
Abstract
Translational research moves scientific discoveries and innovations across the development spectrum for a particular target or disease, trying to bridge in a multidisciplinary fashion the gap between laboratory scientific discoveries and practical, real-world applications in medicine and in healthcare. Translational research aims to move research findings across settings, specific languages, methodologies, and study designs, from laboratory to clinical practice and ultimately into community- and population-level health benefits. In contrast, translational science is a distinct field, which evolved over time toward a systematic study and practice of operationalizing the translation of content from one language, ecosystem, environment, contextual landscape, culture, discipline, area, or domain into another. It involves systematic and transdisciplinary integration of knowledge from basic science, clinical research and population science to improve human health, better longevity, and to ensure disease- and disability-free lives. Translational science often uses knowledge, operational frameworks, and specific capabilities borrowed from other specialties, disciplines, and fields such as operations management, implementation and dissemination science, quality improvement and management, project management, public health, intervention science, change management and leadership, decision science, design thinking, functional design, data science, communication and marketing science, etc. The main goal of this article is to open a series of thematic reviews in this journal, introducing the reader to the main definitions, contingencies, touchpoints, and overlapping areas between translational science and these related specialties, disciplines, and fields of study. Transdisciplinary capabilities borrowing from these related specialties can create a robust translational science machinery for health systems, research organizations, and innovation hubs.
Keywords
Introduction
Societal investment in biomedical research is accomplished via government’s commitment to improve the health of its individuals, communities, and population at large, to ameliorate and cure diseases through research discovery and innovation. Despite significant resources allocated for biomedical research over the past 50 years, advancing new knowledge into clinical practice has been slow. Interestingly, almost 12 decades ago (in 1905), Robert Koch was delivering his Nobel Prize lecture, entitled The Current State of the Struggle Against Tuberculosis. 1 In his presentation, Robert Koch complained about the slow pace of medical research advancing to clinical care and mentioned that the etiology of tuberculosis “shared the fate of so many similar cases in medicine, where a long time has also been necessary before old prejudices were overcome and the new facts were acknowledged to be correct by physicians.” 1
In the United States, policies and specific roadmaps for advancing translational research (TR) and comparative effectiveness research have been published by the National Institutes of Health (NIH) 2 and the Institute of Medicine. 3 In addition, the Agency for Healthcare Research and Quality (AHRQ) outlined over the years healthcare research priorities. 4 In 2011, the NIH established the National Center for Advancing Translational Sciences (NCATS), with the specific charge to pursue, encourage, catalyze, and grow funding opportunities for disruptive translational innovation. 5 The NCATS is currently the funding agency for the Clinical and Translational Science Award (CTSA) hubs. In the emerging iteration of the NCATS strategic plan, one of its aims is to accelerate translation by addressing both scientific and operational barriers, recognizing that innovation, creativity, and technology can aid and accelerate translational science (TS) and TR efforts, including identification of new opportunities to pursue effective and efficient translations, through teamwork and transdisciplinary collaboration. 6
TS, the main topic of this overarching review, is an eclectic discipline that assesses research study and system processes in order to establish their scientific governing principles and inner-workings, moving translation from empiricism to predictivity. 7 It has been asserted that moving an intervention or innovation in the well-described develop–demonstrate–disseminate cycle to public health (PH) requires no less than 20 distinct scientific disciplines, each with its own language, heuristics, frameworks, and specific outcomes. 7 We contend here that some specific competencies, capabilities, tools, and frameworks borrowed from different disciplines can help achieve the TS principles, as described by NCATS. 6 We hope that this high-level overview of the science of translation and the contiguous specialties and fields of study (Table 1) will help the reader acquire the necessary awareness of distinct concepts, tools, and frameworks, in order to create a more complete, effective, efficacious, and informative Team Science approach.
Overview of the main disciplines presenting useful frameworks, capabilities, and approaches for the field of Translational Science.

What is translation?
The initial term translation referred to the art of rendering text, symbols, and spoken words from one language to another, accurately and effectively, and was associated with the work of translators and interpreters who bridged language barriers in literature, law, diplomacy, business, etc. Translation encompasses not only linguistic aspects, but often cultural, social, contextual, and artistic considerations. In ancient medical texts, the term translation referred to the efforts made by wizards, healers, and early doctors to codify (hence the philological connotation) chemicals and procedures used in treatments, that is, linked to the immediate needs of patients, not to the scientific or theoretical underpinning of these interventions. Over time, the practical focus of translation was strengthened by both small and large pharma, which evolved progressively out of alchemy laboratories, community apothecaries, and chemical companies. For them, product commercialization was and remains centered on specific offerings that sell easily in the marketplace, while understanding the pathophysiology behind the scientific innovation is often secondary and sometimes ignored altogether. In the latter part of the 20th century, efforts geared toward translation were applied mainly to the fields of PH and clinical medicine, and occasionally trickled down to identification of some therapeutic and preventative interventions, but seldom to the development of new drugs. Along the translational spectrum, dissemination and adoption of new discoveries have been marred by structural or functional challenges, barriers, system strictures, bottlenecks, funding winters, death valleys, or long unexplained delays. While progress in both basic and translational research remained tightly intertwined with clinical observations, the explosive successes in fundamental laboratory research seen so far in the 21st century far outpaced clinical and translational investigation outputs. This exponential growth in fundamental discoveries led to tremendous progress in our understanding of etio-pathophysiology while generating large amounts of information (big data, deep data, long data, etc.) hence the need for data science (DaS) integration in the processes of translation, and the use of the latest mathematical advances, powerful computational capabilities, and methods such as artificial intelligence (AI), machine learning (ML), deep learning (DL), etc.
What is translational research?
TR is defined by the NCATS as the endeavor to traverse a particular step of the translational development spectrum for a particular target of disease. The goal of TR is to bridge the gap between scientific discoveries and practical, real-world applications in medicine and healthcare. 8 TR is a multidisciplinary approach that encompasses several transition stages (T0–T5) that involve moving research findings across settings (forward and backward), specific languages, methodologies, and study designs, or from laboratory to clinical practice and eventually into community- and population-level health benefits. It aims to accelerate the translation of scientific knowledge into tangible solutions and improvements in healthcare. TR is often used to develop novel medical devices, new therapeutic approaches, strategies, or healthcare interventions based on initial, often laboratory-driven scientific discoveries. TR involves collaboration among scientists, clinicians, patients, community members, government officials, and other stakeholders (team science) to ensure that research findings are effectively translated into clinical practice and PH policy.
What is translational science?
TS and TR are distinct, but contiguous/overlapping concepts, as they share some similarities in their focus on the transfer of knowledge from one context to another. TR refers to the field of study and practice aimed at bridging the gap between scientific discoveries and innovations and their practical applications in medicine. In contrast, TS evolved over time toward a systematic study and practice of operationalizing the translation of content from one language, ecosystem, environment, contextual landscape, culture, discipline, area, or domain into another. It involves systematic and multidisciplinary integration of knowledge from basic science, clinical research, and population science to improve human health, better longevity, and to ensure disease- and disability-free lives. By emphasizing the practical application of scientific knowledge, TS aims to accelerate the pace at which discoveries are translated into tangible benefits for (more) individuals and communities. TS plays a crucial role in advancing medical treatments, interventions, and healthcare practices, ultimately contributing to improvements in PH. Beyond linguistic and cultural considerations, TS deals directly with distinct methodologies, technologies, and processes. Over time, TS has expanded its scope by becoming the art and science of rendering text, symbols, data or specific content from one domain to another, systematically, accurately, synergistically, effectively, and, more importantly, the science of operational processes and methodologies geared toward finding best solutions or strategies to overcome in a sustained fashion the inherent barriers or translational blocks between different phases of investigation.
