
Abstract
The Saskatchewan Caregiver Experience Study sought to map the experiences of family and friend caregivers of older adults in the Canadian province of Saskatchewan. This study aimed to capture the lived experiences of these caregivers through a qualitative survey in June and July of 2022. This manuscript analyzes responses from 354 participants to the question: “What is the most challenging aspect of being a caregiver?” An inductive content analysis approach was taken to analyze the data. We identified key challenges related to caregiving in Saskatchewan, Canada, including exhaustion, balancing personal life, navigating complex systems, self-doubt, and caregiving from a distance. Participants emphasized the need for targeted support and interventions to assist them in their caregiving role. Participants’ experiences reflect a need for more supportive measures in healthcare and policy, especially considering the unique demographic and geographic context of Saskatchewan. A paradigm shift is needed toward supporting caregivers to allow older adults to age in place, rather than relying on institutions and care facilities. In the global context, these findings align with the need for culturally sensitive and region-specific support systems, addressing the universal aspects of caregiving.
Background
With an aging population, the number of older adults who need support is increasing. 1 As such, the caregiver experience affects many individuals worldwide. 2 Family and friend caregivers (also referred to as informal caregivers in other literature) are conceptually defined as individuals who provide holistic help to a person who is unable to do so for themselves. 3 While there are positive aspects associated with the caregiving role, 4 caregiving has been described throughout literature as burdensome. 5 Caregiver burden was seminally defined as the caregiver’s emotional evaluation of the caregiving exchange, expressed as the extent to which the caregiver finds it challenging to care for the recipient. 6 Challenges exist with caregiving, which lead to the burden felt by caregivers.
In Canada, almost half of all caregivers (47%) are adult children providing care to their parents or parents-in-law. 7 Moreover, half of all caregivers are also within the age range of 45 to 65, which are considered prime earning years. 8 For caregivers who are of working age, or are included in the “sandwich generation,” it can also be challenging to find a balance between caregiving, work, and personal life demands. 9 In an Australian study, family and friend caregivers were found to spend almost 5.8 hours per day (40.6 hours per week) providing care to their care recipient. 10 Furthermore, a qualitative study of caregivers to persons with Alzheimer’s disease in the United States shared that caregiver participants reported spending an average of 65 hours (range 8-168) in a typical week providing care, 11 indicating a wide spectrum of caregiving time requirements. It is not uncommon for Canadians to be forced to choose between maintaining their paid employment and acting as a family or friend caregiver.12,13 Spousal caregivers to older adults are often older adults themselves. 14 In 2018, almost one-quarter of older adults in Canada provided care or help to family members or friends with a chronic condition or problems related to aging. 15 Some caregivers also face their own health challenges and these individuals are required to harness strength to care for another person while also managing their own care. 16 It comes as no surprise that the demands of the caregiving role coupled with chronic illness create unique challenges for the older adult caregiver. 17
The Saskatchewan Caregiver Experience Study 18 was an exploratory research project that was undertaken to highlight the caregiver experience and gather perspectives of those who are caregivers to older adults in the Canadian province of Saskatchewan. We undertook this study to create a contextual picture of what the current experiences of caregivers are in our province, as well as to highlight implications for future research, practice and policy. Our objectives were to (1) Explore family and friend caregiver experiences in both large urban and small centre or rural areas of Saskatchewan; and (2) Identify Saskatchewan caregivers’ priority support needs. The purpose of this manuscript is to share our analysis of the challenges reported by Saskatchewan caregivers.
Gaps exist in the research surrounding the challenges experienced by caregivers, which we seek to address. This study explores caregiving experiences across a range of situations, including those caring for individuals with various medical conditions and those living at a distance from their care recipients. This diversity allows the study to address gaps related to the wide range of caregiving contexts and the unique challenges each of these contexts presents. While previous studies have indeed explored various aspects of caregiving, the Saskatchewan Caregiver Experience Study aims to delve into the nuanced experiences of caregivers within this specific region. Saskatchewan’s distinct demographic and geographic makeup, coupled with an aging population, presents a set of challenges and needs that may differ from those documented in other regions or at earlier times. The balance of urban and rural populations in Saskatchewan continues to shift, with 32% of the province’s population living rurally in 2021, compared to 70% in 1951.19,20 Distinct demographic and geographic features of Saskatchewan include higher healthcare costs associated with its rural areas, as they face challenges such as lack of access to specialist healthcare services. 21 Saskatchewan continues to grow at a faster rate in urban areas than in rural, 19 which reflects a global trend towards urbanization. 22 As such, there is an ongoing struggle in rural areas with health-related issues and access to healthcare, which is reflective of the unique challenges faced by these communities. 21
This study, therefore, seeks to update and expand our understanding of the caregiver experience in Saskatchewan, addressing gaps in current literature and providing fresh insights that are vital for developing targeted support systems and policies. The exploration of family and friend caregiver experiences in both urban and rural areas, as well as the identification of caregivers’ priority support needs in this specific context, are crucial for a comprehensive understanding of the caregiving landscape in Saskatchewan. This study acknowledges and addresses the dynamic and regional-specific challenges faced by caregivers, thereby contributing to the field of caregiver research.
