client visits to reschedule. Coordinators then realigned client and provider schedules to the degree possible to align with ECoW principles. Recognizing the importance of client-provider relationships to quality of person-centered care, and the risks that disruptions can pose to frail seniors and those living with dementia, client -provider relationships were preserved wherever possible. Where changes in provider were necessary, a toolkit of strategies was developed to ease necessary changes in providers that included home visits, transition planning and shadowing from one PSW to another. For any escalated concerns, supervisors connected directly with affected clients and families to discuss any concerns and needs before implementing any schedule changes.
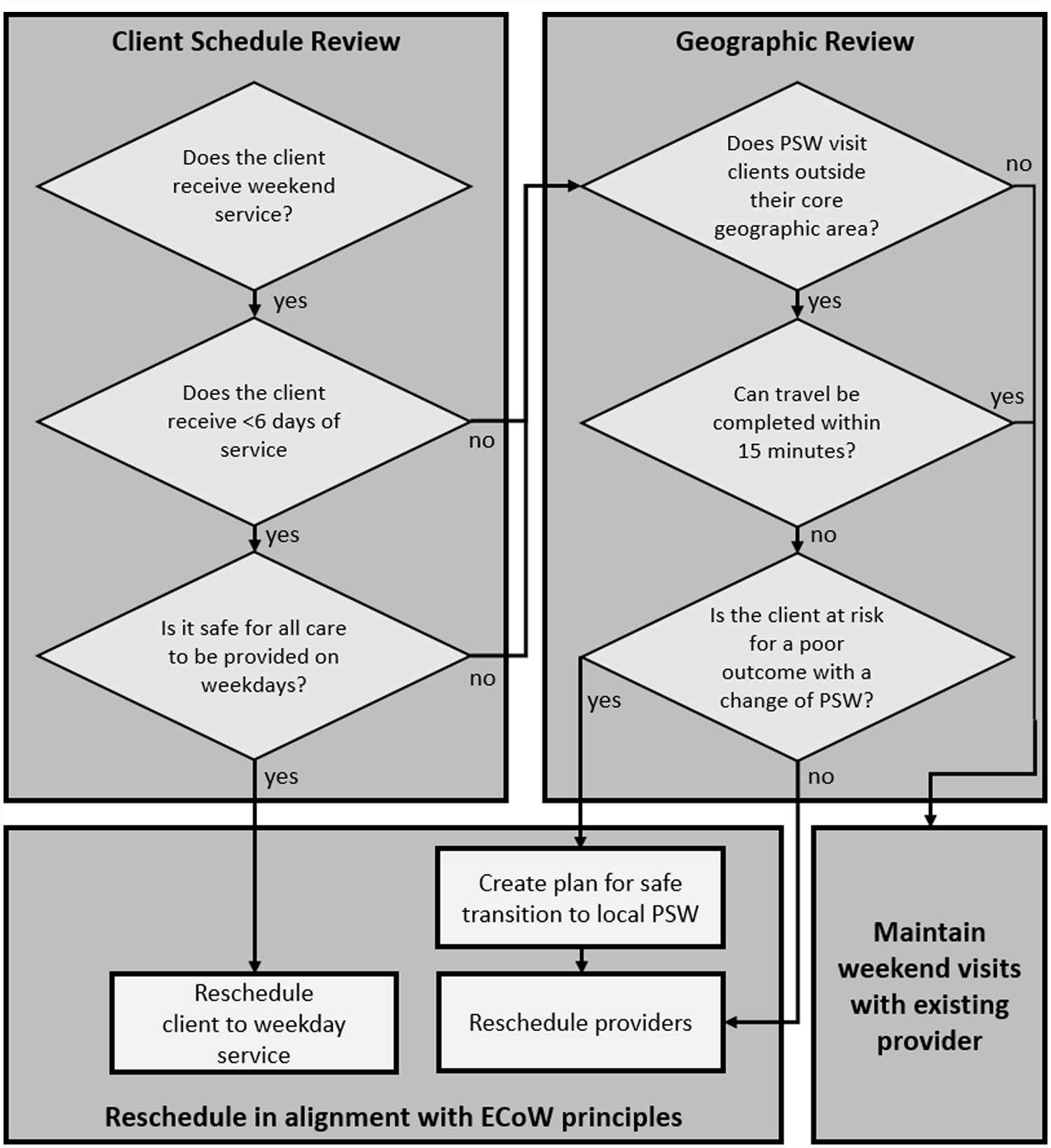
Decision process associated with the clinical and schedule review.