TS encourages transdisciplinary collaborations across basic science, clinical research, epidemiology and PH, biomedical informatics, DaS, and healthcare delivery. We contend here that a successful TS machinery at a CTSA hub should include additional capabilities, which borrow from very distinct, often non-adjacent fields such as Implementation Science (IS), Quality Improvement (QI), Quality Management (QM), Communication Science (CS), Marketing Science (MS), Systems Engineering (SE), Human Factors Engineering (HFE), Industrial Psychology (IP), Intervention Science (IntS), DaS, Decision Science (DS), PH, Project Management, Change Management (CM), Change Leadership (CL), etc (Table 1, Figure 1). Developing and functional use of such capabilities and competencies may serve the field of TS well, allowing team science approaches to accomplish faster adoption, more successfully and to more people overall. 9
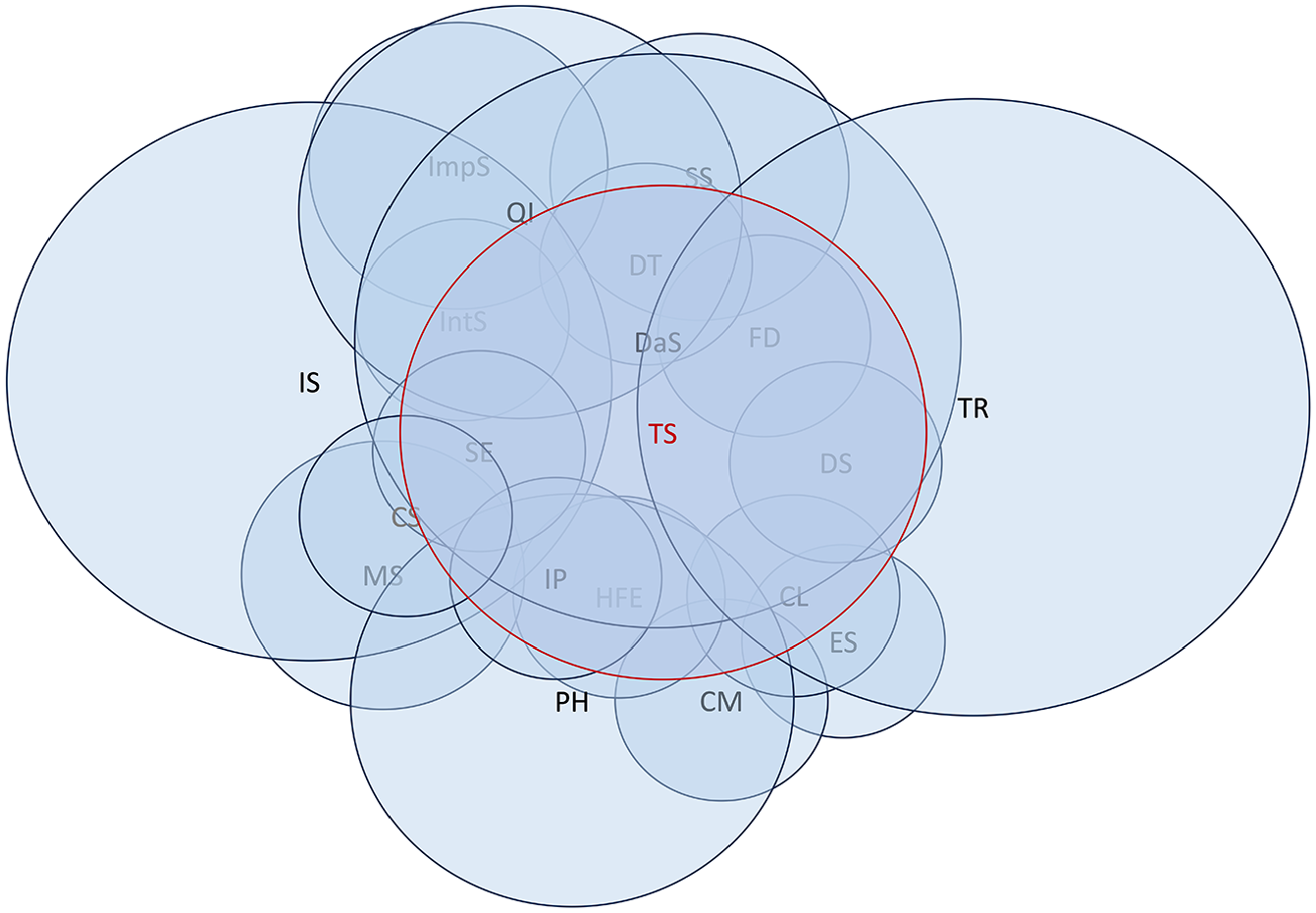
Venn diagram representation of the different overlapping disciplines with the field of TS.
The focus of TS is on the efficiency, effectiveness, and informativeness of the translation of findings from laboratory (“bench”) into practical applications for patient care (“bedside” or “clinic”), to communities and populations at large. However, TS often involves bidirectional processes and guided flows of information, that is, not only “bench to bedside,” but also “bedside to bench.” A patient-centered perspective is central to TS. Additionally, TS seeks to address health disparities by ensuring that scientific advancements benefit all diverse populations and that they are implemented equitably.
Major facilitators for TS are represented by: (1) adequate funding and resources; (2) streamlined regulatory processes and clear guidelines; (3) great stakeholder engagement, involving patients and communities to ensure research relevance and good adoption; and (4) existing, highly functional and collaborative Team Science networks, with strong partnerships between innovation incubators, industry partners, researchers, health system employees, and community members (e.g., in established learning health systems).
Traditional barriers for TS relate to (1) the high complexity of TR pathways, often convoluted, high-risk, costly, and time-consuming; (2) lack of local resources for implementing evidence-based practices (EBPs) and interventions (information, funding, staff, and time); (3) poor training and/or communication between stakeholders (clinicians, researchers, and administrators); (4) resistance to change or aversion to risk; (5) lack of organizational and/or leadership support; (6) regulatory hurdles; and (7) local cultural aspects. Addressing these enablers and barriers is crucial for the success of the local TS engine. At institutional level, a CTSA hub can serve as designer and owner of the translational channel of communication and the catalyst for enlarging the pool of stakeholders communicating and contributing by different sets of abilities, capabilities, and methodologies, in that channel and over specific time periods.
TS principles are not limited to medicine or healthcare and can be used in other fields, such as environmental science, engineering, and technology. Their central tenet is to ensure that scientific advancements do not remain confined to the laboratory or at the point of innovation, and are translated into practical solutions and real-life benefits that improve people’s lives.
What is implementation science?
IS, perhaps a subfield of TS, focuses on the study of methods and strategies to promote the systematic adoption and integration of EBPs or interventions into routine care. 10 Dissemination and implementation science (or simply IS) evolved from the early research endeavors in the field of diffusion of innovation, led by E.M. Rogers and several other research “traditions.” 11 Implementation is an effort specifically designed to get evidence-based or evidence-informed findings and related products into routine and sustained use through appropriate change, uptake, and adoption interventions. The term implementation is not used in the sense of ensuring fidelity of study procedures during a clinical trial, but how the intervention is applied. Dissemination is defined as an effort to communicate tailored information to target audiences, with the goal of engagement and information spreading. Dissemination is often considered an inherent part of the implementation. IS focuses on understanding and overcoming barriers and challenges that can prevent successful implementation of these interventions, for example, lack of resources, limited stakeholder engagement, inadequate training, lack of leadership support, etc.
Dissemination relates heavily on concepts and frameworks used by another field of study, that is, knowledge translation, which refers to the processes of taking new knowledge generated through research and making it accessible, understandable, and useful for broad audiences, especially for those who may ultimately benefit from the applied knowledge, for example, healthcare practitioners, policymakers, community members, and the public at large. It involves activities of synthesizing research findings, sharing them in formats (languages!) that meet the needs and understanding of different audiences, and facilitating the use of newly acquired knowledge in informing decisions, policies, and procedures or practices to improve the desired outcomes. Integrated knowledge translation is a model of research co-production where researchers partner with knowledge users who can use or implement the research recommendations or findings. 12 An integrated knowledge translation approach for research describes how innovators and researchers work closely with knowledge users (policymakers, healthcare professionals, and patients) throughout the research spectrum and processes, ensuring that the research is meaningfully impactful, that is, relevant, usable and with palpable consequences for the ultimate beneficiaries. The goal of this type of partnership is to make the knowledge more understandable, accessible, applicable, and impactful, and to empower knowledge brokers with the right tools for dissemination, while defining and preparing the right diffusion channels and dissemination strategies.
Importantly, IS employs a systematic approach to designing, testing, and refining implementation strategies, often through use of randomized controlled trials (RCTs) and other rigorous evaluation methods. The main IS attributes are represented by fidelity, sustainability, and adaptation.
Fidelity: It relates to the degree to which an intervention is implemented as intended or specified in the original research study or EBP. It includes the degree to which the core components of the intervention are delivered, the quality of the delivery, and the consistency of the intervention across different settings or populations. Fidelity ensures that the intervention produces the expected outcomes and enables replication and comparison of results across studies.
Sustainability: It relates to the long-term maintenance of an intervention or EBP after the initial implementation period. Factors that can influence sustainability are organizational culture, resource availability, stakeholder buy-in, ongoing support, and continuous monitoring. The sustainability ensures that the benefits of the intervention are maintained over time and maximizes the return on investment in implementation efforts.