Methods
The detailed methodology for the Saskatchewan Caregiver Experience Study is described in a separate manuscript. 23 Qualitative description24,25 underpins the design of this study. We aimed to explore the experiences of caregivers in Saskatchewan and identify their support needs. Caregivers of older adults participated in an online survey, adopting a qualitative descriptive approach24,25 under a naturalistic research paradigm. 26 This approach provides detailed summaries of events, ensuring the study findings are closely aligned with the actual data. The study was approved by the University of XX Behavioural Research Ethics Board (Beh ID #3377).
An online qualitative survey was administered via SurveyMonkey. Regarding the representativeness of our sample, the recruitment strategy was crafted to achieve a comprehensive demographic spread. We employed purposive maximum variation sampling, recruiting participants through community newsletters and targeted Facebook advertisements, which allowed us to reach caregivers across diverse geographical strata within the province. We collected demographic data, including geographic location (urban large, urban small/medium, or rural), age of caregiver, age of care recipient, the care recipient’s condition, and the type of caregiving relationship (e.g., caregiving to a spouse, parent, etc.). The survey also posed three open-ended questions regarding: (1) the challenges that caregivers experience; (2) the positive aspects of caregiving; and (3) the support needs and priorities of Saskatchewan caregivers; as well as a fourth question where caregivers could freely express any other experiences or perspectives. This manuscript presents the findings from the survey question regarding the challenges experienced by caregivers. Anonymity in the survey was iterated to participants to encourage candidness and comfort, potentially leading to a more genuine disclosure of personal experiences and challenges.
We used the detailed steps of content analysis provided by Hsieh and Shannon 27 for data analysis. This method involves reading survey responses thoroughly, coding them into categories, and then identifying prevalent themes. The content analysis approach is well-suited for qualitative descriptive studies due to its low interpretative complexity. Our content analysis was inductive in nature. Data were managed and analyzed in NVivo 12 28 qualitative coding software. We employed a bottom-up approach where codes were developed from the data itself rather than being imposed beforehand. This approach aligns with the method described by Hsieh and Shannon 27 where the focus is on deriving codes directly from the text data, allowing themes to emerge organically from the dataset. The data analysis process was initially conducted by SH, under the guidance and regular review of NR. A review of the complete analysis was carried out by LH and SP. Additionally, the coding and preliminary results were periodically reviewed and discussed monthly during monthly meetings with a Saskatchewan-based non-profit organization (XX) and their Caregiver Committee (co-chaired by LH and SP). This process ensured a collaborative environment, enhancing the trustworthiness of our findings.
We used Lincoln and Guba’s 29 literature on credibility, transferability, dependability, and confirmability to ensure rigor and trustworthiness in this qualitative study. In ensuring credibility, regular contact was established and maintained between the first and second authors (SH and NR) during data analysis. As previously mentioned, updates on our data collection and analysis procedures were provided monthly to the entire research team and a local committee of caregivers to older adults. Transferability refers to the ability to demonstrate study findings have applicability in other contexts, 29 which can be achieved through a review of relevant literature. Our previous scoping review of caregiver-identified priorities for support 9 allowed us to understand how the experiences of Saskatchewan caregivers align with caregivers in other geographic contexts. Dependability is described as an audit trail, 29 which was accomplished by keeping detailed notes about the analysis process and recording specific limitations to the study and its data collection. Lastly, confirmability was achieved through salient immersion in the data through adherence to the inductive content analysis process as outlined by Hsieh and Shannon. 27
Findings
Participant Characteristics
N = 355 caregivers responded to the online qualitative survey in June and July of 2022. A total of 354 individuals responded to the question regarding the challenges that caregivers experience. Respondents’ mean age was 61 (range 22-87) and the mean age of their care recipients was 83 (range 55-104). The geographic setting where participants were located was split almost evenly among urban-large, urban-small/medium, and rural (33%, 32%, and 35% respectively). The most common relationship to the care recipient was adult child, followed by spouse. The most common medical condition of the care recipient was dementia, followed by heart/kidney/lung conditions, and cancer. One characteristic that was not collected was participant’s sex and/or gender. Although this was an oversight in our data collection tool, the study’s aims were not to explore or analyze differences in the experiences and perspectives of caregivers based on their sex or gender.
