
Abstract
Shoulder dislocations are prevalent on Earth and pose unique challenges in spaceflight and spaceflight training, particularly during extravehicular activities (EVAs). This case report describes a 50-year-old male who experienced an anterior shoulder dislocation while performing an emergency egress exercise in a SpaceX EVA suit. The report describes the medical thought process, the operational constraints, and the reduction techniques employed to achieve a successful shoulder reduction without fully removing or damaging the suit. NASA estimates a high likelihood of shoulder injuries during long-duration lunar missions, emphasizing the importance of suit designs and rescue protocols. Quick and effective medical intervention is crucial, as delays can lead to complications. This Earth-based case report provides some insight into reduction technique considerations for suited spaceflight operations in varying gravitational environments.
Keywords
Introduction
Shoulder dislocations are the most common of all major joint dislocations, occurring at an estimated incidence rate of 23.9 per 100,000 person-years.1,2 Historically, shoulder injuries have been relatively common in human spaceflight and astronaut training, particularly during extravehicular activity (EVA), colloquially known as “spacewalks.” These injuries can be mission impacting.3‐5 NASA's Human Research Program has estimated that if prior EVA suit injury rates persist, a crew engaging in a 6-month lunar surface mission would have over a 99% probability of experiencing at least 1 shoulder injury during EVA. This projection is based on the roughly 3.5% incidence of shoulder injuries per EVA observed in Apollo (3.57%, 1 in 28 EVA exposures) and ISS missions (3.54%, 4 in 113 mission exposures), extrapolated to the number of EVAs expected in a long-duration expedition. 6
Due to their high incidence and potential to impact mission success, EVA suit engineers, researchers, and medical teams have conducted extensive research on shoulder injuries during EVA and training. The frequency and severity of shoulder injuries during training in the NASA space suit (extravehicular mobility unit, or EMU) were such that in 2002, NASA established the “EMU Shoulder Injury Tiger Team” specialized group comprising engineers, flight surgeons, and other specialists dedicated to investigating and mitigating shoulder injuries associated with space suits. 7 In addition, NASA has conducted studies to quantify the incidence of shoulder injuries during both training and actual EVAs. 6 Based on findings from the EMU Tiger Team and other research, NASA has recommended several design changes to reduce the risk of shoulder injuries. 3 These include, among others, increasing suit flexibility, decreasing suit mass, lowering the center of gravity, and reducing internal pressure. This prior work has helped NASA and commercial spaceflight companies create new protocols and suit designs that are aimed at reducing shoulder injuries in future training and flight suit designs.
We report a case of an anterior shoulder dislocation during ground testing in a SpaceX EVA suit. In this case, a range of approaches were considered, including cutting the suit and self-reduction inside the suit. Ultimately, the shoulder was successfully reduced by medical personnel without damaging or fully removing the suit. This case raises important questions about emergent and nonemergent extrication strategies both in the terrestrial environment and in space. As space travel becomes accessible to a more varied population, the EVA suit's design in relation to human anatomy and rescue will be a growing consideration.
Case Report
A 50-year-old male with a history of right-sided shoulder dislocations (first dislocated during high-intensity interval training in 2009, with 3 subsequent dislocations in 2012, and 1 dislocation in 2023) was practicing an emergency egress exercise in the Dragon spacecraft with the SpaceX Polaris Dawn mission crew in California in spring 2024. The individual was wearing a SpaceX EVA suit (Figure 1) in an unpressurized configuration. He was lifting a heavy raft out of the spacecraft when his foot slipped, and he felt a 9/10, sharp pain in his right shoulder similar to prior dislocations. The individual was unable to abduct and externally rotate his right arm due to pain and a feeling of instability at the shoulder joint. Initially, he tried to self-reduce with the assistance of another crewmember, which was unsuccessful. He then alerted the training team and flight surgeons, who came and evaluated the individual.

SpaceX EVA suit.
The medical team found the subject in the EVA suit, and the suit's circular zipper at the patient's abdomen (used during standard donning and doffing procedures and the most easily accessible entry point) was already opened by the patient. The suit was not pressurized at this time, and the atmospheric pressure inside the suit and outside the suit were equivalent at sea level (101 kPa/14.7 psi). On initial evaluation, the subject arrived with an open suit glove zipper, which allowed access to the hand and the performance of an exam. The neuromuscular examination, though limited by the suit, showed normal muscle strength and intact sensation of the hand, with no signs of radial nerve impairment. Both the radial and ulnar pulses were strong, indicating no vascular compromise.