Adaptation: It is the characteristic that relates to the modifications or adjustments made to an intervention or EBP to fit the needs of the target population or setting. The acceptable degree of adaptation depends on the goals of the intervention, the nature of the modifications, and the potential impact on the outcomes. Adaptation is necessary to increase acceptability, feasibility, and relevance of the intervention to the local context, but it can also pose a risk to fidelity and effectiveness of the intervention.
Various and rigorous research methodologies are used in IS: (1) RCTs that evaluate the efficacy and effectiveness of interventions and the impact of implementation strategies (which can establish causalities); (2) mixed-methods designs (useful for understanding the complexity of implementation and identifying contextual factors that influence the success of an intervention); (3) studies evaluating the implementation process itself, by identifying facilitators and barriers to implementation, measuring fidelity to the intervention, and to assess the quality of the implementation; (4) quasi-experimental designs, used when randomization is not feasible or not ethical; and (5) case studies, which involve detailed, in-depth analyses of a specific implementation effort and useful for understanding the context of implementation, the specific challenges encountered, the strategies employed to overcome them, and identifying best practices or lessons learned. In every IS project, the role of stakeholders cannot be overlooked, as they provide important roles, identifying needs and priorities that make the intervention relevant and tailored to the local context, finding and securing resources (human, financial, training, or material resources) to support the implementation, offering perspectives on feasibility, potential barriers, acceptability, and relevance of the intervention to the target population or setting, and providing support and advocacy for the implementation efforts. For example, one should not study or practice IS without engaging the beneficiaries of the specific activity, that is, patients, their families, and communities.
The traditional constructs of IS are represented by theories, frameworks, and models, terms that were unfortunately used interchangeably, leading to some terminological confusion. Theories present a systematic way of understanding events or behaviors by providing interrelated concepts, definitions, and propositions that explain or predict events by specifying relationships among variables; they are abstract, broadly applicable and are not content- or topic-specific. Frameworks, either strategic or action planning, are constructs that provide a systematic way to develop, manage, and evaluate interventions. Models are often conceptualized as a combination of both IS theories and frameworks.
Is there any overlap between IS and TS?
Yes, there is significant overlap between IS and the TS, particularly in biomedical research and healthcare. Both fields try to bridge the gap between research and practice, ensuring that evidence-based findings are effectively and efficiently integrated into real-world settings, with the ultimate goal to improve patient care and health outcomes. IS emphasizes the systematic study of strategies, approaches, and methods to facilitate the successful adoption and use of EBPs in healthcare settings. TS, while broader, includes a similar goal of moving research findings into practical applications. Both recognize the importance of engaging stakeholders, including healthcare practitioners, patients, policymakers, and community organizations, in the translation and implementation process. Both fields rely on evidence-informed or evidence-based approaches to guide decision-making. IS emphasizes the use of evidence to inform the selection of implementation strategies and the evaluation of their effectiveness. TS incorporates the use of evidence to inform the translation efforts. Both fields embrace the principles of QM, continuous improvement, iterative processes, and adaptation. Both IS and TS recognize the complex and multidisciplinary nature of the challenges addressed, fostering collaboration between researchers, clinicians, policymakers, patients, community members, and other stakeholders to navigate the complexities of healthcare systems and practices. Finally, both fields emphasize the importance of evaluating outcomes, that is, not only clinical effectiveness, but also the impact of various strategies on patient experiences, cost-effectiveness, and the broader health system.
While there is considerable overlap, these specialties may use different terminology (languages) and approaches. IS often focuses on the process of putting evidence into practice, while TS entails a broader spectrum of activities geared toward the translation of research findings across various domains or phases of investigation. Experts in both fields collaborate and draw from each other’s insights and methodologies to advance the adoption of EBPs, interventions, and innovations in healthcare and medicine (Table 3).
What is change management?
CM is a systematic approach to transitioning individuals, teams, and organizations from their current state to a desired, future state. It involves planning, execution, and reinforcing changes to achieve organizational goals and improve overall effectiveness. 13
CM needs to begin with a clear understanding of the necessity for change, identifying drivers of change, either internal (strategic goals and operational improvements) or external (market trends, technological advancements). Next, identifying and analyzing stakeholders is crucial to understand how change will impact different individuals or groups within the organization, their level of influence and interests, and anticipating possible reactions to the proposed change. Leaders should actively sponsor the change, demonstrate commitment, and provide the necessary resources and support to facilitate the transition. Developing detailed execution plans is critical, including specific milestones, timelines, responsibilities, monitoring progress, and making adjustments as needed. CM involves gathering feedback from employees and stakeholders to assess the effectiveness of the change process. Continuous evaluation allows organizations to identify areas for improvement and make adjustments, as necessary. Involving employees in the change process fosters a sense of ownership and commitment. This entails seeking input, involving employees in decision-making and providing opportunities for training and skill development. Resistance to change is a common challenge, especially in healthcare. CM involves identifying sources of resistance, addressing concerns, and creating a supportive environment where employees feel comfortable adapting to new workflows. Necessary training and development opportunities ensure that employees have the skills and knowledge required to succeed in the new environment. This includes technical training, leadership development, and sometimes change-specific workshops. Recognizing and celebrating both achievements and milestones along the way help build momentum, increase adoption, and reinforce the favorable aspects of change, contributing to a positive organizational culture around change.
E. Rogers’ diffusion of innovation theory had five distinct change phases: knowledge (education and communication), persuasion (change champions to stir staff’s interest; peers persuading peers), decision (staff decides whether to accept or reject change), implementation (putting new processes into practice), and confirmation (staff recognizes the value and benefits of the change and continue to use changed processes). 11
CM is applicable in various contexts, including organizational restructuring, process improvements, technology implementations, and cultural transformations. As organizations evolve, CM is a dynamic and iterative process that requires ongoing attention and adaptation. Successful CM contributes to organizational resilience, agility, and ability to navigate and thrive in a constantly changing macroenvironment.
What is change leadership?
CL refers to the ability of individuals or groups within an organization to guide and influence others toward successfully navigating and embracing change. Unlike CM, which often focuses on the processes and methodologies used to implement change, CL emphasizes the human and interpersonal aspects of leading people through a period of transition, sometimes without a clear endpoint.
TR change leaders are responsible for setting a compelling vision for the future, articulating why change is necessary, what the organization is working toward, and how the envisioned future will be better than the current state. A clear and inspiring vision helps aligning individuals and teams with the direction of change. Effective communication is the hallmark of CL, including rationale for change, progress made, and impact on individuals and organization. This includes listening to concerns and feedback, responding with empathy, inspiring and motivating, conveying a sense of urgency, fostering a positive attitude toward change, and encouraging a collective commitment to achieving the goals. 14 Effective communication and storytelling are often employed to connect emotionally with the team. Change leaders empower individuals and teams to contribute to the transformative effort, providing autonomy, recognizing and valuing contributions, and creating opportunities for individuals to take ownership of change. Change leaders promote interdisciplinary collaborations and inclusivity. They involve stakeholders in the decision-making process, seek input from diverse perspectives, and foster a sense of collective ownership through collaborative and supportive change networks. Leading by example is a fundamental aspect of CL. Leaders demonstrate the specific behaviors and attitudes expected, and their actions should align with the values and principles of the change initiative, reinforcing the credibility of the leadership team. Trust is a crucial element of CL, which could be built by being transparent, authentic, and consistent in communication. Trust is essential for overcoming resistance to change and creating an environment where individuals feel safe expressing concerns or uncertainties. Change leaders need to recognize the importance of continuous learning, encouraging a culture of curiosity and experimentation, where individuals and teams can learn from both successes and setbacks. This adaptability contributes to ongoing improvement and innovation. Change leaders have to be adaptable and flexible in the face of uncertainty and ambiguity, to remain resilient, adjust their approach as needed, and contribute to the overall success of the change initiative. CL is particularly relevant in dynamic and complex environments (e.g., in healthcare), where the ability to navigate uncertainty, build a positive organizational culture, and coalesce people with a shared vision are critical for success. 15
While the terms CM and CL are often used interchangeably, there are several important distinctions. CL often complements CM by addressing the human and cultural aspects of organizational transformation. CM focuses primarily on processes, structures, and methods employed to guide an organization through change initiatives. It involves systematic planning, execution, and control of the change, often with a focus on minimizing resistance, ensuring employee buy-in, and achieving the desired outcomes. CM tends to be more procedural and may involve tools, methodologies, or frameworks to facilitate a smooth transition. It often addresses the “how” of change, emphasizing the practical steps and actions needed for successful implementation (IS or TS!). CL emphasizes the human and cultural aspects of change, through setting a compelling vision for the future, inspiring and motivating employees, fostering, and creating a culture that supports and sustains change. CL is about the “why and what” of change, focusing on aligning people with the vision, building trust, and fostering a sense of urgency and commitment. It often involves strong communication, strategic thinking, and the ability to rally individuals and teams toward a common goal.