Qualitative Findings
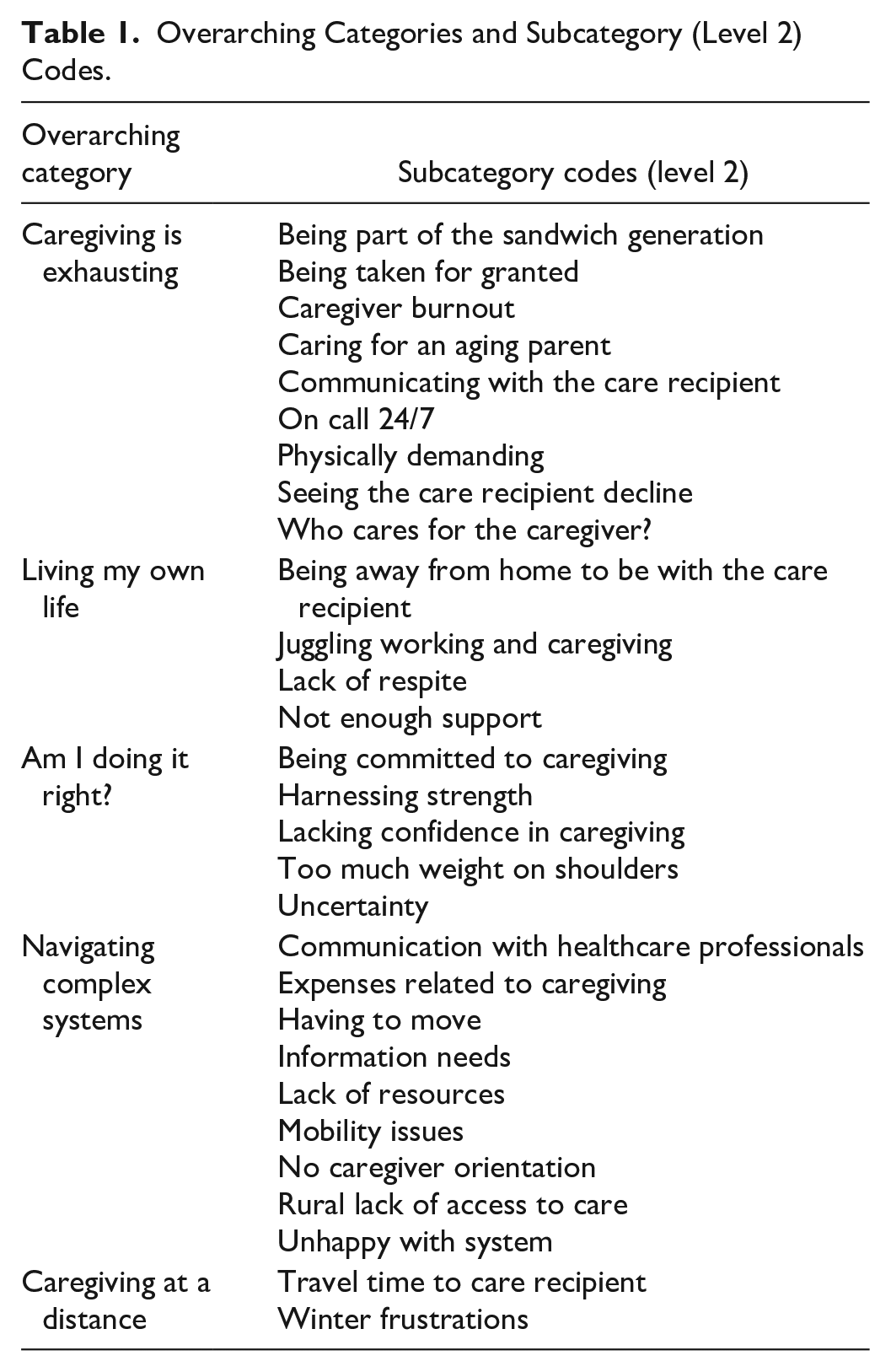
In NVivo, we inductively coded the data collected from the online qualitative survey. Codes were then grouped into three levels. Level 1 was the overarching category, level 2 included codes that became subcategories, and level 3 consisted of smaller meaning units. Table 1 presents the overarching categories and level 2 codes. Our codebook in its entirety is presented in Supplementary File 1.
Overarching Categories and Subcategory (Level 2) Codes.
This study reveals the multifaceted support priorities of caregivers of older adults in Saskatchewan, Canada. Their primary needs encompass not just practical assistance but also emotional support, professional healthcare engagement, and systemic changes in policies and regulations. These insights underline the necessity for a holistic approach in supporting caregivers, recognizing their critical role in the healthcare system. The most emphasized need was for immediate, tangible help in the form of homecare, long-term care, information, and assistance with daily tasks. Many caregivers expressed frustration with the scarcity and inadequacy of available services, especially in rural areas. The high cost and lack of consistent homecare services further compounded these challenges.
The open-ended qualitative survey question in the Saskatchewan Caregiver Experience Study asked participants: “What do you find most challenging about being a caregiver?” The total word count of data collected from this question was 10,327 words, with an average word count of 29 words per response. The range for word counts per response was 1 to 843 words. From our analysis, we found that the overarching categories were: (1) caregiving is exhausting; (2) “living my own life”; (3) navigating complex systems; (4) “am I doing it right?”; and (5) caregiving at a distance.