Given the described mechanism of injury, the inability to voluntarily abduct the arm, and the patient's history of shoulder dislocation on the same side, there was a high suspicion of an anterior shoulder dislocation. The thickness of the fabric made palpation outside of the suit unreliable, and due to the lack of radiography at the training site, the dislocation was not confirmed with radiographic evidence. (Ultrasonography cannot be performed through a suit, as an air gap remains between the suit and the skin).
The EVA suit is made of a composite of fabric, hard and soft, materials with multiple layers and is form-fitting, requiring extensive movements of the arm and shoulders to remove. The suits are unique items, customized to the individual based on individual anthropometric measurements. Normal suit doffing requires shoulder abduction and given the pain and instability of the shoulder joint, the individual was incapable of removing the suit himself. The flight medicine support team considered cutting the suit for immediate access but decided to first attempt to reduce the shoulder without fully removing the suit due to neurovascular stability of the limb and subject's preference.
Given the subject's known history of shoulder dislocation, the flight medicine team was aware of the potential risk and had discussed general management strategies in advance. However, no formal, step-by-step in-suit reduction protocol existed for this scenario. As such, all reduction maneuvers were carried out in real time using standard reduction principles and clinical judgment, rather than a pre-scripted procedure. Multiple attempts were performed by the individual alone using the Davos (Boss-Holzach-Matter) technique, in which the individual used his knee to self-administer traction-countertraction.8,9 These were unsuccessful and were attempted without fully removing the patient's suit. Given neurovascular stability, the subject's preference, and the high chance of success (no analgesia or sedation was needed in all but one of the subject's prior shoulder dislocations), these attempts were made on site.
Utilizing the open abdominal zipper of the suit, the flight surgeon inserted a hand between the suit layer and the astronaut's body to palpate the shoulder, while another team member provided external stabilization on the arm. At this point in time, the flight surgeon was able to palpate the shoulder joint, noting an anteriorly displaced humeral head and palpable sulcus sign, suggestive of anterior dislocation. The flight surgeon then slid their hand and massaged the trapezius, deltoid, and biceps muscles sequentially. This, combined with gentle downward traction and gentle circular motion, was able to reduce the shoulder, culminating in a modified version of the Cunningham technique. 10 The flight surgeon noted a palpable event at this time and noted restoration of normal shoulder contour and improvement in the patient's pain, consistent with successful anatomic realignment. No medications or analgesia techniques were used. Successful reduction occurred approximately 10 min after the dislocation was reported to the flight surgeons.
After the shoulder was successfully reduced, the suit was doffed with assistance from the flight medicine team. Although the crew was usually able to doff unassisted, the suit was not damaged and was removed using standard procedures. The repeat neurovascular exam was unremarkable. The shoulder was then immobilized with a sling, and the subject was taken to a local clinic where a 3-view shoulder series demonstrated anatomic alignment. Over the ensuing weeks, the patient and flight medicine team worked with an orthopedic surgeon and sports medicine physical therapy specialist to develop a return-to-flight protocol, with serial examinations and progressive return to activity with benchmarks. Additionally, the flight team developed a protocol for in-flight shoulder reduction and trained the crew medical officer should a redislocation occur during flight. Maneuvers requiring lifting heavy objects and overhead lifting were avoided by the subject, and mission protocols were altered to prevent these activities. The patient later flew successfully on the Polaris Dawn mission (September 10–15, 2024).
Discussion
Shoulder dislocations are the most common of all major joint dislocations, accounting for 50% of all major dislocations.2,11‐14 Anterior dislocation is most common, accounting for 95% to 97% of cases. Posterior dislocation accounts for 2% to 4%, and inferior dislocation accounts for 0.5%. 2
Risk factors include young age and male sex, with approximately 72% of total presentations occurring in males, and nearly one-half occurring in patients between the ages of 15 and 29 years. 2 Of these, almost one-half of shoulder dislocations occurred while the patient was engaged in a sport or recreational activity.1,2,13 In addition, prior dislocations are a risk factor, with up to 36% of first-time dislocations happening again within 12 months. 27 Further risk factors of recurrent dislocation included bony Bankart lesions, individuals who had not been immobilized in a sling, and higher levels of shoulder activity.