In summary, while CM deals with the reactive, tactical, and operational aspects of change, CL is more proactive, strategic vision-centered, and people-oriented. Effective change initiatives often require a combination of CM and CL, with careful monitoring of the procedural aspects of implementation, but also of the human factors that influence organizational culture and behavior. Organizations that successfully navigate change typically integrate these two perspectives to create a holistic and impactful approach to managing transformations.
Are there areas of intersection between CL, CM, TR, and TS?
These disciplines have a shared focus on facilitating effective organizational transformations, particularly in the fields where new scientific knowledge is translated into practice. Recognizing these intersections, organizations can integrate CL and CM principles into TS and TR initiatives, fostering a collaborative and adaptive environment that maximizes the impact of scientific advancements in practice (Table 1).
First, CL emphasizes the need of creating a compelling vision for the future, aligning people with a shared purpose, similar to TS. Similarly, TR involves translating scientific discoveries across the research continuum. CM ensures that goals and actions are aligned with the overarching vision, with the scientific advancements (TR aims) and organizational structure and function (TS goals) that ensure that the change process is purposeful. Second, CL relies on strong leadership to guide and inspire people through it. CM emphasizes the sponsorship and support of key leaders. In TS, effective leadership is essential for translating scientific findings into impactful applications. Effective communication is crucial in both CL and CM, involving transparent and persuasive messaging to engage stakeholders. TS requires clear communication to bridge the gap between scientific research and practical application. The intersection occurs in crafting communication strategies that convey the value of translational efforts, engage stakeholders, and address concerns during change. CL emphasizes empowering individuals (change agency) and fostering inclusivity. CM/TS involves engaging diverse stakeholders in the change process. In TS, collaboration and inclusivity are essential for successful translation. CM involves tracking metrics to assess the success of change initiatives. Similarly, TS relies on evaluation metrics to measure the impact of scientific discoveries. The intersection involves developing aligned metrics that assess the success of both change efforts and the translational process. Both CM and CL recognize the importance of cultural aspects in driving successful transformations. In TS, there is often a need to foster a culture of collaboration and innovation. The intersection lies in promoting a culture that supports both the translation of scientific knowledge and the adoption of new practices or technologies in an organization. As institutions evolve, CL and CM emphasize adaptability and continuous learning. TR and TS also involve adapting to new knowledge and learning from research outcomes. Cultivating a shared commitment to adaptability and learning across change efforts and TS initiatives is essential. Both TS and change initiatives may involve ethical considerations. The key is to ensure that ethical principles are integrated into CL practices and CM strategies, especially when translating scientific knowledge into practical applications.
What is decision science?
DS uses a collection of quantitative techniques to inform decision-making at individual, community, or population level. It includes decision analysis, risk analysis, cost-benefit and cost-effectiveness analysis, constraint optimization or programming, simulation modeling, and behavioral decision theory. DS borrows concepts from operations research, microeconomics, statistical inference, management control, cognitive and social psychology, and DaS. By focusing on decision as the unit of analysis, DS provides a unique lens for understanding PH problems and for improving policies to address those issues. While most fields of research focus on producing new knowledge, DS is uniquely concerned with making optimal choices based on available information. DS seeks to make plain the scientific issues and value judgments underlying these decisions, and to identify tradeoffs that might accompany any particular action or inaction. 16 DS utilizes a variety of tools, including models of decision-making under conditions of uncertainty, experimental and descriptive studies of decision-making behavior, economic analysis of competitive and strategic decisions, approaches for facilitating decision-making by groups, and mathematical modeling techniques.
DS has been used in business and management, law, education, environmental regulation, military governance, PH, and policy. 17 Several DS analytic methods help inform policies and practices that improve population health by systematically integrating scientific evidence, with explicit consideration of individual and societal values for outcomes such as mortality, disease-specific, or general quality of life and healthcare costs.
What is design thinking?
Design thinking (DT) is a problem-solving and innovation methodology that places a strong emphasis on understanding and empathizing with the needs and perspectives of end-users or customers. It was popularized in the early 2000s but has its roots in earlier design and innovation practices. 18 There are several key components and sequential steps in DT: empathize, synthesize, ideate, prototype, test, implement, and iterate (Table 2). DT can be applied to the design of physical products, services, processes, systems, and organizational strategies and for operationalizing TR. Its human-centric approach to problem-solving fosters creativity, collaboration, and a deep understanding of the end-user’s perspective. One potential advantage for its use in TS is related to its aim to create innovative solutions that are not just functional, but also meaningful and helpful for end-users, resulting in better products and services. The DT end-users can be researchers, practitioners, patients, or community members. The use of DT should lead to new translation models that are value-adding, thus spurring participation of human subjects in clinical studies and in TR projects. Table 2 shows a few examples of how DT can be applied in medicine. For example, a successful project conducted at Medical College of Wisconsin and University of Wisconsin in Milwaukee led to the development of a mobile women health screening unit, which used DT methodology and wide, participatory stakeholder involvement, which ultimately led to the development and iteration of an improved prototype to serve the needs of underserved women in our communities by using a mobile screening and examination unit (currently in production).
Main components of Design Thinking (DT).

What is functional design?
Functional design (FD) uses a design approach that focuses primarily on the function and the performance of a product, system, or object. This is often contrasted with esthetic or form-based design, which emphasizes the visual or esthetic characteristics. In FD, the primary goal is to create a product or system that efficiently and effectively serves its intended purpose or function. FD is centered around the intended purpose or function of the product, beginning with a clear understanding of what the product needs to do and how it should perform. 19 User needs and requirements are also at the forefront of FD, reason why designers aim to create products that meet the needs of users and provide a positive user experience. Efficiency is a key principle of FD, as it aims to minimize waste, reduce unnecessary complexity, and optimize the use of resources such as materials, energy, or time. FD often involves solving specific problems or challenges. Designers may need to address technical constraints, environmental considerations, safety requirements, and other factors to ensure the product’s functionality and specific customization. FD prioritizes performance and functionality over esthetics, focusing on the facilitation of effective operation of the product or system. FD also emphasizes simplicity and clarity, as unnecessary complexity can hinder the functionality and use of a product. User interfaces and interactions should be designed with usability in mind. FD considers not only the practical aspects of a product's use, but also regular maintenance and repairs, with real-world considerations in mind. FD is often employed in medicine, product design, industrial design, engineering, architecture, or software development.20,21 FD sometimes ensures that the designed product or system is both visually appealing and functional, that is, effectively performs the required tasks while minimizing inefficiencies and unnecessary features. For example, in one endeavor of designing and building a new clinic that could serve the care, the research, and the educational needs of the patients and of the involved healthcare workforce, the final architectural plans created using FD frameworks may vary widely from the standard clinical layouts.
Is there any overlap between IS and DT?
Yes, there is significant overlap between IS and DT, particularly in their shared goals of improving adoption and diffusion of innovations and EBPs in various fields. First, both DT and IS emphasize a user-centered approach. DT places a strong emphasis on understanding the needs and perspectives of end-users, while IS is concerned with tailoring interventions and strategies to meet the needs of specific target populations. Both recognize that successful implementation requires a deep understanding of end-users’ context and preferences. Second, both DT and IS are iterative and problem-solving-oriented approaches. DT encourages iterative prototyping and solution testing. Similarly, IS involves ongoing assessment and adaptation of implementation strategies to address barriers and facilitators. DT and IS recognize the importance of engaging stakeholders throughout the process, either in the co-creation of solutions (DT), or in planning, execution, and evaluation of implementation and dissemination efforts (IS). DT is a human-centered design approach, while IS aligns with human-centered principles for implementation and dissemination. Both approaches prioritize the human experience and seek to optimize it through their specific methodologies.
DT encourages creative problem-solving and innovative solutions. While IS may not explicitly emphasize creativity in the same way, it shares a focus on innovative approaches to overcome barriers and promote the uptake of EBPs. Both recognize the importance of adapting solutions and strategies to the specific context. DT’s emphasis on empathy and context is similar to IS considering contextual factors that influence implementation success. Finally, both approaches prioritize collection and analysis of data to inform decision-making: DT relies on user feedback to refine solutions, while IS uses evaluation data to assess the effectiveness of implementation and dissemination efforts and make necessary adjustments.
While there is significant overlap, DT is a broad problem-solving and innovation methodology that can be applied to a wide range of domains, including in IS. DT principles, such as empathy, ideation, prototyping, and testing, can be integrated into IS models to facilitate development and adaptation of implementation and dissemination strategies. In practice, experts may draw from both DT and IS methodologies to create more effective and user-friendly approaches to implementing and disseminating innovations and EBPs.