Caregiving is exhausting
Saskatchewan caregiver participants shared that caregiving is exhausting. Emotions elicited from the burden of caregiving such as sadness and grieving were often reported to be related to loss, such as loss of a social life. Participants also reported feeling guilty when having to place their care recipient in a care home, or long-term care. Many participants reported the significant time commitment caregiving takes, such as being “always on” with a lack of breaks and respite. When the participants do get a break, they reported that their thoughts still wander to their caregiving role, with worries of what could be going on with their care recipient. One caregiver to a parent with dementia and a heart/kidney/lung condition in a large urban setting wrote: “On the rare occasion I have a moment to myself, I’m thinking about mom and her care.”
Feeling overwhelmed
Participants reported feeling overwhelmed by their caregiving role. Some caregivers noted the importance of trying to remain positive, although the responsibilities of caregiving made this more difficult. “Trying to remain kind and positive when you are absolutely overwhelmed. We all feel consumed by others needs sometimes” (Caregiver to a parent in a small/medium urban setting [medical condition undisclosed]). Sometimes participants felt invalidated when their care recipient was unappreciative of their efforts, which contributed to the sentiment of feeling overwhelmed. Isolation is felt by participants when they do not have the support of friends and family or feel as though a support network is unavailable to them. Other participants who did have supportive families still felt isolated due to the time that was invested being away from their family to be with the care recipient, which in turn leads to loneliness. “It really is lonely. Being responsible for everything is really hard” (Caregiver to a spouse with a neurological condition in a rural setting).
Caregiving is emotionally taxing
For participants who had known their care recipient in both sickness and in good health, it was reported that they struggle emotionally watching their care recipient decline. “The anger shown by my wife, who has Alzheimer's, to me, her caregiver. Also, the deterioration. . .” (Caregiver to a spouse with dementia in a large urban setting). Another caregiver stated: “It’s challenging (and trying) to keep from becoming a parent to my parent. It’s difficult watching independence slip away” (Caregiver to a parent with frailty in a large urban setting). Lastly, another caregiver shared: “The mental duress and heartbreak of ongoing care to someone who declines a bit every day. . . scared of them continuing to live and scared of them dying. Being their cheerleader and caregiver while inside I am falling apart” (Caregiver to a parent with dementia, a heart/kidney/lung condition, and frailty in a large urban setting).
“Living My Own Life”
The overarching category “living my own life” includes specific analyses of responses in which participants shared their struggles with maintaining their own lives due to the challenges associated with caregiving. Participants shared that they feel as though there is not enough support from healthcare professionals in different ways.
Lack of support
Some participants felt as though there was a lack of support because healthcare professionals, such as doctors and homecare service providers, sometimes think caregivers can handle the caring situation independently. The lack of access to homecare in both rural and urban settings was mentioned by participants. Limited support from families was a situation that troubled several participants. Participants who care for aging parents recurrently mentioned lack of support from siblings. Sometimes, it was noted that the siblings of the primary caregiver did not believe that the care recipient needed the amount of help they did. Participants cited feelings of abandonment by their families when they were left to live their caregiver experience and care for the care recipient alone. “The biggest challenge I face is the lack of understanding family and friends have of what our life is like” (Caregiver to a spouse with a neurological condition in a large urban setting).
Lack of respite
Lack of respite was a major factor that played into participants’ struggles with living their own lives. Repeated topics within the responses included never getting a break, having no backup, and not having alone time. When the participants reported lack of alone time, they also made comments about how they often, if not always, have to put themselves and their self-care in second place to that of their care recipient: I feel trapped at times. I cannot live my own life without a large amount of preparation including making sure all medications, groceries, everything to do with my mother’s house and finances are in order and that I arrange for someone to cover on call for me. My life falls in second place, and I don’t have that many good years of my own left. (Caregiver to a parent with dementia and frailty in a rural setting)
Social isolation
Participants also cited having no social life, loss of hobbies, and some even said they felt as though they had lost their freedom entirely. “My sister and I are with her daily. The most challenging thing is we have no freedom to have our own lives” (Caregiver to a parent with dementia in a small/medium urban setting). Being away from home to be with the care recipient was also reported to elicit feelings of isolation. Many participants who needed to spend extended amounts of time with the care recipients shared they feel as though they were putting the rest of their family “on the back burner.” Furthermore, because of the lack of respite, participants sometimes miss important life events, or seeing their own children and grandchildren growing up. “There is never a time you can step away. As a caregiver, you are emotionally, mentally, and physically always engaged with those you are providing care to” (Caregiver to a parent with frailty in a large urban setting).
Juggling life and caregiving
Participants reported their difficulties in juggling working at their jobs and caregiving. Some reported even having to quit their jobs due to the demands of their caregiving role. The participants who were adult children caregiving for aging parents reported being in an especially complex situation where they need to juggle their employment, caregiving duties, and being a parent to their own children. “Having to juggle parenting, full-time employment and elder caregiving. I don’t have much time or energy left for myself and my own needs” (Caregiver to a parent with a heart/kidney/lung condition and cancer in a large urban setting).