Astronaut training may be especially provocative for shoulder injury, and pressurized spacesuits have been shown to cause injuries.15‐18 While hands and fingers are the most common sites of injuries during both training and flight, shoulder injuries are still very common. 7 A study conducted from July 2002 to January 2004 found that after training in the Neutral Buoyancy Laboratory, 45.7% of the astronauts reported symptoms, and 21% of these involved the shoulders (47% involved hands; 11% involved feet; 6% each involved arms, legs, and neck; and 3% involved the trunk).5,7 Not only are shoulder injuries common during training, but they have also occurred in spaceflight. A retrospective analysis of medical records, focusing on one injury type—“shoulder injury”—demonstrated an incidence of 3.54% (4 in 113 EVA exposures) per International Space Station EVA and 3.57% (1 in 28 EVA exposures) during the Apollo program.4,6 Extrapolating from this suggests a greater than 30% probability of an EVA shoulder injury in a short stay (<30 days) lunar surface mission and a greater than 99% probability of an EVA shoulder injury during a long stay (between 30 days and 1 year) lunar or Martian surface mission, if injury incidence is not decreased. 6
In addition to being very common, shoulder injuries may impair crew performance and lead to the loss of multiple mission objectives. 6 In 2020, NASA's Human System Risk Board (HSRB) classified the “Risk of Injury and Compromised Performance Due to EVA Operations” as a “red” risk for even short-duration lunar missions. 19 In shoulder dislocations, axillary nerve dysfunction is common and is diagnosed in up to 40% of patients with an anterior dislocation. 14 In the vast majority of cases, dysfunction resolves with reduction or shortly thereafter.
In remote or resource-limited settings, several strategies can aid in diagnosing anterior shoulder dislocation when imaging is unavailable. Simple functional assessments, such as asking the patient to place the hand of the affected arm on the opposite shoulder, can be diagnostic, as patients with anterior dislocation are typically unable to perform this maneuver due to pain and mechanical limitation. Point-of-care ultrasound is another accessible tool that can confirm dislocation by identifying the humeral head position relative to the glenoid. Visual asymmetry, palpable step-off at the shoulder, and restricted or painful external rotation are also key clinical clues. Incorporating these techniques into crew medical training may improve diagnostic confidence when radiographic imaging is not available.
Shoulder dislocations require technical and medical expertise for reduction in order for the arm to be fully functional again. In a Norwegian registry study, two-thirds of shoulder dislocations were reduced in the emergency department, while approximately one-fourth were reduced prior to arrival at the emergency department. 1 Only 0.6% of reductions were reduced spontaneously. While underutilized, multiple studies have shown safe and effective reduction of shoulder joints in wilderness, mountain ski clinics, EMS settings, sports venues, and other prehospital settings, with success rates ranging from 54% to 94.9%.11,20‐24 Timing is also very important: Several studies suggest that delays as brief as 10 min increase the likelihood of failed reduction, increase muscle spasms, and increase the likelihood of neurovascular injury.20,21 As the average time to reduction can exceed 135 min in medical facilities, this case (attempted and completed promptly despite the constraints of a bulky suit) demonstrates the importance of acting quickly in a resource-limited environment. 24
As we look toward the future, it is expected that with an increased number of individuals working and training in EVA suits, potentially drawn from a less-screened population, there is a higher potential for injury. Operational controls need to be designed and implemented to reduce the risk of both acute injury during high-risk activities and chronic “overuse” injuries. Currently, the International Space Station crew has had a minimum of 4–5 days of rest between EVAs. However, current plans for lunar missions assume daily EVAs, and it is estimated that surface EVAs in partial gravity are likely at greater risk due to gravitational force and associated risk of falls compared to EVAs in microgravity. Indeed, Apollo lunar surface EVAs experienced frequent falls, in part due to suit factors such as center of gravity, reduced mobility, uneven terrain, etc. Planned planetary surface suits are significantly heavier than those used in Apollo. Even though the gravitational force is reduced compared to Earth, the inertial mass remains unchanged, potentially lulling the crew into a fall where they may experience higher loads than expected from the reduced-gravity environment. Mission objectives and ergonomic patterns that can reduce lifting heavy objects, repetitive motions, and overhead tasks are also recommended. 7 These changing mission objectives and timelines will require new operational parameters.
In addition to operational controls, suit design is incredibly important. The NASA EMU Shoulder Injury Tiger Team study found that the EMU's (Figure 2) hard upper torso's shoulder joint increased the risk of shoulder injuries, especially when performing overhead tasks and in inverted body positions on Earth during training. The study team recommended increasing ambulatory and functional capability by increasing suit flexibility, decreasing suit mass, lowering the center of gravity, and reducing internal pressure. 17 It is important to note that shoulder injuries encountered in space suits are typically associated with poor ergonomics and restricted range of motion, often leading to overuse or impingement-type injuries. In contrast, dislocations generally result from external loads applied during states of hypermobility. Given that pressurized space suits inherently limit shoulder abduction and external rotation, they may, in some contexts, offer a degree of protection against anterior dislocation by physically preventing the vulnerable arm positions that predispose to such injuries. It may be important to consider that increased flexibility of the suit may have tradeoffs in terms of protection and increased risk of different shoulder injuries.