What is systems engineering?
SE is a field of engineering that focuses on designing and managing complex systems over their life cycles, in a multidisciplinary and holistic fashion. A system is a collection of interacting components or elements that work together to achieve a specific goal. SE takes a holistic view (systems thinking) of a project or problem, considering the entire system and its interactions rather than focusing on individual components in isolation. This approach helps ensure that the system functions cohesively and efficiently.22,23
SE often involves collaboration between different engineering disciplines, such as electrical, mechanical, software engineering, etc. SE considers the entire life cycle of a system, from conception and design to implementation, operation, and decommissioning. Defining and managing requirements is a critical aspect of SE. This involves understanding and documenting the needs and expectations of stakeholders to guide the design and development process. Systems engineers identify and manage risks associated with the development and operation of a system, assessing potential challenges, uncertainties, and external factors that could impact the system’s success. SE often uses modeling and simulation tools to represent and analyze the system behaviors before they are physically built. This helps in identifying potential issues, optimizing design, and predicting system performance. SE involves making difficult trade-offs to balance conflicting requirements or objectives. This may include inputs related to cost, performance, reliability, etc. Configuration management is the process of managing and controlling changes to the components and documentation of a system throughout its life cycle. This ensures consistency and traceability. Systems engineers also oversee the integration of individual components into the overall system and conduct testing to validate that the system meets its requirements. Testing may involve functional, performance, and reliability assessments. SE aims to optimize the overall performance of a system through optimizing resource allocation, improving efficiency, and enhancing the ability of the system to adapt to changing conditions.
Systems engineers act as integrators or coordinators of complex projects, ensuring that all the parts of the system work together seamlessly to achieve the desired outcomes. SE plays a crucial role in creating and managing complex systems that are effective, reliable, and sustainable. SE is used in a wide range of industries, including defense, aerospace, transportation, healthcare,24,25 energy, and information technology. It provides a structured and systematic approach to designing and managing complex systems, ensuring that they meet the needs of stakeholders and operate effectively and reliably in real-world environments.
What is human factors engineering?
HFE (human factors science or science of ergonomics) is a multidisciplinary field that focuses on designing products, systems, and environments to optimize their compatibility with the capabilities, limitations, and needs of human users. 26 Its goal is to enhance overall system performance, safety, usability, and user satisfaction by considering human factors in the design process. HFE places a strong emphasis on a user-centered design approach. It involves understanding the characteristics, human capabilities, limitations, and preferences of the users who interact with the product, system, or environment (or the so-called sociotechnical approaches). HFE uses sometimes anthropometric data to design products and spaces that accommodate a diverse range of body sizes and shapes. Cognitive ergonomics focuses on mental processes such as perception, memory, attention, and decision-making. Design considerations include minimizing cognitive workload, improving information processing, and reducing the risk of errors. Physical ergonomics addresses the relationship between humans and the physical aspects of their environment, including tools, workspaces, and equipment. It aims to prevent musculoskeletal disorders and optimize comfort and efficiency.
HFE plays a crucial role in ensuring usability, improved productivity, and a positive user experience. Designers consider factors such as ease of use, information display, cost, learnability, efficiency, and user satisfaction. Designing effective human–machine interfaces is also a key aspect of HFE. This includes the design of user interfaces for software, control panels, and other interactive systems. HFE also considers the impact of the physical environment on human performance and well-being. This can include factors such as lighting, noise, temperature, and overall workplace design. In addition, HFE aims to reduce the risk of human error and enhance safety in various contexts, from transportation systems to medical devices. This involves designing interfaces and systems that are “forgiving” and easy to use. Designing workspaces that promote comfort, productivity, and well-being is a key application of HFE. This includes considerations of furniture, layout, and the overall organization of the workspace. Task analysis involves breaking down complex tasks into smaller, manageable elements to understand the steps involved and identify opportunities for improvement in efficiencies and user experience.
HFE is applied in various industries, including healthcare,27–29 aviation, automotive, information technology, manufacturing, and consumer product design. By considering the capabilities and limitations of human users from the early stages of design, human factors engineers contribute to the creation of products and systems that are safer, more efficient, and more user-friendly.
Is there any overlap between TS and HFE or SE?
Yes, there is significant overlap between them, especially when addressing complex healthcare problems. Both TS and SE share a holistic approach to problem-solving. TS seeks to bridge the gap between scientific research and practical applications in healthcare, while SE takes a comprehensive view of designing and managing complex systems. TS often involves collaborations between researchers, clinicians, and other stakeholders. Similarly, SE and HFE emphasize interdisciplinary collaboration, bringing together experts from different fields to address complex problems, which is crucial for understanding and solving multifaceted issues. HFE focuses on designing systems, products, or environments that are optimized for human use. This aligns with the user-centered design principles in both TS and SE, where the needs and experiences of end-users are essential considerations. SE and TS involve rigorous requirements analysis and stakeholder engagement. TS requires understanding the needs of patients and healthcare practitioners; SE involves eliciting and managing requirements from various stakeholders to guide the design and development of complex systems. SE and TS share a lifecycle perspective. TS spans the lifecycle of research, from basic discoveries to practical applications, while SE considers the entire lifecycle of a system, from conception to decommissioning, facilitating long-term planning and optimization. Both fields involve optimization and trade-off analysis. Systems engineers aim to optimize the performance of a system, considering factors like cost, reliability, and performance. Translational scientists may also optimize interventions and treatments considering factors like efficacy, safety, and patient outcomes. Modeling and simulation are essential tools for both. In TS, models may represent biological processes, while systems engineers use models to simulate and analyze the behavior of complex systems before implementation. This helps in predicting outcomes and optimizing designs. Both fields involve risk management. Systems engineers identify and manage risks associated with the development and operation of a system, while translational scientists assess risks related to the translation of research findings into practical applications, including clinical interventions. The intersection of TS, SE, and HFE can lead to more effective and user-friendly solutions, especially in healthcare where the integration of research findings into clinical practice often involves complex systems and human interactions. The collaborative and integrative nature of these approaches is valuable for tackling the challenges of developing and implementing innovations in various domains. For example, in developing a new inhaler medication delivery system, TS can provide the foundation for the new medication itself, its absorption through the respiratory epithelium and/or delivering the microparticles uniformly into the tracheobronchial tree; HFE can ensure that the delivery device is easy to manipulate and safe for patients; SE would consider how the entire system (medication, device, and training for healthcare providers) integrates with existing workflows and ensures optimal patient care.
What is industrial (or organizational) psychology?
IP (organizational psychology) is a discipline that applies psychological principles and research methods to understand and solve problems related to human behavior in the workplace. IP focuses on improving organizational effectiveness, employee well-being, and overall functioning of work environments. Industrial psychologists develop and implement methods for selecting and evaluating employees, by designing and validating assessments for performance appraisal, training, and development programs, conducting interviews, and making recommendations for hiring and promotion decisions. Understanding factors that influence employee motivation and job satisfaction is a key focus. Industrial psychologists investigate how work-related variables such as compensation, job design, and leadership impact employee well-being and performance. They also study leadership styles, organizational structures, and management practices to improve leadership effectiveness and institutional performance. Industrial psychologists may provide training and consultation to leaders to build and refine their management skills. Industrial psychologists examine issues related to diversity, equity, and inclusion in the workplace, studying biases, designing interventions to promote diversity, and creating inclusive organizational cultures. Most importantly, IP practitioners analyze organizational culture and climate to understand how they influence employee attitudes and behaviors, recommending strategies to shape a positive and productive work environment, employee well-being, job satisfaction, and work–life balance. Some industrial psychologists specialize in HFE or ergonomics, focusing on the design of work environments, products, and systems geared toward optimizing human performance and minimizing risk of errors and accidents. Industrial psychologists work in diverse settings, such as private corporations, government agencies, consulting firms, and academic institutions. Their IP research and practice contribute to creating healthier, more productive and satisfying work environments.
What is safety science?
Safety science (SS) is an interdisciplinary field focused on understanding, preventing, and managing accidents, injuries, and other incidents that can harm people, property, and/or the environment. It combines concepts and principles from engineering, psychology, medicine, and management to create safer systems, workplaces, healthcare facilities, and communities. SS aims to identify hazards, assess risks, and implement effective measures to prevent accidents and safety events, while trying to mitigate their consequences, building and maintaining a culture of safety. Concepts and frameworks from SS, SE, and HFE are highly relevant in healthcare.26,30 SS applied to medicine focuses on improving patient safety, reducing medical errors, and designing health systems that enhance the overall safety and well-being of patients and practitioners alike. Some describe SS as including several distinct disciplines: occupational safety and health, SE, HFE, product, industrial and environmental safety, etc.