Navigating complex systems
Fractures in care
Navigating the complex healthcare and governmental systems is a challenge for caregivers. Participants reported frustrations of having to constantly repeat the care recipient’s story, including health history and the acute problem at hand to multiple professionals during the same visit. Participants recognized that the barriers to receiving healthcare in Saskatchewan are plentiful, especially with the increasing staffing issues that the province is facing. As well, a common frustration felt by participants is that the dyad of care recipient and caregiver are not acknowledged as a partnership by healthcare professionals. Participants reported feeling that if they had this acknowledgment, navigation of the healthcare system may be better facilitated: Being the supporter at doctor appointments. More gets accomplished or acknowledged if you, the caregiver, is present which is frustrating since my parent is very capable of communicating their needs themselves. I often have to indicate I’m present for support and [to be the] driver but will express my concerns if I feel there is a need. (Caregiver to a parent living with a heart/kidney/lung condition in a rural setting)
Scarce and hidden resources
The lack of available resources or knowing where to go for resources was a challenge reported by the participants. They shared that it is hard to access long-term care, but also hard to know when to make the decision to place the care recipient in care due to not receiving adequate support and navigation assistance. Furthermore, the participants felt as though the Saskatchewan healthcare system is not oriented to older adults aging in place, as was identified through responses that detailed the lack of resources for aging and older adults. One caregiver in a large urban setting stated that the “system is not set up for our aging population.” Participants recognized that the lack of access to services has also been exacerbated by the COVID-19 pandemic, which shut down many community health programs.
Caregiving has a price tag
Expenses related to caregiving complicate matters further, when participants reported that the current systems offer limited funding, if any. Examples of financial costs that participants incur through their role include household cleaning, preparing meals, transportation (e.g., rural caregivers traveling to cities), renovations to enhance living spaces for mobility, homecare, assisted living, and many more. In addition to these complications, participants reported that lack of tax breaks or government grants for caregivers currently exist in Saskatchewan. “Lack of programs, support, and respite care for caregivers. Very limited tax breaks for caregivers. It costs a lot of money as well as most requiring care have a limited income” (Caregiver to a parent with dementia in a rural setting). Adult children acting as caregivers to their aging parents may also have children of their own, which adds to the lengthy list of expenses.
Rural healthcare challenges
In rural Saskatchewan, with increasing closures of healthcare facilities and rural hospitals, participants report they are becoming frustrated. The rural participants shared they often must travel with the care recipient to large urban centers to receive care, which can also be disorienting to the care recipient to be out of their regular environment. As well, rural healthcare facilities often have limited hours. Participants in northern communities also reported there was an entire absence of care homes in their areas, meaning they had no respite services at all. “[Lack of] support systems, respite care, getting to specialist appointments, financial aspect of maintaining a home and bills while caring for your loved one in a northern community with no respite or care homes” (Caregiver to a parent with a heart/kidney/lung condition and frailty in a rural setting).
“Am I Doing it Right?”
This overarching category encompasses how caregivers often reported a lack of confidence in their role, especially when it came to decision making. Participants made comments towards the concept of “winging it” in their role. As such, feelings of guilt and inadequacy were tied to these responses. “Feeling of guilt, hoping that I’m doing a good job, and wishing for more support” (Caregiver to a parent with dementia and cancer in a rural setting).
Feelings of inadequacy
Some participants felt inadequate when they were facing their caregiver experience alone, or without sufficient help. “Being the lone engaged family member, making it up as I go along, having to set boundaries with care recipients in order not to completely lose myself” (Caregiver to a parent with dementia and a heart/kidney/lung condition in a large urban setting). Participants reported having to take the care recipient into consideration with making any decision, whether it was for the care recipient or themselves. Family dynamics sometimes complicate the caregiver experience, when other family members do not agree with the decisions that are being made by the primary caregiver. “Time demands and expectation that I’m available immediately at all times. Criticism from siblings for being there too much or how things are being done” (Caregiver to a parent with a heart/kidney/lung condition and cancer in a rural setting).
No guide to caregiving
Not having easy access to information or orientation to the caregiving role creates challenges as well. “Always have [to] dig for info and fight hard to get what you want. Policies are often outdated and ask for information that is unavailable” (Caregiver to a sibling with an acquired injury, diabetes, and cancer in a large urban setting). Ultimately, participants reported finding themselves having to harness emotional and physical strength to face their challenges. Participants shared it takes much patience to be a caregiver, especially when forging on their caregiving journey alone. “The dementia journey is long with an unpredictable path. Sheer stamina and my own endurance for the journey was very challenging. Frankly, it’s likely a good thing I didn’t realize how long it would go on” (Caregiver to a parent with dementia and a heart/kidney/lung condition in a small/medium urban setting).