Methods
Prior to ECoW implementation, an evaluation plan was designed to track operational and outcome measures. Operational measures allowed tracking of operational fidelity to the central tenets of ECoW and focused on (1) the percentage of weekend visits that were delivered to clients with high-intensity care needs (those requiring PS care on 6 or 7 days per week) and (2) the percentage of PSWs working outside of their core geography on weekends. Selected outcome measures were used to reflect whether ECoW implementation achieved the desired impacts. These focused on: (1) changes in the percentage of client visits designated as “missed care” (i.e., care was missed and the organization was unable to attend or appropriately reschedule the visit), both during the weekend and on weekdays; (2) PSW schedule stability, as indicated by the number of unassigned weekend visits at the beginning of each week; (3) weekend capacity, as measured by the total number of weekend visits that were delivered each week, and (4) acceptance of PS service referrals for new clients requiring care on 6 or 7 days per week.
A staged implementation, with 1 to 2 teams starting every 1 to 2 weeks, permitted the ECoW steering committee to work closely with each team’s supervisor and scheduling coordinator to support fidelity to the ECoW protocol. A 3-week lead-in period in each team allowed time for communication with clients and families, clinical and geographical review of schedules, and collection of pre-implementation data prior to the launch of schedule changes. Following a 6-week adjustment period after the launch of schedule changes, 3 weeks of post-implementation data were collected.
Results
The ECoW program was phased in over the 10 pilot teams over a period of 17 weeks. Each team was comprised of a supervisor, scheduling coordinators and 35 to 61 PSWs, with each team providing care for 126 to 311 clients/week. Across the 10 participating teams, weekly averages of 443 PSWs provided service to 2136 clients.
The operational measures show that ECoW was carried out as intended. Following implementation, a higher proportion of weekend PSW visits were to clients with higher intensity care needs (95%, an increase of 6.7% over the pre-ECoW rate). Clinical review found that approximately half of clients with lower intensity care needs, who previously received weekend service, were rescheduled to weekdays, permitting a 55% reduction in weekend visits for lower-intensity clients. Following ECoW implementation, only 26% of staff were scheduled for visits outside of their core geographic region, approximately half of the 45% who worked outside of their core geographies pre-implementation.
A key objective of ECoW was to improve service reliability as indicated by reductions in missed care, particularly on the weekends. Following ECoW implementation, there was a 38% reduction in missed care on the weekends. Weekday missed care was also monitored to ensure that this was not negatively impacted by efforts to address weekend capacity; weekday missed care decreased by 40% following program implementation.
Improvements were also seen in PSW schedule stability, the number of weekend visits that were delivered each week, and referral acceptance for clients requiring higher intensity care. Following ECoW implementation, the number of unassigned weekend visits at the beginning of each week was halved, indicating increased schedule stability for both clients and providers. Additionally, a small but significant increase (3.2%, t(29) = 2.69, p = .012) was seen in the weekly number of scheduled weekend visits, indicating a modest weekend capacity increase. This capacity increase was double the 1.6% increase in active PSWs between pre- and post-implementation observations. While the number of new referrals accepted was stable between the pre- and post-implementation periods (t(29) = 2.05, p = .69), there was a 33% increase in the number of accepted clients with high intensity care needs.
Discussion
Essential Care on Weekends is a scheduling optimization strategy focused on travel distance, clinical care needs, and prioritization of weekday visits where possible, that was tested to mitigate home care PSW capacity constraints. It was created to acknowledge and address the consequences for clients of persistent weekend staffing challenges that became more acute than ever through the COVID-19 pandemic. When the care needs of all clients cannot be met due to an excess of demand and a scarcity of resources, it becomes an ethical issue to decide who receives care. 19 ECoW operationalized the values-based health care framework to prioritize the provision of publicly-funded personal support for clients requiring high-intensity care. This strategy provides a clear and ethical structure to guide supervisors and scheduling coordinators to work collaboratively with clients and families to ensure essential care is provided to those who need it most.