What is intervention science?
IntS is considered by some a larger framework for IS. IntS is an interdisciplinary field that focuses on development, evaluation, and dissemination of interventions designed to improve human well-being and prevent or address various health and social issues. IntS also emphasizes the use of EBPs, that is, interventions that have been rigorously tested and shown to be effective through scientific research. This evidence serves as a foundation for designing interventions that can produce positive outcomes. The interventions are often tailored to specific populations or groups facing particular challenges, for example, children, adolescents, adults, or specific communities dealing with issues such as substance abuse, mental health, obesity, or transmittable infectious diseases. IntS can entail either prevention, treatment, or supportive measures. Prevention interventions aim to prevent the onset of problems, therapeutic interventions focus on addressing existing issues and promoting recovery, while supportive interventions aim to provide ongoing support and assistance to individuals or groups facing specific challenges, for example, support groups for chronic illness patients.
Rigorous evaluation is a fundamental aspect of IntS. Researchers assess the effectiveness of interventions by measuring predefined outcomes, such as changes in behavior, health status, or community well-being. Successful interventions often involve collaboration with the communities and populations affected by the issues being addressed. Community engagement ensures that interventions are culturally sensitive, contextually relevant, and have a higher likelihood of being accepted and sustained. Interventions are often adapted and tailored to the specific needs and characteristics of the target population. This customization increases the relevance and effectiveness of the intervention in diverse settings. IntS may also involve efforts to inform and influence public policy to support the widespread adoption of EBPs. Advocacy for supportive policies helps create an environment conducive to the success of interventions. IntS generally considers the long-term impact of interventions on individuals, communities, and various systems. This involves assessing not only short-term outcomes, but also sustained positive changes over time.
Common areas of focus for IntS include mental health (substance use, health promotion), PH (transmittable disease outbreak, obesity prevention and management), education (school-based interventions, addressing behavioral issues such as bullying, burnout prevention), criminal justice, etc. Researchers and practitioners in IntS work collaboratively to develop interventions that are not only effective in controlled research settings but also practical, adaptive, and impactful in real-world conditions.
What is communication science?
CS is an academic discipline that explores the processes, functions, and effects of human communication. It involves the systematic study of verbal and nonverbal communication, interpersonal communication, mass communication, organizational or intercultural communication, and the impact of communication technologies. CS seeks to understand how communication occurs, the various channels through which it takes place, and the factors that influence encoding, transmission, and decoding of messages (translation!). The study of interpersonal communication focuses on how individuals interact one-to-one or in small groups. Topics include relationship development, conflict resolution, and the dynamics of face-to-face communication. Mass communication explores the creation, distribution, and reception of messages through media channels such as television, radio, newspapers, magazines, and the internet. This area also includes the study of media effects on individuals and society. Organizational communication examines communication within and between organizations. This includes studying communication structures, leadership communication, team dynamics, and the role of communication in organizational culture.
Media studies, a subset of CS, focuses on the critical analysis of media content, media industries and media effects. Health communication explores the communication processes related to healthcare, health promotion, and PH campaigns. Communication scientists employ a variety of research methods, including surveys, experiments, content analysis, and qualitative approaches, to systematically investigate communication phenomena and derive meaningful insights. The development and application of communication theories are fundamental to CS. Theories provide frameworks for understanding and explaining communication processes and effects.
CS is a dynamic and evolving field that intersects with other disciplines such as psychology, sociology, anthropology, and media studies. Scholars and researchers in CS contribute to our understanding of human communication and its role in shaping individual behavior, societal structures, and cultural dynamics. The field has practical applications in areas such as journalism, public relations, advertising, education, and healthcare. 11
What is marketing science?
MS is a comprehensive, multifaceted business function that involves creation, communication, delivery, and exchange of products or services that have value for customers, clients, partners, or other constituents. Marketing processes include identifying customer needs and wants, developing products or services to meet those needs, and employing various strategies to promote and sell those offerings. MS begins with a deep understanding of the customer needs, preferences, and behaviors, by gathering information about target audiences, competitors, and industry trends. Once customer needs are identified, marketers collaborate with product development teams to create offerings that meet those needs. This includes designing products, determining features and setting prices. MS is centered around creating value for customers. Marketers develop compelling value propositions that communicate the unique benefits and advantages of their products or services compared to competitors. Marketers often divide the market into segments based on demographics, psychographics, behavior, or other factors (segmentation). Afterward, they target specific segments with tailored marketing strategies to maximize relevance and effectiveness. Promotion involves communicating the value of products or services to target audiences and includes advertising, public relations, social media messaging, etc., via specific communication channels. The goal is to create awareness, interest, and desire among potential customers.
MS also involves decisions about appropriate distribution channels, managing relationships with intermediaries and optimizing the supply chain. Pricing is a critical element in marketing strategy. Customer relationship management is also part of marketing and focuses on building and maintaining long-term relationships with customers through personalized interactions and customer support, sometimes maximizing customer lifetime value for the company. MS often employs rigorous methods and scientific experiments to solve marketing problems through mathematical modeling, simulation, and optimization. Marketers continuously analyze market trends, monitor competitors, and evaluate the performance of marketing strategies. This information is used to adapt and refine marketing efforts to stay competitive and meet changing customer needs. Marketing decisions and actions should be guided by ethical considerations and social responsibility. This includes transparent communication, fair pricing, and addressing environmental or societal concerns. In the modern era, digital marketing plays a major role. This includes online advertising, social media marketing, search engine optimization, email marketing, and other digital channels to reach and engage with audiences.
Effective MS is crucial for the success of businesses and organizations, as it helps create awareness, generate demand, build brand loyalty, and drive revenue. Further, MS has additional benefits such as improved decision-making, increased efficiency, and improved customer satisfaction. One key marketing concept in the exercise of TS projects is the lifetime customer value, in which the benefits of the offerings are judged over longer time periods, and not on a single transactional basis.
What is public health?
PH is a multidisciplinary field focused on promoting and protecting the health and well-being of populations. It involves efforts to prevent disease and prolong and improve quality of life for individuals and communities. PH encompasses a wide range of activities, from disease prevention or health promotion (T3–T4), to health system management and development of policies that contribute to well-being of entire populations (T5). Some examples of efforts in the realm of disease prevention are represented by vaccinations, health education, and promotion of healthy behaviors to reduce the risk of illness. PH also addresses the impact of environmental factors on health. This includes efforts to ensure clean air and water, manage waste, control environmental hazards, and to promote a safe, healthy living environment.
Epidemiology is a core discipline in the field of PH, which involves the study of the distribution and determinants of disease in populations. Epidemiologists investigate patterns of health and illness to inform control and prevention strategies. Biostatistics is another essential discipline that involves the application of statistical methods to PH research. It helps analyze health data, assess the effectiveness of interventions and make evidence-based decisions. PH professionals engage in policy development and management to create and implement strategies that improve health systems and services. This includes planning, resource allocation, and evaluation of health policies. Global health involves addressing health issues that transcend national boundaries. PH efforts at the global level focus on addressing infectious diseases, promoting maternal and child health, and improving healthcare infrastructure worldwide. PH plays a crucial role in preparing for and responding to PH emergencies, including natural disasters, infectious disease outbreaks, and other crises. This involves planning, coordination, and communication to protect the health of the population. Achieving health equity is a central goal of PH. This involves ensuring that all individuals can attain their highest level of health, regardless of socioeconomic status, race, ethnicity, or other socioecological determinants of health.
PH professionals work closely with communities to identify health needs and develop tailored interventions. Community health efforts involve collaboration with local stakeholders and organizations to address specific health challenges. PH interventions often require collaboration among government agencies, non-profit organizations, healthcare providers, and community members. The field is dynamic and responsive to emerging health challenges and societal needs.
Is there a connection between PH and TS?
PH and TS share the aim of improving health and well-being of populations by bridging the gap between scientific knowledge and practical applications, with a focus on translating research findings into interventions and policies that positively impact PH outcomes.