Caregiving at a distance
Caregiving at a distance, although a smaller category, seemed to be important in the context of Saskatchewan caregivers due to the broad geographic distribution of persons within the province. “I have to drive 4 hours to see my mom and I go once or twice a month. It is time and money consuming” (Caregiver to a parent with dementia, a heart/kidney/lung condition, and frailty [caregiver lives in a rural setting]). Regardless of the amount of distance between the caregiver and care recipient, participants reported distance to be a significant challenge.
Moreover, participants who were at a distance from the care recipient reported struggling to get extended amounts of time off work to travel and be with the care recipient. “We share the role with 3 other siblings to my in-laws. Not being in the same city and having to take a week off work a month to provide care is tough” (Caregiver to a parent with dementia [caregiver lives in a large urban setting]). Distance also seemed to be a contributor to further feelings of guilt, when participants had to juggle their time between locations and felt they were not meeting anyone’s needs: Trying to meet my dad’s needs and being his main source of emotional support while living in another community and trying to take care of my other family members while working. I constantly feel guilty about not doing enough to meet anyone’s needs, and I also feel guilty if I take any time for myself. (Caregiver to a parent with dementia, frailty, and mental illness [caregiver lives in a large urban setting])
Discussion
The conceptual definition of caregiving for the Saskatchewan Caregiver Experience Study was provided from the concept analysis by Hermanns and Mastel-Smith. 3 They defined caregiving as a process of helping another person in physical, mental, emotional, and social domains when that person is unable to do so for themselves. 3 This definition highlights the complexities of the caregiving role, which are undoubtedly associated with challenges. Caregivers are challenged by the necessity to adjust to new roles while dealing with unclear responsibilities. 30 As such, it comes as no surprise that participants reported a breadth of challenges exist in their caregiver experience in Saskatchewan. While the challenges identified by caregivers in our study may appear universal, the unique context of Saskatchewan significantly enriches our understanding of these issues. The Saskatchewan Caregiver Experience Study specifically contributes novel insights into the caregiving challenges within this region’s distinct demographic and geographic landscape. Saskatchewan’s caregiver population faces unique obstacles due to its considerable rural expanses, which complicate access to healthcare services and support systems. This geographical challenge is further exacerbated by the province’s demographic shifts towards urban centers, leaving rural caregivers increasingly isolated. By highlighting these unique Saskatchewan-centric challenges and the caregivers’ expressed needs for support, this study contributes significantly to the broader caregiving literature by adding depth to the understanding of how geographical and demographic contexts influence caregiving experiences. This context-specific knowledge is important for developing targeted policies and support mechanisms that can be adapted to similar contexts globally, thus enhancing the practical relevance of our research beyond the provincial scope.
It was clear from participant responses that caregiving can be exhausting and emotionally taxing, which has been iterated in previous literature. Emotional exhaustion is defined as feeling overloaded, unable to continue, and drained when facing the caregiver experience. 31 A qualitative study of caregivers to persons living with dementia revealed participants describe their gamut of feelings using the terms emotional, exhausted, and on edge. 32 Juggling additional responsibilities such as parenting children and maintaining employment was reported by participants. As the population ages, there is a growing number of individuals who find themselves providing care to older adults while satisfying their other commitments such as employment and childcare. 33 Caregivers who hold the responsibility of childcare and caregiving to older adults have been referred to as being “sandwiched” 34 or part of the “sandwich generation.” 35
Saskatchewan’s healthcare system was regarded as fragmented by participants in this study, as caregivers lamented at the lack of consistency in accessing and receiving healthcare services in the province. Caregivers frequently function as care coordinators to advocate for their care recipients, as they attempt to navigate the complexities of the healthcare system without assistance from professionals. 36 Furthermore, rural Saskatchewan residents face challenges with accessing the healthcare system from a distance. Rural participants reported the lack of allied health professionals in their areas as a challenge to receiving coordinated care. The involvement of allied health professionals in care teams, such as dietitians, occupational therapists, and physical therapists, has been found to reduce appointment burden for both patients and caregivers and provide a more seamless care experience36 -39 but these professionals can often only be accessed during a hospital admission. For care recipients being discharged from the hospital setting, better communication between hospital providers, homecare providers, and caregivers is needed to improve care coordination and facilitate healthy recovery at home. 40 Navigating the complexities of the healthcare system is complicated further when both the caregiver and care recipient are living with chronic conditions. Many older Canadians are increasingly relied upon to take on caregiving, even though they may experience health issues of their own. 15
