
Abstract

This issue of JIM publishes an interesting perspective article written by Professor Dr Gailen D Marshall Jr,1 which includes a high-level critical appraisal of the current state of medical research and the emerging concept of ‘team science’.2 The article also provides an overview of the existing researcher pipeline, challenges and opportunities for physician scientists, translational medicine or clinical investigators in an environment that is both shifting in priorities, resources and approaches, and perhaps drifting strategically.
Despite tremendous advances in medical research, our clinicians face daunting challenges, ranging from new conditions (COVID-19 infection?), a myriad of disease phenoendotypes and variations in response to available therapeutic interventions, and ever-increasing numbers of people with chronic disorders. The gap between biomedical research and unmet clinical needs could and should be addressed by teams of investigators focused on swift, collaborative translational, bench-to-bedside exploration. As such, the process of recruitment, training and retention of talented physician scientists working in interdisciplinary teams, addressing these complex health problems becomes a top national priority.
History of medical research and its funding strategies is marked by an initial working approach to separate or delineate domains, distinct areas or separate ‘bins’, such as basic science,3 clinical trials or population health (paradigm 1, figure 1). There are concomitant advantages and risks in taking such an approach. Structure creates function, and function shapes structure. As such, one unintended consequence of these distinct funding and development pipelines was de facto creation of separate ‘silos’, with limited communication or even common language. Over time, the entire process of discovery became plagued by lack of communication, subpar collaboration, unidisciplinary approaches, too many rhetorical or unasked ‘so what?'s, and even suboptimal outputs. The next major approach to strengthen translational research (paradigm 2, figure 1) delineated several domains organized around a prescribed discovery journey from bench research (T0), to animal models (T1), to human trials (T2), followed by implementation science studies (T3) and population studies (T4). One major drawback of this model was related to its extreme linearity, the phase-based, compartmentalized, unidirectional communication and somewhat restricted feedback loops.
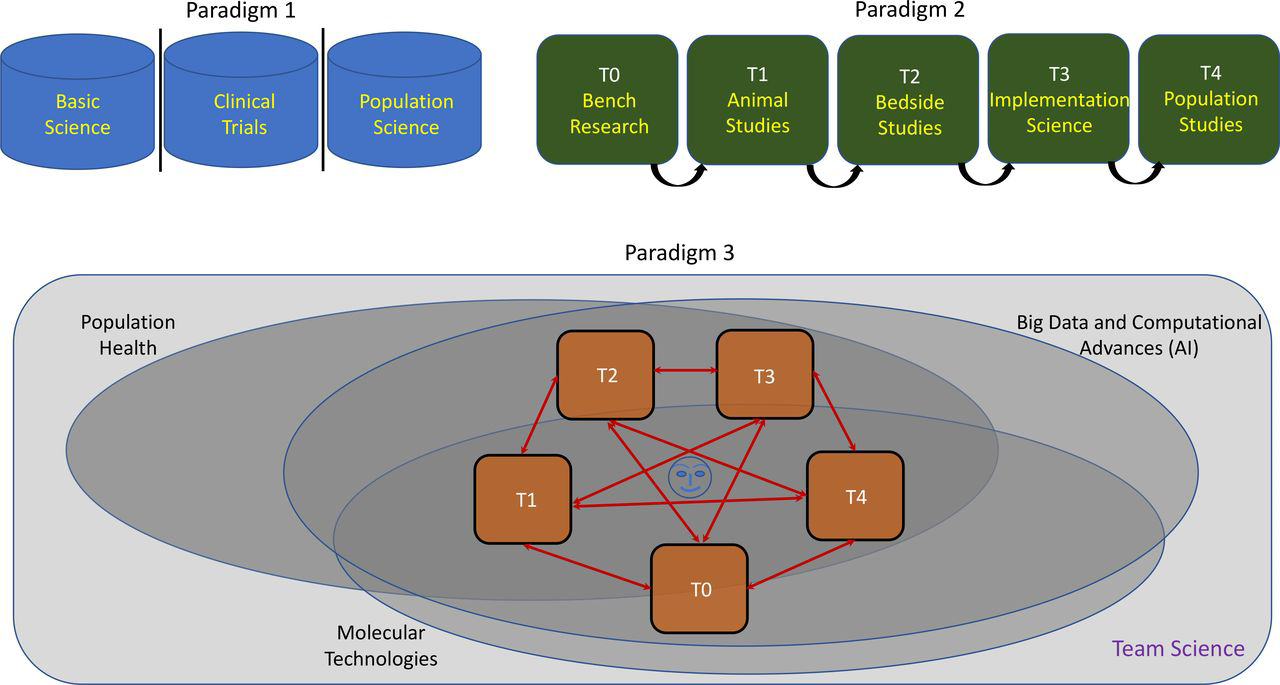
Three major paradigms for the journey of medical discovery: (1) the ‘silos’ of basic science, clinical trials and population health; (2) the linear structure consisting of various domains (T0–T4) in translational research; and (3) an integrated approach encompassing non-linear, bidirectional relationships between T0 (eg, in vitro or in silico studies), T1 (eg, in vivo animal studies), T2 (eg, human clinical trials), T3 (eg, implementation science, healthcare delivery science, quality improvement-based studies) and T4 (populational studies) in a larger context of ‘team science’, which incorporates also population health platforms, ‘big data’, the most advanced computational capabilities including artificial intelligence (AI), and the latest advances in molecular, high-throughput assays coupled with the newest and most powerful technologies, all in a patient and family-centric fashion.
The good news is that the infrastructure-building journey continues and promises great progress in creating real collaborative teams (paradigm 3, figure 1).4-7 The latest, powerful computational advances, the newest artificial intelligence (AI) capabilities, increasing availability of ‘big data’, significant molecular and technological advances and population health platforms can be all aligned with the goal of real science teams, in the service of patient and family-centric research. The article written by Dr. Marshall also discusses the necessary, deliberate efforts that have to be put into mentoring junior faculty and early investigators, and to balance the pull from different directions (between traditional academic milieu and the new realities of the business of healthcare, between clinical loads and ‘protected’ scholarly time, and so on).
One consistent message that we should deliver to our governments, regulators and leaders of various funding agencies is that the amount, ease of access, and significance of these funding flows are ultimately commensurate in the immediate, medium and long term with the ranking one country has on the stage of medical discovery worldwide. Commensurate with the future number of Nobel prizes for medicine and science. From this very point of view, the perspective article written by Dr Marshall provides both implicitly and explicitly a robust call to arms into this noble (sic!) battle.