TS involves the application of research findings from science (such as laboratory studies) to real-world settings. In the context of PH, TS aims to translate discoveries into EBPs that can be implemented to prevent disease, promote health and improve healthcare delivery. IS, a subset of TS, focuses on the systematic study of methods to promote the adoption and integration of EBPs into routine practice. In PH, IS helps ensure that effective interventions are successfully implemented and sustained in diverse community settings. Both fields are concerned with health disparities and promoting health equity. TS in PH involves tailoring interventions to the specific needs of diverse populations and communities, ensuring that research findings are applicable and accessible to all segments of society. PH and TS often emphasize community engagement as a crucial component of their work. Engaging communities in the research process, from study design to implementation, helps ensure that interventions are culturally relevant, acceptable, and sustainable. 31
TS contributes to evidence-informed policy development in PH. Research findings are used to advocate for and inform policies that address PH challenges, ranging from environmental health issues to infectious disease control. The translation of scientific evidence into policy is a key aspect of both fields. TS plays a pivotal role in identifying effective prevention and intervention strategies. In PH, translational efforts focus on translating research into practical measures to prevent the spread of diseases, promote healthy behaviors, and improve overall population health. Many academic institutions and research centers have established specific units or centers dedicated to research translation in PH. These entities facilitate the translation of scientific discoveries into policies, programs, and interventions that have a direct impact on PH. PH research often involves surveillance and epidemiological studies to monitor the health of populations. TS contributes to turning surveillance data and epidemiological findings into actionable insights that inform PH decision-making. In the context of global health, TS plays a critical role in translating research findings into interventions that can be implemented across diverse global settings. This involves addressing health challenges that may vary based on cultural, economic, and geographical factors.
The connection between PH and TS highlights the importance of moving beyond the discovery of scientific knowledge to its practical application in real-world settings. Collaboration between researchers, practitioners, communities, and policymakers is essential to maximize the impact of translational efforts on PH outcomes.
Are there any synergies between TS and MS?
While TS and MS operate in distinct realms, TS focuses on bridging the gap between scientific discoveries and practical applications, while MS is concerned with creating, communicating, and delivering value to customers. Both TS and MS rely on effective communication: translational scientists need to communicate complex scientific concepts to diverse audiences, including patients, clinicians, policymakers, research participants, and general public; MS specializes in crafting messages that resonate with target audiences to promote products or services. Strategies from MS such as message framing and storytelling can be applied to enhance the communication of TS findings or to engage larger communities in research. TS often involves engaging stakeholders, including patients, practitioners, and policymakers; MS emphasizes understanding and engaging with target audiences. Techniques used in market segmentation, targeting, and positioning can be valuable for translational scientists in identifying and reaching specific stakeholder groups effectively. Both fields are concerned with influencing behavior: in TS, the goal is often to change health-related behaviors or to promote therapeutic adherence; MS has expertise in understanding consumer behavior and developing strategies to influence purchasing decisions. Techniques used in marketing such as social marketing principles can inform strategies for promoting health behavior change. Establishing a strong brand and managing reputation are critical in both fields: in TS, researchers and institutions seek to build credibility and trust in their work; MS provides useful insights into building and managing brands, understanding brand perception, and cultivating a positive reputation (relevant in TS!). Market research is fundamental in MS, involving data collection and analysis to inform business decisions. In TS, understanding the needs and preferences of target audiences is crucial for successful implementation. Techniques from market research such as surveys and focus groups can be applied in TS to gather insights from stakeholders. Both fields leverage digital channels and technology: in MS, digital strategies are employed to reach and engage with audiences online; in TS, digital communication platforms and technologies can be used to disseminate research findings, engage and educate the public, and facilitate collaboration between stakeholders. Both TS and MS involve creation and communication of value: translational scientists seek to demonstrate the value of their research in improving health outcomes; MS focuses on creating value propositions that resonate with customers. Aligning TS efforts with effective value propositions can enhance the adoption of research findings and innovations. While multiple synergies exist, it is essential to recognize the ethical considerations in applying marketing principles to TS, particularly in health communication. Balancing the need for effective communication with transparency and accuracy is crucial to maintaining the integrity of TS efforts. Collaboration between experts in both fields can lead to innovative and effective strategies for translating effectively scientific discoveries into meaningful applications.
What is data science?
DaS is a multidisciplinary field that involves extracting insights and knowledge from structured and unstructured data, using a wide range of techniques, processes, algorithms, and systems to analyze and interpret complex datasets. DaS combines elements of statistics, mathematics, computer science, and domain-specific knowledge to gain meaningful insights, inform decision-making, and solve real-world problems. Key components of DaS include data collection, cleaning, processing, standardization and quality assurance, data visualization and data analysis, statistical evaluations, model development, and often the use of advanced computational capabilities in ML, DL, or AI.
DaS involves gathering data from various sources, including databases, sensors, web scraping, and other data repositories; cleaning and organizing raw data to ensure accuracy, consistency, and completeness (e.g., handling missing values, dealing with outliers and transforming data into a suitable formats); analyzing and visualizing data in exploratory data analyses to discover patterns, trends, and relationships, which often helps in formulating hypotheses and guiding subsequent analyses, etc. DaS also may involve feature engineering, that is, creating new features or modifying existing ones to enhance the performance of various models. This step involves selecting relevant variables and transforming data to improve model accuracy. Employing ML algorithms to build predictive models or uncover hidden patterns in the data often require using techniques such as classification, regression, clustering, and recommendation systems. DaS sometimes deals with applying advanced statistical methods to validate hypotheses, assess the significance of findings, and make inferences about the population based on sample data. DaS may include assessing the performance of ML/DL models using metrics like accuracy, precision, recall, and F1-score. Model validation ensures that the chosen model generalizes well to new, unseen data. DaS often entails incorporating AI techniques such as natural language processing (NLP) and computer vision to enable machines to understand, interpret, and respond to human-generated data. Data ethics and privacy represent very significant domains in AI, as they help addressing ethical considerations related to data usage, ensuring privacy, and adhering to regulations and standards governing data handling.
DaS is widely applied in finance, healthcare, marketing and technology, aiming to derive valuable insights, automate processes, and support decision-making. Data scientists possess a combination of analytical, statistical, programming, and domain-specific skills. The field continues to evolve with advancements in technology, and its applications are expanding into areas like DL, reinforcement learning, and explainable AI.
What are the connections between DaS and TS?
DaS and TS share several facets, especially in biomedical research and healthcare. Both fields involve use of data to derive meaningful insights, inform decision-making, and drive advancements. They share similarities in data sourcing and use, biomedical informatics capabilities, modeling frameworks and intent (e.g., drug discovery vs TS processes). In TS, researchers work to bridge the gap between basic scientific discoveries and practical applications, while DaS plays a crucial role in this process by analyzing and interpreting diverse data types (e.g., omics, large clinical datasets). Data-driven insights help researchers understand disease mechanisms, identify potential therapeutic targets, and develop personalized treatment approaches. Biomedical informatics is considered by some the interdisciplinary field that integrates DaS with TS. It involves the application of computational and analytical methods to biomedical data. DaS techniques, such as ML and data mining, are often used to extract knowledge from large-scale biological and clinical datasets, supporting TR efforts. DaS techniques are applied to electronic health records, medical imaging data, and other clinical datasets to identify patterns, predict disease risks, and optimize treatment strategies, while TS uses these insights to implement EBPs in clinical settings.
Methods, such as predictive modeling and risk stratification, are used in both fields to forecast patient outcomes. TS leverages these models to identify patients at higher risk for specific diseases, enabling early intervention and personalized treatment approaches. DaS techniques, including bioinformatics and computational genomics, are employed to analyze large-scale genomic datasets. TS uses omics to understand the genetic basis of diseases, identify biomarkers, and develop targeted therapies. DaS is also increasingly applied in drug discovery and development processes. Computational approaches, such as virtual screening and molecular modeling, help identify potential drug candidates. TS then plays a role in moving promising candidates from preclinical studies to clinical trials, evaluating their safety and efficacy in human populations. Both fields contribute to the advancement of precision medicine. DaS techniques enable the identification of patient subgroups based on molecular and clinical characteristics. TS uses this information to design clinical trials that target specific patient populations, leading to more effective and personalized treatments. While IS focuses on translating research findings into routine practice, health informatics, a field closely related to DaS, supports this process by optimizing the use of information technology in healthcare delivery. Together, they contribute to the successful integration of EBPs into healthcare systems.
In summary, DaS and TS complement each other in leveraging data-driven approaches to advance biomedical research, improve health and patient care, and facilitate the translation of scientific knowledge into practical applications in healthcare settings. The integration of these disciplines is increasingly important in the era of precision medicine and personalized healthcare.
What is QI, QM, or Lean Six Sigma?
QI is a systematic and continuous approach to enhancing processes, products, or services within an organization, with the primary goal to improve efficiency, effectiveness, and overall quality. QI involves identifying areas for improvement, implementing changes, and measuring the impact of those changes over time. It is often applied within specific processes or functions to optimize performance, reduce errors, and enhance the overall quality of products or services. QI methodologies include plan-do-study-act (PDSA) cycles, root cause analysis, and other process improvement approaches.