The complexities of governmental systems also create challenges for caregivers. Participants in this study noted that Saskatchewan’s current systems are not oriented to older adults aging in place. Limited and lack of funding and resources leads to uncertainty in the accessibility of care, when government cuts decrease program availability. 39 Overly restrictive eligibility criteria, convoluted and repetitive application processes, and other gatekeeping mechanisms are a few layers of red tape caregivers must cut through to access government support. 41 While there is increasing recognition within government policies of the contribution of caregivers, financial support often comes with a trade-off such as restrictions on employment, which limits opportunities for managing financial burden. 42 For support in providing care at home, the most basic form of financial support Canadian caregivers can receive is a federal tax credit, yet only a small minority qualify 43 and government portals for tax information are also difficult to navigate. 44 Moreover, caregivers have reported difficulties in making sense of eligibility requirements and maneuvering application systems while juggling the demands of their role. 42
Caregiving at a distance was narratively found to be a component of many of the participants’ caregiver experience in this study. Geographical proximity is an important structural factor that determines the extent of a caregiving exchange. 45 It is common for adult children to move away, leaving parents with an “empty nest,” which is especially true for those living in rural areas. 46 With younger generations leaving rural areas, usually in search of work, older generations who are often of lower income are left behind. 47
Caregivers need to feel as though they are doing the right thing with their care labor to achieve personal well-being and satisfaction in their role. 48 In many cases, caregivers express being unprepared for the impact of their caregiving role.36,49 To mitigate this unpreparedness along the trajectory of an illness such as dementia, caregivers have reported that they must be psychologically primed for what is to come to be able to effectively cope. 48 The accruement of knowledge helps caregivers advance in their role and allows them to both prevent and cope with difficult situations. 50 In a study of caregivers to older adults with heart failure, many caregivers described a lack of confidence in monitoring signs and symptoms, since healthcare professionals did not provide them with this critical knowledge. 49 The participants in this study described similar experiences, which was referred to as “going it alone.” A participant in the study by Durante et al 49 stated: “Nobody gave suggestions to us, so I had to develop strategies that helped me to keep my husband’s situation under control, but I don’t know if what I do is correct” (p. E31). Taking into consideration the weight that rests on the shoulders of caregivers in terms of responsibilities, receiving reassurance and validation in their caregiving abilities from social networks and healthcare professionals directly relates to enhanced confidence, competence, and strength in the caregiving role. 51
Health literacy, defined as the ability to obtain, understand, and use health information, is a crucial factor influencing the caregiving experience. 52 Caregivers with higher health literacy, especially in aspects such as question-asking, are found to experience lower levels of anxiety and a higher quality of life. 53 This notion underscores the importance of supporting caregivers in developing health literacy skills, as it directly impacts their emotional and psychological well-being. The findings of the Saskatchewan Caregiver Experience Study can be better contextualized by considering the health literacy levels of caregivers. Analyzing our findings through the lens of health literacy could provide deeper insights into the specific needs and barriers encountered by caregivers in managing health information and decision-making. Future secondary analyses of our expansive data set of 355 caregiver responses will include an analysis of responses that highlight the importance of health literacy in caregivers. The interaction between caregivers and the healthcare system is significantly influenced by the caregivers’ health literacy. Reduced health literacy can create obstacles in navigating the complex healthcare environment, affecting the caregivers’ ability to advocate for and provide effective care, which is particularly true in culturally diverse contexts, where the complexity is magnified by linguistic and cultural barriers. 54 Therefore, it is essential to develop resources and interventions that are accessible and tailored to the varied literacy levels of caregivers, facilitating better communication and navigation within the healthcare system. Addressing health literacy challenges among caregivers through tailored interventions is critical. Such interventions should focus on improving communication skills and providing caregivers with the necessary knowledge and resources to manage the health of their care recipients effectively. Enhancing health literacy among caregivers not only improves their own well-being but also positively impacts the health outcomes of the care recipients. 53 Ideal interventions specifically address the unique challenges faced by caregivers in understanding and navigating the healthcare system. 53
Global Context
The findings from the Saskatchewan Caregiver Experience Study carry significant implications that transcend provincial and national boundaries, shedding light on the universal aspects of the caregiving experience. As illuminated in the study, the challenges faced by Saskatchewan caregivers, such as the categories identified in this manuscript, are echoed in global contexts, resonating with caregivers’ experiences worldwide. For instance, Montenegro and Ortega 55 emphasize the need for global mental health interventions to be contextualized and culturally adapted, which aligns with the need for locally sensitive support systems for caregivers. Similarly, Szlamka et al. 56 highlight the importance of considering socio-economic contexts, including poverty, which can significantly impact caregiver experiences and service access both in Saskatchewan and globally. These themes underscore the universality of caregiving experiences and the potential for Saskatchewan’s findings to inform and enhance caregiver support strategies internationally. When compared to global contexts, there are both similarities and differences in caregiving experiences. For example, in a study assessing Indigenous cancer supports in Saskatchewan, the complexity of the healthcare system and the need for culturally relevant healthcare provision were highlighted. 57 These challenges can be seen in other parts of the world, where cultural factors play a significant role in caregiving.