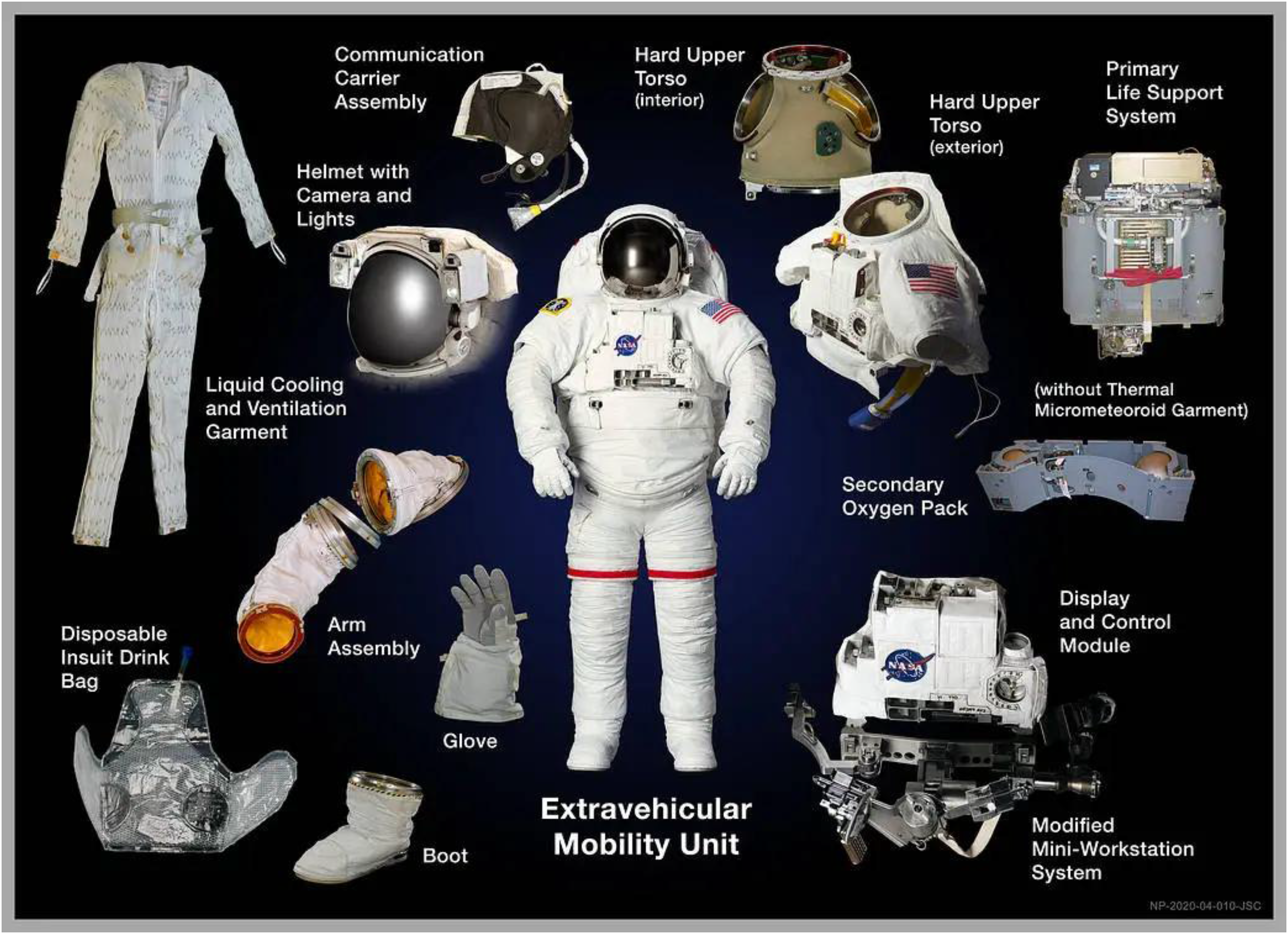
NASA EMU suit (https://www.nasa.gov/image-article/extravehicular-mobility-unit-emu/).