QM is a broader organizational approach that encompasses all activities and functions within an organization to ensure that quality is built into its products or services. It involves setting quality standards, monitoring performance against these standards, and continually seeking ways to improve processes. QM is a holistic and systematic framework that may include elements of quality planning, quality assurance, and quality control. It often involves the establishment of a QM system that defines processes, responsibilities, and procedures to achieve consistent quality.
Lean Six Sigma is a combination of the two methodologies, which aims to improve efficiency, eliminate waste, and reduce variations in processes. Lean principles focus on reducing waste and optimizing processes by identifying and eliminating non-value-added activities, creating value for the customer while minimizing resources and time. Six Sigma is a data-driven approach that aims to reduce defects and variations in processes, using statistical methods to measure and improve process performance, with the ultimate goal of achieving near-perfect quality. Lean Six Sigma integrates the principles of both Lean and Six Sigma to provide a comprehensive approach to process improvement. It is structured around the Define, Measure, Analyze, Improve, Control (DMAIC) methodology.
While QI often focuses on specific processes or functions within an organization, QM encompasses nearly all its activities and functions, while Lean Six Sigma focuses on improving efficiency and reducing variations in processes. QI addresses waste and inefficiencies in processes, QM seeks to optimize all processes for efficiency, while Lean Six Sigma specifically incorporates Lean principles to eliminate waste. QI may use data but may not be as rigorously data driven as Six Sigma; QM focuses on ensuring processes are efficient and effective but may not rely extensively on statistical data; in contrast, Lean Six Sigma incorporates robust statistical methods for measuring and improving process performance.
In summary, while QI focuses on specific improvements, QM encompasses an organization-wide commitment to quality, and Lean Six Sigma integrates Lean and Six Sigma principles for comprehensive process improvement. Each approach has its strengths and organizations may choose the one that best aligns with their goals and context.
Is Rapid Cycle Development (RCD) relatedto IS or QI?
The concept of RCD is not attributed to a single individual and has evolved over time in various fields, particularly in the context of QI, project management, and agile methodologies. The concept of rapid cycle improvement is closely associated with QI initiatives, particularly in healthcare. Pioneers in this field, such as W. Edwards Deming and Walter Shewhart, emphasized the importance of iterative cycles of PDSA to continuously improve processes and outcomes. This iterative approach has been influential in other industries, beyond healthcare. 32 In the realm of software development, the Agile Manifesto, published in 2001 by a group of software developers, advocated for iterative and incremental development practices. 33 Agile methodologies, including Scrum and Extreme Programming, are built on the idea of rapid cycles of development, testing, and deployment to respond to changing requirements and deliver value quickly. 34 Lean principles, derived from Toyota's production system and popularized by authors like James P. Womack and Daniel T. Jones, emphasize continuous improvement through elimination of waste. 35 Lean thinking often involves shortening cycles, reducing lead times, and responding to customer needs swiftly.
In project management, the concept of iterative development has been embraced in approaches like the Rapid Application Development model, which seeks to speed up software development through rapid prototyping and frequent feedback. 36 In the realm of design and product development, human-centered design methodologies like DT encourage iterative prototyping, user feedback, and rapid cycles of development to create products and services that better meet user needs.
The concept of RCD is a general approach that has been adapted and evolved across many fields. The specific practices and terminology associated with RCD may vary depending on the context. In healthcare QI, for instance, it is often referred to as PDSA cycle, while in software development, it aligns with agile practices like Scrum and Kanban. The common thread is the emphasis on iterative, rapid cycles to improve processes, products, or services.
What is engagement science?
Engagement science (ES) is a transdisciplinary field focused on understanding, measuring, and enhancing the ways individuals and groups interact with various systems, technologies, organizations, or social structures. ES studies how to effectively engage people to achieve the desired outcomes in healthcare, education, marketing, PH, or community development. ES combines insights from behavioral and organizational psychology, sociology, technology, CS, MS, and PH, focusing on interactions and people engage with systems, services, and with each other. ES uses various tools and methods to quantify levels of engagement, via surveys, behavioral analytics, qualitative, observational, and experimental studies. ES develops and tests strategies to enhance involvement such as personalized communications, incentives, feedback systems, and community-building activities. 37 ES theories are standard frameworks designed to explain the ways in which active participation and meaningful interaction can enhance learning, motivation, and performance across various contexts, such as education, business, and technology. The theories emphasize the importance of collaboration, interaction, and active involvement to foster deeper engagement and achieve better outcomes, relying on several key components: active learning via discussions, problem-solving, and hands-on projects; collaborative efforts (encouraging teamwork, participation in meaningful tasks, and sharing ideas) to achieve common goals. 37 ES often leverages the latest and the most interactive technologies and social media platforms to facilitate engagement by providing interactive, dynamic, and personalized learning experiences. The elemental principles of ES theories are: relate (i.e., learning together), create (via constructive activities), and donate (effort, time, resources). At Medical College of Wisconsin and CTSI of Southeast Wisconsin, we have developed TR and TS on trust-based community engagement as a core pillar of our mission, relying on several faith-based community ecosystems for engagement activities that are highly grounded in ES theories and aimed at improving the health of more people in the local community.
What is improvement science?
Improvement science (ImpS), a combination of IS and QI, is defined as the field of study or discipline focused on understanding and implementing methods needed to enhance quality, efficiency, and effectiveness of processes, particularly in healthcare, education, and other service-oriented environments. ImpS applies rigorous scientific methods to identify areas prime for improvement, test changes, and measure the impact of different interventions to achieve better outcomes such as enhanced patient safety, better educational outcomes, or increased process efficiencies. ImpS uses systematic approaches and structured methodologies to diagnose problems, develop interventions, and evaluate outcomes, performing iterative testing and change refinements in an inter- or transdisciplinary fashion, with a strong focus on outcomes. The discipline relies heavily on DaS and analytics to inform decision-making, for tracking progress, and to determine the effectiveness of various interventions.
What are the connections between QI, IS, ImpS, and TS?
There are several areas of intersection and similarities between these fields. First, they share a continuous improvement focus, entailing systematic and iterative processes that aim to enhance outcomes over time. Second, they employ data-driven approaches, recognizing that data are a critical component in each field. Whether measuring process efficiency, evaluating the success of implementation, or assessing the impact of translational efforts, data-driven decision-making is near -emphasized. Third, engaging stakeholders is essential in all three. This includes involving individuals or groups affected by changes, interventions, or research to ensure a wide collaborative and informed approach. Transdisciplinary collaboration is often the norm in all three disciplines. Finally, adaptability, flexibility, and continuous learning are key principles, recognizing the dynamic nature of their respective domains and the importance of adapting strategies based on new information and insights. Perhaps not surprisingly, they all have to deal with the trade-off between fidelity and adaptability of their interventions, albeit with slightly different approaches. There are several differences between these fields too, some related to scope, scale, or time horizon of the activities, others related to methodologies, outcome measures, or context (Table 4). Understanding these similarities and differences can help organizations tailor their approaches and strategies based on their specific goals, whether itis process optimization, effective implementation of EBPs and interventions, or the translation of scientific discoveries into practical applications.
An overview of how design thinking (DT) can be applied and medicine or healthcare, and in translational science (TS).

Matrix representation of the main differences of approach between quality improvement (QI), implementation science (IS), and translational science (TS).

At Medical College of Wisconsin and CTSA hub of Southeast Wisconsin, we have enriched the expertise of our Team Science Ensembles and pilot award investigator teams by putting together a TS Core, which brings together resources and faculty with various skillsets, toolboxes, frameworks, specific knowledge bases, and approaches from some of the contiguous specialties and disciplines described above (Figure 1). The declared intent of this endeavor is to have the TS Core activated and involved in the Pre-ensemble forming phase of the Team Science creation, with expertise customization and consultation, as needed for various research- or practice-related projects, which may benefit greatly from various specialists and early input in the design and successful deployment of their studies.
In summary, building a robust TS machinery or engine is essential to the success of moving along research findings and innovations into practice, communities, and populations at large. This type of infrastructural enhancement and service portfolio development may require equipping CTSA hubs with specific capabilities from other fields of study, specialties, or disciplines. This can be accomplished by borrowing, developing, and/or employing consultative services provided by specialists from very different and sometimes overlapping domains, fields, or disciplines.
Footnotes
Correction (April 2025):
Author contributions
Both OCI and RS contributed to the manuscript (concept and writing).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH (NCATS) UL1 TR001436 (MCW IRB# FP00015891); PI: Reza Shaker.