The shared global challenge of caregiving calls for a collaborative approach to knowledge and resource exchange, enabling caregivers everywhere to benefit from these insights. Internationally, caregiving in rural areas shares common challenges with the Saskatchewan context, such as the emotional toll of caregiving, the complexities of navigating healthcare systems, and the cultural expectations of caregiving roles, which often include a significant amount of unpaid labor and personal sacrifice. This issue is also prevalent in other rural areas globally, where distance and limited resources can impact the quality and availability of support for caregivers and care recipients.58,59 Research indicates that neurodegenerative diseases, for example, pose a significant challenge in rural areas, where families often experience isolation and limited access to professional support, highlighting the need for a specific portfolio of services tailored to such regions. 60 Similarly, the experience of family caregivers during the COVID-19 pandemic has underscored the importance of telemedicine and other remote healthcare interventions, which have the potential to improve access to care and reduce the workload for caregivers, particularly in rural settings where traditional services may be sparse or difficult to access.61,62 While there are unique aspects to caregiving in Saskatchewan, such as the challenges faced in rural areas and the influence of cultural and societal factors, many of these experiences are echoed in global contexts. This suggests that insights gained from the Saskatchewan caregiving context can be valuable in understanding and improving caregiving experiences worldwide.
Study Implications
The findings of the Saskatchewan Caregiver Experience Study provide insights that can directly inform both scholarship and practical applications in home healthcare management and practice. These insights emphasize the necessity for targeted interventions to support family and friend caregivers, which has several implications for healthcare policies and practices, particularly in home healthcare contexts. The study highlights the urgent need for policies that facilitate better support systems for caregivers. For example, developing guidelines that ease caregivers’ access to respite care and mental health services can help mitigate the exhaustion and emotional strain that caregivers frequently face. Policies aimed at integrating caregiver assessments into routine care plans could ensure that caregivers’ needs are systematically identified and addressed. The challenges identified by caregivers, such as the high cost of home care and the scarcity of services, especially in rural areas, call for a re-evaluation of how home care is structured.
Enhancing the availability and affordability of home care services can significantly aid caregivers, potentially reducing their burden and improving the quality of care provided to older adults. As identified through this study and previous literature, caregivers often feel unprepared for their roles. Providing training and educational resources as part of home healthcare services can empower caregivers with the skills and knowledge necessary to manage their duties more effectively and with greater confidence. Encouraging the use of technology in home healthcare can also play a pivotal role. For instance, telehealth services can provide caregivers with easier access to healthcare professionals and support groups, which is particularly valuable for those living in remote or rural areas. Creating and maintaining robust support networks for caregivers through community health programs and online platforms can foster a sense of community and shared experience, reducing feelings of isolation and stress.
Limitations
The Saskatchewan Caregiver Experience Study provides valuable insights into the challenges faced by caregivers in Saskatchewan. However, the study collected data solely through an online survey distributed via Facebook and community newsletters. This method may have introduced sampling bias as it relied on individuals to access and use these online platforms. Caregivers who do not use Facebook or have limited internet access may not be represented in the sample. As well, the study primarily relied on open-ended survey questions, which led to challenges in analyzing the breadth of qualitative data comprehensively. The quality of responses varied, and some responses were unclear or lacked depth. The variation in length of responses (1 to 843 words) also posed a limitation. Analyzing such diverse responses was challenging, and some valuable insights may have been buried within lengthy or verbose responses. Future research could address some of these limitations to provide a more comprehensive understanding of caregiver experiences.
Conclusion
The purpose of the Saskatchewan Caregiver Experience Study was to highlight the experiences of caregivers to older adults in the Canadian province of Saskatchewan. Future research should seek to understand how caregiver experiences evolve over time and how different types of support impact their well-being. Comparing caregiver experiences across different regions could reveal regional-specific needs and inform targeted interventions. Additionally, examining the influence of factors like gender, ethnicity, and socio-economic status on caregiving experiences can offer insights into the challenges faced by diverse caregiver groups. We have presented the five main categories of the challenges identified by caregiver participants in this manuscript. It is important to explore and document the challenges experienced by this population to be able to work toward improving the lives of caregivers and the older adults they provide care to. An understanding of the challenges caregivers experience can also provide direction to researchers, clinicians, and policymakers for the development of future services and interventions to mitigate the negative aspects of caregiving, and to facilitate caregivers in their caring role.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223241254084 – Supplemental material for Challenges Reported by Family and Friend Caregivers to Older Adults in the Saskatchewan Caregiver Experience Study
Supplemental material, sj-docx-1-hhc-10.1177_10848223241254084 for Challenges Reported by Family and Friend Caregivers to Older Adults in the Saskatchewan Caregiver Experience Study by Steven Hall, Noelle Rohatinsky, Lorraine Holtslander and Shelley Peacock in Home Health Care Management & Practice
Footnotes
Acknowledgements
We would like to thank the Saskatoon Council on Aging and their Caregiver Committee for their support in the development and launch of the Saskatchewan Caregiver Experience Study. As well, thank you to the caregivers of Saskatchewan for their interest and participation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was received from the Saskatoon Council on Aging, a not-for-profit organization in Saskatchewan that provides support to older adults and their caregivers.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.