Given the likelihood of musculoskeletal injuries and the case mentioned previously, it is also important to consider rescue and treatment of medical conditions. In the case of the EMU, the suit arm is attached to the torso via a scye bearing (Figure 2), potentially allowing the removal of the suit arm to provide access to the shoulder joint for direct manipulation. However, the solid torso construction could potentially preclude extrication without significant sedation and would be outright impossible to “cut” in-flight. While EVA suits are the focus of the risk discussion, crew members don a separate intravehicular (IV) pressure suit for dynamic events such as launch, landing, and docking to provide protection in the event of a loss of cabin pressurization. A failure to reduce a dislocation would preclude IV suit donning, not only costing mission objectives but also placing that crewmember at increased risk in a vehicle contingency. Human-in-the-loop testing is critical for identifying and reducing strain on anatomic weak points and enabling better ergonomic design of future space suits.
Lastly, access and medical treatment considerations are important. During long-duration space missions, pain management may be required for unanticipated accidents (eg, fractures of bones, lacerations, or blunt trauma), medical conditions such as appendicitis, or a perforated viscus. Quick access to the individual may be important in designing future suits. An example of this occurred in 2014 with the Stratex Project, a high-altitude balloon flight that culminated in a free-fall from 41,422 m (135,890 ft). In this unique mission, the medical support team coordinated with the pressure suit assembly engineer team for integration, training in suit removal, definition of a priori contingency leadership on site, creation of color-coded extraction scenarios, and extraction drills with a suit mock-up.25,26 These scenarios demonstrated that coordination between suit designers and medical teams can help optimize suits and procedures in the case of emergencies.
Regardless of the suit design, conditions such as microgravity may present challenges to shoulder reduction. Techniques that require torque, such as scapular manipulation, would require that the patient and the person providing the reduction be fixed. Ways to restrain individuals for certain medical interventions (eg, CPR) have been tested in zero-G flights and have been implemented on the International Space Station. However, these restraint mechanisms have not been studied at great length for potential reductions, nor would they necessarily be the best options for restraining individuals. Furthermore, whereas the ISS has crews of 7 or more astronauts at a time (and thus significant help can be summoned), initial lunar missions include mission phases with only two individuals in a vehicle—including the lunar surface phase during which EVAs would be conducted.
Simplified analgesic and anxiolytic protocols could be valuable in future missions. At a baseline, crew medical training should emphasize general principles to enhance effectiveness, such as maintaining a calm environment, minimizing painful or abrupt movements that provoke muscle spasm, and progressing slowly through reduction attempts. Nonpharmacologic techniques, such as guided imagery or a light hypnotic trance (taught in wilderness EMS settings and shown to facilitate joint reductions), may also offer a low-resource means to relax muscle spasm and allow patient cooperation. 28 Oral nonsedating analgesics, muscle relaxants, ultrasound-guided nerve blocks, or small-dose oral benzodiazepines could potentially aid cooperation while retaining airway safety in environments where sedation monitoring is limited. Sedation, if performed, may need to be conducted by the same, single individual that would also have to perform the reduction, with limited monitoring tools and potentially limited reversal agents. Although astronauts receive some medical training, it does not include moderate sedation for procedures. Additionally, most astronauts are not physicians, and there is currently no requirement for a physician-astronaut on future flights. The risks associated with sedation (aspiration, airway management, and rescue techniques) in micro- or reduced gravity are still unknown.
Even if the reduction is deemed successful, imaging modalities to assess the injury and reduction are limited; there are no plans for radiographic imaging in current design reference missions, and ultrasound imaging capability is not guaranteed. A return to Earth may take over a week, depending on the mission phase and orbital mechanics.
The return to duty—both for contingency/return to Earth scenarios as well as return to full duty (including return to performing EVAs)—will also require careful assessment of the individuals’ particular injury, recovery, and functional status by the flight surgeon and specialists on Earth.
Conclusion
Shoulder dislocations are the most commonly reported of all major joint dislocations on Earth and present a risk to human spaceflight, particularly during EVA. We report an anterior shoulder dislocation in a SpaceX EVA suit that was reduced without fully removing the suit. As space travel becomes accessible to a more diverse population, a suit’s design in relation to human anatomy and medical interventions will become a growing consideration. Preserving suit integrity and function is critical not just for EVAs but also during operations that could result in loss of cabin pressure, where pressure suits are used to mitigate risk by protecting the crew against hypobaric exposure. In addition, further research is needed on how to determine the best reduction techniques for unique space environments with microgravity or partial gravity.
Footnotes
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.