There is a current and future need to increase home care capacity for clients with complex care needs. This is driven by a trend to discharge clients from the hospital sooner and with greater medical acuity, combined with an increased number of individuals living with chronic conditions and multiple co-morbidities that is expected to increase in the coming decades. 1
Implementation of ECoW demonstrated success in increasing access to and consistency of care for clients with the highest care needs: weekend capacity increased, access to care improved for clients requiring daily or near-daily care, and missed care rates decreased. Although there was a small increase in staffing over the implementation period, the magnitudes of changes to outcomes exceeded the increase in staffing. It is therefore reasonable to surmise that these changes were enabled at least in part through the reallocation of existing resources with ECoW scheduling. These successes were achieved while maintaining sensitivity to individual care needs (e.g., through flexible understanding of what was considered essential, as this could vary for individual clients), while adhering to the general program guidelines.
ECoW improved the reliability of care both on weekends and during the week; it also improved access to care for clients requiring daily or near-daily PS service. This was enabled by re-scheduling PSWs working outside their core geographic area. With less PSW travel, more care visits could be provided. In some cases, this required introducing a new local PSW to provide weekend service. Acknowledging that this can negatively impact client experience, 20 this was only done following clinical review, with sensitivity and the development of an appropriate transition plan to support the change in PSW. The 26% of PSWs who were still traveling outside their assigned geographies following ECoW implementation were able to complete travel within 15 minutes due to proximity of the client home to geographic boundaries.
While ECoW emphasized the provision of weekend care to clients requiring 6 or 7 days of service per week, clinical review identified that nearly half of clients with less frequent visits who had previously received weekend service would continue to require this (in some cases because they did require daily care, with weekday visits provided by other organizations or private caregivers). This is reflected in the 5% of weekend visits that were delivered to people requiring 5 or fewer visits per week.
ECoW addresses both access to care and issues related to the design of work by shifting care to weekdays where possible and requiring weekend visits when necessary to provide safety-critical care for clients with high-intensity care needs. PSWs, like other health care workers, experience increased strain from weekend work in terms of their safety, family lives, and physical and mental health.15-18 The PSW scheduling improvements achieved through ECoW can also reduce key pain points for providers that have been found to impact home care workforce participation—namely work outside of their assigned geographies. 13 While always aligned with sound operations, sensitivity to the impacts of work on care providers’ work-life balance is of heightened importance during a time when constrained health human resources are a limiting factor in health system capacity and patients’ access to home care.21-23
This evaluation of a novel approach to weekend scheduling focused on the short-term impact of program implementation and was carried out within one geographic region at one not-for-profit home care provider organization. The evaluation is based on administrative data and does not reflect qualitative elements of client and provider experience. Notably though, it was observed that there was no increase in client complaints recorded during ECoW implementation and positive informal feedback was received from PSWs about the impact on their schedules. Possible improvements to total provider compensation due to reduction of gap times and scheduling more clients in their work availability were not addressed through this evaluation.
Conclusion
Essential Care on Weekends is a values-based, ethical and person-centered scheduling optimization strategy that was tested to mitigate home care PSW capacity constraints while prioritizing care delivery to clients with high-intensity needs. Clients and families were informed of the need to schedule weekend care differently and engaged to develop a weekend care plan to address their priority needs. Implementation of this strategy did not require new technology and was supported by a robust communications plan, a clear, ethical decision-making framework for supervisors and scheduling coordinators, and personnel to support change management during each team’s transition.
Other service provider organizations may benefit from the implementation of this program, which leverages changes in scheduling practices to increase the organization’s capacity in the context of increasingly limited health human resource capacity. The implementation of ECoW optimized PSW schedules to improve home care access on weekends for clients with high-intensity care needs. This schedule optimization also had positive impacts for PSWs which included a reduction in travel and gap time, thereby increasing weekend earning potential. These improvements did not require substantial investment; they were achieved through changes in priorities and practices that enabled more efficient use of available resources. Broader use of this strategy holds the potential to increase system capacity to meet the needs of vulnerable clients who rely on home care to remain in their communities.
Footnotes
Acknowledgements
The authors appreciate the clients, families and staff who participated in the focus groups and FastLab sessions to enable model development, as well as the support provided by the Toronto Central HCCSS Directors, Managers and Care Coordinators. Collaboration with all of these stakeholders was vital to the development, implementation and success of this program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.